Can a brief phone call intervention promote treatment seeking in adults with severe alcohol use disorder?
Screening, brief intervention, and referral to treatment reduces alcohol use among individuals with milder alcohol use disorder, but the referral to treatment component for those with more severe alcohol use disorder has been less effective. The present study tested whether cognitive behavioral therapy (CBT) delivered by phone would help more people with severe alcohol use disorder seek treatment.
The authors of the present study previously developed Cognitive Behavioral Therapy (CBT) for Treatment Seeking as a single session (45-60 minute), telephone-delivered intervention designed to promote the use of alcohol treatment among individuals with severe alcohol use disorder. Previous findings indicate that in a sample of individuals with alcohol use disorder who had not been to treatment (i.e., “treatment naïve”), those receiving this CBT adaptation were more than twice as likely to seek alcohol treatment than those in the control who listened to information from a pamphlet about alcohol use disorder treatment. The present study built on prior work by testing CBT for treatment seeking in a randomized controlled trial.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial comparing CBT for treatment seeking to an NIAAA pamphlet on alcohol use disorder treatment. Eligibility criteria for inclusion in the study were as follows: 1) 18 years of age or older; 2) score >16 on the Alcohol Use Disorders Identification Test; 3) exceeding recommended limits for low-risk drinking within the past 30 days (≥4 standard drinks on any occasion or >7 drinks per week [women]; ≥5 drinks on any occasion or >14 drinks per week [men]). Participants were excluded if they lacked English proficiency, were currently experiencing alcohol withdrawal necessitating medical evaluation, or if they had any prior history of professional alcohol-related treatment (does not include mutual help organization attendance, such as Alcoholics Anonymous). Participants were equally male and female, primarily White (79%), and an average age of 40 years. A total of 400 participants were randomized to either the CBT for treatment seeking intervention (n=197) or control (n=203) condition which consisted of reviewing an NIAAA pamphlet on alcohol use disorder treatment.
CBT for treatment seeking is a brief, structured, telephone-based, single session intervention lasting between 45 to 60 minutes. The underlying aim of CBT for treatment seeking is to change beliefs related to a person’s decision to seek alcohol treatment. The session involves four consecutive stages: 1) discussing alcohol consumption, 2) discussing strategies used to manage drinking (if any), 3) eliciting beliefs about alcohol treatment, and 4) discussing each belief in detail. The interventionist is tasked with seeking to modify each belief with the participant. Though the structure of the intervention remains consistent, the content discussed within each session is tailored to respond to the participant’s beliefs. Local treatment resources and different treatment options were also discussed upon request. The control group received an NIAAA pamphlet presenting information on alcohol use disorder symptoms and evidence-based treatment options, which was reviewed during a 10–15-minute phone call with a study staff member.
Assessments were conducted at baseline, and 1-, 3-, and 6-months post-randomization. The primary outcome assessed was any recorded professional alcohol use disorder treatment use over 3-month follow-up, including any of the following 11 sources: (1) family or social services agency; (2) alcohol or drug detoxification ward or clinic; (3) inpatient ward of a general hospital, community mental health program or inpatient psychiatric hospital; (4) outpatient program including day or partial hospital treatment; (5) alcohol or drug rehabilitation program; (6) emergency room or urgent care facility; (7) halfway house or therapeutic community; (8) crisis center; (9) employee assistance program; (10) member of the clergy including a priest, rabbi or any type of religious counselor; and (11) private provider including primary care physician, psychologist, psychiatrist, social worker, nurse or another professional counselor (Alcohol Use Disorders Identification and Associated Disabilities Interview). Secondary outcomes related to past 30-day alcohol consumption at 6-month follow-up accounted for alcohol intensity (i.e., average number of standard drinks per day of drinking in the past 30 days) and alcohol frequency (i.e., number of days of drinking in the past 30 days; Timeline Follow Back Interview).
The primary hypothesis was that individuals who received the CBT for treatment seeking intervention would be more likely to attend one or more alcohol use disorder treatment sessions by 3-month follow-up, compared to controls who reviewed a pamphlet on treatment with study staff. Those with missing treatment initiation data were assumed not to have sought treatment, a rigorous approach to handling missing outcome data and providing a more stringent test of whether the single session CBT intervention enhanced treatment engagement as designed. The secondary hypothesis was that compared to those assigned to the control group, individuals in the intervention group would experience greater reductions in alcohol use at 6-month follow-up. The authors also hypothesized that reductions in alcohol consumption experienced by the intervention group would be explained by increases in alcohol treatment engagement.
WHAT DID THIS STUDY FIND?
The intervention did not improve outcomes
The primary hypothesis suggesting that CBT for treatment seeking would increase treatment initiation during 3-month follow-up was not supported. There were no significant differences in treatment uptake between intervention (19%) and control (18%) conditions. As shown in the figure below, treatment attendance in the first month, as well as the second and third months, were similar for both groups.
Figure. CBT for treatment seeking did not improve treatment attendance compared to reviewing an NIAAA pamphlet with study staff.
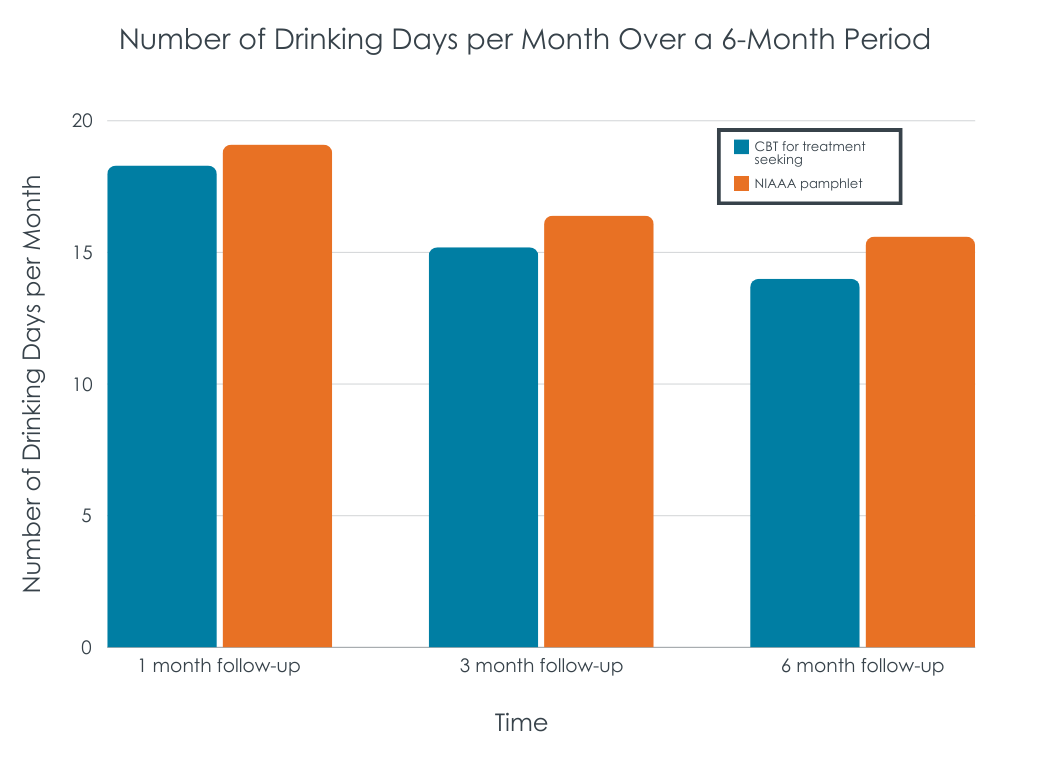
The secondary hypothesis that participants in the intervention condition would experience greater reductions in alcohol use relative to the control at 6-month follow-up was not supported. There were no observed differences between the two groups on alcohol use intensity or frequency at any time point. When combining the results from the two arms, there were linear reductions in past month number of drinks per occasion (from 6.0 drinks per day at 1-month follow-up to 4.4 drinks per day at 6-months) and past month number of drinking days (from 18.2 days at 1-month follow-up to 13.7 days at 6-month follow-up). However, there was no interaction between time and condition, meaning the intervention did not impact changes in drinking behaviors beyond what was observed over time for those who reviewed an NIAAA pamphlet with study staff. The lack of evidence for the direct effect of CBT for treatment seeking on alcohol use outcomes removed the need for analyses testing whether enhanced treatment accounted for this difference as there was no difference.
Figure. CBT for treatment seeking did not improve drinking outcomes compared to reviewing an NIAAA pamphlet with study staff.
There was evidence to suggest the effects of the intervention varied by sex
In exploratory analyses, more men in the intervention group (22%) initiated alcohol treatment at 3-month follow-up than men in the control (14%), however this difference was not statistically significant. The intervention was less helpful than the control for women, as only 17% of those assigned to the intervention group sought treatment compared to 24% of women assigned to the control, though again the difference was not statistically significant. Within the control condition, more women (24%) than men (13%) sought alcohol treatment. There were no treatment effect differences by age or level of alcohol use disorder severity; that is, CBT for treatment seeking was similar to reviewing an NIAAA pamphlet with someone over the phone irrespective of participant age or score on an alcohol use disorder screener.
While the present study attempted to address this issue of treatment linkage among those with more severe alcohol use disorder, results did not support the intervention as being better than a briefer simpler intervention. Importantly, these findings showing no difference between CBT and an informational pamphlet ran counter to those from an earlier trial with the same two conditions showing CBT improved treatment seeking but it did not assess alcohol use outcomes. The current study conducted March 2019 to December 2021 overlapped with the most impactful months of the COVID-19 pandemic including limitations to in-person treatments and recovery supports. It is possible that the pandemic constrained treatment options, which may dampen any potential positive effects of receiving CBT for treatment seeking. The study, however, did not include analyses examining only participants who entered the study between March 2019 and March 2020 (before the COVID-19 public health emergency) to test such a hypothesis. Also of note, the study did not measure mutual-help group involvement (e.g., AA, or LifeRing, SMART Recovery, etc.) despite substantial evidence that participation in these community-based groups improves outcomes for individuals with alcohol use disorder. As they are the most commonly attended of all professional and non-professional recovery support options, it is possible that many also attended such organizations.
Given the complexities associated with addressing the large treatment gap among those with severe alcohol use disorder, there is a need to continue conducting research aiming to better understand what formats (e.g., focusing on individual with alcohol use disorder versus family member to help influence their involvement), delivery types (e.g., in-person, telephone, virtual), levels of assertiveness (e.g., scheduling appointments during the referral to treatment component, providing transportation, etc.) and levels of intensity/dosages (number and pacing of sessions, duration of sessions) of SBIRT interventions are most effective for encouraging treatment uptake among this population.
Recruitment took place solely via paid social media ads in a specific region of upstate New York, potentially affecting the generalizability of the results.
The COVID-19 pandemic and associated social distancing restrictions occurred mid-way through study recruitment. This may have had an impact on participants’ treatment seeking and alcohol use behaviors.
Mutual-help group participation was not measured despite the fact that such groups (e.g., AA) are associated with strong effects on increasing alcohol use disorder remission and are the most commonly attended services among professional and non-professional recovery support options.
BOTTOM LINE
CBT for treatment seeking – a one-session CBT-based telephone intervention to address negative beliefs about alcohol use disorder treatment – was not better than a briefer and simpler intervention involving reviewing a standard alcohol pamphlet via phone for promoting treatment use and reducing alcohol use. Continued efforts to improve upon the referral to treatment component of SBIRT interventions for individuals with severe alcohol use disorder are needed to increase treatment engagement and improve outcomes. These efforts may benefit from including more active and personalized interventions to address treatment-seeking barriers.
For individuals and families seeking recovery: For individuals struggling with severe alcohol use disorder and their families, a one-session CBT-focused telephone session, while helpful for some, might not be enough to change beliefs about barriers to seeking alcohol treatment and encourage treatment initiation for most. Encouraging ongoing discussions about alcohol use and various alcohol treatments in a variety of settings (e.g., with a trusted healthcare provider) could help to encourage changes in beliefs over time. For families, empirically-supported interventions like the Community Reinforcement and Family Training approach that teach concerned significant others skills to make treatment seeking more likely may be useful.
For treatment professionals and treatment systems: Given the finding that a single-session telephone-delivered CBT for treatment seeking intervention did not increase treatment seeking among individuals with severe alcohol use disorder, there is a need to continue to explore strategies to encourage engagement with evidence-based treatments and to address common barriers to treatment seeking. Such efforts may benefit from being personalized to each individual, addressing logistical barriers like transportation, and involving family members to develop skills that help facilitate their loved one’s entry into treatment.
For scientists: Findings from this phase-II randomized control trial did not support the superiority of a CBT-based, telephone-delivered, single session intervention for increasing treatment seeking and reducing alcohol use among individuals with severe alcohol use disorder when compared to a simpler briefer telephone based review of an NIAAA pamphlet. Findings underscore the importance of continued research addressing the linkage to treatment component of screening, brief intervention, and referral to treatment (SBIRT) interventions for those with more severe alcohol use behaviors. Exploring additional intervention modalities – such as implementing technology-based screening interventions in medical care settings – as well as pairing SBIRT with Community Reinforcement and Family training for increasing alcohol use disorder treatment engagement is warranted. More research is needed to better understand what formats, delivery type (e.g., in-person, telephone, virtual), and dosages (number of sessions, duration of sessions) of SBIRT interventions are most effective for encouraging treatment uptake among those with severe alcohol use disorder and for whom (based on varying sociodemographic backgrounds, barriers to treatment, etc.).
For policy makers: Screening, brief intervention, and referral to treatment (SBIRT) interventions for alcohol use disorder delivered over the phone offer expansive reach and could produce immense public health benefits; however, this study highlights the challenges of encouraging treatment engagement among those with more severe alcohol use disorder using brief interventions. There is a need for continued funding to support ongoing research seeking to better understand and address the barriers to seeking evidence-based treatment among this population, including SBIRT interventions in a variety of formats and settings, in order to maximize public health benefits of existing evidence-based alcohol use disorder treatments.
The authors of the present study previously developed Cognitive Behavioral Therapy (CBT) for Treatment Seeking as a single session (45-60 minute), telephone-delivered intervention designed to promote the use of alcohol treatment among individuals with severe alcohol use disorder. Previous findings indicate that in a sample of individuals with alcohol use disorder who had not been to treatment (i.e., “treatment naïve”), those receiving this CBT adaptation were more than twice as likely to seek alcohol treatment than those in the control who listened to information from a pamphlet about alcohol use disorder treatment. The present study built on prior work by testing CBT for treatment seeking in a randomized controlled trial.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial comparing CBT for treatment seeking to an NIAAA pamphlet on alcohol use disorder treatment. Eligibility criteria for inclusion in the study were as follows: 1) 18 years of age or older; 2) score >16 on the Alcohol Use Disorders Identification Test; 3) exceeding recommended limits for low-risk drinking within the past 30 days (≥4 standard drinks on any occasion or >7 drinks per week [women]; ≥5 drinks on any occasion or >14 drinks per week [men]). Participants were excluded if they lacked English proficiency, were currently experiencing alcohol withdrawal necessitating medical evaluation, or if they had any prior history of professional alcohol-related treatment (does not include mutual help organization attendance, such as Alcoholics Anonymous). Participants were equally male and female, primarily White (79%), and an average age of 40 years. A total of 400 participants were randomized to either the CBT for treatment seeking intervention (n=197) or control (n=203) condition which consisted of reviewing an NIAAA pamphlet on alcohol use disorder treatment.
CBT for treatment seeking is a brief, structured, telephone-based, single session intervention lasting between 45 to 60 minutes. The underlying aim of CBT for treatment seeking is to change beliefs related to a person’s decision to seek alcohol treatment. The session involves four consecutive stages: 1) discussing alcohol consumption, 2) discussing strategies used to manage drinking (if any), 3) eliciting beliefs about alcohol treatment, and 4) discussing each belief in detail. The interventionist is tasked with seeking to modify each belief with the participant. Though the structure of the intervention remains consistent, the content discussed within each session is tailored to respond to the participant’s beliefs. Local treatment resources and different treatment options were also discussed upon request. The control group received an NIAAA pamphlet presenting information on alcohol use disorder symptoms and evidence-based treatment options, which was reviewed during a 10–15-minute phone call with a study staff member.
Assessments were conducted at baseline, and 1-, 3-, and 6-months post-randomization. The primary outcome assessed was any recorded professional alcohol use disorder treatment use over 3-month follow-up, including any of the following 11 sources: (1) family or social services agency; (2) alcohol or drug detoxification ward or clinic; (3) inpatient ward of a general hospital, community mental health program or inpatient psychiatric hospital; (4) outpatient program including day or partial hospital treatment; (5) alcohol or drug rehabilitation program; (6) emergency room or urgent care facility; (7) halfway house or therapeutic community; (8) crisis center; (9) employee assistance program; (10) member of the clergy including a priest, rabbi or any type of religious counselor; and (11) private provider including primary care physician, psychologist, psychiatrist, social worker, nurse or another professional counselor (Alcohol Use Disorders Identification and Associated Disabilities Interview). Secondary outcomes related to past 30-day alcohol consumption at 6-month follow-up accounted for alcohol intensity (i.e., average number of standard drinks per day of drinking in the past 30 days) and alcohol frequency (i.e., number of days of drinking in the past 30 days; Timeline Follow Back Interview).
The primary hypothesis was that individuals who received the CBT for treatment seeking intervention would be more likely to attend one or more alcohol use disorder treatment sessions by 3-month follow-up, compared to controls who reviewed a pamphlet on treatment with study staff. Those with missing treatment initiation data were assumed not to have sought treatment, a rigorous approach to handling missing outcome data and providing a more stringent test of whether the single session CBT intervention enhanced treatment engagement as designed. The secondary hypothesis was that compared to those assigned to the control group, individuals in the intervention group would experience greater reductions in alcohol use at 6-month follow-up. The authors also hypothesized that reductions in alcohol consumption experienced by the intervention group would be explained by increases in alcohol treatment engagement.
WHAT DID THIS STUDY FIND?
The intervention did not improve outcomes
The primary hypothesis suggesting that CBT for treatment seeking would increase treatment initiation during 3-month follow-up was not supported. There were no significant differences in treatment uptake between intervention (19%) and control (18%) conditions. As shown in the figure below, treatment attendance in the first month, as well as the second and third months, were similar for both groups.
Figure. CBT for treatment seeking did not improve treatment attendance compared to reviewing an NIAAA pamphlet with study staff.
The secondary hypothesis that participants in the intervention condition would experience greater reductions in alcohol use relative to the control at 6-month follow-up was not supported. There were no observed differences between the two groups on alcohol use intensity or frequency at any time point. When combining the results from the two arms, there were linear reductions in past month number of drinks per occasion (from 6.0 drinks per day at 1-month follow-up to 4.4 drinks per day at 6-months) and past month number of drinking days (from 18.2 days at 1-month follow-up to 13.7 days at 6-month follow-up). However, there was no interaction between time and condition, meaning the intervention did not impact changes in drinking behaviors beyond what was observed over time for those who reviewed an NIAAA pamphlet with study staff. The lack of evidence for the direct effect of CBT for treatment seeking on alcohol use outcomes removed the need for analyses testing whether enhanced treatment accounted for this difference as there was no difference.
Figure. CBT for treatment seeking did not improve drinking outcomes compared to reviewing an NIAAA pamphlet with study staff.
There was evidence to suggest the effects of the intervention varied by sex
In exploratory analyses, more men in the intervention group (22%) initiated alcohol treatment at 3-month follow-up than men in the control (14%), however this difference was not statistically significant. The intervention was less helpful than the control for women, as only 17% of those assigned to the intervention group sought treatment compared to 24% of women assigned to the control, though again the difference was not statistically significant. Within the control condition, more women (24%) than men (13%) sought alcohol treatment. There were no treatment effect differences by age or level of alcohol use disorder severity; that is, CBT for treatment seeking was similar to reviewing an NIAAA pamphlet with someone over the phone irrespective of participant age or score on an alcohol use disorder screener.
While the present study attempted to address this issue of treatment linkage among those with more severe alcohol use disorder, results did not support the intervention as being better than a briefer simpler intervention. Importantly, these findings showing no difference between CBT and an informational pamphlet ran counter to those from an earlier trial with the same two conditions showing CBT improved treatment seeking but it did not assess alcohol use outcomes. The current study conducted March 2019 to December 2021 overlapped with the most impactful months of the COVID-19 pandemic including limitations to in-person treatments and recovery supports. It is possible that the pandemic constrained treatment options, which may dampen any potential positive effects of receiving CBT for treatment seeking. The study, however, did not include analyses examining only participants who entered the study between March 2019 and March 2020 (before the COVID-19 public health emergency) to test such a hypothesis. Also of note, the study did not measure mutual-help group involvement (e.g., AA, or LifeRing, SMART Recovery, etc.) despite substantial evidence that participation in these community-based groups improves outcomes for individuals with alcohol use disorder. As they are the most commonly attended of all professional and non-professional recovery support options, it is possible that many also attended such organizations.
Given the complexities associated with addressing the large treatment gap among those with severe alcohol use disorder, there is a need to continue conducting research aiming to better understand what formats (e.g., focusing on individual with alcohol use disorder versus family member to help influence their involvement), delivery types (e.g., in-person, telephone, virtual), levels of assertiveness (e.g., scheduling appointments during the referral to treatment component, providing transportation, etc.) and levels of intensity/dosages (number and pacing of sessions, duration of sessions) of SBIRT interventions are most effective for encouraging treatment uptake among this population.
Recruitment took place solely via paid social media ads in a specific region of upstate New York, potentially affecting the generalizability of the results.
The COVID-19 pandemic and associated social distancing restrictions occurred mid-way through study recruitment. This may have had an impact on participants’ treatment seeking and alcohol use behaviors.
Mutual-help group participation was not measured despite the fact that such groups (e.g., AA) are associated with strong effects on increasing alcohol use disorder remission and are the most commonly attended services among professional and non-professional recovery support options.
BOTTOM LINE
CBT for treatment seeking – a one-session CBT-based telephone intervention to address negative beliefs about alcohol use disorder treatment – was not better than a briefer and simpler intervention involving reviewing a standard alcohol pamphlet via phone for promoting treatment use and reducing alcohol use. Continued efforts to improve upon the referral to treatment component of SBIRT interventions for individuals with severe alcohol use disorder are needed to increase treatment engagement and improve outcomes. These efforts may benefit from including more active and personalized interventions to address treatment-seeking barriers.
For individuals and families seeking recovery: For individuals struggling with severe alcohol use disorder and their families, a one-session CBT-focused telephone session, while helpful for some, might not be enough to change beliefs about barriers to seeking alcohol treatment and encourage treatment initiation for most. Encouraging ongoing discussions about alcohol use and various alcohol treatments in a variety of settings (e.g., with a trusted healthcare provider) could help to encourage changes in beliefs over time. For families, empirically-supported interventions like the Community Reinforcement and Family Training approach that teach concerned significant others skills to make treatment seeking more likely may be useful.
For treatment professionals and treatment systems: Given the finding that a single-session telephone-delivered CBT for treatment seeking intervention did not increase treatment seeking among individuals with severe alcohol use disorder, there is a need to continue to explore strategies to encourage engagement with evidence-based treatments and to address common barriers to treatment seeking. Such efforts may benefit from being personalized to each individual, addressing logistical barriers like transportation, and involving family members to develop skills that help facilitate their loved one’s entry into treatment.
For scientists: Findings from this phase-II randomized control trial did not support the superiority of a CBT-based, telephone-delivered, single session intervention for increasing treatment seeking and reducing alcohol use among individuals with severe alcohol use disorder when compared to a simpler briefer telephone based review of an NIAAA pamphlet. Findings underscore the importance of continued research addressing the linkage to treatment component of screening, brief intervention, and referral to treatment (SBIRT) interventions for those with more severe alcohol use behaviors. Exploring additional intervention modalities – such as implementing technology-based screening interventions in medical care settings – as well as pairing SBIRT with Community Reinforcement and Family training for increasing alcohol use disorder treatment engagement is warranted. More research is needed to better understand what formats, delivery type (e.g., in-person, telephone, virtual), and dosages (number of sessions, duration of sessions) of SBIRT interventions are most effective for encouraging treatment uptake among those with severe alcohol use disorder and for whom (based on varying sociodemographic backgrounds, barriers to treatment, etc.).
For policy makers: Screening, brief intervention, and referral to treatment (SBIRT) interventions for alcohol use disorder delivered over the phone offer expansive reach and could produce immense public health benefits; however, this study highlights the challenges of encouraging treatment engagement among those with more severe alcohol use disorder using brief interventions. There is a need for continued funding to support ongoing research seeking to better understand and address the barriers to seeking evidence-based treatment among this population, including SBIRT interventions in a variety of formats and settings, in order to maximize public health benefits of existing evidence-based alcohol use disorder treatments.
The authors of the present study previously developed Cognitive Behavioral Therapy (CBT) for Treatment Seeking as a single session (45-60 minute), telephone-delivered intervention designed to promote the use of alcohol treatment among individuals with severe alcohol use disorder. Previous findings indicate that in a sample of individuals with alcohol use disorder who had not been to treatment (i.e., “treatment naïve”), those receiving this CBT adaptation were more than twice as likely to seek alcohol treatment than those in the control who listened to information from a pamphlet about alcohol use disorder treatment. The present study built on prior work by testing CBT for treatment seeking in a randomized controlled trial.
HOW WAS THIS STUDY CONDUCTED?
This was a randomized controlled trial comparing CBT for treatment seeking to an NIAAA pamphlet on alcohol use disorder treatment. Eligibility criteria for inclusion in the study were as follows: 1) 18 years of age or older; 2) score >16 on the Alcohol Use Disorders Identification Test; 3) exceeding recommended limits for low-risk drinking within the past 30 days (≥4 standard drinks on any occasion or >7 drinks per week [women]; ≥5 drinks on any occasion or >14 drinks per week [men]). Participants were excluded if they lacked English proficiency, were currently experiencing alcohol withdrawal necessitating medical evaluation, or if they had any prior history of professional alcohol-related treatment (does not include mutual help organization attendance, such as Alcoholics Anonymous). Participants were equally male and female, primarily White (79%), and an average age of 40 years. A total of 400 participants were randomized to either the CBT for treatment seeking intervention (n=197) or control (n=203) condition which consisted of reviewing an NIAAA pamphlet on alcohol use disorder treatment.
CBT for treatment seeking is a brief, structured, telephone-based, single session intervention lasting between 45 to 60 minutes. The underlying aim of CBT for treatment seeking is to change beliefs related to a person’s decision to seek alcohol treatment. The session involves four consecutive stages: 1) discussing alcohol consumption, 2) discussing strategies used to manage drinking (if any), 3) eliciting beliefs about alcohol treatment, and 4) discussing each belief in detail. The interventionist is tasked with seeking to modify each belief with the participant. Though the structure of the intervention remains consistent, the content discussed within each session is tailored to respond to the participant’s beliefs. Local treatment resources and different treatment options were also discussed upon request. The control group received an NIAAA pamphlet presenting information on alcohol use disorder symptoms and evidence-based treatment options, which was reviewed during a 10–15-minute phone call with a study staff member.
Assessments were conducted at baseline, and 1-, 3-, and 6-months post-randomization. The primary outcome assessed was any recorded professional alcohol use disorder treatment use over 3-month follow-up, including any of the following 11 sources: (1) family or social services agency; (2) alcohol or drug detoxification ward or clinic; (3) inpatient ward of a general hospital, community mental health program or inpatient psychiatric hospital; (4) outpatient program including day or partial hospital treatment; (5) alcohol or drug rehabilitation program; (6) emergency room or urgent care facility; (7) halfway house or therapeutic community; (8) crisis center; (9) employee assistance program; (10) member of the clergy including a priest, rabbi or any type of religious counselor; and (11) private provider including primary care physician, psychologist, psychiatrist, social worker, nurse or another professional counselor (Alcohol Use Disorders Identification and Associated Disabilities Interview). Secondary outcomes related to past 30-day alcohol consumption at 6-month follow-up accounted for alcohol intensity (i.e., average number of standard drinks per day of drinking in the past 30 days) and alcohol frequency (i.e., number of days of drinking in the past 30 days; Timeline Follow Back Interview).
The primary hypothesis was that individuals who received the CBT for treatment seeking intervention would be more likely to attend one or more alcohol use disorder treatment sessions by 3-month follow-up, compared to controls who reviewed a pamphlet on treatment with study staff. Those with missing treatment initiation data were assumed not to have sought treatment, a rigorous approach to handling missing outcome data and providing a more stringent test of whether the single session CBT intervention enhanced treatment engagement as designed. The secondary hypothesis was that compared to those assigned to the control group, individuals in the intervention group would experience greater reductions in alcohol use at 6-month follow-up. The authors also hypothesized that reductions in alcohol consumption experienced by the intervention group would be explained by increases in alcohol treatment engagement.
WHAT DID THIS STUDY FIND?
The intervention did not improve outcomes
The primary hypothesis suggesting that CBT for treatment seeking would increase treatment initiation during 3-month follow-up was not supported. There were no significant differences in treatment uptake between intervention (19%) and control (18%) conditions. As shown in the figure below, treatment attendance in the first month, as well as the second and third months, were similar for both groups.
Figure. CBT for treatment seeking did not improve treatment attendance compared to reviewing an NIAAA pamphlet with study staff.
The secondary hypothesis that participants in the intervention condition would experience greater reductions in alcohol use relative to the control at 6-month follow-up was not supported. There were no observed differences between the two groups on alcohol use intensity or frequency at any time point. When combining the results from the two arms, there were linear reductions in past month number of drinks per occasion (from 6.0 drinks per day at 1-month follow-up to 4.4 drinks per day at 6-months) and past month number of drinking days (from 18.2 days at 1-month follow-up to 13.7 days at 6-month follow-up). However, there was no interaction between time and condition, meaning the intervention did not impact changes in drinking behaviors beyond what was observed over time for those who reviewed an NIAAA pamphlet with study staff. The lack of evidence for the direct effect of CBT for treatment seeking on alcohol use outcomes removed the need for analyses testing whether enhanced treatment accounted for this difference as there was no difference.
Figure. CBT for treatment seeking did not improve drinking outcomes compared to reviewing an NIAAA pamphlet with study staff.
There was evidence to suggest the effects of the intervention varied by sex
In exploratory analyses, more men in the intervention group (22%) initiated alcohol treatment at 3-month follow-up than men in the control (14%), however this difference was not statistically significant. The intervention was less helpful than the control for women, as only 17% of those assigned to the intervention group sought treatment compared to 24% of women assigned to the control, though again the difference was not statistically significant. Within the control condition, more women (24%) than men (13%) sought alcohol treatment. There were no treatment effect differences by age or level of alcohol use disorder severity; that is, CBT for treatment seeking was similar to reviewing an NIAAA pamphlet with someone over the phone irrespective of participant age or score on an alcohol use disorder screener.
While the present study attempted to address this issue of treatment linkage among those with more severe alcohol use disorder, results did not support the intervention as being better than a briefer simpler intervention. Importantly, these findings showing no difference between CBT and an informational pamphlet ran counter to those from an earlier trial with the same two conditions showing CBT improved treatment seeking but it did not assess alcohol use outcomes. The current study conducted March 2019 to December 2021 overlapped with the most impactful months of the COVID-19 pandemic including limitations to in-person treatments and recovery supports. It is possible that the pandemic constrained treatment options, which may dampen any potential positive effects of receiving CBT for treatment seeking. The study, however, did not include analyses examining only participants who entered the study between March 2019 and March 2020 (before the COVID-19 public health emergency) to test such a hypothesis. Also of note, the study did not measure mutual-help group involvement (e.g., AA, or LifeRing, SMART Recovery, etc.) despite substantial evidence that participation in these community-based groups improves outcomes for individuals with alcohol use disorder. As they are the most commonly attended of all professional and non-professional recovery support options, it is possible that many also attended such organizations.
Given the complexities associated with addressing the large treatment gap among those with severe alcohol use disorder, there is a need to continue conducting research aiming to better understand what formats (e.g., focusing on individual with alcohol use disorder versus family member to help influence their involvement), delivery types (e.g., in-person, telephone, virtual), levels of assertiveness (e.g., scheduling appointments during the referral to treatment component, providing transportation, etc.) and levels of intensity/dosages (number and pacing of sessions, duration of sessions) of SBIRT interventions are most effective for encouraging treatment uptake among this population.
Recruitment took place solely via paid social media ads in a specific region of upstate New York, potentially affecting the generalizability of the results.
The COVID-19 pandemic and associated social distancing restrictions occurred mid-way through study recruitment. This may have had an impact on participants’ treatment seeking and alcohol use behaviors.
Mutual-help group participation was not measured despite the fact that such groups (e.g., AA) are associated with strong effects on increasing alcohol use disorder remission and are the most commonly attended services among professional and non-professional recovery support options.
BOTTOM LINE
CBT for treatment seeking – a one-session CBT-based telephone intervention to address negative beliefs about alcohol use disorder treatment – was not better than a briefer and simpler intervention involving reviewing a standard alcohol pamphlet via phone for promoting treatment use and reducing alcohol use. Continued efforts to improve upon the referral to treatment component of SBIRT interventions for individuals with severe alcohol use disorder are needed to increase treatment engagement and improve outcomes. These efforts may benefit from including more active and personalized interventions to address treatment-seeking barriers.
For individuals and families seeking recovery: For individuals struggling with severe alcohol use disorder and their families, a one-session CBT-focused telephone session, while helpful for some, might not be enough to change beliefs about barriers to seeking alcohol treatment and encourage treatment initiation for most. Encouraging ongoing discussions about alcohol use and various alcohol treatments in a variety of settings (e.g., with a trusted healthcare provider) could help to encourage changes in beliefs over time. For families, empirically-supported interventions like the Community Reinforcement and Family Training approach that teach concerned significant others skills to make treatment seeking more likely may be useful.
For treatment professionals and treatment systems: Given the finding that a single-session telephone-delivered CBT for treatment seeking intervention did not increase treatment seeking among individuals with severe alcohol use disorder, there is a need to continue to explore strategies to encourage engagement with evidence-based treatments and to address common barriers to treatment seeking. Such efforts may benefit from being personalized to each individual, addressing logistical barriers like transportation, and involving family members to develop skills that help facilitate their loved one’s entry into treatment.
For scientists: Findings from this phase-II randomized control trial did not support the superiority of a CBT-based, telephone-delivered, single session intervention for increasing treatment seeking and reducing alcohol use among individuals with severe alcohol use disorder when compared to a simpler briefer telephone based review of an NIAAA pamphlet. Findings underscore the importance of continued research addressing the linkage to treatment component of screening, brief intervention, and referral to treatment (SBIRT) interventions for those with more severe alcohol use behaviors. Exploring additional intervention modalities – such as implementing technology-based screening interventions in medical care settings – as well as pairing SBIRT with Community Reinforcement and Family training for increasing alcohol use disorder treatment engagement is warranted. More research is needed to better understand what formats, delivery type (e.g., in-person, telephone, virtual), and dosages (number of sessions, duration of sessions) of SBIRT interventions are most effective for encouraging treatment uptake among those with severe alcohol use disorder and for whom (based on varying sociodemographic backgrounds, barriers to treatment, etc.).
For policy makers: Screening, brief intervention, and referral to treatment (SBIRT) interventions for alcohol use disorder delivered over the phone offer expansive reach and could produce immense public health benefits; however, this study highlights the challenges of encouraging treatment engagement among those with more severe alcohol use disorder using brief interventions. There is a need for continued funding to support ongoing research seeking to better understand and address the barriers to seeking evidence-based treatment among this population, including SBIRT interventions in a variety of formats and settings, in order to maximize public health benefits of existing evidence-based alcohol use disorder treatments.

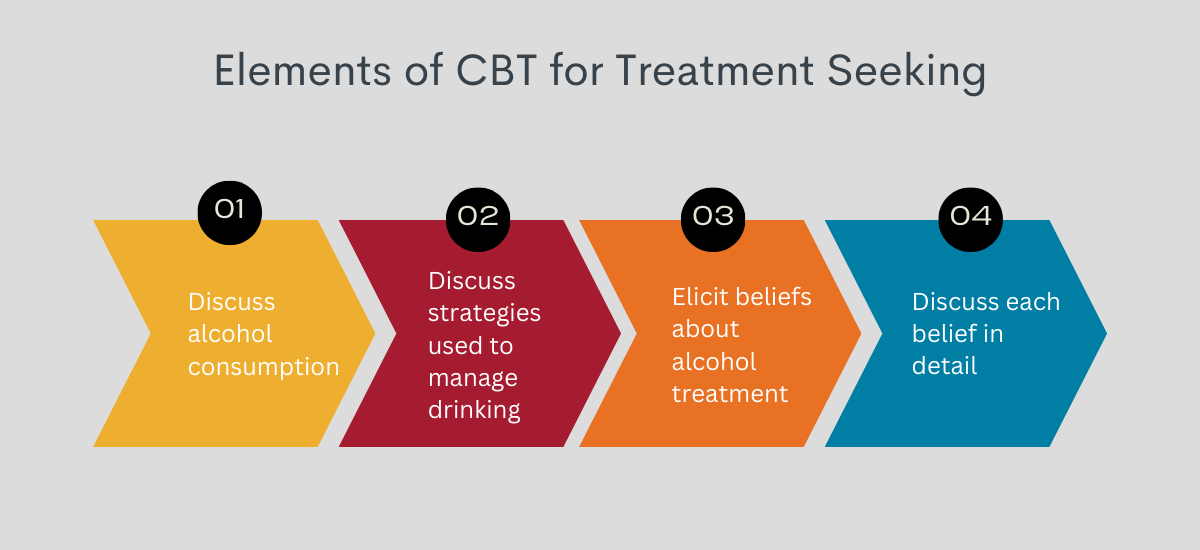
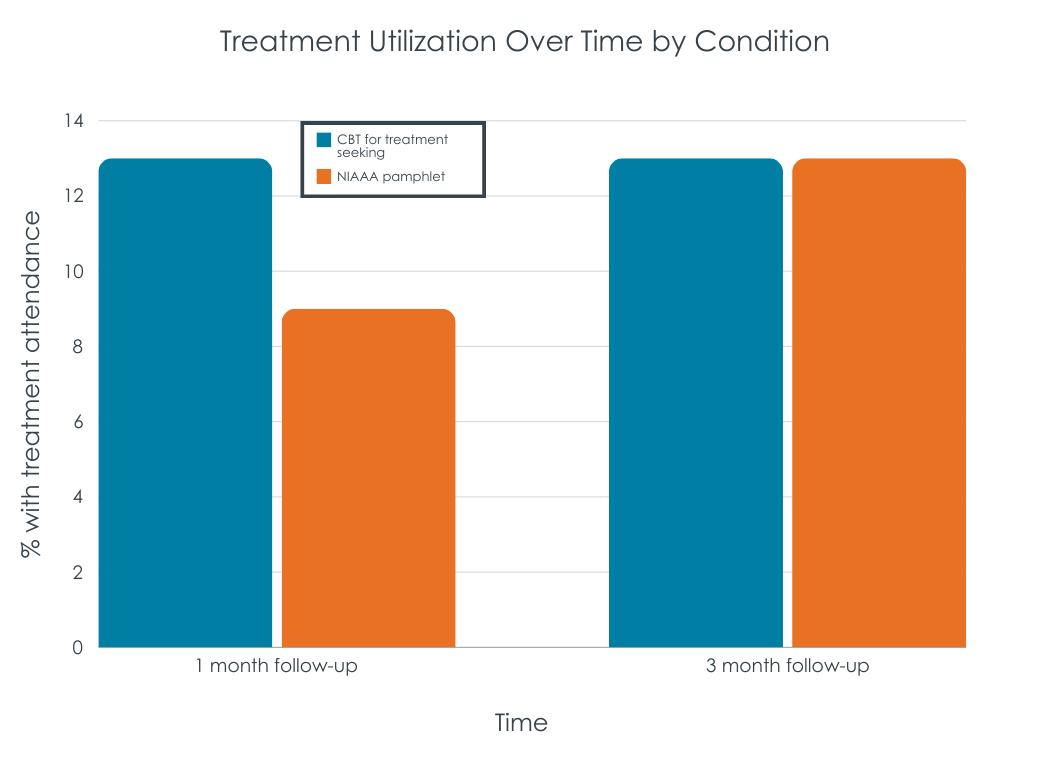 Figure. CBT for treatment seeking did not improve treatment attendance compared to reviewing an NIAAA pamphlet with study staff.
Figure. CBT for treatment seeking did not improve treatment attendance compared to reviewing an NIAAA pamphlet with study staff.