Shared racial identity improves support for public health-based opioid policy
Opioid policies have shifted over time from punitive to treatment-based, which may be due to the identities of the populations affected. This study examined how different identity attributes of a person with substance use disorder influence public opinions of opioid policies and individual blame.
When President Nixon waged the “War on Drugs” in 1971, policy responses to drug use were based primarily on punishment rather than treatment and healthcare. The efforts were then greatly expanded by President Ronald Reagan in 1981, who further strengthened the focus on punishment in response to the “crack epidemic” of the 1980s, leading to mass incarceration that disproportionately affected Black people. For instance, the mandatory sentencing minimums established by the Anti-Drug Abuse Act of 1986 were not applied equally across all drugs – possession of just 5 grams of crack cocaine, for example – users of which were 80% Black people -resulted in a minimum of a 5-year sentence, while possession of 500 grams of powder cocaine resulted in the same minimum sentence. However, policy responses to the current opioid crisis have begun to shift away from such punitive policies towards more treatment-based ones.
One suggested explanation for these changes involves different populations that were affected. The crack epidemic of the 1980s primarily affected non-White people who lived in urban locations. Conversely, the opioid crisis has affected more White people who live in rural locations than has been the case during previous drug crises. This has led to more White and rural people with substance use disorder being depicted in the media. Prior research has shown that linking people from racial minorities with certain policies, such as welfare, may result in opposition of the policy among White people. Accordingly, it is possible that these depictions of more White people with opioid use disorder led to more support for treatment-based policies, and that shared identities may play a role.
People who share identities often form an attachment to each other, sometimes referred to as in-group favoritism, and this influences people’s opinions on social policy issues. If the policy is believed to benefit the in-group, it is more likely to be supported than policies that are believed to benefit the out-group. In this study, the researchers examined how sharing identities with a person with substance use disorder influences public opinion on opioid policies and the degree to which the individual is perceived to be deserving of blame. Such research helps to shed light on how media portrayals of people with substance use disorder affect public opinion, which can influence stigma and policy.
HOW WAS THIS STUDY CONDUCTED?
This study examined how sharing different identity attributes (race, gender, and residential location) with a person with substance use disorder and the initial drug that was used leading to their disorder influences public opinion on opioid policies and individual blame. These identity attributes were experimentally manipulated and randomly chosen to be featured in a fictional news story. Participants were then given a survey that assessed their support for opioid policies and perceptions of the degree to which the person in the news story was blameworthy.
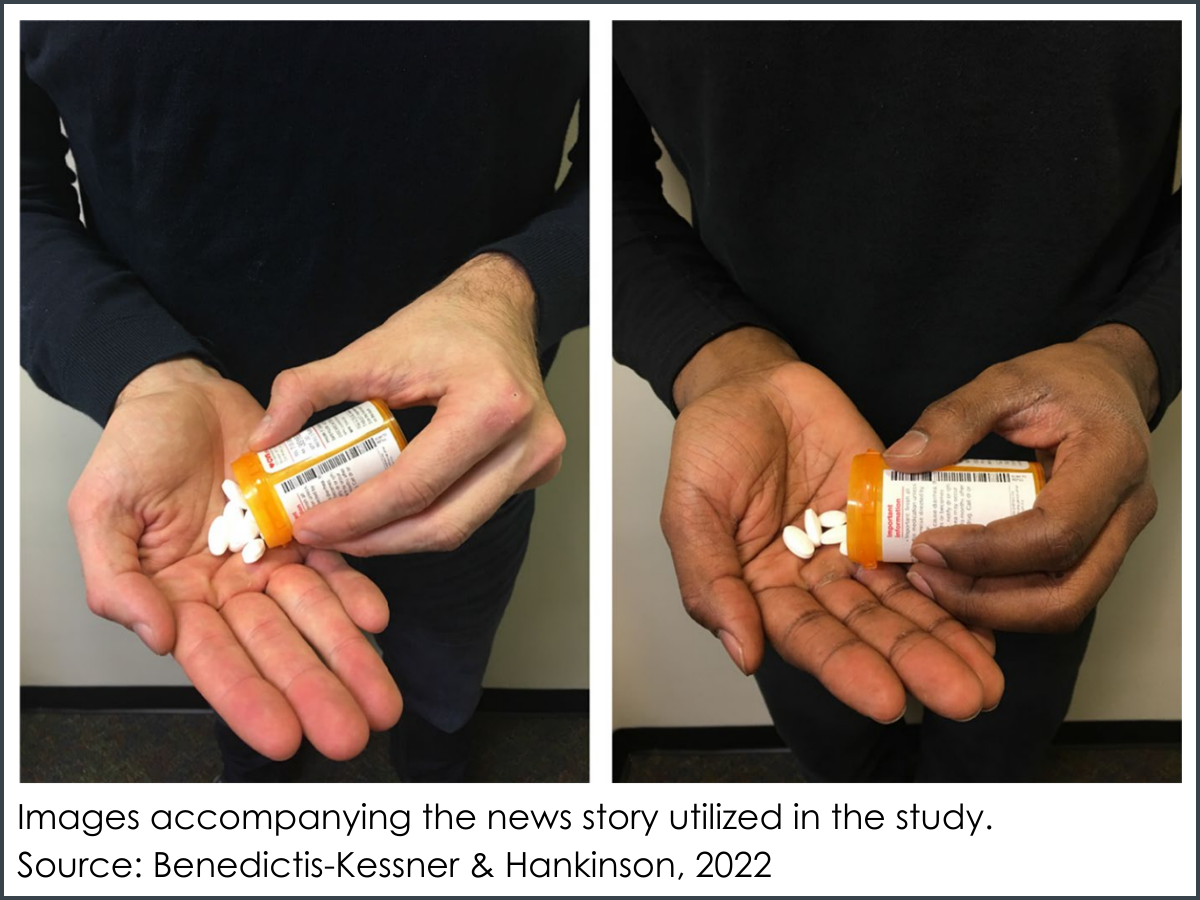
Race was manipulated by showing the hands of either a White or Black person in the story and using different names. Gender was manipulated by using male or female pronouns and names, as well as showing the hands of a man or woman. Variations of residential location that were referenced in the story included an urban downtown center, a quiet suburb, and rural farm. Variations of the initial drug used included heroin, OxyContin for medical use (prescribed by a physician), or non-medical use of OxyContin. These variations were referenced in the story and shown as pictures of either a needle or pills.
The main outcomes of interest included support for opioid treatment spending policy, as measured by the desired degree of change to federal funding for opioid treatment programs, and support for law enforcement spending policy, as measured by the desired degree of change to federal funding for law enforcement to arrest and prosecute people with opioid use disorder. Individual blame was examined as a potential mechanism beyond the main effects of identity and was assessed by the question, “Would you agree or disagree that individuals addicted to opioids are to blame for their own addiction?” The researchers also collected demographic information and zip codes to determine participants’ residential location.
Participants were recruited via NORC’s AmeriSpeak Panel and included a nationally-representative sample of 3,112 adults. The majority of participants were White with an average age of 48 and lived in a suburban location. Approximately half were women.
WHAT DID THIS STUDY FIND?
Race – but not other attributes – affected support for opioid policies.
Among all study participants, there was generally positive support for both the treatment and law enforcement spending policies. However, none of the 3 identity attributes of the person with substance use disorder that was depicted in the news story affected levels of support for either policy. Support levels were overall similar regardless of whether the person depicted was White or Black, a man or woman, and lived in an urban, suburban, or rural residential location.
There were differences, however, based on the match between the race of the study participant and the individual depicted in the news story. When the racial identity of the respondent matched that of the person depicted in the news story, support levels for both the treatment and law enforcement policies were affected.
Among Black study participants, those who received the story about a Black person with substance use disorder were more likely to support the treatment spending policy than when they received the story about a White person. Among White participants, those who received the story about a Black person with substance use disorder were less likely to support the treatment spending policy than when they received the story depicting a White person with substance use disorder.
Black study participants who received the news story about a Black person with substance use disorder were less likely to support the law enforcement spending policy than when they received the story about a White person. Among White study participants, however, there were no differences in support of the law enforcement spending policy between the racial identities of the person depicted in the news story.
There were no differences in support levels for both the treatment and law enforcement spending policies when the study participant was a man and the person depicted in the news story was a man, as well as when the study participant was a woman and person depicted in the news story was a woman. Likewise, there were no differences in support levels for both the treatment and law enforcement spending policies when the participants’ residential location matched that of the person with substance use disorder depicted in the news story.
Pharmaceutical opioids – compared to heroin – reduced blame.
Approximately half of all participants (52%) somewhat or strongly agreed with the statement that those addicted to opioids are to blame for their addiction. This view was associated with a lower likelihood of supporting the treatment spending policy and a higher likelihood of supporting the law enforcement spending policy.
However, when the news story depicted the person with a substance use disorder as initially using OxyContin, participants perceived them as less blameworthy than people who were depicted as initially using heroin. This effect was greater for people whose initial OxyContin use was described as being prescribed by a physician than for people who initially used OxyContin for non-medical purposes.
Aligning race improves policy attitudes only for certain types of opioids.
For those who initially used heroin, perceptions of individual blame were uniformly much higher with shared identity not affecting support for the treatment or law enforcement spending policies.
For those who initially began using opioids through prescribed pills, matching racial identities between the study participant and the person in the news story was associated with an increase in support for the treatment spending policy. Specifically, this meant that when the participant shared the racial identity of the person in the news story, participants had higher levels of support for treatment spending policy. However, matching gender identities had no effect.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study examined the role of shared identities on support for opioid policies and blameworthiness. Results showed that shared racial identities were associated with an increase in support of the treatment spending policy and a decrease in support of the law enforcement spending policy, while shared gender identity and residential location were not associated with support for either policy. Further, perceptions of blame were highest when the person in the news article was depicted as having their opioid use disorder originate from heroin, rather than medical use of OxyContin. Shared racial identity only influenced treatment spending policy support in the latter scenario.
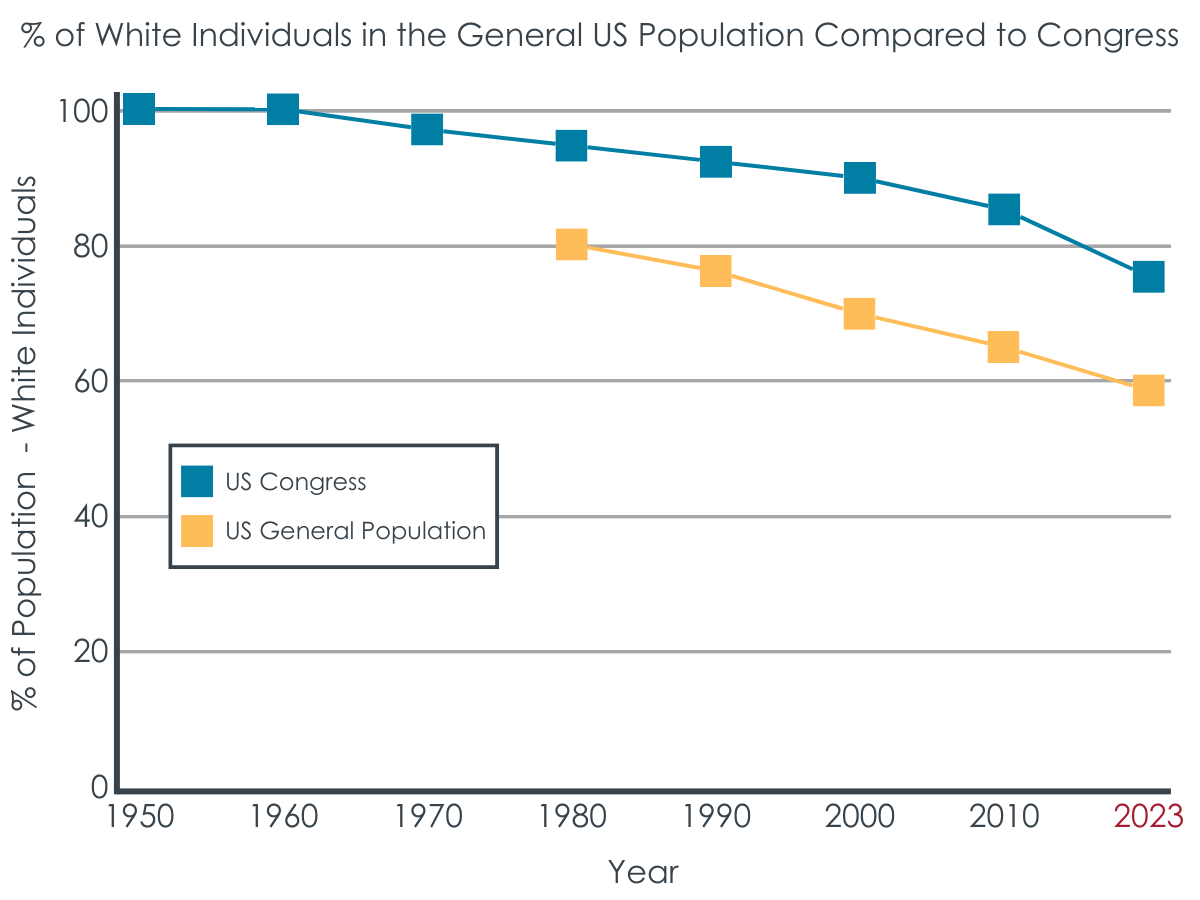
Figure 2 adapted based on original figure from Schaeffer & Pew Research Center, 2023, featuring data from Congressional Research Service, CQ Roll Call, Brookings Institution, Census Bureau population figures.
Notably, the researchers assessed support for the treatment and law enforcement policies and blame by only asking 1 question for each. This is a rather simple way to measure the outcomes and may not comprehensively capture the intended construct (i.e., policy attitudes). Asking more questions that target different dimensions of the constructs could have been a more comprehensive way to measure the constructs of interests, which may have affected the study’s results.
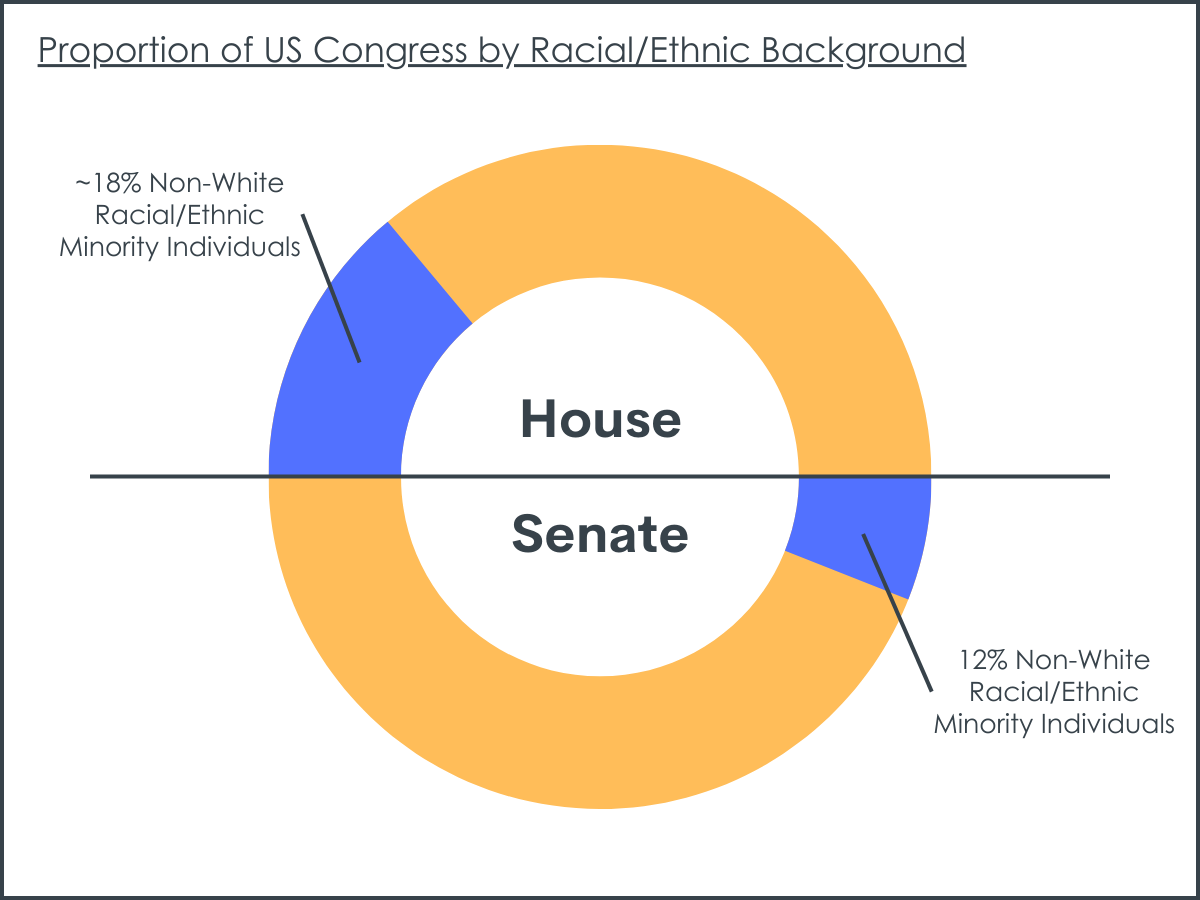
Figure 4 adapted based on original figure from Schaeffer & Pew Research Center, 2023 featuring data from Congressional Research Service, CQ Roll Call, Brookings Institution.
The finding that perceptions of blame were highest when the person in the news article was depicted as having their substance use opioid originate from heroin and lowest when it was depicted as originating from medical use of OxyContin is not surprising – the majority of Americans reported understanding that “accidental” addiction to opioids can happen. This is likely due to the number of opioid use disorders that began with prescription opioids from a physician, which is different from past drug crises. In prior drug crises, people who used drugs were viewed as personally responsible for their actions, whereas in the current crisis it appears that some or all of blame can be put on prescribing physicians and pharmaceutical companies.
At a broader level, the study’s findings are consistent with other research studies that have similarly demonstrated how much media portrayals related to substance use can influence public opinion. Varying socioeconomic status, focusing on violence, and how successful treatment is portrayed may all greatly influence public opinion and stigma. Taken together, this research highlights the importance of how substance use disorders are portrayed in the media.
The researchers measured the outcomes of interest by asking only 1 question for each. This limits how comprehensively they were assessed. Asking several questions for each area of interest may have affected the results by providing a more nuanced and comprehensive assessment of the constructs.
The study’s results may not extend to real-world settings, outside of a research environment where specific variables can be controlled and manipulated, and the attitudes and beliefs examined here may not relate to actual behavior or policy decisions.
Participants were only exposed to the news story once and asked the questions once. Accordingly, the effect of repeated media exposures about people with substance use disorder on support of policies is unclear. It is also unclear whether the results are limited to a certain time period after the exposure or if they extend longer-term.
The research team did not investigate or control for how much participants consumed media regarding the opioid crisis, which may have further increased support of treatment-based policies and reduced perceptions of blame by improving knowledge and understanding.
BOTTOM LINE
Sharing racial identity with someone who has an opioid use disorder is associated with an increase in support of opioid use disorder treatment spending policy and a decrease in support of law enforcement spending policy to arrest and prosecute people with opioid use disorder. Gender and residential setting (urban vs. rural), however, did not impact opioid policy attitudes. These findings support the notion of racial in-group favoritism, which has important implications for how drug policy is created and implemented.
For individuals and families seeking recovery: Individuals may be more likely to support opioid treatment spending policy when they share racial identity with someone with opioid disorder. Individuals also may be more likely to support treatment policy and perceive the person as less blame-worthy when the disorder originates from prescription opioids rather than heroin. If individuals increase their awareness of such biases and seek out opportunities to spend time with people outside of their racial group, stigma may be reduced, and treatment-based policy support may be improved.
For treatment professionals and treatment systems: This study focused on perceptions of the general population but has implications for treatment providers as well. In-group favoritism may be operating outside of awareness. Particularly for therapists who are part of the dominant culture (e.g., White race) treating patients part of non-dominant cultures (e.g., Black race), sustained efforts may be needed to identify and address potential biases in supervision and to understand and empathize with the worldview of the patient.
For scientists: Given that the current study asked only 1 question for each assessed outcome, future research that increases content validity of these outcome domains could provide a more comprehensive understanding of how shared racial identity influences support of treatment-based policies. Further, additional research that examines this potential influence over a longer period of time would shed light on how long the effect of media portrayals lasts. Finally, future research that examines the effects of dosage (i.e., the extent of the exposure to media portrayals, including consumption of media outside of the study) would further improve our understanding of the effects of media portrayals.
For policy makers: Results from this study demonstratedthat individuals are more likely to support opioid treatment spending policy when they share racial identity with someone with opioid disorder, providing support for racial in-group favoritism. Such biases may be overcome, however, by promoting prosocial behaviors, such as empathy, and facilitating integration between different groups, as well as working to understand each other’s viewpoints (i.e., perspective-taking). Accordingly, supporting policies that promote these behaviors may help to reduce in-group bias, thereby benefiting all people rather than only those who have the same race. In addition, including more members of the out-group so that each race is better represented in policymaking contexts would likely result in more equitable policies that benefita larger number of people.
When President Nixon waged the “War on Drugs” in 1971, policy responses to drug use were based primarily on punishment rather than treatment and healthcare. The efforts were then greatly expanded by President Ronald Reagan in 1981, who further strengthened the focus on punishment in response to the “crack epidemic” of the 1980s, leading to mass incarceration that disproportionately affected Black people. For instance, the mandatory sentencing minimums established by the Anti-Drug Abuse Act of 1986 were not applied equally across all drugs – possession of just 5 grams of crack cocaine, for example – users of which were 80% Black people -resulted in a minimum of a 5-year sentence, while possession of 500 grams of powder cocaine resulted in the same minimum sentence. However, policy responses to the current opioid crisis have begun to shift away from such punitive policies towards more treatment-based ones.
One suggested explanation for these changes involves different populations that were affected. The crack epidemic of the 1980s primarily affected non-White people who lived in urban locations. Conversely, the opioid crisis has affected more White people who live in rural locations than has been the case during previous drug crises. This has led to more White and rural people with substance use disorder being depicted in the media. Prior research has shown that linking people from racial minorities with certain policies, such as welfare, may result in opposition of the policy among White people. Accordingly, it is possible that these depictions of more White people with opioid use disorder led to more support for treatment-based policies, and that shared identities may play a role.
People who share identities often form an attachment to each other, sometimes referred to as in-group favoritism, and this influences people’s opinions on social policy issues. If the policy is believed to benefit the in-group, it is more likely to be supported than policies that are believed to benefit the out-group. In this study, the researchers examined how sharing identities with a person with substance use disorder influences public opinion on opioid policies and the degree to which the individual is perceived to be deserving of blame. Such research helps to shed light on how media portrayals of people with substance use disorder affect public opinion, which can influence stigma and policy.
HOW WAS THIS STUDY CONDUCTED?
This study examined how sharing different identity attributes (race, gender, and residential location) with a person with substance use disorder and the initial drug that was used leading to their disorder influences public opinion on opioid policies and individual blame. These identity attributes were experimentally manipulated and randomly chosen to be featured in a fictional news story. Participants were then given a survey that assessed their support for opioid policies and perceptions of the degree to which the person in the news story was blameworthy.
Race was manipulated by showing the hands of either a White or Black person in the story and using different names. Gender was manipulated by using male or female pronouns and names, as well as showing the hands of a man or woman. Variations of residential location that were referenced in the story included an urban downtown center, a quiet suburb, and rural farm. Variations of the initial drug used included heroin, OxyContin for medical use (prescribed by a physician), or non-medical use of OxyContin. These variations were referenced in the story and shown as pictures of either a needle or pills.
The main outcomes of interest included support for opioid treatment spending policy, as measured by the desired degree of change to federal funding for opioid treatment programs, and support for law enforcement spending policy, as measured by the desired degree of change to federal funding for law enforcement to arrest and prosecute people with opioid use disorder. Individual blame was examined as a potential mechanism beyond the main effects of identity and was assessed by the question, “Would you agree or disagree that individuals addicted to opioids are to blame for their own addiction?” The researchers also collected demographic information and zip codes to determine participants’ residential location.
Participants were recruited via NORC’s AmeriSpeak Panel and included a nationally-representative sample of 3,112 adults. The majority of participants were White with an average age of 48 and lived in a suburban location. Approximately half were women.
WHAT DID THIS STUDY FIND?
Race – but not other attributes – affected support for opioid policies.
Among all study participants, there was generally positive support for both the treatment and law enforcement spending policies. However, none of the 3 identity attributes of the person with substance use disorder that was depicted in the news story affected levels of support for either policy. Support levels were overall similar regardless of whether the person depicted was White or Black, a man or woman, and lived in an urban, suburban, or rural residential location.
There were differences, however, based on the match between the race of the study participant and the individual depicted in the news story. When the racial identity of the respondent matched that of the person depicted in the news story, support levels for both the treatment and law enforcement policies were affected.
Among Black study participants, those who received the story about a Black person with substance use disorder were more likely to support the treatment spending policy than when they received the story about a White person. Among White participants, those who received the story about a Black person with substance use disorder were less likely to support the treatment spending policy than when they received the story depicting a White person with substance use disorder.
Black study participants who received the news story about a Black person with substance use disorder were less likely to support the law enforcement spending policy than when they received the story about a White person. Among White study participants, however, there were no differences in support of the law enforcement spending policy between the racial identities of the person depicted in the news story.
There were no differences in support levels for both the treatment and law enforcement spending policies when the study participant was a man and the person depicted in the news story was a man, as well as when the study participant was a woman and person depicted in the news story was a woman. Likewise, there were no differences in support levels for both the treatment and law enforcement spending policies when the participants’ residential location matched that of the person with substance use disorder depicted in the news story.
Pharmaceutical opioids – compared to heroin – reduced blame.
Approximately half of all participants (52%) somewhat or strongly agreed with the statement that those addicted to opioids are to blame for their addiction. This view was associated with a lower likelihood of supporting the treatment spending policy and a higher likelihood of supporting the law enforcement spending policy.
However, when the news story depicted the person with a substance use disorder as initially using OxyContin, participants perceived them as less blameworthy than people who were depicted as initially using heroin. This effect was greater for people whose initial OxyContin use was described as being prescribed by a physician than for people who initially used OxyContin for non-medical purposes.
Aligning race improves policy attitudes only for certain types of opioids.
For those who initially used heroin, perceptions of individual blame were uniformly much higher with shared identity not affecting support for the treatment or law enforcement spending policies.
For those who initially began using opioids through prescribed pills, matching racial identities between the study participant and the person in the news story was associated with an increase in support for the treatment spending policy. Specifically, this meant that when the participant shared the racial identity of the person in the news story, participants had higher levels of support for treatment spending policy. However, matching gender identities had no effect.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study examined the role of shared identities on support for opioid policies and blameworthiness. Results showed that shared racial identities were associated with an increase in support of the treatment spending policy and a decrease in support of the law enforcement spending policy, while shared gender identity and residential location were not associated with support for either policy. Further, perceptions of blame were highest when the person in the news article was depicted as having their opioid use disorder originate from heroin, rather than medical use of OxyContin. Shared racial identity only influenced treatment spending policy support in the latter scenario.
Figure 2 adapted based on original figure from Schaeffer & Pew Research Center, 2023, featuring data from Congressional Research Service, CQ Roll Call, Brookings Institution, Census Bureau population figures.
Notably, the researchers assessed support for the treatment and law enforcement policies and blame by only asking 1 question for each. This is a rather simple way to measure the outcomes and may not comprehensively capture the intended construct (i.e., policy attitudes). Asking more questions that target different dimensions of the constructs could have been a more comprehensive way to measure the constructs of interests, which may have affected the study’s results.
Figure 4 adapted based on original figure from Schaeffer & Pew Research Center, 2023 featuring data from Congressional Research Service, CQ Roll Call, Brookings Institution.
The finding that perceptions of blame were highest when the person in the news article was depicted as having their substance use opioid originate from heroin and lowest when it was depicted as originating from medical use of OxyContin is not surprising – the majority of Americans reported understanding that “accidental” addiction to opioids can happen. This is likely due to the number of opioid use disorders that began with prescription opioids from a physician, which is different from past drug crises. In prior drug crises, people who used drugs were viewed as personally responsible for their actions, whereas in the current crisis it appears that some or all of blame can be put on prescribing physicians and pharmaceutical companies.
At a broader level, the study’s findings are consistent with other research studies that have similarly demonstrated how much media portrayals related to substance use can influence public opinion. Varying socioeconomic status, focusing on violence, and how successful treatment is portrayed may all greatly influence public opinion and stigma. Taken together, this research highlights the importance of how substance use disorders are portrayed in the media.
The researchers measured the outcomes of interest by asking only 1 question for each. This limits how comprehensively they were assessed. Asking several questions for each area of interest may have affected the results by providing a more nuanced and comprehensive assessment of the constructs.
The study’s results may not extend to real-world settings, outside of a research environment where specific variables can be controlled and manipulated, and the attitudes and beliefs examined here may not relate to actual behavior or policy decisions.
Participants were only exposed to the news story once and asked the questions once. Accordingly, the effect of repeated media exposures about people with substance use disorder on support of policies is unclear. It is also unclear whether the results are limited to a certain time period after the exposure or if they extend longer-term.
The research team did not investigate or control for how much participants consumed media regarding the opioid crisis, which may have further increased support of treatment-based policies and reduced perceptions of blame by improving knowledge and understanding.
BOTTOM LINE
Sharing racial identity with someone who has an opioid use disorder is associated with an increase in support of opioid use disorder treatment spending policy and a decrease in support of law enforcement spending policy to arrest and prosecute people with opioid use disorder. Gender and residential setting (urban vs. rural), however, did not impact opioid policy attitudes. These findings support the notion of racial in-group favoritism, which has important implications for how drug policy is created and implemented.
For individuals and families seeking recovery: Individuals may be more likely to support opioid treatment spending policy when they share racial identity with someone with opioid disorder. Individuals also may be more likely to support treatment policy and perceive the person as less blame-worthy when the disorder originates from prescription opioids rather than heroin. If individuals increase their awareness of such biases and seek out opportunities to spend time with people outside of their racial group, stigma may be reduced, and treatment-based policy support may be improved.
For treatment professionals and treatment systems: This study focused on perceptions of the general population but has implications for treatment providers as well. In-group favoritism may be operating outside of awareness. Particularly for therapists who are part of the dominant culture (e.g., White race) treating patients part of non-dominant cultures (e.g., Black race), sustained efforts may be needed to identify and address potential biases in supervision and to understand and empathize with the worldview of the patient.
For scientists: Given that the current study asked only 1 question for each assessed outcome, future research that increases content validity of these outcome domains could provide a more comprehensive understanding of how shared racial identity influences support of treatment-based policies. Further, additional research that examines this potential influence over a longer period of time would shed light on how long the effect of media portrayals lasts. Finally, future research that examines the effects of dosage (i.e., the extent of the exposure to media portrayals, including consumption of media outside of the study) would further improve our understanding of the effects of media portrayals.
For policy makers: Results from this study demonstratedthat individuals are more likely to support opioid treatment spending policy when they share racial identity with someone with opioid disorder, providing support for racial in-group favoritism. Such biases may be overcome, however, by promoting prosocial behaviors, such as empathy, and facilitating integration between different groups, as well as working to understand each other’s viewpoints (i.e., perspective-taking). Accordingly, supporting policies that promote these behaviors may help to reduce in-group bias, thereby benefiting all people rather than only those who have the same race. In addition, including more members of the out-group so that each race is better represented in policymaking contexts would likely result in more equitable policies that benefita larger number of people.
When President Nixon waged the “War on Drugs” in 1971, policy responses to drug use were based primarily on punishment rather than treatment and healthcare. The efforts were then greatly expanded by President Ronald Reagan in 1981, who further strengthened the focus on punishment in response to the “crack epidemic” of the 1980s, leading to mass incarceration that disproportionately affected Black people. For instance, the mandatory sentencing minimums established by the Anti-Drug Abuse Act of 1986 were not applied equally across all drugs – possession of just 5 grams of crack cocaine, for example – users of which were 80% Black people -resulted in a minimum of a 5-year sentence, while possession of 500 grams of powder cocaine resulted in the same minimum sentence. However, policy responses to the current opioid crisis have begun to shift away from such punitive policies towards more treatment-based ones.
One suggested explanation for these changes involves different populations that were affected. The crack epidemic of the 1980s primarily affected non-White people who lived in urban locations. Conversely, the opioid crisis has affected more White people who live in rural locations than has been the case during previous drug crises. This has led to more White and rural people with substance use disorder being depicted in the media. Prior research has shown that linking people from racial minorities with certain policies, such as welfare, may result in opposition of the policy among White people. Accordingly, it is possible that these depictions of more White people with opioid use disorder led to more support for treatment-based policies, and that shared identities may play a role.
People who share identities often form an attachment to each other, sometimes referred to as in-group favoritism, and this influences people’s opinions on social policy issues. If the policy is believed to benefit the in-group, it is more likely to be supported than policies that are believed to benefit the out-group. In this study, the researchers examined how sharing identities with a person with substance use disorder influences public opinion on opioid policies and the degree to which the individual is perceived to be deserving of blame. Such research helps to shed light on how media portrayals of people with substance use disorder affect public opinion, which can influence stigma and policy.
HOW WAS THIS STUDY CONDUCTED?
This study examined how sharing different identity attributes (race, gender, and residential location) with a person with substance use disorder and the initial drug that was used leading to their disorder influences public opinion on opioid policies and individual blame. These identity attributes were experimentally manipulated and randomly chosen to be featured in a fictional news story. Participants were then given a survey that assessed their support for opioid policies and perceptions of the degree to which the person in the news story was blameworthy.
Race was manipulated by showing the hands of either a White or Black person in the story and using different names. Gender was manipulated by using male or female pronouns and names, as well as showing the hands of a man or woman. Variations of residential location that were referenced in the story included an urban downtown center, a quiet suburb, and rural farm. Variations of the initial drug used included heroin, OxyContin for medical use (prescribed by a physician), or non-medical use of OxyContin. These variations were referenced in the story and shown as pictures of either a needle or pills.
The main outcomes of interest included support for opioid treatment spending policy, as measured by the desired degree of change to federal funding for opioid treatment programs, and support for law enforcement spending policy, as measured by the desired degree of change to federal funding for law enforcement to arrest and prosecute people with opioid use disorder. Individual blame was examined as a potential mechanism beyond the main effects of identity and was assessed by the question, “Would you agree or disagree that individuals addicted to opioids are to blame for their own addiction?” The researchers also collected demographic information and zip codes to determine participants’ residential location.
Participants were recruited via NORC’s AmeriSpeak Panel and included a nationally-representative sample of 3,112 adults. The majority of participants were White with an average age of 48 and lived in a suburban location. Approximately half were women.
WHAT DID THIS STUDY FIND?
Race – but not other attributes – affected support for opioid policies.
Among all study participants, there was generally positive support for both the treatment and law enforcement spending policies. However, none of the 3 identity attributes of the person with substance use disorder that was depicted in the news story affected levels of support for either policy. Support levels were overall similar regardless of whether the person depicted was White or Black, a man or woman, and lived in an urban, suburban, or rural residential location.
There were differences, however, based on the match between the race of the study participant and the individual depicted in the news story. When the racial identity of the respondent matched that of the person depicted in the news story, support levels for both the treatment and law enforcement policies were affected.
Among Black study participants, those who received the story about a Black person with substance use disorder were more likely to support the treatment spending policy than when they received the story about a White person. Among White participants, those who received the story about a Black person with substance use disorder were less likely to support the treatment spending policy than when they received the story depicting a White person with substance use disorder.
Black study participants who received the news story about a Black person with substance use disorder were less likely to support the law enforcement spending policy than when they received the story about a White person. Among White study participants, however, there were no differences in support of the law enforcement spending policy between the racial identities of the person depicted in the news story.
There were no differences in support levels for both the treatment and law enforcement spending policies when the study participant was a man and the person depicted in the news story was a man, as well as when the study participant was a woman and person depicted in the news story was a woman. Likewise, there were no differences in support levels for both the treatment and law enforcement spending policies when the participants’ residential location matched that of the person with substance use disorder depicted in the news story.
Pharmaceutical opioids – compared to heroin – reduced blame.
Approximately half of all participants (52%) somewhat or strongly agreed with the statement that those addicted to opioids are to blame for their addiction. This view was associated with a lower likelihood of supporting the treatment spending policy and a higher likelihood of supporting the law enforcement spending policy.
However, when the news story depicted the person with a substance use disorder as initially using OxyContin, participants perceived them as less blameworthy than people who were depicted as initially using heroin. This effect was greater for people whose initial OxyContin use was described as being prescribed by a physician than for people who initially used OxyContin for non-medical purposes.
Aligning race improves policy attitudes only for certain types of opioids.
For those who initially used heroin, perceptions of individual blame were uniformly much higher with shared identity not affecting support for the treatment or law enforcement spending policies.
For those who initially began using opioids through prescribed pills, matching racial identities between the study participant and the person in the news story was associated with an increase in support for the treatment spending policy. Specifically, this meant that when the participant shared the racial identity of the person in the news story, participants had higher levels of support for treatment spending policy. However, matching gender identities had no effect.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study examined the role of shared identities on support for opioid policies and blameworthiness. Results showed that shared racial identities were associated with an increase in support of the treatment spending policy and a decrease in support of the law enforcement spending policy, while shared gender identity and residential location were not associated with support for either policy. Further, perceptions of blame were highest when the person in the news article was depicted as having their opioid use disorder originate from heroin, rather than medical use of OxyContin. Shared racial identity only influenced treatment spending policy support in the latter scenario.
Figure 2 adapted based on original figure from Schaeffer & Pew Research Center, 2023, featuring data from Congressional Research Service, CQ Roll Call, Brookings Institution, Census Bureau population figures.
Notably, the researchers assessed support for the treatment and law enforcement policies and blame by only asking 1 question for each. This is a rather simple way to measure the outcomes and may not comprehensively capture the intended construct (i.e., policy attitudes). Asking more questions that target different dimensions of the constructs could have been a more comprehensive way to measure the constructs of interests, which may have affected the study’s results.
Figure 4 adapted based on original figure from Schaeffer & Pew Research Center, 2023 featuring data from Congressional Research Service, CQ Roll Call, Brookings Institution.
The finding that perceptions of blame were highest when the person in the news article was depicted as having their substance use opioid originate from heroin and lowest when it was depicted as originating from medical use of OxyContin is not surprising – the majority of Americans reported understanding that “accidental” addiction to opioids can happen. This is likely due to the number of opioid use disorders that began with prescription opioids from a physician, which is different from past drug crises. In prior drug crises, people who used drugs were viewed as personally responsible for their actions, whereas in the current crisis it appears that some or all of blame can be put on prescribing physicians and pharmaceutical companies.
At a broader level, the study’s findings are consistent with other research studies that have similarly demonstrated how much media portrayals related to substance use can influence public opinion. Varying socioeconomic status, focusing on violence, and how successful treatment is portrayed may all greatly influence public opinion and stigma. Taken together, this research highlights the importance of how substance use disorders are portrayed in the media.
The researchers measured the outcomes of interest by asking only 1 question for each. This limits how comprehensively they were assessed. Asking several questions for each area of interest may have affected the results by providing a more nuanced and comprehensive assessment of the constructs.
The study’s results may not extend to real-world settings, outside of a research environment where specific variables can be controlled and manipulated, and the attitudes and beliefs examined here may not relate to actual behavior or policy decisions.
Participants were only exposed to the news story once and asked the questions once. Accordingly, the effect of repeated media exposures about people with substance use disorder on support of policies is unclear. It is also unclear whether the results are limited to a certain time period after the exposure or if they extend longer-term.
The research team did not investigate or control for how much participants consumed media regarding the opioid crisis, which may have further increased support of treatment-based policies and reduced perceptions of blame by improving knowledge and understanding.
BOTTOM LINE
Sharing racial identity with someone who has an opioid use disorder is associated with an increase in support of opioid use disorder treatment spending policy and a decrease in support of law enforcement spending policy to arrest and prosecute people with opioid use disorder. Gender and residential setting (urban vs. rural), however, did not impact opioid policy attitudes. These findings support the notion of racial in-group favoritism, which has important implications for how drug policy is created and implemented.
For individuals and families seeking recovery: Individuals may be more likely to support opioid treatment spending policy when they share racial identity with someone with opioid disorder. Individuals also may be more likely to support treatment policy and perceive the person as less blame-worthy when the disorder originates from prescription opioids rather than heroin. If individuals increase their awareness of such biases and seek out opportunities to spend time with people outside of their racial group, stigma may be reduced, and treatment-based policy support may be improved.
For treatment professionals and treatment systems: This study focused on perceptions of the general population but has implications for treatment providers as well. In-group favoritism may be operating outside of awareness. Particularly for therapists who are part of the dominant culture (e.g., White race) treating patients part of non-dominant cultures (e.g., Black race), sustained efforts may be needed to identify and address potential biases in supervision and to understand and empathize with the worldview of the patient.
For scientists: Given that the current study asked only 1 question for each assessed outcome, future research that increases content validity of these outcome domains could provide a more comprehensive understanding of how shared racial identity influences support of treatment-based policies. Further, additional research that examines this potential influence over a longer period of time would shed light on how long the effect of media portrayals lasts. Finally, future research that examines the effects of dosage (i.e., the extent of the exposure to media portrayals, including consumption of media outside of the study) would further improve our understanding of the effects of media portrayals.
For policy makers: Results from this study demonstratedthat individuals are more likely to support opioid treatment spending policy when they share racial identity with someone with opioid disorder, providing support for racial in-group favoritism. Such biases may be overcome, however, by promoting prosocial behaviors, such as empathy, and facilitating integration between different groups, as well as working to understand each other’s viewpoints (i.e., perspective-taking). Accordingly, supporting policies that promote these behaviors may help to reduce in-group bias, thereby benefiting all people rather than only those who have the same race. In addition, including more members of the out-group so that each race is better represented in policymaking contexts would likely result in more equitable policies that benefita larger number of people.