The Affordable Care Act increased insurance access, but not treatment engagement, for people with substance use disorders
Racial/Ethnic minorities in the US historically have had lower rates of health insurance than White Americans, which can impact substance use disorder treatment access. The Affordable Care Act (ACA) was designed to address some of these gaps in healthcare coverage/access. This study examined how the expansion of Medicaid through the ACA changed healthcare coverage and treatment seeking among racial/ethnic minorities of low-income who had substance use disorders across the US.
The Affordable Care Act (ACA) has increased health care coverage of low-income adults by expanding Medicaid. Some studies suggest that the expansion of Medicaid through the ACA has reduced the coverage gaps between low-income racial/ethnic minorities and Whites. To date, however, it is unclear how Medicaid expansion has impacted healthcare coverage among low-income Americans who also have substance use disorders. It is also unknown if coverage increases occurred among Black, Hispanic, and White individuals at similar rates, whether such gains helped to reduce disparities in coverage, and if Medicaid expansion increased substance use disorder treatment among these groups. To understand the impacts of the ACA specifically on low-income individuals with substance use disorder, the current study assessed changes in health care coverage in nationally representative samples of Black, White, and Hispanic low-income adults with substance use disorders both before and after the 2014 ACA Medicaid expansion.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the National Survey on Drug Use and Health (NSDUH). The NSDUH is a nationwide survey conducted annually to collect estimates of substance use disorders among the US population. Data for the current analyses were derived from survey data collected between 2008 and 2019. The analyses compared health care coverage before and after the 2014 ACA Medicaid expansion. Participants included in the current analyses (N=749,033) were: (1) 18 – 64 years old; (2) low-income (self-reported income ≤138% federal poverty line; and (3) met criteria for past year substance use disorder (SUD). The NSDUH did not survey individuals who were 1) homeless or 2) institutionalized (e.g., imprisoned); therefore, this study did not include such individuals.
All variables for the present study were derived via self-report measures of the NSDUH. Past year SUD was defined as meeting criteria for past-year DSM-IV alcohol, cannabis, cocaine, and heroin dependence or abuse. Race/ethnicity of participants was defined via 2 items; “Which of these groups describes you? White, Black, or African American, etc.” and “Are you of Hispanic, Latino, or Spanish origin or descent?”. The authors refer to non-Hispanic White participants as White and non-Hispanic Black participants as Black. In addition, the NSDUH collects self-reported information on age, sex, family income, marital status, education level, employment status, general health status (fair or poor, good, very good, and excellent), and state of residence.
Participants’ state of residence was either defined as “expansion” or “non-expansion states.” Expansion states consisted of the 26 states (and the District of Columbia) that had expanded Medicaid by the end of 2014. The remaining 24 states were considered non-expansion states. Analyses included these variables to control their impact on outcomes of health insurance status and substance use disorder treatment seeking.
The primary outcomes for this study were health insurance coverage and substance use treatment. Participants were asked as part of the NSDUH survey about their current health insurance (e.g., Medicare, Medicaid, private health insurance, etc.). Responses were hierarchically grouped into Medicaid, other public insurance (Medicare or military health care), private insurance, and no insurance. Participants were then asked if they had received any substance use treatment in the past year. Such treatment included services within a hospital, rehabilitation facility, mental health center, emergency department, private physician’s office, other organized settings, and self-help attendance. Insurance-eligible treatment excluded self-help. Services provided in prisons or jails, which are not reimbursed by insurance, were not included.
WHAT DID THIS STUDY FIND?
Low-income adults with substance use disorders in Medicaid-expansion states were more likely to have insurance post-ACA.
After 2014 (when the Medicaid expansion provision of the ACA was enacted) the number of uninsured people with a low-income and substance use disorder decreased. This was observed across all racial/ethnic groups and did not differ between these groups.
Insurance rates varied by race/ethnicity post-ACA in Medicaid non-expansion states.
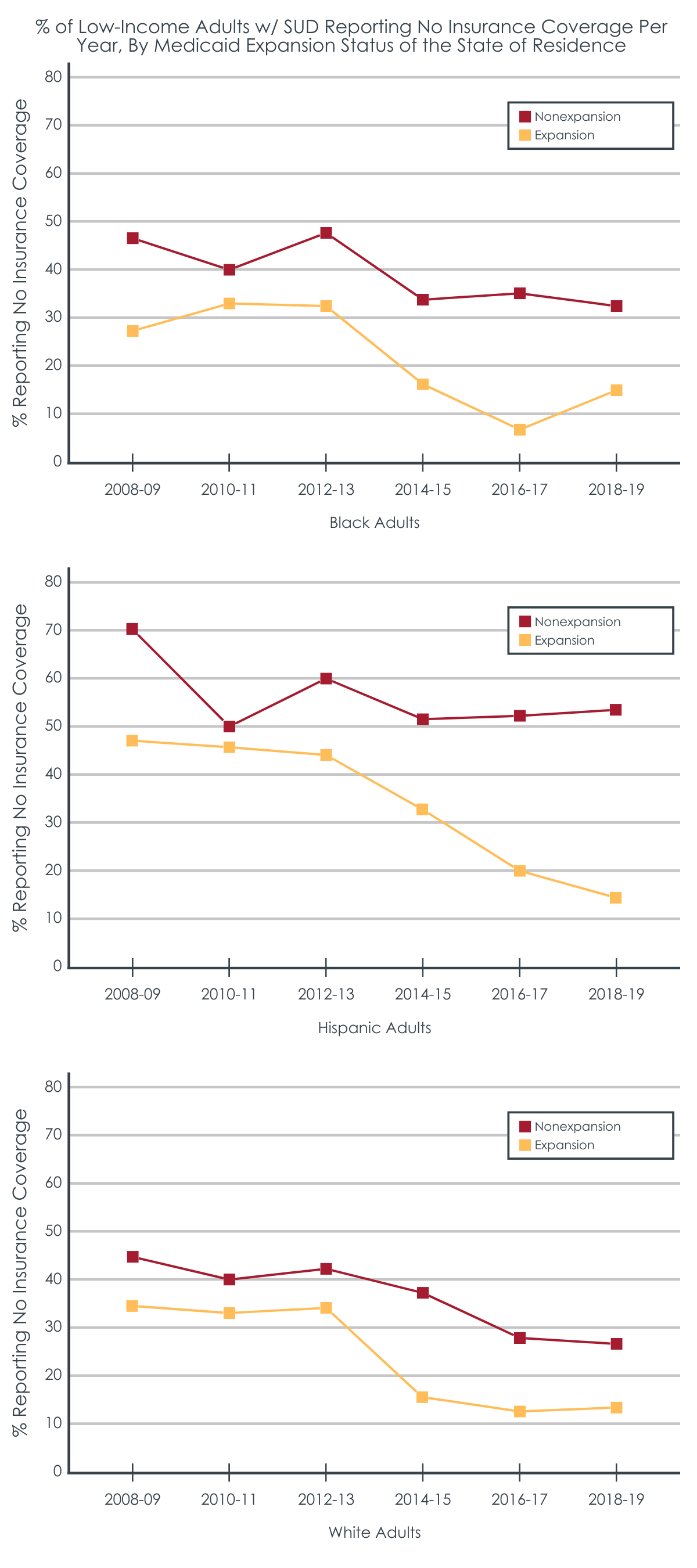
In expansion states, insurance coverage increased for people of all races/ethnicities. However, in non-expansion states, uninsurance rates for Black and White low-income adults with substance use disorders declined. Insurance rates among low-income Hispanic adults with substance use disorders did not change (i.e., remained low) relative to White and Black people.
Despite more healthcare coverage, rates of past year substance use disorder treatment were unchanged.
Analyses showed that most participants did not receive treatment for SUD. In fact, analyses showed that in expansion states the number of White participants receiving SUD treatment decreased after 2014. The number of Hispanic and Black participants receiving SUD treatment did not change regardless of where they lived.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the expansion of Medicaid through the ACA increased health insurance coverage for low-income Americans with SUDs. However, this increase in coverage was uneven across regions and did not translate into increased substance use treatment engagement.
The researchers found that insurance coverage increased among low-income people with SUD living in expansion states relative to those living in non-expansion states. They also found that only White low-income people with SUD had increased insurance coverage in non-expansion states. Taken together, efforts to close the insurance gap based on race/ethnicity were more successful in states that expanded Medicaid. In states that did not expand Medicaid, Black and Hispanic low-income people with SUDs likely continued to face barriers to accessing services. Medicaid expansion appeared to be a critical factor for increased insurance access resulting from the ACA among low-income individuals with SUD.
The results of this research also suggest that increased healthcare coverage did not lead to increased SUD treatment utilization. These results corroborate other research which also found expanding Medicaid did not increase treatment usage. It is unclear why this was the case, but one possible reason could be that some of the sampled individuals with an SUD did not seek treatment because they did not perceive a need to. The sample included individuals who met criteria for a DSM IV “substance abuse” diagnosis, which specifies a set of symptoms less severe than those of substance dependence. It is possible participants who met the criteria for this less severe diagnosis, consequently, did not feel the need to seek any help. More research is needed to uncover the exact reasons for this finding, but these results suggest that access to SUD insurance coverage is not the main barrier to accessing SUD treatment.
Another explanation why participants may not have sought care for SUD despite increased coverage was due to a lack of available substance use treatment close by. In the US SUD treatment is somewhat specialized- research suggests that some clinicians believe that treatment should come from specialists despite substance misuse being fairly common. Being able to access SUD treatment through primary care (e.g., prescribing buprenorphine) could impact SUD treatment usage. It is also possible that differences in SUD treatment availability varies across urban and rural regions of the US. Furthermore, not all SUD treatment centers accept Medicaid making SUD treatment more difficult to obtain for low-income people.
The measure used to define SUDs may have been too broad. The NSDUH survey used in this analysis used the DSM IV diagnostic tool for substance use problems, which differentiates substance use across two conditions: substance abuse and substance dependence. Substance abuse is defined as endorsing one or more symptoms in the past 12 months with no prior history of dependance (e.g., physical withdrawal) for that substance. Such symptoms include “Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home.” Substance dependence is meant to capture more severe SUD- defined as meeting 3 or more criteria in the past 12 months. In some cases, participants may not have sought SUD treatment because they did not feel they needed it. That is, behaviors which may have been flagged as symptoms of a substance abuse diagnosis may have been perceived as not warranting help. For instance, missing a class (i.e., a “role obligation” as a student) due to being hungover could have been perceived as normal behavior to a college student.
The analyses did not stratify participants by whether they sought treatment for SUD. The data suggest that expanding Medicaid did not improve SUD treatment usage, but it is unknown if this lack of usage was due to participants being unable to access care. As described above, if participants felt they did not need care than they may not have sought it.
The study did not examine how population density may have impacted the findings. It is unclear based on the presented results if ACA policies may have been implemented differently within states. For example, it may have been easier for low-income people with SUD living in urban areas to receive treatment relative to people living in more rural areas due to geographical proximity to clinics. This conjecture is somewhat supported by the study results- states with some of the most populace cities in the country (e.g., New York and California) were among the expansion states whereas the non-expansion states tended to be more sparsely populated (e.g., Alaska and Utah), though analyses did not control specifically for residential setting (i.e., urban vs. rural).
Heath care coverage increased among low-income American adults with SUD after the ACA expansion of Medicaid was implemented. However, not all states chose to expand Medicaid coverage and this increase was most pronounced in states that did expand it. Despite increased coverage for low-income individuals with substance use disorder, however, this did not translate into higher rates of SUD treatment engagement. Other factors, including perceived treatment need, may be one reason why insurance – and therefore access – increased, but treatment seeking did not. This also suggests that access to SUD insurance coverage by itself may not be enough to increase treatment engagement.
For individuals and families seeking recovery: Low-income people with SUD may not utilize SUD treatment. However, it is unclear why. It is possible there is a dearth of SUD treatment providers who take Medicaid. For those seeking recovery for themselves or others it is important to be aware of treatment options available. Medicaid does cover addiction treatment, including drug and alcohol rehabilitation. Psychoeducation in general healthcare and other medical settings (e.g., primary care) may help raise patients’ awareness regarding the signs/symptoms of SUD, increasing their motivation to make a change.
For treatment professionals and treatment systems: It is unclear why discrepancies in healthcare coverage and treatment utilization occurred. However, it seems that the way Medicaid expansion was implemented across regions played a role in the observed differences. Those providing treatment to and/or work in healthcare system settings serving racial/ethnic minorities patients may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs. In addition, clinicians may want to modify their communication strategies to be more broadly accessible (e.g., having Spanish versions of patient intake forms, employing bilingual staff, etc.).
For scientists: There is a need for scientists to investigate the reasons for observed differences in Medicaid expansion and SUD treatment utilization. It is possible that some strategies to roll out Medicaid were ineffective at reaching vulnerable populations. There are also myriad possible reasons individuals do not seek treatment including low perceived need for treatment, stigma associated with substance use and related treatment, and beliefs about treatment efficacy. By examining how such factors impacted healthcare coverage and treatment, researchers can make recommendations on developing intervention points to ensure vulnerable populations get the coverage/care they need.
For policy makers: Medicaid expansion reduced health insurance coverage gaps only in states that expanded Medicaid. This resulted in Hispanic low-income people with SUD still having lower rates of coverage relative to other groups. Although it is still unclear exactly why this occurred, it can be inferred that how Medicaid is implemented in non-expansion states is not apt for reaching these populations. As such, policymakers may want to consider strategies to augment Medicaid implementation. This could include partnering with local foundations to channel funding where it is needed most. In addition, investing in culturally/ linguistically appropriate public health communications could be a useful means to increase Medicaid enrollment in Hispanic communities.
The Affordable Care Act (ACA) has increased health care coverage of low-income adults by expanding Medicaid. Some studies suggest that the expansion of Medicaid through the ACA has reduced the coverage gaps between low-income racial/ethnic minorities and Whites. To date, however, it is unclear how Medicaid expansion has impacted healthcare coverage among low-income Americans who also have substance use disorders. It is also unknown if coverage increases occurred among Black, Hispanic, and White individuals at similar rates, whether such gains helped to reduce disparities in coverage, and if Medicaid expansion increased substance use disorder treatment among these groups. To understand the impacts of the ACA specifically on low-income individuals with substance use disorder, the current study assessed changes in health care coverage in nationally representative samples of Black, White, and Hispanic low-income adults with substance use disorders both before and after the 2014 ACA Medicaid expansion.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the National Survey on Drug Use and Health (NSDUH). The NSDUH is a nationwide survey conducted annually to collect estimates of substance use disorders among the US population. Data for the current analyses were derived from survey data collected between 2008 and 2019. The analyses compared health care coverage before and after the 2014 ACA Medicaid expansion. Participants included in the current analyses (N=749,033) were: (1) 18 – 64 years old; (2) low-income (self-reported income ≤138% federal poverty line; and (3) met criteria for past year substance use disorder (SUD). The NSDUH did not survey individuals who were 1) homeless or 2) institutionalized (e.g., imprisoned); therefore, this study did not include such individuals.
All variables for the present study were derived via self-report measures of the NSDUH. Past year SUD was defined as meeting criteria for past-year DSM-IV alcohol, cannabis, cocaine, and heroin dependence or abuse. Race/ethnicity of participants was defined via 2 items; “Which of these groups describes you? White, Black, or African American, etc.” and “Are you of Hispanic, Latino, or Spanish origin or descent?”. The authors refer to non-Hispanic White participants as White and non-Hispanic Black participants as Black. In addition, the NSDUH collects self-reported information on age, sex, family income, marital status, education level, employment status, general health status (fair or poor, good, very good, and excellent), and state of residence.
Participants’ state of residence was either defined as “expansion” or “non-expansion states.” Expansion states consisted of the 26 states (and the District of Columbia) that had expanded Medicaid by the end of 2014. The remaining 24 states were considered non-expansion states. Analyses included these variables to control their impact on outcomes of health insurance status and substance use disorder treatment seeking.
The primary outcomes for this study were health insurance coverage and substance use treatment. Participants were asked as part of the NSDUH survey about their current health insurance (e.g., Medicare, Medicaid, private health insurance, etc.). Responses were hierarchically grouped into Medicaid, other public insurance (Medicare or military health care), private insurance, and no insurance. Participants were then asked if they had received any substance use treatment in the past year. Such treatment included services within a hospital, rehabilitation facility, mental health center, emergency department, private physician’s office, other organized settings, and self-help attendance. Insurance-eligible treatment excluded self-help. Services provided in prisons or jails, which are not reimbursed by insurance, were not included.
WHAT DID THIS STUDY FIND?
Low-income adults with substance use disorders in Medicaid-expansion states were more likely to have insurance post-ACA.
After 2014 (when the Medicaid expansion provision of the ACA was enacted) the number of uninsured people with a low-income and substance use disorder decreased. This was observed across all racial/ethnic groups and did not differ between these groups.
Insurance rates varied by race/ethnicity post-ACA in Medicaid non-expansion states.
In expansion states, insurance coverage increased for people of all races/ethnicities. However, in non-expansion states, uninsurance rates for Black and White low-income adults with substance use disorders declined. Insurance rates among low-income Hispanic adults with substance use disorders did not change (i.e., remained low) relative to White and Black people.
Despite more healthcare coverage, rates of past year substance use disorder treatment were unchanged.
Analyses showed that most participants did not receive treatment for SUD. In fact, analyses showed that in expansion states the number of White participants receiving SUD treatment decreased after 2014. The number of Hispanic and Black participants receiving SUD treatment did not change regardless of where they lived.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the expansion of Medicaid through the ACA increased health insurance coverage for low-income Americans with SUDs. However, this increase in coverage was uneven across regions and did not translate into increased substance use treatment engagement.
The researchers found that insurance coverage increased among low-income people with SUD living in expansion states relative to those living in non-expansion states. They also found that only White low-income people with SUD had increased insurance coverage in non-expansion states. Taken together, efforts to close the insurance gap based on race/ethnicity were more successful in states that expanded Medicaid. In states that did not expand Medicaid, Black and Hispanic low-income people with SUDs likely continued to face barriers to accessing services. Medicaid expansion appeared to be a critical factor for increased insurance access resulting from the ACA among low-income individuals with SUD.
The results of this research also suggest that increased healthcare coverage did not lead to increased SUD treatment utilization. These results corroborate other research which also found expanding Medicaid did not increase treatment usage. It is unclear why this was the case, but one possible reason could be that some of the sampled individuals with an SUD did not seek treatment because they did not perceive a need to. The sample included individuals who met criteria for a DSM IV “substance abuse” diagnosis, which specifies a set of symptoms less severe than those of substance dependence. It is possible participants who met the criteria for this less severe diagnosis, consequently, did not feel the need to seek any help. More research is needed to uncover the exact reasons for this finding, but these results suggest that access to SUD insurance coverage is not the main barrier to accessing SUD treatment.
Another explanation why participants may not have sought care for SUD despite increased coverage was due to a lack of available substance use treatment close by. In the US SUD treatment is somewhat specialized- research suggests that some clinicians believe that treatment should come from specialists despite substance misuse being fairly common. Being able to access SUD treatment through primary care (e.g., prescribing buprenorphine) could impact SUD treatment usage. It is also possible that differences in SUD treatment availability varies across urban and rural regions of the US. Furthermore, not all SUD treatment centers accept Medicaid making SUD treatment more difficult to obtain for low-income people.
The measure used to define SUDs may have been too broad. The NSDUH survey used in this analysis used the DSM IV diagnostic tool for substance use problems, which differentiates substance use across two conditions: substance abuse and substance dependence. Substance abuse is defined as endorsing one or more symptoms in the past 12 months with no prior history of dependance (e.g., physical withdrawal) for that substance. Such symptoms include “Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home.” Substance dependence is meant to capture more severe SUD- defined as meeting 3 or more criteria in the past 12 months. In some cases, participants may not have sought SUD treatment because they did not feel they needed it. That is, behaviors which may have been flagged as symptoms of a substance abuse diagnosis may have been perceived as not warranting help. For instance, missing a class (i.e., a “role obligation” as a student) due to being hungover could have been perceived as normal behavior to a college student.
The analyses did not stratify participants by whether they sought treatment for SUD. The data suggest that expanding Medicaid did not improve SUD treatment usage, but it is unknown if this lack of usage was due to participants being unable to access care. As described above, if participants felt they did not need care than they may not have sought it.
The study did not examine how population density may have impacted the findings. It is unclear based on the presented results if ACA policies may have been implemented differently within states. For example, it may have been easier for low-income people with SUD living in urban areas to receive treatment relative to people living in more rural areas due to geographical proximity to clinics. This conjecture is somewhat supported by the study results- states with some of the most populace cities in the country (e.g., New York and California) were among the expansion states whereas the non-expansion states tended to be more sparsely populated (e.g., Alaska and Utah), though analyses did not control specifically for residential setting (i.e., urban vs. rural).
Heath care coverage increased among low-income American adults with SUD after the ACA expansion of Medicaid was implemented. However, not all states chose to expand Medicaid coverage and this increase was most pronounced in states that did expand it. Despite increased coverage for low-income individuals with substance use disorder, however, this did not translate into higher rates of SUD treatment engagement. Other factors, including perceived treatment need, may be one reason why insurance – and therefore access – increased, but treatment seeking did not. This also suggests that access to SUD insurance coverage by itself may not be enough to increase treatment engagement.
For individuals and families seeking recovery: Low-income people with SUD may not utilize SUD treatment. However, it is unclear why. It is possible there is a dearth of SUD treatment providers who take Medicaid. For those seeking recovery for themselves or others it is important to be aware of treatment options available. Medicaid does cover addiction treatment, including drug and alcohol rehabilitation. Psychoeducation in general healthcare and other medical settings (e.g., primary care) may help raise patients’ awareness regarding the signs/symptoms of SUD, increasing their motivation to make a change.
For treatment professionals and treatment systems: It is unclear why discrepancies in healthcare coverage and treatment utilization occurred. However, it seems that the way Medicaid expansion was implemented across regions played a role in the observed differences. Those providing treatment to and/or work in healthcare system settings serving racial/ethnic minorities patients may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs. In addition, clinicians may want to modify their communication strategies to be more broadly accessible (e.g., having Spanish versions of patient intake forms, employing bilingual staff, etc.).
For scientists: There is a need for scientists to investigate the reasons for observed differences in Medicaid expansion and SUD treatment utilization. It is possible that some strategies to roll out Medicaid were ineffective at reaching vulnerable populations. There are also myriad possible reasons individuals do not seek treatment including low perceived need for treatment, stigma associated with substance use and related treatment, and beliefs about treatment efficacy. By examining how such factors impacted healthcare coverage and treatment, researchers can make recommendations on developing intervention points to ensure vulnerable populations get the coverage/care they need.
For policy makers: Medicaid expansion reduced health insurance coverage gaps only in states that expanded Medicaid. This resulted in Hispanic low-income people with SUD still having lower rates of coverage relative to other groups. Although it is still unclear exactly why this occurred, it can be inferred that how Medicaid is implemented in non-expansion states is not apt for reaching these populations. As such, policymakers may want to consider strategies to augment Medicaid implementation. This could include partnering with local foundations to channel funding where it is needed most. In addition, investing in culturally/ linguistically appropriate public health communications could be a useful means to increase Medicaid enrollment in Hispanic communities.
The Affordable Care Act (ACA) has increased health care coverage of low-income adults by expanding Medicaid. Some studies suggest that the expansion of Medicaid through the ACA has reduced the coverage gaps between low-income racial/ethnic minorities and Whites. To date, however, it is unclear how Medicaid expansion has impacted healthcare coverage among low-income Americans who also have substance use disorders. It is also unknown if coverage increases occurred among Black, Hispanic, and White individuals at similar rates, whether such gains helped to reduce disparities in coverage, and if Medicaid expansion increased substance use disorder treatment among these groups. To understand the impacts of the ACA specifically on low-income individuals with substance use disorder, the current study assessed changes in health care coverage in nationally representative samples of Black, White, and Hispanic low-income adults with substance use disorders both before and after the 2014 ACA Medicaid expansion.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the National Survey on Drug Use and Health (NSDUH). The NSDUH is a nationwide survey conducted annually to collect estimates of substance use disorders among the US population. Data for the current analyses were derived from survey data collected between 2008 and 2019. The analyses compared health care coverage before and after the 2014 ACA Medicaid expansion. Participants included in the current analyses (N=749,033) were: (1) 18 – 64 years old; (2) low-income (self-reported income ≤138% federal poverty line; and (3) met criteria for past year substance use disorder (SUD). The NSDUH did not survey individuals who were 1) homeless or 2) institutionalized (e.g., imprisoned); therefore, this study did not include such individuals.
All variables for the present study were derived via self-report measures of the NSDUH. Past year SUD was defined as meeting criteria for past-year DSM-IV alcohol, cannabis, cocaine, and heroin dependence or abuse. Race/ethnicity of participants was defined via 2 items; “Which of these groups describes you? White, Black, or African American, etc.” and “Are you of Hispanic, Latino, or Spanish origin or descent?”. The authors refer to non-Hispanic White participants as White and non-Hispanic Black participants as Black. In addition, the NSDUH collects self-reported information on age, sex, family income, marital status, education level, employment status, general health status (fair or poor, good, very good, and excellent), and state of residence.
Participants’ state of residence was either defined as “expansion” or “non-expansion states.” Expansion states consisted of the 26 states (and the District of Columbia) that had expanded Medicaid by the end of 2014. The remaining 24 states were considered non-expansion states. Analyses included these variables to control their impact on outcomes of health insurance status and substance use disorder treatment seeking.
The primary outcomes for this study were health insurance coverage and substance use treatment. Participants were asked as part of the NSDUH survey about their current health insurance (e.g., Medicare, Medicaid, private health insurance, etc.). Responses were hierarchically grouped into Medicaid, other public insurance (Medicare or military health care), private insurance, and no insurance. Participants were then asked if they had received any substance use treatment in the past year. Such treatment included services within a hospital, rehabilitation facility, mental health center, emergency department, private physician’s office, other organized settings, and self-help attendance. Insurance-eligible treatment excluded self-help. Services provided in prisons or jails, which are not reimbursed by insurance, were not included.
WHAT DID THIS STUDY FIND?
Low-income adults with substance use disorders in Medicaid-expansion states were more likely to have insurance post-ACA.
After 2014 (when the Medicaid expansion provision of the ACA was enacted) the number of uninsured people with a low-income and substance use disorder decreased. This was observed across all racial/ethnic groups and did not differ between these groups.
Insurance rates varied by race/ethnicity post-ACA in Medicaid non-expansion states.
In expansion states, insurance coverage increased for people of all races/ethnicities. However, in non-expansion states, uninsurance rates for Black and White low-income adults with substance use disorders declined. Insurance rates among low-income Hispanic adults with substance use disorders did not change (i.e., remained low) relative to White and Black people.
Despite more healthcare coverage, rates of past year substance use disorder treatment were unchanged.
Analyses showed that most participants did not receive treatment for SUD. In fact, analyses showed that in expansion states the number of White participants receiving SUD treatment decreased after 2014. The number of Hispanic and Black participants receiving SUD treatment did not change regardless of where they lived.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the expansion of Medicaid through the ACA increased health insurance coverage for low-income Americans with SUDs. However, this increase in coverage was uneven across regions and did not translate into increased substance use treatment engagement.
The researchers found that insurance coverage increased among low-income people with SUD living in expansion states relative to those living in non-expansion states. They also found that only White low-income people with SUD had increased insurance coverage in non-expansion states. Taken together, efforts to close the insurance gap based on race/ethnicity were more successful in states that expanded Medicaid. In states that did not expand Medicaid, Black and Hispanic low-income people with SUDs likely continued to face barriers to accessing services. Medicaid expansion appeared to be a critical factor for increased insurance access resulting from the ACA among low-income individuals with SUD.
The results of this research also suggest that increased healthcare coverage did not lead to increased SUD treatment utilization. These results corroborate other research which also found expanding Medicaid did not increase treatment usage. It is unclear why this was the case, but one possible reason could be that some of the sampled individuals with an SUD did not seek treatment because they did not perceive a need to. The sample included individuals who met criteria for a DSM IV “substance abuse” diagnosis, which specifies a set of symptoms less severe than those of substance dependence. It is possible participants who met the criteria for this less severe diagnosis, consequently, did not feel the need to seek any help. More research is needed to uncover the exact reasons for this finding, but these results suggest that access to SUD insurance coverage is not the main barrier to accessing SUD treatment.
Another explanation why participants may not have sought care for SUD despite increased coverage was due to a lack of available substance use treatment close by. In the US SUD treatment is somewhat specialized- research suggests that some clinicians believe that treatment should come from specialists despite substance misuse being fairly common. Being able to access SUD treatment through primary care (e.g., prescribing buprenorphine) could impact SUD treatment usage. It is also possible that differences in SUD treatment availability varies across urban and rural regions of the US. Furthermore, not all SUD treatment centers accept Medicaid making SUD treatment more difficult to obtain for low-income people.
The measure used to define SUDs may have been too broad. The NSDUH survey used in this analysis used the DSM IV diagnostic tool for substance use problems, which differentiates substance use across two conditions: substance abuse and substance dependence. Substance abuse is defined as endorsing one or more symptoms in the past 12 months with no prior history of dependance (e.g., physical withdrawal) for that substance. Such symptoms include “Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home.” Substance dependence is meant to capture more severe SUD- defined as meeting 3 or more criteria in the past 12 months. In some cases, participants may not have sought SUD treatment because they did not feel they needed it. That is, behaviors which may have been flagged as symptoms of a substance abuse diagnosis may have been perceived as not warranting help. For instance, missing a class (i.e., a “role obligation” as a student) due to being hungover could have been perceived as normal behavior to a college student.
The analyses did not stratify participants by whether they sought treatment for SUD. The data suggest that expanding Medicaid did not improve SUD treatment usage, but it is unknown if this lack of usage was due to participants being unable to access care. As described above, if participants felt they did not need care than they may not have sought it.
The study did not examine how population density may have impacted the findings. It is unclear based on the presented results if ACA policies may have been implemented differently within states. For example, it may have been easier for low-income people with SUD living in urban areas to receive treatment relative to people living in more rural areas due to geographical proximity to clinics. This conjecture is somewhat supported by the study results- states with some of the most populace cities in the country (e.g., New York and California) were among the expansion states whereas the non-expansion states tended to be more sparsely populated (e.g., Alaska and Utah), though analyses did not control specifically for residential setting (i.e., urban vs. rural).
Heath care coverage increased among low-income American adults with SUD after the ACA expansion of Medicaid was implemented. However, not all states chose to expand Medicaid coverage and this increase was most pronounced in states that did expand it. Despite increased coverage for low-income individuals with substance use disorder, however, this did not translate into higher rates of SUD treatment engagement. Other factors, including perceived treatment need, may be one reason why insurance – and therefore access – increased, but treatment seeking did not. This also suggests that access to SUD insurance coverage by itself may not be enough to increase treatment engagement.
For individuals and families seeking recovery: Low-income people with SUD may not utilize SUD treatment. However, it is unclear why. It is possible there is a dearth of SUD treatment providers who take Medicaid. For those seeking recovery for themselves or others it is important to be aware of treatment options available. Medicaid does cover addiction treatment, including drug and alcohol rehabilitation. Psychoeducation in general healthcare and other medical settings (e.g., primary care) may help raise patients’ awareness regarding the signs/symptoms of SUD, increasing their motivation to make a change.
For treatment professionals and treatment systems: It is unclear why discrepancies in healthcare coverage and treatment utilization occurred. However, it seems that the way Medicaid expansion was implemented across regions played a role in the observed differences. Those providing treatment to and/or work in healthcare system settings serving racial/ethnic minorities patients may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs. In addition, clinicians may want to modify their communication strategies to be more broadly accessible (e.g., having Spanish versions of patient intake forms, employing bilingual staff, etc.).
For scientists: There is a need for scientists to investigate the reasons for observed differences in Medicaid expansion and SUD treatment utilization. It is possible that some strategies to roll out Medicaid were ineffective at reaching vulnerable populations. There are also myriad possible reasons individuals do not seek treatment including low perceived need for treatment, stigma associated with substance use and related treatment, and beliefs about treatment efficacy. By examining how such factors impacted healthcare coverage and treatment, researchers can make recommendations on developing intervention points to ensure vulnerable populations get the coverage/care they need.
For policy makers: Medicaid expansion reduced health insurance coverage gaps only in states that expanded Medicaid. This resulted in Hispanic low-income people with SUD still having lower rates of coverage relative to other groups. Although it is still unclear exactly why this occurred, it can be inferred that how Medicaid is implemented in non-expansion states is not apt for reaching these populations. As such, policymakers may want to consider strategies to augment Medicaid implementation. This could include partnering with local foundations to channel funding where it is needed most. In addition, investing in culturally/ linguistically appropriate public health communications could be a useful means to increase Medicaid enrollment in Hispanic communities.