“Drink like a man”: Masculinity and hazardous drinking among lesbian and bisexual women
Lesbian and bisexual identified women have higher rates of hazardous drinking than heterosexual women. Health disparities in alcohol use may be explained by greater stress resulting from heterosexism, but also by increased hazardous use in order to align with perceived “masculine” drinking norms. To help disentangle these potential explanations, this study examined lesbian and bisexual women’s experiences with alcohol, minority stress, and gender expression.
Disparities in alcohol use between LGBTQ+ and heterosexual populations, may be due, in part, to the stigmatization and subsequent stigma-related stressors (“minority stress”) LGBTQ+ people face.
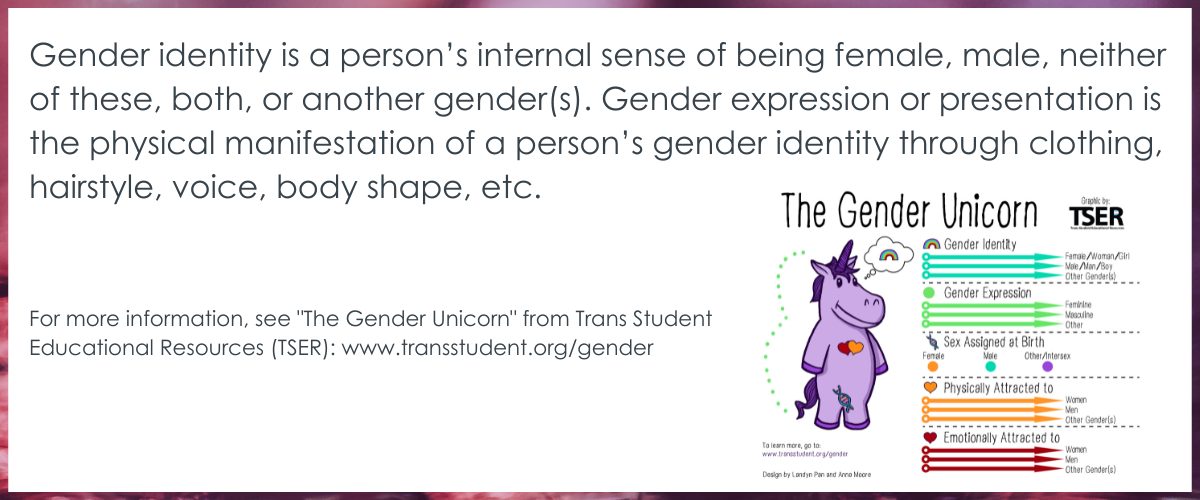
The stigmatization of LGBTQ+ people is based in heterosexual hegemony (sometimes referred to as ‘heteronormativity’ or ‘cisnormativity’), that collapse gender into a single binary that ties sex/gender/sexuality together, whereby a person’s sex assigned at birth is either assumed to be female or male, which is then assumed to determine a person’s gender and sexuality. This plays out in society through routines deemed acceptable (considered the default or the “norm”) – for example, people assigned female sex at birth are presumed to identify as women (sex and gender identity), women are presumed to dress in a feminine way (gender expression/presentation), and women are presumed to be attracted to men (sexuality). This intersection of heterosexism, sexism, and misogyny is particularly relevant for lesbian and bisexual women, who may more commonly adopt a more masculine presenting appearance or social role than heterosexual women.
While gender nonconformity among lesbian and bisexual women could carry important implications for the visibility of their stigmatized sexual identity, and subsequent experience and coping with minority stress (e.g., alcohol use), masculinity may also influence alcohol-use norms and exposure to heavy drinking venues. Among heterosexual individuals, higher levels of masculinity are associated with greater alcohol consumption among men and women, but there is still much to learn in this regard.
Taken together, the researchers wanted to know, among lesbian and bisexual women, is more masculinity associated with greater hazardous drinking, and greater femininity associated with lower hazardous drinking? Are these differences actually accounted for by differences in minority stress? The thought is that by understanding more about the factors underlying lesbian and bisexual women’s hazardous drinking, more helpful treatment and policy approaches could be developed to reduce harms in this at-risk group.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional analysis of wave 3 data (2010-2012) from a 22-year longitudinal cohort study of sexual minority women. Nearly 600 lesbian and bisexual women living in the Chicago area (N = 598) answered questions at a single time point about their gender identity and expression (masculinity and femininity), past year experiences of minority stress (discrimination, awareness/expectation, and internalized), and past year alcohol use, alcohol-related problems, and alcohol use disorder symptoms.
Participants were included in this study if they identified as lesbian, mostly lesbian, or bisexual, were age 18 or older, fluent in English, and lived in the Chicago metropolitan area. For this analysis, the researchers excluded participants if they reported lifetime or past 12-month abstinence from alcohol.
The researchers asked participants, “How often did you have 6 or more drinks of wine, beer, or liquor in a single day?” and “About how many drinks would you have on a typical day when you drank?” Participants who reported consuming ≥ 6 drinks on one or more days in the past 12 months or if they reported consuming ≥ 4 drinks on a typical drinking day were classified as experiencing “any heavy episodic drinking” (hereafter referred to simply as “heavy drinking”).
To assess alcohol-related problems, participants were given a list of 8 negative consequences related to drinking, such as driving a car while intoxicated or fights with their partner or other people when drinking and asked if any of the events on the list had happened to them in the past 12 months. Participants were classified based on whether they reported at least one alcohol-related problem.
To assess potential symptoms of alcohol use disorder (based on DSM-IV alcohol dependence criteria), participants were asked if they had experienced any one of a list of 5 symptoms in the previous 12 months, such as inability to stop drinking before becoming intoxicated and inability to stop or cut down on drinking over time. Participants were classified as “any” or “no symptoms reported.”
For gender identity, participants were asked on a scale from 1 to 7, “In general, how masculine do you think you are?” and “In general, how feminine do you think you are?” For gender expression, participants were asked, “How masculine do you act, appear, and come across to others?” and “How feminine do you act, appear, and come across to others?” Responses were categorized as “not at all/very little” (1–2), “moderately” (3–5), and “extremely” (6–7).
Three different questionnaires validated in prior research were used to measure minority stress in the past 12 months: discrimination, stigma awareness and sensitivity, and internalized stigma.
The analyses tested the association between participants’ gender identity and expression (masculine and feminine) and alcohol outcomes (heavy drinking, alcohol problems, alcohol use disorder symptoms), while accounting for participants minority stress (discrimination, stigma awareness and sensitivity, and internalized stigma), as well as participant characteristics (age, race/ethnicity, sexual identity, and education). This allowed the researchers to examine if gender expression or minority stress was a greater influence on drinking, while accounting for demographic characteristics that could also influence drinking (e.g., younger individuals tend to have higher rates of heavy episodic drinking compared to older individuals).
There was a relatively equal number of participants across young, middle, and older age, with an average age of 39 years. About 1/3 of the sample identified as Black/African American, 1/3 Hispanic/Latinx, and 1/3 White, non-Hispanic. A majority of participants (74%) identified as lesbian or mostly lesbian. 50% of participants believed others viewed them as moderately masculine, and 62% reported their self-perceived gender identity as moderately masculine. Femininity was similar with 55% of participants reporting moderately feminine self-perceived gender identity and 51% reporting a belief that other people viewed them as moderately feminine.
WHAT DID THIS STUDY FIND?
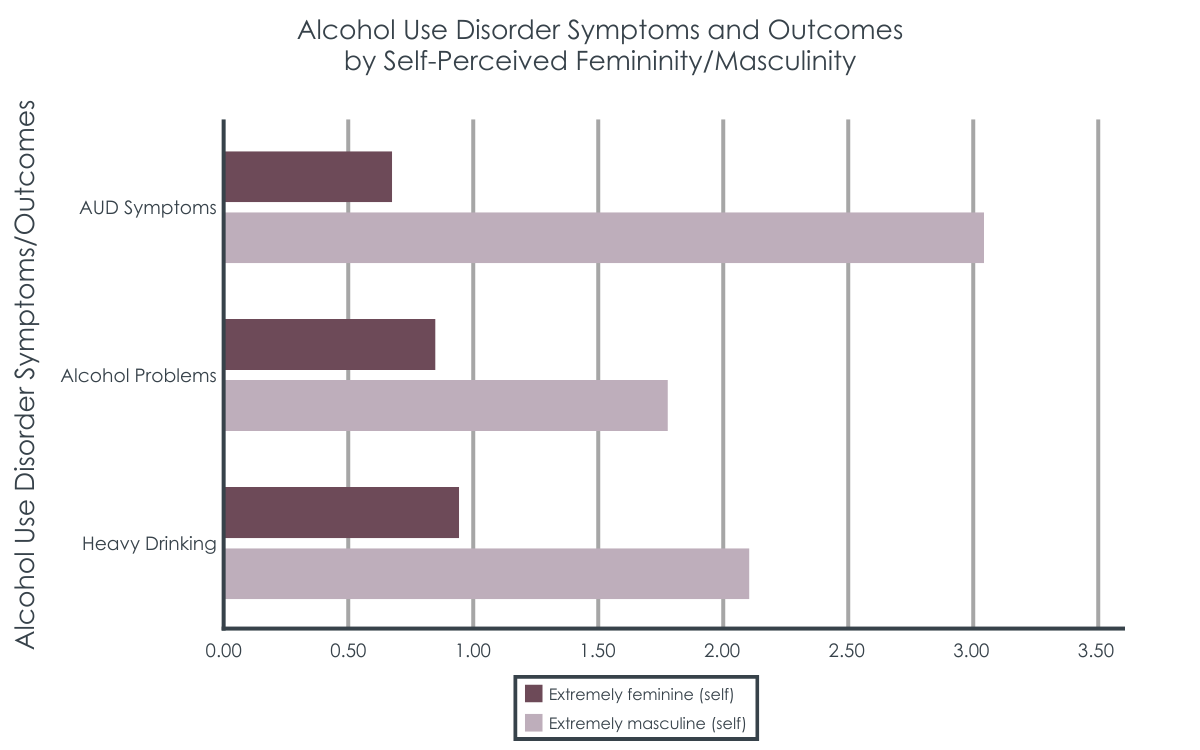
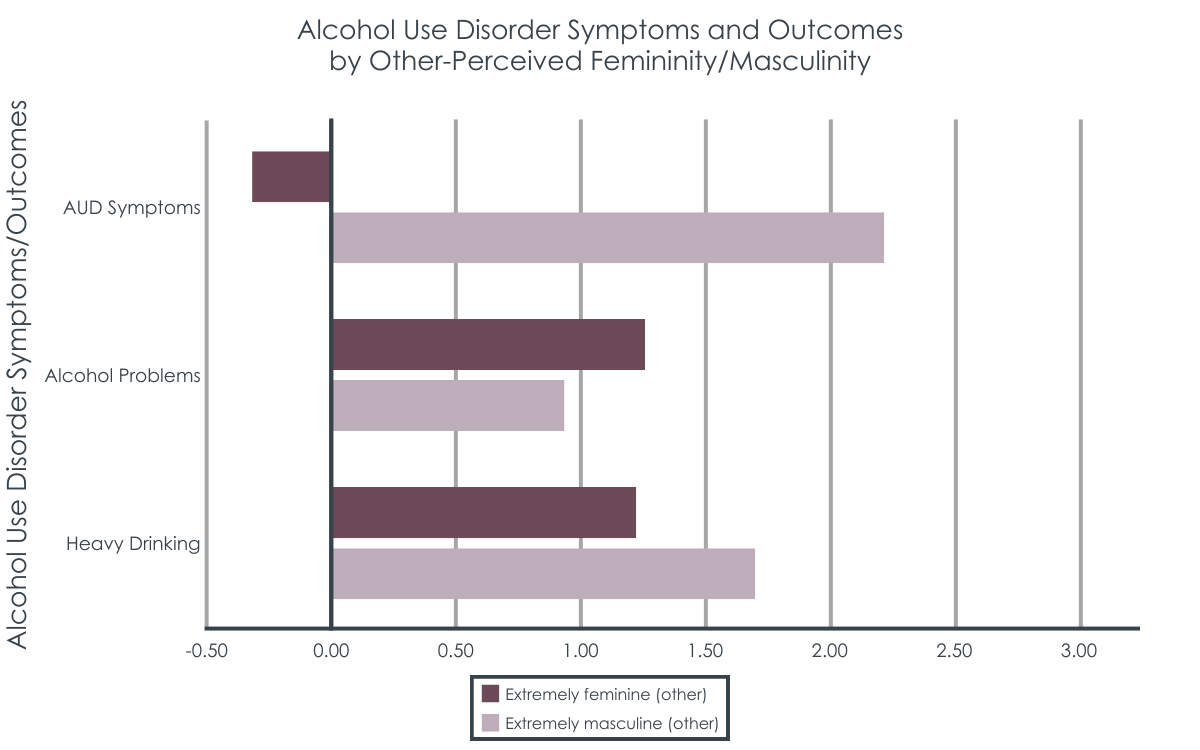
Masculine lesbian and bisexual women reported greater drinking alcohol problems, and alcohol use disorder symptoms.
Lesbian and bisexual women who perceived themselves as extremely masculine were 2 times more likely to experience at least one episode of heavy drinking over the past year, compared to women who described themselves as not at all masculine. Masculine lesbian and bisexual women were also 3 times more likely to have at least one symptom of alcohol use disorder. Ratings of femininity were not associated with alcohol outcomes.
Minority stress was not associated with alcohol outcomes when accounting for gender self-concept.
None of the minority stress variables (identity-based discrimination, stigma sensitivity/awareness, internalized stigma) were significantly associated with any of the hazardous drinking outcomes (heavy drinking, alcohol problems, alcohol use disorder symptoms) in these models, nor did they impact the association between gender expression and hazardous drinking.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this survey of lesbian and bisexual women living in the Chicago greater area, masculinity, in particular masculine gender expression, was associated with hazardous drinking. This association was not explained by minority stress as the research team had predicted.
The researchers had good theoretical reasons to believe that minority stress could play a role in greater drinking outcomes among lesbian and bisexual women through gender nonconformity; however, this was not supported in the current study.
This is surprising, given that other research has found an association between minority stress, drinking, and alcohol problems, such as among MSM living with HIV. For some lesbian and bisexual women, gender nonconformity may be protective against minority stress-related risk for hazardous drinking. For example, gender nonconformity is associated with greater connectedness with other lesbians and bisexual women, which can bolster social support, and may buffer against negative minority stress-related health outcomes. Conversely, in this sample, it appears that perhaps gender nonconformity and perceptions of gender-related drinking norms played a larger role in reported drinking and related problems.
Bisexual women in this study had greater odds of alcohol use disorder symptoms than lesbian women. This is consistent with a national study of adults with alcohol use disorder, where bisexual participants, among gay and lesbian participants as well, had more severe alcohol use disorder symptoms and more co-morbid drug use and mood disorders compared to heterosexual participants. Bisexual individuals were also much more likely to seek help for alcohol use disorder across treatment venues compared to heterosexual, gay, and lesbian individuals, whereas there were no differences in help-seeking between gay, lesbian, and heterosexual participants. As mentioned above, community connection may buffer against minority stress, and bisexual women may not feel as much a part of the lesbian community due to stigma (i.e., monosexism – a presumption that everyone is, or should be, attracted to no more than one gender) that permeates the LGBTQ+ community as well as heterosexism outside the community, which may relate to worse mental health symptoms, greater alcohol use, and increased help-seeking. In other words, bisexual women may feel greater stress as they may not feel fully accepted in either the LGBTQ+ community, nor by heterosexual individuals.
Rates of alcohol use disorder in the U.S. have been higher among men, and decades of research has examined the biological and social mechanisms for these differences. One difference, simply put, is that men tend to drink more frequently and in greater quantities than women do. In recent years, in general, men still consume more alcohol and experience and cause more alcohol-related injuries and deaths than women do, but the gaps are narrowing. This has put additional attention on social factors that could influence drinking differences between men and women, rather than biological sex factors alone. For example, in a large sample of college students, masculine gender-orientation was positively associated with heavy episodic drinking, regardless of sex. This suggests potentially a perception or social norm that associates masculinity with heavier drinking.
Research on heavy drinking among college students also points to the effects of social norms, whereby college students’ drinking is influenced by perceptions of how their peers drink, and these perceptions are often incorrect, overestimating peer drinking norms. If inaccurate perceptions can be corrected, young people may drink less. Similarly, if inaccurate perceptions about masculinity and drinking can be corrected, individuals with a more masculine gender-orientation may drink less as well. Early innovative research is being conducted in this area, testing app-delivered social norms interventions specifically for lesbian and bisexual women.
Social norms interventions are meant to correct this misperception by providing information about actual student drinking norms and personalized feedback comparing actual student drinking patterns and perceptions of the norm, pointing out discrepancies. In order to effectively provide such an intervention for lesbian and bisexual women, we need accurate population-level data of LGBTQ+-identified individuals and their drinking, and not all national health surveys measure sexual orientation and gender identity information well, or at all. That aside, social norms interventions only have some evidence supporting their effectiveness to reduce drinking and related problems and should be combined with other evidence-supported interventions to reduce drinking, as they are not considered effective enough on their own to reduce alcohol use or misuse among college students over the long-term.
It is notable in this study that indicators of hazardous drinking were measured at a relatively low threshold – participants only needed to endorse one instance of heavy episodic drinking, an alcohol-related problem, or one alcohol use disorder symptom in the past year to be included in the hazardous drinking category. Additionally, individuals who had periods of abstinence were excluded from these analyses, which may have excluded individuals with more severe alcohol problems and alcohol use disorder symptoms seeking or engaging in treatment. This may have also contributed to the lack of association between minority stress and alcohol outcomes when accounting for gender self-concept: if participants with more severe alcohol problems also had greater minority stress and were potentially excluded from analyses because of any attempt or period of abstinence, this could have limited the range and severity of minority stress experienced in this sample. Indeed, participants in this study reported an average of 1 experience of sexual identity-based discrimination in the past year. However, the researchers did not report minority stress scores of participants excluded in the study, so ultimately it is unknown how including participants with periods of abstinence could have affected the association between minority stress and alcohol outcomes.
The threshold for hazardous drinking in the current study was quite low, meaning that the researchers categorized any endorsement of drinking 6 or more drinks on a single occasion in the last 12 months as heavy episodic drinking. These criteria are also based on older drinking limit recommendations from the NIAAA, which have been updated since the data were collected. The researchers accounted for this change by also counting participants who indicated they drank 4 or more drinks on a typical drinking day. This means that participants who drink very infrequently but in higher amounts were categorized the same as participants who were regularly drinking more than 7 drinks per week. This is reflected in their analyses showing that participants aged 18-29 were more likely to have any heavy episodic drinking, where high drinking quantity but lower frequency is more common. Although there are health risks (e.g., accidents and injuries) associated with drinking 4 or more drinks on any occasion for women, it may not be indicative of alcohol misuse if very infrequent, whereas alcohol-related problems or symptoms of alcohol use disorder may be better indicators.
Participants with prior abstinence were not included in these analyses, and the researchers did not provide detailed information on how this was measured. This means that participants could have been excluded who had periods of abstinence for other medical reasons or life stage events, such as pregnancy. It may have also excluded participants seeking or involved in alcohol treatment. This could have unknown effects on their analyses, in particular related to conclusions about minority stress and the lack of association with hazardous drinking. It is possible that participants who experienced greater minority stress also had greater problems and attempts/periods of abstinence, which would have excluded them from these analyses.
The researchers chose to dichotomize their outcome measures, which limited their statistical power to run additional interaction analyses, even though they had a relatively very large sample of lesbian and bisexual women. It’s possible the researchers used dichotomous outcomes for ease in interpretation of the results; however, they may have had more power to run additional interaction analyses between gender self-concept and other demographic characteristics, like sexual orientation and race/ethnicity if they had left the measures on a more continuous, interval-level, scale.
BOTTOM LINE
This study found that, among a large sample of nearly 600 lesbian and bisexual women in the Chicago area, masculine gender expression was associated with a greater likelihood of reporting at least one indicator hazardous drinking, and minority stress did not explain this association. This may mean that social norms associated with masculinity and drinking may be a risk factor for hazardous use, and that alcohol interventions could be tailored to address perceptions of social drinking norms.
For individuals and families seeking recovery: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. If we work to decouple the perception that heavy drinking is a masculine behavior, masculine individuals may drink less and experience fewer alcohol problems.
For treatment professionals and treatment systems: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. For some individuals drinking at risky levels or seeking alcohol treatment, it may be important to correct inaccurate perceptions of gendered drinking norms. For LGBTQ+ individuals with a more masculine gender self-concept, working to decouple the perception that heavy drinking is a masculine behavior may increase motivation to reduce drinking.
For scientists: Findings from this cross-sectional analysis of wave 3 data (2010-2012) from a 22-year longitudinal cohort study of sexual minority women in the Chicago area found that lesbian and bisexual women with greater masculine gender expression had a 2-3xs greater odds of having any instance of heavy episodic drinking, one or more alcohol problem, and one or more alcohol use disorder symptom in the past 12 months, controlling for minority stress (identity-based discrimination, stigma sensitivity and awareness, and internalized stigma) and demographics (age, race/ethnicity, sexual identity, and education). Contrary to hypotheses, minority stress was not significantly associated with indicators of hazardous drinking in models accounting for gender self-concept and demographic characteristics, nor influenced the association between gender self-concept and hazardous drinking. Participants with any lifetime history of abstinence were excluded from analyses and there is a lack of detail in how this was operationalized in the current study, making it unclear how this may have affected the results. Future studies should test longitudinal models of hazardous drinking, gender self-concept, and minority stress among large LGBTQ+ samples, to establish temporal associations. At the same time, research should also focus on developing and testing clinical and public health approaches to remedy alcohol use inequities.
For policy makers: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. Making information available to the public to correct inaccurate perceptions of drinking norms could help individuals drink less and experience fewer alcohol problems. In order to provide accurate information about actual drinking norms, national health surveys need well validated measures of sexual orientation, gender identity, and alcohol use.
Disparities in alcohol use between LGBTQ+ and heterosexual populations, may be due, in part, to the stigmatization and subsequent stigma-related stressors (“minority stress”) LGBTQ+ people face.
The stigmatization of LGBTQ+ people is based in heterosexual hegemony (sometimes referred to as ‘heteronormativity’ or ‘cisnormativity’), that collapse gender into a single binary that ties sex/gender/sexuality together, whereby a person’s sex assigned at birth is either assumed to be female or male, which is then assumed to determine a person’s gender and sexuality. This plays out in society through routines deemed acceptable (considered the default or the “norm”) – for example, people assigned female sex at birth are presumed to identify as women (sex and gender identity), women are presumed to dress in a feminine way (gender expression/presentation), and women are presumed to be attracted to men (sexuality). This intersection of heterosexism, sexism, and misogyny is particularly relevant for lesbian and bisexual women, who may more commonly adopt a more masculine presenting appearance or social role than heterosexual women.
While gender nonconformity among lesbian and bisexual women could carry important implications for the visibility of their stigmatized sexual identity, and subsequent experience and coping with minority stress (e.g., alcohol use), masculinity may also influence alcohol-use norms and exposure to heavy drinking venues. Among heterosexual individuals, higher levels of masculinity are associated with greater alcohol consumption among men and women, but there is still much to learn in this regard.
Taken together, the researchers wanted to know, among lesbian and bisexual women, is more masculinity associated with greater hazardous drinking, and greater femininity associated with lower hazardous drinking? Are these differences actually accounted for by differences in minority stress? The thought is that by understanding more about the factors underlying lesbian and bisexual women’s hazardous drinking, more helpful treatment and policy approaches could be developed to reduce harms in this at-risk group.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional analysis of wave 3 data (2010-2012) from a 22-year longitudinal cohort study of sexual minority women. Nearly 600 lesbian and bisexual women living in the Chicago area (N = 598) answered questions at a single time point about their gender identity and expression (masculinity and femininity), past year experiences of minority stress (discrimination, awareness/expectation, and internalized), and past year alcohol use, alcohol-related problems, and alcohol use disorder symptoms.
Participants were included in this study if they identified as lesbian, mostly lesbian, or bisexual, were age 18 or older, fluent in English, and lived in the Chicago metropolitan area. For this analysis, the researchers excluded participants if they reported lifetime or past 12-month abstinence from alcohol.
The researchers asked participants, “How often did you have 6 or more drinks of wine, beer, or liquor in a single day?” and “About how many drinks would you have on a typical day when you drank?” Participants who reported consuming ≥ 6 drinks on one or more days in the past 12 months or if they reported consuming ≥ 4 drinks on a typical drinking day were classified as experiencing “any heavy episodic drinking” (hereafter referred to simply as “heavy drinking”).
To assess alcohol-related problems, participants were given a list of 8 negative consequences related to drinking, such as driving a car while intoxicated or fights with their partner or other people when drinking and asked if any of the events on the list had happened to them in the past 12 months. Participants were classified based on whether they reported at least one alcohol-related problem.
To assess potential symptoms of alcohol use disorder (based on DSM-IV alcohol dependence criteria), participants were asked if they had experienced any one of a list of 5 symptoms in the previous 12 months, such as inability to stop drinking before becoming intoxicated and inability to stop or cut down on drinking over time. Participants were classified as “any” or “no symptoms reported.”
For gender identity, participants were asked on a scale from 1 to 7, “In general, how masculine do you think you are?” and “In general, how feminine do you think you are?” For gender expression, participants were asked, “How masculine do you act, appear, and come across to others?” and “How feminine do you act, appear, and come across to others?” Responses were categorized as “not at all/very little” (1–2), “moderately” (3–5), and “extremely” (6–7).
Three different questionnaires validated in prior research were used to measure minority stress in the past 12 months: discrimination, stigma awareness and sensitivity, and internalized stigma.
The analyses tested the association between participants’ gender identity and expression (masculine and feminine) and alcohol outcomes (heavy drinking, alcohol problems, alcohol use disorder symptoms), while accounting for participants minority stress (discrimination, stigma awareness and sensitivity, and internalized stigma), as well as participant characteristics (age, race/ethnicity, sexual identity, and education). This allowed the researchers to examine if gender expression or minority stress was a greater influence on drinking, while accounting for demographic characteristics that could also influence drinking (e.g., younger individuals tend to have higher rates of heavy episodic drinking compared to older individuals).
There was a relatively equal number of participants across young, middle, and older age, with an average age of 39 years. About 1/3 of the sample identified as Black/African American, 1/3 Hispanic/Latinx, and 1/3 White, non-Hispanic. A majority of participants (74%) identified as lesbian or mostly lesbian. 50% of participants believed others viewed them as moderately masculine, and 62% reported their self-perceived gender identity as moderately masculine. Femininity was similar with 55% of participants reporting moderately feminine self-perceived gender identity and 51% reporting a belief that other people viewed them as moderately feminine.
WHAT DID THIS STUDY FIND?
Masculine lesbian and bisexual women reported greater drinking alcohol problems, and alcohol use disorder symptoms.
Lesbian and bisexual women who perceived themselves as extremely masculine were 2 times more likely to experience at least one episode of heavy drinking over the past year, compared to women who described themselves as not at all masculine. Masculine lesbian and bisexual women were also 3 times more likely to have at least one symptom of alcohol use disorder. Ratings of femininity were not associated with alcohol outcomes.
Minority stress was not associated with alcohol outcomes when accounting for gender self-concept.
None of the minority stress variables (identity-based discrimination, stigma sensitivity/awareness, internalized stigma) were significantly associated with any of the hazardous drinking outcomes (heavy drinking, alcohol problems, alcohol use disorder symptoms) in these models, nor did they impact the association between gender expression and hazardous drinking.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this survey of lesbian and bisexual women living in the Chicago greater area, masculinity, in particular masculine gender expression, was associated with hazardous drinking. This association was not explained by minority stress as the research team had predicted.
The researchers had good theoretical reasons to believe that minority stress could play a role in greater drinking outcomes among lesbian and bisexual women through gender nonconformity; however, this was not supported in the current study.
This is surprising, given that other research has found an association between minority stress, drinking, and alcohol problems, such as among MSM living with HIV. For some lesbian and bisexual women, gender nonconformity may be protective against minority stress-related risk for hazardous drinking. For example, gender nonconformity is associated with greater connectedness with other lesbians and bisexual women, which can bolster social support, and may buffer against negative minority stress-related health outcomes. Conversely, in this sample, it appears that perhaps gender nonconformity and perceptions of gender-related drinking norms played a larger role in reported drinking and related problems.
Bisexual women in this study had greater odds of alcohol use disorder symptoms than lesbian women. This is consistent with a national study of adults with alcohol use disorder, where bisexual participants, among gay and lesbian participants as well, had more severe alcohol use disorder symptoms and more co-morbid drug use and mood disorders compared to heterosexual participants. Bisexual individuals were also much more likely to seek help for alcohol use disorder across treatment venues compared to heterosexual, gay, and lesbian individuals, whereas there were no differences in help-seeking between gay, lesbian, and heterosexual participants. As mentioned above, community connection may buffer against minority stress, and bisexual women may not feel as much a part of the lesbian community due to stigma (i.e., monosexism – a presumption that everyone is, or should be, attracted to no more than one gender) that permeates the LGBTQ+ community as well as heterosexism outside the community, which may relate to worse mental health symptoms, greater alcohol use, and increased help-seeking. In other words, bisexual women may feel greater stress as they may not feel fully accepted in either the LGBTQ+ community, nor by heterosexual individuals.
Rates of alcohol use disorder in the U.S. have been higher among men, and decades of research has examined the biological and social mechanisms for these differences. One difference, simply put, is that men tend to drink more frequently and in greater quantities than women do. In recent years, in general, men still consume more alcohol and experience and cause more alcohol-related injuries and deaths than women do, but the gaps are narrowing. This has put additional attention on social factors that could influence drinking differences between men and women, rather than biological sex factors alone. For example, in a large sample of college students, masculine gender-orientation was positively associated with heavy episodic drinking, regardless of sex. This suggests potentially a perception or social norm that associates masculinity with heavier drinking.
Research on heavy drinking among college students also points to the effects of social norms, whereby college students’ drinking is influenced by perceptions of how their peers drink, and these perceptions are often incorrect, overestimating peer drinking norms. If inaccurate perceptions can be corrected, young people may drink less. Similarly, if inaccurate perceptions about masculinity and drinking can be corrected, individuals with a more masculine gender-orientation may drink less as well. Early innovative research is being conducted in this area, testing app-delivered social norms interventions specifically for lesbian and bisexual women.
Social norms interventions are meant to correct this misperception by providing information about actual student drinking norms and personalized feedback comparing actual student drinking patterns and perceptions of the norm, pointing out discrepancies. In order to effectively provide such an intervention for lesbian and bisexual women, we need accurate population-level data of LGBTQ+-identified individuals and their drinking, and not all national health surveys measure sexual orientation and gender identity information well, or at all. That aside, social norms interventions only have some evidence supporting their effectiveness to reduce drinking and related problems and should be combined with other evidence-supported interventions to reduce drinking, as they are not considered effective enough on their own to reduce alcohol use or misuse among college students over the long-term.
It is notable in this study that indicators of hazardous drinking were measured at a relatively low threshold – participants only needed to endorse one instance of heavy episodic drinking, an alcohol-related problem, or one alcohol use disorder symptom in the past year to be included in the hazardous drinking category. Additionally, individuals who had periods of abstinence were excluded from these analyses, which may have excluded individuals with more severe alcohol problems and alcohol use disorder symptoms seeking or engaging in treatment. This may have also contributed to the lack of association between minority stress and alcohol outcomes when accounting for gender self-concept: if participants with more severe alcohol problems also had greater minority stress and were potentially excluded from analyses because of any attempt or period of abstinence, this could have limited the range and severity of minority stress experienced in this sample. Indeed, participants in this study reported an average of 1 experience of sexual identity-based discrimination in the past year. However, the researchers did not report minority stress scores of participants excluded in the study, so ultimately it is unknown how including participants with periods of abstinence could have affected the association between minority stress and alcohol outcomes.
The threshold for hazardous drinking in the current study was quite low, meaning that the researchers categorized any endorsement of drinking 6 or more drinks on a single occasion in the last 12 months as heavy episodic drinking. These criteria are also based on older drinking limit recommendations from the NIAAA, which have been updated since the data were collected. The researchers accounted for this change by also counting participants who indicated they drank 4 or more drinks on a typical drinking day. This means that participants who drink very infrequently but in higher amounts were categorized the same as participants who were regularly drinking more than 7 drinks per week. This is reflected in their analyses showing that participants aged 18-29 were more likely to have any heavy episodic drinking, where high drinking quantity but lower frequency is more common. Although there are health risks (e.g., accidents and injuries) associated with drinking 4 or more drinks on any occasion for women, it may not be indicative of alcohol misuse if very infrequent, whereas alcohol-related problems or symptoms of alcohol use disorder may be better indicators.
Participants with prior abstinence were not included in these analyses, and the researchers did not provide detailed information on how this was measured. This means that participants could have been excluded who had periods of abstinence for other medical reasons or life stage events, such as pregnancy. It may have also excluded participants seeking or involved in alcohol treatment. This could have unknown effects on their analyses, in particular related to conclusions about minority stress and the lack of association with hazardous drinking. It is possible that participants who experienced greater minority stress also had greater problems and attempts/periods of abstinence, which would have excluded them from these analyses.
The researchers chose to dichotomize their outcome measures, which limited their statistical power to run additional interaction analyses, even though they had a relatively very large sample of lesbian and bisexual women. It’s possible the researchers used dichotomous outcomes for ease in interpretation of the results; however, they may have had more power to run additional interaction analyses between gender self-concept and other demographic characteristics, like sexual orientation and race/ethnicity if they had left the measures on a more continuous, interval-level, scale.
BOTTOM LINE
This study found that, among a large sample of nearly 600 lesbian and bisexual women in the Chicago area, masculine gender expression was associated with a greater likelihood of reporting at least one indicator hazardous drinking, and minority stress did not explain this association. This may mean that social norms associated with masculinity and drinking may be a risk factor for hazardous use, and that alcohol interventions could be tailored to address perceptions of social drinking norms.
For individuals and families seeking recovery: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. If we work to decouple the perception that heavy drinking is a masculine behavior, masculine individuals may drink less and experience fewer alcohol problems.
For treatment professionals and treatment systems: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. For some individuals drinking at risky levels or seeking alcohol treatment, it may be important to correct inaccurate perceptions of gendered drinking norms. For LGBTQ+ individuals with a more masculine gender self-concept, working to decouple the perception that heavy drinking is a masculine behavior may increase motivation to reduce drinking.
For scientists: Findings from this cross-sectional analysis of wave 3 data (2010-2012) from a 22-year longitudinal cohort study of sexual minority women in the Chicago area found that lesbian and bisexual women with greater masculine gender expression had a 2-3xs greater odds of having any instance of heavy episodic drinking, one or more alcohol problem, and one or more alcohol use disorder symptom in the past 12 months, controlling for minority stress (identity-based discrimination, stigma sensitivity and awareness, and internalized stigma) and demographics (age, race/ethnicity, sexual identity, and education). Contrary to hypotheses, minority stress was not significantly associated with indicators of hazardous drinking in models accounting for gender self-concept and demographic characteristics, nor influenced the association between gender self-concept and hazardous drinking. Participants with any lifetime history of abstinence were excluded from analyses and there is a lack of detail in how this was operationalized in the current study, making it unclear how this may have affected the results. Future studies should test longitudinal models of hazardous drinking, gender self-concept, and minority stress among large LGBTQ+ samples, to establish temporal associations. At the same time, research should also focus on developing and testing clinical and public health approaches to remedy alcohol use inequities.
For policy makers: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. Making information available to the public to correct inaccurate perceptions of drinking norms could help individuals drink less and experience fewer alcohol problems. In order to provide accurate information about actual drinking norms, national health surveys need well validated measures of sexual orientation, gender identity, and alcohol use.
Disparities in alcohol use between LGBTQ+ and heterosexual populations, may be due, in part, to the stigmatization and subsequent stigma-related stressors (“minority stress”) LGBTQ+ people face.
The stigmatization of LGBTQ+ people is based in heterosexual hegemony (sometimes referred to as ‘heteronormativity’ or ‘cisnormativity’), that collapse gender into a single binary that ties sex/gender/sexuality together, whereby a person’s sex assigned at birth is either assumed to be female or male, which is then assumed to determine a person’s gender and sexuality. This plays out in society through routines deemed acceptable (considered the default or the “norm”) – for example, people assigned female sex at birth are presumed to identify as women (sex and gender identity), women are presumed to dress in a feminine way (gender expression/presentation), and women are presumed to be attracted to men (sexuality). This intersection of heterosexism, sexism, and misogyny is particularly relevant for lesbian and bisexual women, who may more commonly adopt a more masculine presenting appearance or social role than heterosexual women.
While gender nonconformity among lesbian and bisexual women could carry important implications for the visibility of their stigmatized sexual identity, and subsequent experience and coping with minority stress (e.g., alcohol use), masculinity may also influence alcohol-use norms and exposure to heavy drinking venues. Among heterosexual individuals, higher levels of masculinity are associated with greater alcohol consumption among men and women, but there is still much to learn in this regard.
Taken together, the researchers wanted to know, among lesbian and bisexual women, is more masculinity associated with greater hazardous drinking, and greater femininity associated with lower hazardous drinking? Are these differences actually accounted for by differences in minority stress? The thought is that by understanding more about the factors underlying lesbian and bisexual women’s hazardous drinking, more helpful treatment and policy approaches could be developed to reduce harms in this at-risk group.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional analysis of wave 3 data (2010-2012) from a 22-year longitudinal cohort study of sexual minority women. Nearly 600 lesbian and bisexual women living in the Chicago area (N = 598) answered questions at a single time point about their gender identity and expression (masculinity and femininity), past year experiences of minority stress (discrimination, awareness/expectation, and internalized), and past year alcohol use, alcohol-related problems, and alcohol use disorder symptoms.
Participants were included in this study if they identified as lesbian, mostly lesbian, or bisexual, were age 18 or older, fluent in English, and lived in the Chicago metropolitan area. For this analysis, the researchers excluded participants if they reported lifetime or past 12-month abstinence from alcohol.
The researchers asked participants, “How often did you have 6 or more drinks of wine, beer, or liquor in a single day?” and “About how many drinks would you have on a typical day when you drank?” Participants who reported consuming ≥ 6 drinks on one or more days in the past 12 months or if they reported consuming ≥ 4 drinks on a typical drinking day were classified as experiencing “any heavy episodic drinking” (hereafter referred to simply as “heavy drinking”).
To assess alcohol-related problems, participants were given a list of 8 negative consequences related to drinking, such as driving a car while intoxicated or fights with their partner or other people when drinking and asked if any of the events on the list had happened to them in the past 12 months. Participants were classified based on whether they reported at least one alcohol-related problem.
To assess potential symptoms of alcohol use disorder (based on DSM-IV alcohol dependence criteria), participants were asked if they had experienced any one of a list of 5 symptoms in the previous 12 months, such as inability to stop drinking before becoming intoxicated and inability to stop or cut down on drinking over time. Participants were classified as “any” or “no symptoms reported.”
For gender identity, participants were asked on a scale from 1 to 7, “In general, how masculine do you think you are?” and “In general, how feminine do you think you are?” For gender expression, participants were asked, “How masculine do you act, appear, and come across to others?” and “How feminine do you act, appear, and come across to others?” Responses were categorized as “not at all/very little” (1–2), “moderately” (3–5), and “extremely” (6–7).
Three different questionnaires validated in prior research were used to measure minority stress in the past 12 months: discrimination, stigma awareness and sensitivity, and internalized stigma.
The analyses tested the association between participants’ gender identity and expression (masculine and feminine) and alcohol outcomes (heavy drinking, alcohol problems, alcohol use disorder symptoms), while accounting for participants minority stress (discrimination, stigma awareness and sensitivity, and internalized stigma), as well as participant characteristics (age, race/ethnicity, sexual identity, and education). This allowed the researchers to examine if gender expression or minority stress was a greater influence on drinking, while accounting for demographic characteristics that could also influence drinking (e.g., younger individuals tend to have higher rates of heavy episodic drinking compared to older individuals).
There was a relatively equal number of participants across young, middle, and older age, with an average age of 39 years. About 1/3 of the sample identified as Black/African American, 1/3 Hispanic/Latinx, and 1/3 White, non-Hispanic. A majority of participants (74%) identified as lesbian or mostly lesbian. 50% of participants believed others viewed them as moderately masculine, and 62% reported their self-perceived gender identity as moderately masculine. Femininity was similar with 55% of participants reporting moderately feminine self-perceived gender identity and 51% reporting a belief that other people viewed them as moderately feminine.
WHAT DID THIS STUDY FIND?
Masculine lesbian and bisexual women reported greater drinking alcohol problems, and alcohol use disorder symptoms.
Lesbian and bisexual women who perceived themselves as extremely masculine were 2 times more likely to experience at least one episode of heavy drinking over the past year, compared to women who described themselves as not at all masculine. Masculine lesbian and bisexual women were also 3 times more likely to have at least one symptom of alcohol use disorder. Ratings of femininity were not associated with alcohol outcomes.
Minority stress was not associated with alcohol outcomes when accounting for gender self-concept.
None of the minority stress variables (identity-based discrimination, stigma sensitivity/awareness, internalized stigma) were significantly associated with any of the hazardous drinking outcomes (heavy drinking, alcohol problems, alcohol use disorder symptoms) in these models, nor did they impact the association between gender expression and hazardous drinking.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this survey of lesbian and bisexual women living in the Chicago greater area, masculinity, in particular masculine gender expression, was associated with hazardous drinking. This association was not explained by minority stress as the research team had predicted.
The researchers had good theoretical reasons to believe that minority stress could play a role in greater drinking outcomes among lesbian and bisexual women through gender nonconformity; however, this was not supported in the current study.
This is surprising, given that other research has found an association between minority stress, drinking, and alcohol problems, such as among MSM living with HIV. For some lesbian and bisexual women, gender nonconformity may be protective against minority stress-related risk for hazardous drinking. For example, gender nonconformity is associated with greater connectedness with other lesbians and bisexual women, which can bolster social support, and may buffer against negative minority stress-related health outcomes. Conversely, in this sample, it appears that perhaps gender nonconformity and perceptions of gender-related drinking norms played a larger role in reported drinking and related problems.
Bisexual women in this study had greater odds of alcohol use disorder symptoms than lesbian women. This is consistent with a national study of adults with alcohol use disorder, where bisexual participants, among gay and lesbian participants as well, had more severe alcohol use disorder symptoms and more co-morbid drug use and mood disorders compared to heterosexual participants. Bisexual individuals were also much more likely to seek help for alcohol use disorder across treatment venues compared to heterosexual, gay, and lesbian individuals, whereas there were no differences in help-seeking between gay, lesbian, and heterosexual participants. As mentioned above, community connection may buffer against minority stress, and bisexual women may not feel as much a part of the lesbian community due to stigma (i.e., monosexism – a presumption that everyone is, or should be, attracted to no more than one gender) that permeates the LGBTQ+ community as well as heterosexism outside the community, which may relate to worse mental health symptoms, greater alcohol use, and increased help-seeking. In other words, bisexual women may feel greater stress as they may not feel fully accepted in either the LGBTQ+ community, nor by heterosexual individuals.
Rates of alcohol use disorder in the U.S. have been higher among men, and decades of research has examined the biological and social mechanisms for these differences. One difference, simply put, is that men tend to drink more frequently and in greater quantities than women do. In recent years, in general, men still consume more alcohol and experience and cause more alcohol-related injuries and deaths than women do, but the gaps are narrowing. This has put additional attention on social factors that could influence drinking differences between men and women, rather than biological sex factors alone. For example, in a large sample of college students, masculine gender-orientation was positively associated with heavy episodic drinking, regardless of sex. This suggests potentially a perception or social norm that associates masculinity with heavier drinking.
Research on heavy drinking among college students also points to the effects of social norms, whereby college students’ drinking is influenced by perceptions of how their peers drink, and these perceptions are often incorrect, overestimating peer drinking norms. If inaccurate perceptions can be corrected, young people may drink less. Similarly, if inaccurate perceptions about masculinity and drinking can be corrected, individuals with a more masculine gender-orientation may drink less as well. Early innovative research is being conducted in this area, testing app-delivered social norms interventions specifically for lesbian and bisexual women.
Social norms interventions are meant to correct this misperception by providing information about actual student drinking norms and personalized feedback comparing actual student drinking patterns and perceptions of the norm, pointing out discrepancies. In order to effectively provide such an intervention for lesbian and bisexual women, we need accurate population-level data of LGBTQ+-identified individuals and their drinking, and not all national health surveys measure sexual orientation and gender identity information well, or at all. That aside, social norms interventions only have some evidence supporting their effectiveness to reduce drinking and related problems and should be combined with other evidence-supported interventions to reduce drinking, as they are not considered effective enough on their own to reduce alcohol use or misuse among college students over the long-term.
It is notable in this study that indicators of hazardous drinking were measured at a relatively low threshold – participants only needed to endorse one instance of heavy episodic drinking, an alcohol-related problem, or one alcohol use disorder symptom in the past year to be included in the hazardous drinking category. Additionally, individuals who had periods of abstinence were excluded from these analyses, which may have excluded individuals with more severe alcohol problems and alcohol use disorder symptoms seeking or engaging in treatment. This may have also contributed to the lack of association between minority stress and alcohol outcomes when accounting for gender self-concept: if participants with more severe alcohol problems also had greater minority stress and were potentially excluded from analyses because of any attempt or period of abstinence, this could have limited the range and severity of minority stress experienced in this sample. Indeed, participants in this study reported an average of 1 experience of sexual identity-based discrimination in the past year. However, the researchers did not report minority stress scores of participants excluded in the study, so ultimately it is unknown how including participants with periods of abstinence could have affected the association between minority stress and alcohol outcomes.
The threshold for hazardous drinking in the current study was quite low, meaning that the researchers categorized any endorsement of drinking 6 or more drinks on a single occasion in the last 12 months as heavy episodic drinking. These criteria are also based on older drinking limit recommendations from the NIAAA, which have been updated since the data were collected. The researchers accounted for this change by also counting participants who indicated they drank 4 or more drinks on a typical drinking day. This means that participants who drink very infrequently but in higher amounts were categorized the same as participants who were regularly drinking more than 7 drinks per week. This is reflected in their analyses showing that participants aged 18-29 were more likely to have any heavy episodic drinking, where high drinking quantity but lower frequency is more common. Although there are health risks (e.g., accidents and injuries) associated with drinking 4 or more drinks on any occasion for women, it may not be indicative of alcohol misuse if very infrequent, whereas alcohol-related problems or symptoms of alcohol use disorder may be better indicators.
Participants with prior abstinence were not included in these analyses, and the researchers did not provide detailed information on how this was measured. This means that participants could have been excluded who had periods of abstinence for other medical reasons or life stage events, such as pregnancy. It may have also excluded participants seeking or involved in alcohol treatment. This could have unknown effects on their analyses, in particular related to conclusions about minority stress and the lack of association with hazardous drinking. It is possible that participants who experienced greater minority stress also had greater problems and attempts/periods of abstinence, which would have excluded them from these analyses.
The researchers chose to dichotomize their outcome measures, which limited their statistical power to run additional interaction analyses, even though they had a relatively very large sample of lesbian and bisexual women. It’s possible the researchers used dichotomous outcomes for ease in interpretation of the results; however, they may have had more power to run additional interaction analyses between gender self-concept and other demographic characteristics, like sexual orientation and race/ethnicity if they had left the measures on a more continuous, interval-level, scale.
BOTTOM LINE
This study found that, among a large sample of nearly 600 lesbian and bisexual women in the Chicago area, masculine gender expression was associated with a greater likelihood of reporting at least one indicator hazardous drinking, and minority stress did not explain this association. This may mean that social norms associated with masculinity and drinking may be a risk factor for hazardous use, and that alcohol interventions could be tailored to address perceptions of social drinking norms.
For individuals and families seeking recovery: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. If we work to decouple the perception that heavy drinking is a masculine behavior, masculine individuals may drink less and experience fewer alcohol problems.
For treatment professionals and treatment systems: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. For some individuals drinking at risky levels or seeking alcohol treatment, it may be important to correct inaccurate perceptions of gendered drinking norms. For LGBTQ+ individuals with a more masculine gender self-concept, working to decouple the perception that heavy drinking is a masculine behavior may increase motivation to reduce drinking.
For scientists: Findings from this cross-sectional analysis of wave 3 data (2010-2012) from a 22-year longitudinal cohort study of sexual minority women in the Chicago area found that lesbian and bisexual women with greater masculine gender expression had a 2-3xs greater odds of having any instance of heavy episodic drinking, one or more alcohol problem, and one or more alcohol use disorder symptom in the past 12 months, controlling for minority stress (identity-based discrimination, stigma sensitivity and awareness, and internalized stigma) and demographics (age, race/ethnicity, sexual identity, and education). Contrary to hypotheses, minority stress was not significantly associated with indicators of hazardous drinking in models accounting for gender self-concept and demographic characteristics, nor influenced the association between gender self-concept and hazardous drinking. Participants with any lifetime history of abstinence were excluded from analyses and there is a lack of detail in how this was operationalized in the current study, making it unclear how this may have affected the results. Future studies should test longitudinal models of hazardous drinking, gender self-concept, and minority stress among large LGBTQ+ samples, to establish temporal associations. At the same time, research should also focus on developing and testing clinical and public health approaches to remedy alcohol use inequities.
For policy makers: Lesbian and bisexual women report higher rates of hazardous drinking compared to heterosexual women. In this study, lesbian and bisexual women with more masculine gender expressions were 2-3xs more likely to experience at least one alcohol problem or alcohol use disorder symptom, which may be related to perceptions of masculinity and social alcohol use norms. Making information available to the public to correct inaccurate perceptions of drinking norms could help individuals drink less and experience fewer alcohol problems. In order to provide accurate information about actual drinking norms, national health surveys need well validated measures of sexual orientation, gender identity, and alcohol use.