Sexual minorities and women veterans die younger than straight veterans due to alcohol use
Lesbian, gay, and bisexual (LGB) veterans die younger than heterosexual veterans due to alcohol related harms. This study investigated specific alcohol harms and whether this disproportionate burden experienced by LGB veterans is more prominent in certain harms versus others.
This study was a follow-up to an already published analysis of Veteran’s Health Administration electronic health record data. People included in the analysis (N=5,402,606) were veteran patients enrolled in the Veteran’s Health Administration between October 1999 and July 2019. Veterans were classified as LGB based on a validated machine learning-based language processing computer program designed to scan written electronic health records. Veterans without text documentation who had one or more administrative code indicating sexual minority orientation (e.g., diagnosis code Z72.52 [High risk homosexual behavior]) were also included. This resulted in a cohort of 102,085 LGB veterans. All veterans who did not have documentation of LGB identity/behavior in text or codes comprised the heterosexual cohort (n = 5,300,521).
The research team measured alcohol consumption via scores of a modified version of the Alcohol Use Disorder Identification Test (AUDIT-C) contained within veterans’ electronic medical records. If a person had multiple AUDIT-C scores, the researchers selected one at random. AUDIT-C scores range from 0 (no past year alcohol use) to 12 (daily heavy drinking in the past year). AUDIT-C items were used to estimate average drinks per day. These scores were then used to group veterans into birth-sex-specific drinking cut-offs: no, low, medium, and high alcohol use.
The researchers examined whether years of potential life lost for each alcohol attributable death differed as a function of sexual identity and gender. The four sexual identity/gender groups were: heterosexual men (referent), heterosexual women, LGB men, and LGB women. The researchers also ranked the top ten alcohol-related deaths for these groups. Causes of death were then compared across groups to determine if there were differences in harms across sexual identity and gender (i.e., if some groups were more vulnerable to certain harms than others).
WHAT DID THIS STUDY FIND?
LGB veterans died of alcohol-related health issues younger than heterosexual veterans.
LGB veterans were more likely to die due to alcohol and died earlier than heterosexual veterans. For example, alcohol-related liver disease was the top cause of alcohol attributable death for all veterans, but the age at which veterans died of this condition varied across birth sexes and sexual orientation. LGB and heterosexual men died due to alcohol liver disease, on average at ages 57.5 and 62.8 (19 and 24 years younger than expected), and LGB and heterosexual women died at ages 50.4 and 53.8 respectively (32 and 35 years younger than expected).
LGB male and all female veterans were more likely to die suddenly due to alcohol relative to heterosexual men.
LGB male and all female veterans were more likely to die due to acute alcohol attributable deaths (e.g., alcohol related deaths that happened suddenly) compared to heterosexual men. For instance, suicide was the third most common cause of death among LGB male and all female veterans.
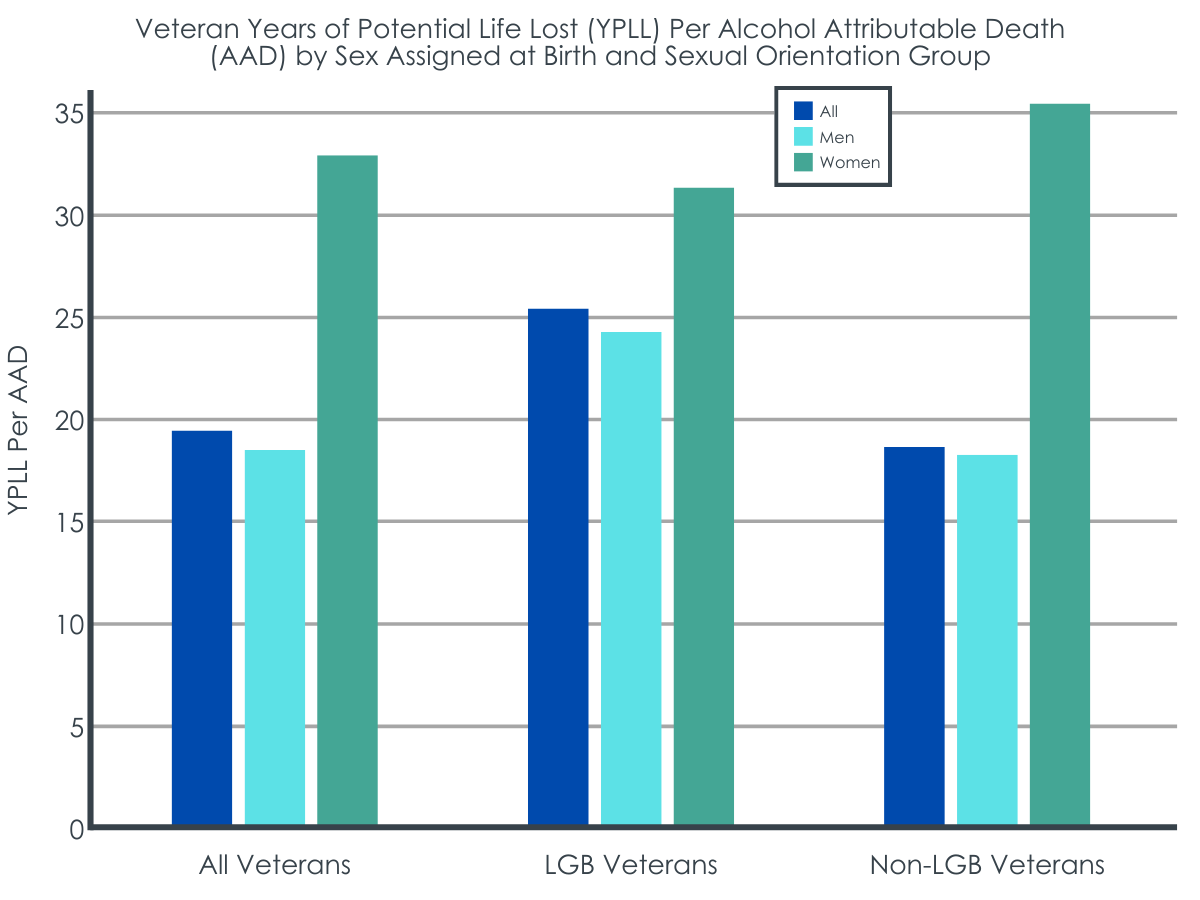
LGB male and all female veterans had higher years of potential life lost relative to heterosexual men.
When adjusted for age (US-based men and women have a calculated life expectancies of 76.2 and 81.2 respectively) LGB male and all female veterans were more likely to die earlier and suddenly because of alcohol. This combination of factors contributed to these veterans missing more potential years of life. For example, LGB males and all females died from sudden alcohol poisoning at ages 46.8, 46.1, and 43.6 years of age, respectively. By comparison, heterosexual males died to alcohol poisoning at age 49.1.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the etiology of alcohol-related diseases (from hazardous alcohol use to alcohol use disorders, to resultant disease [e.g., cirrhosis], and ultimately death) may occur faster among veteran women and LGB men relative to heterosexual male veterans.
The researchers found that although alcohol had a universally negative health effect, LGB male and all female veterans were more impacted earlier in life by alcohol’s health effects than heterosexual male veterans. LGB males and all females died due to alcohol at younger ages than heterosexual males. In addition, these deaths were often due to violence (e.g., suicide) or quickly developing conditions (e.g., alcohol poisoning). Together these findings suggest that the progression from hazardous alcohol use to harms may be accelerated among LGB men and women veterans. Previous research does suggest that sex assigned at birth impacts alcohol liver disease etiology, however, it is unclear how the intersection of sexual orientation and sex assigned at birth impacts this relationship.
The results of this work also highlight an opportunity for Veterans Health Administration services to more effectively address female and LGB veterans’ needs. That is, although all sampled veterans had access to healthcare, there were notable health disparities between LGB/female and heterosexual male veterans. Particularly, the worse health outcomes among the sampled veterans may not have been due to lack of service utilization – another study conducted by the researchers suggests that LGB veterans access more healthcare services than heterosexual veterans. Findings here and from prior work suggest the notable alcohol-related health disparity among LGB and female Veterans may not be due to differences in service utilization but rather the lack of specific attention to LGB/women’s needs in those health care services.
Indeed, the present work suggests there is a need for interventions targeting LGB/female veterans’ hazardous alcohol use behavior. Specifically, the data suggest that LGB/female veterans may benefit from behavioral interventions earlier than heterosexual male veterans. Beyond this, however, the scope of the presented research precludes suggesting the best intervention strategies.
Research has been done testing alcohol interventions for veterans, however continued work is needed. Namely the previous study suggested female veterans did not benefit as much from the intervention as men, so more work is needed to determine how best to intervene on female veterans’ alcohol use. It is also unknown how many LGB veterans received the intervention, so it is unclear how LGB veterans would benefit from this treatment. It is critical for researchers to further investigate strategies to mitigate the alcohol-related disease morbidity/mortality among LGB/female veterans.
As the research team mentions, the AUDIT-C was used to estimate alcohol attributable deaths. This is a limitation because the AUDIT-C only captures past year drinking. Therefore, veterans who used to drink but had not in the year prior to their AUDIT-C assessment would be categorized as non-alcohol users in the analysis. This may have led to an underestimation of alcohol attributable deaths as the accumulated impact of lifetime hazardous drinking would not necessarily have been captured.
Also as mentioned by the research team, veterans were categorized as LGB solely based on providers’ documentation of patients’ sexual orientation in their medical record. This may have led to under reporting of the number of LGB individuals in Veterans Health Administration. In addition, criteria to be labeled as an LGB veteran included behavior in absence of self-identity (e.g., engaging in same-sex sexual behavior). This is problematic because sexual identity and behavior are not the same – same-sex sexual behavior does not necessarily denote an LGB identity. More importantly, evidence suggests that heterosexual identified individuals who engage in same-sex behavior tend to drink more and have more alcohol-related problems compared to self-identified LGB individuals. It is not possible to disaggregate veterans who identified as LGB from those who engaged in same-sex behavior but did not identify as LGB in this sample.
The current study does not have data on factors germane to health outcomes and treatment utilization. For instance, experiences of discrimination among LGB veterans have been shown to play an important role in health outcomes. A better understanding of the social forces impacting LGB veterans would offer insights into points of intervention for this community, but the present research lacks these data.
BOTTOM LINE
In this study, the researchers found that although there were notable universal negative alcohol-attributable health impacts overall, American LGB veterans and all female veterans died younger due to alcohol-related health issues compared to American male heterosexual veterans. Results of this research suggest that the progression from hazardous alcohol use to health problems may be accelerated among LGB men and women veterans. It is plausible that minority-related stress among female veterans and LGB veterans as well as and related stigma and discrimination among LGB individuals may increase vulnerability to health impacts, but there is a need to further investigate the factors responsible for this accelerated impact. In the interim, it is also critical to develop outreach strategies that decrease acute harms (e.g., alcohol poisoning) and chronic health problems (e.g., liver cirrhosis) due to alcohol with strategies tailored to the specific needs and experiences of LGB/female veterans.
For individuals and families seeking recovery: The present research does not provide data on treatment utilization, nor does it directly relate to treatment options for LGB veterans. As such it is difficult to make recommendations for those seeking recovery. That said, United States veterans are entitled to a wide range of substance use treatment options. Individuals interested in any of these services may want to discuss this with their physician.
For treatment professionals and treatment systems: It is unknown why sampled LGB/female veterans were disproportionately impacted by alcohol-related health disparities. One possible explanation could be that LGB/female veterans both suffer from minority-related stressors and stigma and discrimination stressors, and these aspects are not being addressed by the Veterans Health Administration. Those providing treatment to and/or work in healthcare system settings serving LGB/female veteran patients may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs.
For scientists:Scientists may continue to investigate the possible socio-environmental reasons for the observed alcohol-related health disparities. For instance, past research suggests that experiences of discrimination among LGB veterans play an important role in healthcare service utilization. Similarly, female veterans have reported that stigma has been a barrier to them receiving care from the Veterans Health Administration. By examining how discrimination/stigma impacts LGB/female veterans, researchers can make recommendations on developing intervention points to ensure LGB/female veterans’ needs are being met.
For policy makers: This study suggests that LGB/female veterans are experiencing more alcohol-related harms at earlier ages compared to heterosexual male veterans. Unfortunately, understanding why this phenomenon occurs is beyond the scope of this research. This makes it difficult to offer specific advice on how policymakers could reduce this alcohol-related health disparity. Until research offers empirical evidence to the cause of this health disparity, it may be helpful for policymakers to consider implementing guidelines to increase alcohol use screening among all veterans. That is, if LGB/female veterans are displaying alcohol-related harms at younger than expected ages, it may be prudent for providers to be especially diligent in assessing alcohol use and connecting patients to relevant treatment resources.
This study was a follow-up to an already published analysis of Veteran’s Health Administration electronic health record data. People included in the analysis (N=5,402,606) were veteran patients enrolled in the Veteran’s Health Administration between October 1999 and July 2019. Veterans were classified as LGB based on a validated machine learning-based language processing computer program designed to scan written electronic health records. Veterans without text documentation who had one or more administrative code indicating sexual minority orientation (e.g., diagnosis code Z72.52 [High risk homosexual behavior]) were also included. This resulted in a cohort of 102,085 LGB veterans. All veterans who did not have documentation of LGB identity/behavior in text or codes comprised the heterosexual cohort (n = 5,300,521).
The research team measured alcohol consumption via scores of a modified version of the Alcohol Use Disorder Identification Test (AUDIT-C) contained within veterans’ electronic medical records. If a person had multiple AUDIT-C scores, the researchers selected one at random. AUDIT-C scores range from 0 (no past year alcohol use) to 12 (daily heavy drinking in the past year). AUDIT-C items were used to estimate average drinks per day. These scores were then used to group veterans into birth-sex-specific drinking cut-offs: no, low, medium, and high alcohol use.
The researchers examined whether years of potential life lost for each alcohol attributable death differed as a function of sexual identity and gender. The four sexual identity/gender groups were: heterosexual men (referent), heterosexual women, LGB men, and LGB women. The researchers also ranked the top ten alcohol-related deaths for these groups. Causes of death were then compared across groups to determine if there were differences in harms across sexual identity and gender (i.e., if some groups were more vulnerable to certain harms than others).
WHAT DID THIS STUDY FIND?
LGB veterans died of alcohol-related health issues younger than heterosexual veterans.
LGB veterans were more likely to die due to alcohol and died earlier than heterosexual veterans. For example, alcohol-related liver disease was the top cause of alcohol attributable death for all veterans, but the age at which veterans died of this condition varied across birth sexes and sexual orientation. LGB and heterosexual men died due to alcohol liver disease, on average at ages 57.5 and 62.8 (19 and 24 years younger than expected), and LGB and heterosexual women died at ages 50.4 and 53.8 respectively (32 and 35 years younger than expected).
LGB male and all female veterans were more likely to die suddenly due to alcohol relative to heterosexual men.
LGB male and all female veterans were more likely to die due to acute alcohol attributable deaths (e.g., alcohol related deaths that happened suddenly) compared to heterosexual men. For instance, suicide was the third most common cause of death among LGB male and all female veterans.
LGB male and all female veterans had higher years of potential life lost relative to heterosexual men.
When adjusted for age (US-based men and women have a calculated life expectancies of 76.2 and 81.2 respectively) LGB male and all female veterans were more likely to die earlier and suddenly because of alcohol. This combination of factors contributed to these veterans missing more potential years of life. For example, LGB males and all females died from sudden alcohol poisoning at ages 46.8, 46.1, and 43.6 years of age, respectively. By comparison, heterosexual males died to alcohol poisoning at age 49.1.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the etiology of alcohol-related diseases (from hazardous alcohol use to alcohol use disorders, to resultant disease [e.g., cirrhosis], and ultimately death) may occur faster among veteran women and LGB men relative to heterosexual male veterans.
The researchers found that although alcohol had a universally negative health effect, LGB male and all female veterans were more impacted earlier in life by alcohol’s health effects than heterosexual male veterans. LGB males and all females died due to alcohol at younger ages than heterosexual males. In addition, these deaths were often due to violence (e.g., suicide) or quickly developing conditions (e.g., alcohol poisoning). Together these findings suggest that the progression from hazardous alcohol use to harms may be accelerated among LGB men and women veterans. Previous research does suggest that sex assigned at birth impacts alcohol liver disease etiology, however, it is unclear how the intersection of sexual orientation and sex assigned at birth impacts this relationship.
The results of this work also highlight an opportunity for Veterans Health Administration services to more effectively address female and LGB veterans’ needs. That is, although all sampled veterans had access to healthcare, there were notable health disparities between LGB/female and heterosexual male veterans. Particularly, the worse health outcomes among the sampled veterans may not have been due to lack of service utilization – another study conducted by the researchers suggests that LGB veterans access more healthcare services than heterosexual veterans. Findings here and from prior work suggest the notable alcohol-related health disparity among LGB and female Veterans may not be due to differences in service utilization but rather the lack of specific attention to LGB/women’s needs in those health care services.
Indeed, the present work suggests there is a need for interventions targeting LGB/female veterans’ hazardous alcohol use behavior. Specifically, the data suggest that LGB/female veterans may benefit from behavioral interventions earlier than heterosexual male veterans. Beyond this, however, the scope of the presented research precludes suggesting the best intervention strategies.
Research has been done testing alcohol interventions for veterans, however continued work is needed. Namely the previous study suggested female veterans did not benefit as much from the intervention as men, so more work is needed to determine how best to intervene on female veterans’ alcohol use. It is also unknown how many LGB veterans received the intervention, so it is unclear how LGB veterans would benefit from this treatment. It is critical for researchers to further investigate strategies to mitigate the alcohol-related disease morbidity/mortality among LGB/female veterans.
As the research team mentions, the AUDIT-C was used to estimate alcohol attributable deaths. This is a limitation because the AUDIT-C only captures past year drinking. Therefore, veterans who used to drink but had not in the year prior to their AUDIT-C assessment would be categorized as non-alcohol users in the analysis. This may have led to an underestimation of alcohol attributable deaths as the accumulated impact of lifetime hazardous drinking would not necessarily have been captured.
Also as mentioned by the research team, veterans were categorized as LGB solely based on providers’ documentation of patients’ sexual orientation in their medical record. This may have led to under reporting of the number of LGB individuals in Veterans Health Administration. In addition, criteria to be labeled as an LGB veteran included behavior in absence of self-identity (e.g., engaging in same-sex sexual behavior). This is problematic because sexual identity and behavior are not the same – same-sex sexual behavior does not necessarily denote an LGB identity. More importantly, evidence suggests that heterosexual identified individuals who engage in same-sex behavior tend to drink more and have more alcohol-related problems compared to self-identified LGB individuals. It is not possible to disaggregate veterans who identified as LGB from those who engaged in same-sex behavior but did not identify as LGB in this sample.
The current study does not have data on factors germane to health outcomes and treatment utilization. For instance, experiences of discrimination among LGB veterans have been shown to play an important role in health outcomes. A better understanding of the social forces impacting LGB veterans would offer insights into points of intervention for this community, but the present research lacks these data.
BOTTOM LINE
In this study, the researchers found that although there were notable universal negative alcohol-attributable health impacts overall, American LGB veterans and all female veterans died younger due to alcohol-related health issues compared to American male heterosexual veterans. Results of this research suggest that the progression from hazardous alcohol use to health problems may be accelerated among LGB men and women veterans. It is plausible that minority-related stress among female veterans and LGB veterans as well as and related stigma and discrimination among LGB individuals may increase vulnerability to health impacts, but there is a need to further investigate the factors responsible for this accelerated impact. In the interim, it is also critical to develop outreach strategies that decrease acute harms (e.g., alcohol poisoning) and chronic health problems (e.g., liver cirrhosis) due to alcohol with strategies tailored to the specific needs and experiences of LGB/female veterans.
For individuals and families seeking recovery: The present research does not provide data on treatment utilization, nor does it directly relate to treatment options for LGB veterans. As such it is difficult to make recommendations for those seeking recovery. That said, United States veterans are entitled to a wide range of substance use treatment options. Individuals interested in any of these services may want to discuss this with their physician.
For treatment professionals and treatment systems: It is unknown why sampled LGB/female veterans were disproportionately impacted by alcohol-related health disparities. One possible explanation could be that LGB/female veterans both suffer from minority-related stressors and stigma and discrimination stressors, and these aspects are not being addressed by the Veterans Health Administration. Those providing treatment to and/or work in healthcare system settings serving LGB/female veteran patients may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs.
For scientists:Scientists may continue to investigate the possible socio-environmental reasons for the observed alcohol-related health disparities. For instance, past research suggests that experiences of discrimination among LGB veterans play an important role in healthcare service utilization. Similarly, female veterans have reported that stigma has been a barrier to them receiving care from the Veterans Health Administration. By examining how discrimination/stigma impacts LGB/female veterans, researchers can make recommendations on developing intervention points to ensure LGB/female veterans’ needs are being met.
For policy makers: This study suggests that LGB/female veterans are experiencing more alcohol-related harms at earlier ages compared to heterosexual male veterans. Unfortunately, understanding why this phenomenon occurs is beyond the scope of this research. This makes it difficult to offer specific advice on how policymakers could reduce this alcohol-related health disparity. Until research offers empirical evidence to the cause of this health disparity, it may be helpful for policymakers to consider implementing guidelines to increase alcohol use screening among all veterans. That is, if LGB/female veterans are displaying alcohol-related harms at younger than expected ages, it may be prudent for providers to be especially diligent in assessing alcohol use and connecting patients to relevant treatment resources.
This study was a follow-up to an already published analysis of Veteran’s Health Administration electronic health record data. People included in the analysis (N=5,402,606) were veteran patients enrolled in the Veteran’s Health Administration between October 1999 and July 2019. Veterans were classified as LGB based on a validated machine learning-based language processing computer program designed to scan written electronic health records. Veterans without text documentation who had one or more administrative code indicating sexual minority orientation (e.g., diagnosis code Z72.52 [High risk homosexual behavior]) were also included. This resulted in a cohort of 102,085 LGB veterans. All veterans who did not have documentation of LGB identity/behavior in text or codes comprised the heterosexual cohort (n = 5,300,521).
The research team measured alcohol consumption via scores of a modified version of the Alcohol Use Disorder Identification Test (AUDIT-C) contained within veterans’ electronic medical records. If a person had multiple AUDIT-C scores, the researchers selected one at random. AUDIT-C scores range from 0 (no past year alcohol use) to 12 (daily heavy drinking in the past year). AUDIT-C items were used to estimate average drinks per day. These scores were then used to group veterans into birth-sex-specific drinking cut-offs: no, low, medium, and high alcohol use.
The researchers examined whether years of potential life lost for each alcohol attributable death differed as a function of sexual identity and gender. The four sexual identity/gender groups were: heterosexual men (referent), heterosexual women, LGB men, and LGB women. The researchers also ranked the top ten alcohol-related deaths for these groups. Causes of death were then compared across groups to determine if there were differences in harms across sexual identity and gender (i.e., if some groups were more vulnerable to certain harms than others).
WHAT DID THIS STUDY FIND?
LGB veterans died of alcohol-related health issues younger than heterosexual veterans.
LGB veterans were more likely to die due to alcohol and died earlier than heterosexual veterans. For example, alcohol-related liver disease was the top cause of alcohol attributable death for all veterans, but the age at which veterans died of this condition varied across birth sexes and sexual orientation. LGB and heterosexual men died due to alcohol liver disease, on average at ages 57.5 and 62.8 (19 and 24 years younger than expected), and LGB and heterosexual women died at ages 50.4 and 53.8 respectively (32 and 35 years younger than expected).
LGB male and all female veterans were more likely to die suddenly due to alcohol relative to heterosexual men.
LGB male and all female veterans were more likely to die due to acute alcohol attributable deaths (e.g., alcohol related deaths that happened suddenly) compared to heterosexual men. For instance, suicide was the third most common cause of death among LGB male and all female veterans.
LGB male and all female veterans had higher years of potential life lost relative to heterosexual men.
When adjusted for age (US-based men and women have a calculated life expectancies of 76.2 and 81.2 respectively) LGB male and all female veterans were more likely to die earlier and suddenly because of alcohol. This combination of factors contributed to these veterans missing more potential years of life. For example, LGB males and all females died from sudden alcohol poisoning at ages 46.8, 46.1, and 43.6 years of age, respectively. By comparison, heterosexual males died to alcohol poisoning at age 49.1.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that the etiology of alcohol-related diseases (from hazardous alcohol use to alcohol use disorders, to resultant disease [e.g., cirrhosis], and ultimately death) may occur faster among veteran women and LGB men relative to heterosexual male veterans.
The researchers found that although alcohol had a universally negative health effect, LGB male and all female veterans were more impacted earlier in life by alcohol’s health effects than heterosexual male veterans. LGB males and all females died due to alcohol at younger ages than heterosexual males. In addition, these deaths were often due to violence (e.g., suicide) or quickly developing conditions (e.g., alcohol poisoning). Together these findings suggest that the progression from hazardous alcohol use to harms may be accelerated among LGB men and women veterans. Previous research does suggest that sex assigned at birth impacts alcohol liver disease etiology, however, it is unclear how the intersection of sexual orientation and sex assigned at birth impacts this relationship.
The results of this work also highlight an opportunity for Veterans Health Administration services to more effectively address female and LGB veterans’ needs. That is, although all sampled veterans had access to healthcare, there were notable health disparities between LGB/female and heterosexual male veterans. Particularly, the worse health outcomes among the sampled veterans may not have been due to lack of service utilization – another study conducted by the researchers suggests that LGB veterans access more healthcare services than heterosexual veterans. Findings here and from prior work suggest the notable alcohol-related health disparity among LGB and female Veterans may not be due to differences in service utilization but rather the lack of specific attention to LGB/women’s needs in those health care services.
Indeed, the present work suggests there is a need for interventions targeting LGB/female veterans’ hazardous alcohol use behavior. Specifically, the data suggest that LGB/female veterans may benefit from behavioral interventions earlier than heterosexual male veterans. Beyond this, however, the scope of the presented research precludes suggesting the best intervention strategies.
Research has been done testing alcohol interventions for veterans, however continued work is needed. Namely the previous study suggested female veterans did not benefit as much from the intervention as men, so more work is needed to determine how best to intervene on female veterans’ alcohol use. It is also unknown how many LGB veterans received the intervention, so it is unclear how LGB veterans would benefit from this treatment. It is critical for researchers to further investigate strategies to mitigate the alcohol-related disease morbidity/mortality among LGB/female veterans.
As the research team mentions, the AUDIT-C was used to estimate alcohol attributable deaths. This is a limitation because the AUDIT-C only captures past year drinking. Therefore, veterans who used to drink but had not in the year prior to their AUDIT-C assessment would be categorized as non-alcohol users in the analysis. This may have led to an underestimation of alcohol attributable deaths as the accumulated impact of lifetime hazardous drinking would not necessarily have been captured.
Also as mentioned by the research team, veterans were categorized as LGB solely based on providers’ documentation of patients’ sexual orientation in their medical record. This may have led to under reporting of the number of LGB individuals in Veterans Health Administration. In addition, criteria to be labeled as an LGB veteran included behavior in absence of self-identity (e.g., engaging in same-sex sexual behavior). This is problematic because sexual identity and behavior are not the same – same-sex sexual behavior does not necessarily denote an LGB identity. More importantly, evidence suggests that heterosexual identified individuals who engage in same-sex behavior tend to drink more and have more alcohol-related problems compared to self-identified LGB individuals. It is not possible to disaggregate veterans who identified as LGB from those who engaged in same-sex behavior but did not identify as LGB in this sample.
The current study does not have data on factors germane to health outcomes and treatment utilization. For instance, experiences of discrimination among LGB veterans have been shown to play an important role in health outcomes. A better understanding of the social forces impacting LGB veterans would offer insights into points of intervention for this community, but the present research lacks these data.
BOTTOM LINE
In this study, the researchers found that although there were notable universal negative alcohol-attributable health impacts overall, American LGB veterans and all female veterans died younger due to alcohol-related health issues compared to American male heterosexual veterans. Results of this research suggest that the progression from hazardous alcohol use to health problems may be accelerated among LGB men and women veterans. It is plausible that minority-related stress among female veterans and LGB veterans as well as and related stigma and discrimination among LGB individuals may increase vulnerability to health impacts, but there is a need to further investigate the factors responsible for this accelerated impact. In the interim, it is also critical to develop outreach strategies that decrease acute harms (e.g., alcohol poisoning) and chronic health problems (e.g., liver cirrhosis) due to alcohol with strategies tailored to the specific needs and experiences of LGB/female veterans.
For individuals and families seeking recovery: The present research does not provide data on treatment utilization, nor does it directly relate to treatment options for LGB veterans. As such it is difficult to make recommendations for those seeking recovery. That said, United States veterans are entitled to a wide range of substance use treatment options. Individuals interested in any of these services may want to discuss this with their physician.
For treatment professionals and treatment systems: It is unknown why sampled LGB/female veterans were disproportionately impacted by alcohol-related health disparities. One possible explanation could be that LGB/female veterans both suffer from minority-related stressors and stigma and discrimination stressors, and these aspects are not being addressed by the Veterans Health Administration. Those providing treatment to and/or work in healthcare system settings serving LGB/female veteran patients may want to consider what barriers their patients face to receiving treatment. For instance, clinicians may find it helpful to ask their patients if they face challenges in receiving care and/or if they have unmet health needs.
For scientists:Scientists may continue to investigate the possible socio-environmental reasons for the observed alcohol-related health disparities. For instance, past research suggests that experiences of discrimination among LGB veterans play an important role in healthcare service utilization. Similarly, female veterans have reported that stigma has been a barrier to them receiving care from the Veterans Health Administration. By examining how discrimination/stigma impacts LGB/female veterans, researchers can make recommendations on developing intervention points to ensure LGB/female veterans’ needs are being met.
For policy makers: This study suggests that LGB/female veterans are experiencing more alcohol-related harms at earlier ages compared to heterosexual male veterans. Unfortunately, understanding why this phenomenon occurs is beyond the scope of this research. This makes it difficult to offer specific advice on how policymakers could reduce this alcohol-related health disparity. Until research offers empirical evidence to the cause of this health disparity, it may be helpful for policymakers to consider implementing guidelines to increase alcohol use screening among all veterans. That is, if LGB/female veterans are displaying alcohol-related harms at younger than expected ages, it may be prudent for providers to be especially diligent in assessing alcohol use and connecting patients to relevant treatment resources.