DO-MoST they can: Veterans’ views on alcohol interventions during medical-surgical care
There is a high, and often underreported, prevalence of adults receiving medical care that also engage in hazardous alcohol use. Yet, drinking can be an important determinant of medical-surgical outcomes. This study qualitatively explored how Veterans engaged in medical-surgical care felt about discussing their alcohol use and participating in a short, patient-led intervention. Providers’ views of existing barriers to medical-surgical patients’ alcohol care were also investigated.
The Veterans Administration (VA) is the largest integrated healthcare system in the U.S., providing services for over 5 million veterans annually. Alcohol use and alcohol use disorder are the most frequently misused substance and diagnosed substance use disorder among Veterans, which makes alcohol use a key issue for the VA. In general, alcohol use contributes to over 200 health conditions and injuries, including liver disease, cancer, and suicide. Veterans receiving medical-surgical care are a specific group of Veterans that may be negatively impacted by alcohol use more than others. Hazardous drinking and medical-surgical conditions are linked in three ways: hazardous drinking may 1) be a casual factor in developing a medical condition (e.g., alcohol-related liver disease), 2) exacerbate existing medical conditions (e.g., diabetes), and 3) complicate management of existing medical conditions (e.g., medication adherence, diet). Addressing drinking during medical-surgical care may directly and indirectly improve health among Veterans.
Significant efforts are underway to develop effective alcohol treatment and recovery options. For instance, the National Institute on Alcohol Abuse and Alcoholism has a 2023 budget exceeding $595 million, with millions going specifically to alcohol treatment research. However, Veterans tend to show different treatment and engagement patterns compared to non-Veterans. Tailored interventions have shown to be effective. For example, group-delivered motivational interviewing, an evidenced based treatment often delivered individually, can increase treatment and mutual-help attendance, as well as improve alcohol use outcomes in the short-term among Veterans. Meeting Veterans where they are at and when they are in contact with clinical providers is an important opportunity to screen and link them to services. For example, one study found that engaging adults in the general population during a hospitalization increased the likelihood of a patient engaging in substance use disorder treatment following discharge.
Alcohol-related discussions with Veterans who screen positive for hazardous drinking during medical-surgical care may improve alcohol and medical-surgical outcomes. One intervention in development that attempts to address this gap is DO-MoST—a patient-centered, motivational approach to shared decision making. A randomized control trial of DO-MoST is currently underway. In tandem with the parent control trial, this study explored how Veterans felt about discussing their alcohol use during medical-surgical care and if they believed the DO-MoST intervention was effective. The study also asked medical-surgical providers about the barriers they perceived Veterans to face in engaging in alcohol-related care.
HOW WAS THIS STUDY CONDUCTED?
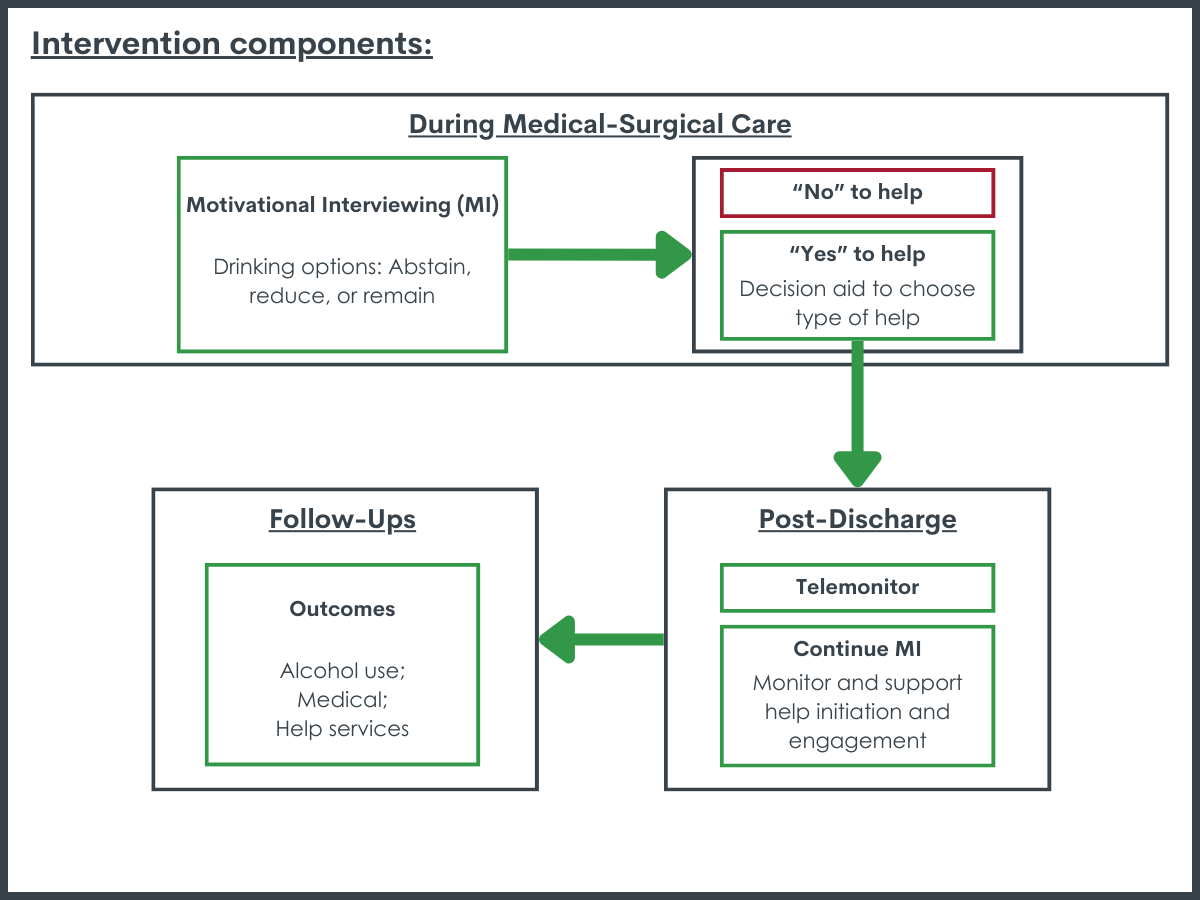
This study was a qualitative evaluation of DO-MoST (Drinking Options-Motivate, Shared Decisions, Telemonitor) that involved interviewing Veterans that participated in a trial of the intervention during medical-surgical care as well as providers of medical-surgical care. DO-MoST is designed to be delivered during a medical care episode by a clinical provider and aims to help an individual increase their awareness of alcohol use patterns, identify potential supports (e.g., behavioral/pharmacological treatment, mutual-help groups), engage supports, and improve alcohol use and health outcomes. The intervention has three components: motivational interviewing (MI) to increase motivation to change drinking patterns, a decision aid to facilitate identification of and linkage to alcohol-related help, and telemonitoring to continue MI or further support linkage to services. An initial 50-min session during the medical-surgical care is conducted to implement MI and, if desired, link to the decision aid. The decision aid, who is a trained clinical provider, then helps identify the types, availability, and engagement processes of various supports (e.g., treatment, mutual help). Following discharge, the decision aid conducts six bi-weekly 15-min telephone sessions to continue MI or transition to facilitating help-initiation and engagement. The intervention is designed to strike a balance between being intensive enough to produce change yet efficient enough to be useful in busy clinical settings with limited availability of staff with psychology training.
Veterans from the DO-MoST trial were recruited during the second half of the trial to participate in this qualitative study. For initial DO-MoST trial participation, the Veterans had to be in a current episode of inpatient or specialty outpatient medical-surgical care (e.g., cancer treatment, diabetes management, orthopedic surgeries), screen for hazardous drinking via the AUDIT-C, have no addiction treatment or mutual-help group attending during the last 60 days, no significant cognitive impairment, access to a phone, and a personal contact who knows their contact information. Additionally, all participants had to have completed the 12-month follow-up of the DO-MoST trial. All Veterans were recruited from the VA Palo Alto or Ann Arbor Health Care systems. Clinical providers of care to medical-surgical patients (i.e., psychologists, social workers, unit or clinic physician-directors, nurses) were emailed by senior study staff and followed up with by phone to answer questions regarding participation in this study.
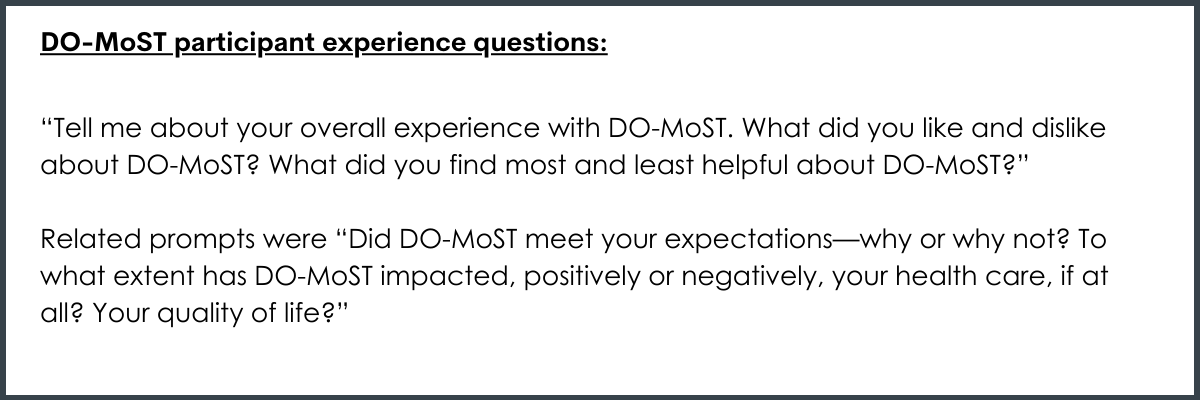
During semi-structured interviews, Veterans were first asked what they thought about being approached to discuss their alcohol use during a medical-surgical care treatment episode and if such discussions would meet the needs of others in medical-surgical care who may need help to reduce their drinking. Then, they were asked to reflect on the DO-MoST intervention. Providers, however, were asked to share their perspectives on patient-, program-, and system-level barriers that impede medical-surgical patients’ initiation and engagement in alcohol treatment. All interviews were recorded, transcribed, and analyzed to identify themes surrounding alcohol discussion and DO-MoST effectiveness, barriers to treatment initiation and engagement, and other emergent topics.
Twenty Veterans participated in this qualitative study. All but one Veteran identified as male, and the average age was 66. The majority were white (80%) and not Hispanic (90%). Sixteen providers participated. Half of the providers identified as female, but their race and ethnicity were not reported. Veterans that participated in this qualitative study were selected from those that chose to participate in the DO-MoST trial, completed it, and did the 12-month follow-up. Thus, it is likely that they had more positive experiences and outcomes with DO-MoST, which should be considered when interpreting these findings.
WHAT DID THIS STUDY FIND?
Veterans were receptive and comfortable discussing drinking during medical-surgical care.
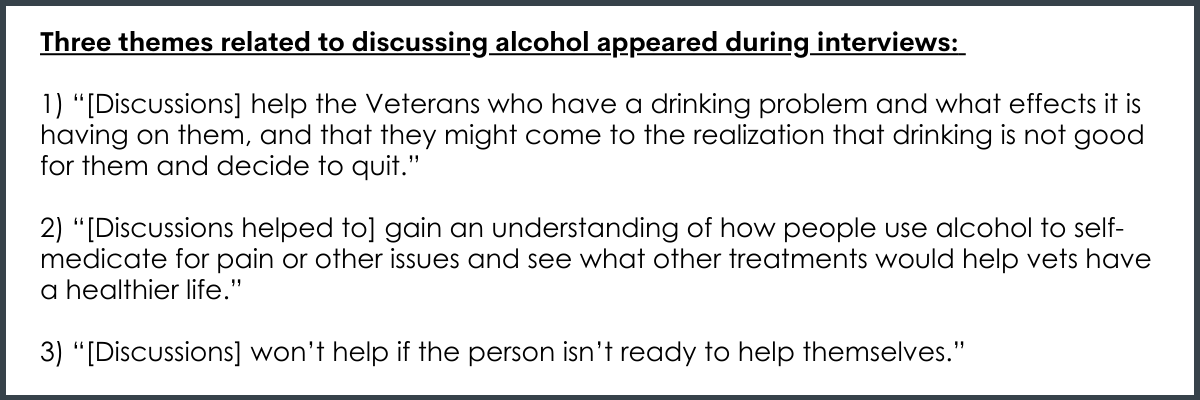
Three themes surrounding alcohol discussing during medical-surgical care emerged from the interviews with patients. First, discussions could help patients recognize their drinking is problematic and identify how to get help. Second, discussions may directly help patients’ medical-surgical and mental health problems by increasing understanding of the effects of alcohol use. Third, discussion would not be helpful if patients did not see their drinking as problematic.
Veterans perceived components of DO-MoST to be effective.
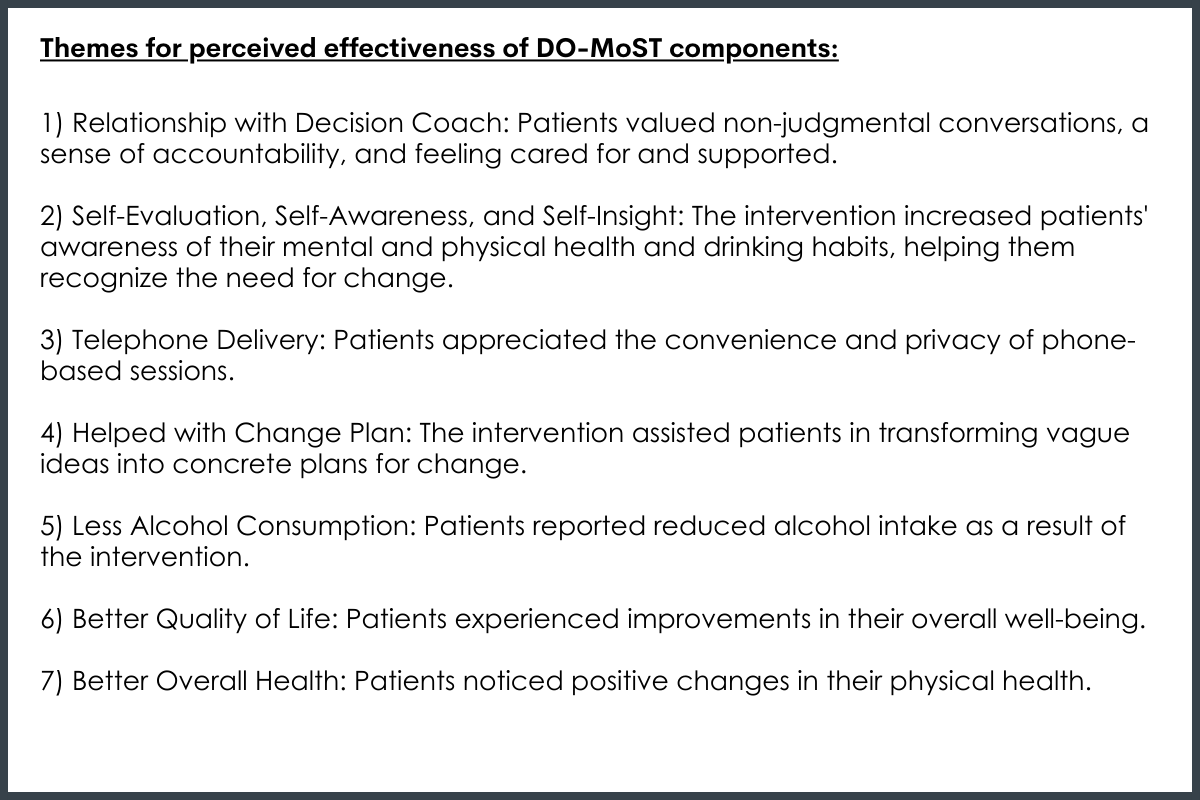
The DO-MoST intervention was perceived as effective by patients, represented by the following 7 themes:
Providers identified many barriers to alcohol care.
Providers identified barriers to alcohol care for medical-surgical patients across levels. Barriers included patients’ lack of motivation or denial of an alcohol-related problem, limited availability of desired treatments, stigma associated with addiction and treatment, life context factors (e.g., homelessness), home environment (e.g., a significant other who drinks), co-occurring health conditions, and difficulties in making treatment appointments. Additionally, providers mentioned barriers related to the provider and setting, which included provider-patient relationship, provider confidence in alcohol care, and staff discomfort with substance use. Lastly, at the system level, providers identified a general lack of treatment resources.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study qualitatively evaluated an on-going clinical trial of DO-MoST among Veterans in medical-surgical care who engage in hazardous drinking. DO-MoST is implemented during a medical-surgical care treatment episode and aims to motivate patients to change their drinking, identify and seek help, and thus improve drinking and medical-surgical health outcomes. The evaluation consisted of 20 interviews with Veterans who participated in the DO-MoST intervention and 16 interviews with clinical providers of care to medical-surgical patients.
Veterans engaging in hazardous drinking were receptive to discussing their alcohol use during medical-surgical care and found the DO-MoST intervention helpful. This suggests that incorporating a motivational, patient-centered intervention during medical-surgical care may be a viable approach to addressing hazardous drinking and initiating behavior change. Additionally, the importance of the provider-patient relationship was highlighted by both patients and providers. Patients valued non-judgmental conversations, a sense of accountability, and feeling cared for and supported. This highlights the need for health care providers to establish trust and rapport with patients, which may require additional addiction-specific training. Furthermore, although the DO-MoST intervention was perceived to effectively address several barriers to treatment, there remain individual and system-level barriers that, if unaddressed, will likely hinder long-term success. For example, the limited availability of desired treatments and complex life contexts (e.g., homelessness) require system-level changes. Lastly, these qualitative results merit continued investigation into intervention effectiveness.
Only Veterans that completed the DO-MoST intervention and its 12-month follow-up were interviewed. Thus, perceptions of DO-MoST as well as openness to discussing alcohol use is likely skewed positive. Individuals with less desirable experiences with DO-MoST likely did not stay until the end of the trial or did not elect to participate in the interviews. Similarly, respondents that did complete the intervention trial may have been more motivated to engage with DO-MoST and participate in interviews. Individuals who did complete the intervention may also feel pressure to report positive experiences.
Only Veterans at two VA systems participated in DO-MoST and were eligible for this study. Thus, findings may not generalize to other populations or regions. However, the VA is the largest healthcare system in the US and likely generalizes to millions of adults in the US.
The medical-surgical condition necessitating care was not assessed. Experiences of DO-MoST and future alcohol use may vary across specific conditions. For example, if alcohol-related liver disease is the qualifying condition for medical-surgical care.
BOTTOM LINE
Medical-surgical care presents an opportunity for clinical providers to connect with Veterans engaging in hazardous drinking. Findings from this study suggest that Veterans are open to discussing their drinking behaviors and engaging with alcohol-related support. The DO-MoST intervention appears to address several barriers to alcohol care among this population. However, patient and system-level barriers must also be addressed to support the long-term success of DO-MoST specifically and alcohol-related care generally.
For individuals and families seeking recovery: Evidence suggests that Veterans are more likely to suffer from mental health issues than their non-Veteran counterparts, and alcohol is the most misused substance among Veterans. Engaging in alcohol-related support during and through medical-surgical care could improve both alcohol and medical-surgical outcomes. Veterans in this study felt open and receptive to discussing alcohol behaviors and participating in an intervention. Discussing alcohol use behaviors is likely to help and unlikely to hurt medical-surgical patient outcomes. If you or a loved one is engaged in medical-surgical care and are drinking regularly, exploring alcohol use patterns and alcohol’s impact on health, specifically related to the medical-surgical condition being treated, could lead to improved health.
For treatment professionals and treatment systems: Engaging Veterans who are in medical-surgical care in patient-led alcohol interventions may be an important opportunity to influence alcohol use behavior change among Veterans engaging in hazardous alcohol use. In general, Veterans in medical-surgical care were open to discussing alcohol use and thought the DO-MoST intervention, a motivational, patient-led alcohol intervention, was effective at addressing patient- and system-level barriers. However, improving access and availability of treatment and reducing stigma were some key barriers that continue to hinder treatment engagement. Exploring Veteran preferences in alcohol-related supports may improve overall help-seeking initiation and engagement.
For scientists: This qualitative study explored perceptions and experiences of Veterans that participated in DO-MoST and views on treatment barriers among clinical providers of care to medical-surgical patients. In general, findings supported medical-surgical care as an opportunity to increase alcohol behavior awareness and link to patient-selected treatments. Furthermore, the DO-MoST intervention was perceived to be effective at motivating behavior change and linking to alcohol supports. However, the effect size of the intervention and its statistical and practical significance has yet to be confirmed. Future investigations should explore the effectiveness of DO-MoST at improving alcohol and medical-surgical outcomes. Additional investigation is also needed to confirm experiences of Veterans that identify as female, non-binary, and races other than white. Future qualitative study may also purposively sample Veterans who had negative perceptions of DO-MoST in order to explore the counterfactual–discussing alcohol during medical-surgical care is not appropriate and DO-MoST is not effective. Ongoing evaluation of this intervention and long-term health outcomes may help facilitate immediate and lasting behavior change among Veterans.
For policy makers: The VA is the largest health care system in the US, and Veterans receiving medical-surgical care that also engage in hazardous drinking may benefit in compounding ways from a motivational, patient-led intervention. Veterans that have participated in such an intervention during medical-surgical care were open to discussing alcohol use and receptive to the intervention. Additional funding to support intervention evaluation and dissemination could have immediate and long-term health benefits as well as cost reductions in medical care. However, system-level barriers, including availability of preferred alcohol treatment and addiction-related stigma, were cited by patients and providers. Increasing funding for a variety of alcohol treatments could improve engagement and retention.
The Veterans Administration (VA) is the largest integrated healthcare system in the U.S., providing services for over 5 million veterans annually. Alcohol use and alcohol use disorder are the most frequently misused substance and diagnosed substance use disorder among Veterans, which makes alcohol use a key issue for the VA. In general, alcohol use contributes to over 200 health conditions and injuries, including liver disease, cancer, and suicide. Veterans receiving medical-surgical care are a specific group of Veterans that may be negatively impacted by alcohol use more than others. Hazardous drinking and medical-surgical conditions are linked in three ways: hazardous drinking may 1) be a casual factor in developing a medical condition (e.g., alcohol-related liver disease), 2) exacerbate existing medical conditions (e.g., diabetes), and 3) complicate management of existing medical conditions (e.g., medication adherence, diet). Addressing drinking during medical-surgical care may directly and indirectly improve health among Veterans.
Significant efforts are underway to develop effective alcohol treatment and recovery options. For instance, the National Institute on Alcohol Abuse and Alcoholism has a 2023 budget exceeding $595 million, with millions going specifically to alcohol treatment research. However, Veterans tend to show different treatment and engagement patterns compared to non-Veterans. Tailored interventions have shown to be effective. For example, group-delivered motivational interviewing, an evidenced based treatment often delivered individually, can increase treatment and mutual-help attendance, as well as improve alcohol use outcomes in the short-term among Veterans. Meeting Veterans where they are at and when they are in contact with clinical providers is an important opportunity to screen and link them to services. For example, one study found that engaging adults in the general population during a hospitalization increased the likelihood of a patient engaging in substance use disorder treatment following discharge.
Alcohol-related discussions with Veterans who screen positive for hazardous drinking during medical-surgical care may improve alcohol and medical-surgical outcomes. One intervention in development that attempts to address this gap is DO-MoST—a patient-centered, motivational approach to shared decision making. A randomized control trial of DO-MoST is currently underway. In tandem with the parent control trial, this study explored how Veterans felt about discussing their alcohol use during medical-surgical care and if they believed the DO-MoST intervention was effective. The study also asked medical-surgical providers about the barriers they perceived Veterans to face in engaging in alcohol-related care.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative evaluation of DO-MoST (Drinking Options-Motivate, Shared Decisions, Telemonitor) that involved interviewing Veterans that participated in a trial of the intervention during medical-surgical care as well as providers of medical-surgical care. DO-MoST is designed to be delivered during a medical care episode by a clinical provider and aims to help an individual increase their awareness of alcohol use patterns, identify potential supports (e.g., behavioral/pharmacological treatment, mutual-help groups), engage supports, and improve alcohol use and health outcomes. The intervention has three components: motivational interviewing (MI) to increase motivation to change drinking patterns, a decision aid to facilitate identification of and linkage to alcohol-related help, and telemonitoring to continue MI or further support linkage to services. An initial 50-min session during the medical-surgical care is conducted to implement MI and, if desired, link to the decision aid. The decision aid, who is a trained clinical provider, then helps identify the types, availability, and engagement processes of various supports (e.g., treatment, mutual help). Following discharge, the decision aid conducts six bi-weekly 15-min telephone sessions to continue MI or transition to facilitating help-initiation and engagement. The intervention is designed to strike a balance between being intensive enough to produce change yet efficient enough to be useful in busy clinical settings with limited availability of staff with psychology training.
Veterans from the DO-MoST trial were recruited during the second half of the trial to participate in this qualitative study. For initial DO-MoST trial participation, the Veterans had to be in a current episode of inpatient or specialty outpatient medical-surgical care (e.g., cancer treatment, diabetes management, orthopedic surgeries), screen for hazardous drinking via the AUDIT-C, have no addiction treatment or mutual-help group attending during the last 60 days, no significant cognitive impairment, access to a phone, and a personal contact who knows their contact information. Additionally, all participants had to have completed the 12-month follow-up of the DO-MoST trial. All Veterans were recruited from the VA Palo Alto or Ann Arbor Health Care systems. Clinical providers of care to medical-surgical patients (i.e., psychologists, social workers, unit or clinic physician-directors, nurses) were emailed by senior study staff and followed up with by phone to answer questions regarding participation in this study.
During semi-structured interviews, Veterans were first asked what they thought about being approached to discuss their alcohol use during a medical-surgical care treatment episode and if such discussions would meet the needs of others in medical-surgical care who may need help to reduce their drinking. Then, they were asked to reflect on the DO-MoST intervention. Providers, however, were asked to share their perspectives on patient-, program-, and system-level barriers that impede medical-surgical patients’ initiation and engagement in alcohol treatment. All interviews were recorded, transcribed, and analyzed to identify themes surrounding alcohol discussion and DO-MoST effectiveness, barriers to treatment initiation and engagement, and other emergent topics.
Twenty Veterans participated in this qualitative study. All but one Veteran identified as male, and the average age was 66. The majority were white (80%) and not Hispanic (90%). Sixteen providers participated. Half of the providers identified as female, but their race and ethnicity were not reported. Veterans that participated in this qualitative study were selected from those that chose to participate in the DO-MoST trial, completed it, and did the 12-month follow-up. Thus, it is likely that they had more positive experiences and outcomes with DO-MoST, which should be considered when interpreting these findings.
WHAT DID THIS STUDY FIND?
Veterans were receptive and comfortable discussing drinking during medical-surgical care.
Three themes surrounding alcohol discussing during medical-surgical care emerged from the interviews with patients. First, discussions could help patients recognize their drinking is problematic and identify how to get help. Second, discussions may directly help patients’ medical-surgical and mental health problems by increasing understanding of the effects of alcohol use. Third, discussion would not be helpful if patients did not see their drinking as problematic.
Veterans perceived components of DO-MoST to be effective.
The DO-MoST intervention was perceived as effective by patients, represented by the following 7 themes:
Providers identified many barriers to alcohol care.
Providers identified barriers to alcohol care for medical-surgical patients across levels. Barriers included patients’ lack of motivation or denial of an alcohol-related problem, limited availability of desired treatments, stigma associated with addiction and treatment, life context factors (e.g., homelessness), home environment (e.g., a significant other who drinks), co-occurring health conditions, and difficulties in making treatment appointments. Additionally, providers mentioned barriers related to the provider and setting, which included provider-patient relationship, provider confidence in alcohol care, and staff discomfort with substance use. Lastly, at the system level, providers identified a general lack of treatment resources.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study qualitatively evaluated an on-going clinical trial of DO-MoST among Veterans in medical-surgical care who engage in hazardous drinking. DO-MoST is implemented during a medical-surgical care treatment episode and aims to motivate patients to change their drinking, identify and seek help, and thus improve drinking and medical-surgical health outcomes. The evaluation consisted of 20 interviews with Veterans who participated in the DO-MoST intervention and 16 interviews with clinical providers of care to medical-surgical patients.
Veterans engaging in hazardous drinking were receptive to discussing their alcohol use during medical-surgical care and found the DO-MoST intervention helpful. This suggests that incorporating a motivational, patient-centered intervention during medical-surgical care may be a viable approach to addressing hazardous drinking and initiating behavior change. Additionally, the importance of the provider-patient relationship was highlighted by both patients and providers. Patients valued non-judgmental conversations, a sense of accountability, and feeling cared for and supported. This highlights the need for health care providers to establish trust and rapport with patients, which may require additional addiction-specific training. Furthermore, although the DO-MoST intervention was perceived to effectively address several barriers to treatment, there remain individual and system-level barriers that, if unaddressed, will likely hinder long-term success. For example, the limited availability of desired treatments and complex life contexts (e.g., homelessness) require system-level changes. Lastly, these qualitative results merit continued investigation into intervention effectiveness.
Only Veterans that completed the DO-MoST intervention and its 12-month follow-up were interviewed. Thus, perceptions of DO-MoST as well as openness to discussing alcohol use is likely skewed positive. Individuals with less desirable experiences with DO-MoST likely did not stay until the end of the trial or did not elect to participate in the interviews. Similarly, respondents that did complete the intervention trial may have been more motivated to engage with DO-MoST and participate in interviews. Individuals who did complete the intervention may also feel pressure to report positive experiences.
Only Veterans at two VA systems participated in DO-MoST and were eligible for this study. Thus, findings may not generalize to other populations or regions. However, the VA is the largest healthcare system in the US and likely generalizes to millions of adults in the US.
The medical-surgical condition necessitating care was not assessed. Experiences of DO-MoST and future alcohol use may vary across specific conditions. For example, if alcohol-related liver disease is the qualifying condition for medical-surgical care.
BOTTOM LINE
Medical-surgical care presents an opportunity for clinical providers to connect with Veterans engaging in hazardous drinking. Findings from this study suggest that Veterans are open to discussing their drinking behaviors and engaging with alcohol-related support. The DO-MoST intervention appears to address several barriers to alcohol care among this population. However, patient and system-level barriers must also be addressed to support the long-term success of DO-MoST specifically and alcohol-related care generally.
For individuals and families seeking recovery: Evidence suggests that Veterans are more likely to suffer from mental health issues than their non-Veteran counterparts, and alcohol is the most misused substance among Veterans. Engaging in alcohol-related support during and through medical-surgical care could improve both alcohol and medical-surgical outcomes. Veterans in this study felt open and receptive to discussing alcohol behaviors and participating in an intervention. Discussing alcohol use behaviors is likely to help and unlikely to hurt medical-surgical patient outcomes. If you or a loved one is engaged in medical-surgical care and are drinking regularly, exploring alcohol use patterns and alcohol’s impact on health, specifically related to the medical-surgical condition being treated, could lead to improved health.
For treatment professionals and treatment systems: Engaging Veterans who are in medical-surgical care in patient-led alcohol interventions may be an important opportunity to influence alcohol use behavior change among Veterans engaging in hazardous alcohol use. In general, Veterans in medical-surgical care were open to discussing alcohol use and thought the DO-MoST intervention, a motivational, patient-led alcohol intervention, was effective at addressing patient- and system-level barriers. However, improving access and availability of treatment and reducing stigma were some key barriers that continue to hinder treatment engagement. Exploring Veteran preferences in alcohol-related supports may improve overall help-seeking initiation and engagement.
For scientists: This qualitative study explored perceptions and experiences of Veterans that participated in DO-MoST and views on treatment barriers among clinical providers of care to medical-surgical patients. In general, findings supported medical-surgical care as an opportunity to increase alcohol behavior awareness and link to patient-selected treatments. Furthermore, the DO-MoST intervention was perceived to be effective at motivating behavior change and linking to alcohol supports. However, the effect size of the intervention and its statistical and practical significance has yet to be confirmed. Future investigations should explore the effectiveness of DO-MoST at improving alcohol and medical-surgical outcomes. Additional investigation is also needed to confirm experiences of Veterans that identify as female, non-binary, and races other than white. Future qualitative study may also purposively sample Veterans who had negative perceptions of DO-MoST in order to explore the counterfactual–discussing alcohol during medical-surgical care is not appropriate and DO-MoST is not effective. Ongoing evaluation of this intervention and long-term health outcomes may help facilitate immediate and lasting behavior change among Veterans.
For policy makers: The VA is the largest health care system in the US, and Veterans receiving medical-surgical care that also engage in hazardous drinking may benefit in compounding ways from a motivational, patient-led intervention. Veterans that have participated in such an intervention during medical-surgical care were open to discussing alcohol use and receptive to the intervention. Additional funding to support intervention evaluation and dissemination could have immediate and long-term health benefits as well as cost reductions in medical care. However, system-level barriers, including availability of preferred alcohol treatment and addiction-related stigma, were cited by patients and providers. Increasing funding for a variety of alcohol treatments could improve engagement and retention.
The Veterans Administration (VA) is the largest integrated healthcare system in the U.S., providing services for over 5 million veterans annually. Alcohol use and alcohol use disorder are the most frequently misused substance and diagnosed substance use disorder among Veterans, which makes alcohol use a key issue for the VA. In general, alcohol use contributes to over 200 health conditions and injuries, including liver disease, cancer, and suicide. Veterans receiving medical-surgical care are a specific group of Veterans that may be negatively impacted by alcohol use more than others. Hazardous drinking and medical-surgical conditions are linked in three ways: hazardous drinking may 1) be a casual factor in developing a medical condition (e.g., alcohol-related liver disease), 2) exacerbate existing medical conditions (e.g., diabetes), and 3) complicate management of existing medical conditions (e.g., medication adherence, diet). Addressing drinking during medical-surgical care may directly and indirectly improve health among Veterans.
Significant efforts are underway to develop effective alcohol treatment and recovery options. For instance, the National Institute on Alcohol Abuse and Alcoholism has a 2023 budget exceeding $595 million, with millions going specifically to alcohol treatment research. However, Veterans tend to show different treatment and engagement patterns compared to non-Veterans. Tailored interventions have shown to be effective. For example, group-delivered motivational interviewing, an evidenced based treatment often delivered individually, can increase treatment and mutual-help attendance, as well as improve alcohol use outcomes in the short-term among Veterans. Meeting Veterans where they are at and when they are in contact with clinical providers is an important opportunity to screen and link them to services. For example, one study found that engaging adults in the general population during a hospitalization increased the likelihood of a patient engaging in substance use disorder treatment following discharge.
Alcohol-related discussions with Veterans who screen positive for hazardous drinking during medical-surgical care may improve alcohol and medical-surgical outcomes. One intervention in development that attempts to address this gap is DO-MoST—a patient-centered, motivational approach to shared decision making. A randomized control trial of DO-MoST is currently underway. In tandem with the parent control trial, this study explored how Veterans felt about discussing their alcohol use during medical-surgical care and if they believed the DO-MoST intervention was effective. The study also asked medical-surgical providers about the barriers they perceived Veterans to face in engaging in alcohol-related care.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative evaluation of DO-MoST (Drinking Options-Motivate, Shared Decisions, Telemonitor) that involved interviewing Veterans that participated in a trial of the intervention during medical-surgical care as well as providers of medical-surgical care. DO-MoST is designed to be delivered during a medical care episode by a clinical provider and aims to help an individual increase their awareness of alcohol use patterns, identify potential supports (e.g., behavioral/pharmacological treatment, mutual-help groups), engage supports, and improve alcohol use and health outcomes. The intervention has three components: motivational interviewing (MI) to increase motivation to change drinking patterns, a decision aid to facilitate identification of and linkage to alcohol-related help, and telemonitoring to continue MI or further support linkage to services. An initial 50-min session during the medical-surgical care is conducted to implement MI and, if desired, link to the decision aid. The decision aid, who is a trained clinical provider, then helps identify the types, availability, and engagement processes of various supports (e.g., treatment, mutual help). Following discharge, the decision aid conducts six bi-weekly 15-min telephone sessions to continue MI or transition to facilitating help-initiation and engagement. The intervention is designed to strike a balance between being intensive enough to produce change yet efficient enough to be useful in busy clinical settings with limited availability of staff with psychology training.
Veterans from the DO-MoST trial were recruited during the second half of the trial to participate in this qualitative study. For initial DO-MoST trial participation, the Veterans had to be in a current episode of inpatient or specialty outpatient medical-surgical care (e.g., cancer treatment, diabetes management, orthopedic surgeries), screen for hazardous drinking via the AUDIT-C, have no addiction treatment or mutual-help group attending during the last 60 days, no significant cognitive impairment, access to a phone, and a personal contact who knows their contact information. Additionally, all participants had to have completed the 12-month follow-up of the DO-MoST trial. All Veterans were recruited from the VA Palo Alto or Ann Arbor Health Care systems. Clinical providers of care to medical-surgical patients (i.e., psychologists, social workers, unit or clinic physician-directors, nurses) were emailed by senior study staff and followed up with by phone to answer questions regarding participation in this study.
During semi-structured interviews, Veterans were first asked what they thought about being approached to discuss their alcohol use during a medical-surgical care treatment episode and if such discussions would meet the needs of others in medical-surgical care who may need help to reduce their drinking. Then, they were asked to reflect on the DO-MoST intervention. Providers, however, were asked to share their perspectives on patient-, program-, and system-level barriers that impede medical-surgical patients’ initiation and engagement in alcohol treatment. All interviews were recorded, transcribed, and analyzed to identify themes surrounding alcohol discussion and DO-MoST effectiveness, barriers to treatment initiation and engagement, and other emergent topics.
Twenty Veterans participated in this qualitative study. All but one Veteran identified as male, and the average age was 66. The majority were white (80%) and not Hispanic (90%). Sixteen providers participated. Half of the providers identified as female, but their race and ethnicity were not reported. Veterans that participated in this qualitative study were selected from those that chose to participate in the DO-MoST trial, completed it, and did the 12-month follow-up. Thus, it is likely that they had more positive experiences and outcomes with DO-MoST, which should be considered when interpreting these findings.
WHAT DID THIS STUDY FIND?
Veterans were receptive and comfortable discussing drinking during medical-surgical care.
Three themes surrounding alcohol discussing during medical-surgical care emerged from the interviews with patients. First, discussions could help patients recognize their drinking is problematic and identify how to get help. Second, discussions may directly help patients’ medical-surgical and mental health problems by increasing understanding of the effects of alcohol use. Third, discussion would not be helpful if patients did not see their drinking as problematic.
Veterans perceived components of DO-MoST to be effective.
The DO-MoST intervention was perceived as effective by patients, represented by the following 7 themes:
Providers identified many barriers to alcohol care.
Providers identified barriers to alcohol care for medical-surgical patients across levels. Barriers included patients’ lack of motivation or denial of an alcohol-related problem, limited availability of desired treatments, stigma associated with addiction and treatment, life context factors (e.g., homelessness), home environment (e.g., a significant other who drinks), co-occurring health conditions, and difficulties in making treatment appointments. Additionally, providers mentioned barriers related to the provider and setting, which included provider-patient relationship, provider confidence in alcohol care, and staff discomfort with substance use. Lastly, at the system level, providers identified a general lack of treatment resources.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study qualitatively evaluated an on-going clinical trial of DO-MoST among Veterans in medical-surgical care who engage in hazardous drinking. DO-MoST is implemented during a medical-surgical care treatment episode and aims to motivate patients to change their drinking, identify and seek help, and thus improve drinking and medical-surgical health outcomes. The evaluation consisted of 20 interviews with Veterans who participated in the DO-MoST intervention and 16 interviews with clinical providers of care to medical-surgical patients.
Veterans engaging in hazardous drinking were receptive to discussing their alcohol use during medical-surgical care and found the DO-MoST intervention helpful. This suggests that incorporating a motivational, patient-centered intervention during medical-surgical care may be a viable approach to addressing hazardous drinking and initiating behavior change. Additionally, the importance of the provider-patient relationship was highlighted by both patients and providers. Patients valued non-judgmental conversations, a sense of accountability, and feeling cared for and supported. This highlights the need for health care providers to establish trust and rapport with patients, which may require additional addiction-specific training. Furthermore, although the DO-MoST intervention was perceived to effectively address several barriers to treatment, there remain individual and system-level barriers that, if unaddressed, will likely hinder long-term success. For example, the limited availability of desired treatments and complex life contexts (e.g., homelessness) require system-level changes. Lastly, these qualitative results merit continued investigation into intervention effectiveness.
Only Veterans that completed the DO-MoST intervention and its 12-month follow-up were interviewed. Thus, perceptions of DO-MoST as well as openness to discussing alcohol use is likely skewed positive. Individuals with less desirable experiences with DO-MoST likely did not stay until the end of the trial or did not elect to participate in the interviews. Similarly, respondents that did complete the intervention trial may have been more motivated to engage with DO-MoST and participate in interviews. Individuals who did complete the intervention may also feel pressure to report positive experiences.
Only Veterans at two VA systems participated in DO-MoST and were eligible for this study. Thus, findings may not generalize to other populations or regions. However, the VA is the largest healthcare system in the US and likely generalizes to millions of adults in the US.
The medical-surgical condition necessitating care was not assessed. Experiences of DO-MoST and future alcohol use may vary across specific conditions. For example, if alcohol-related liver disease is the qualifying condition for medical-surgical care.
BOTTOM LINE
Medical-surgical care presents an opportunity for clinical providers to connect with Veterans engaging in hazardous drinking. Findings from this study suggest that Veterans are open to discussing their drinking behaviors and engaging with alcohol-related support. The DO-MoST intervention appears to address several barriers to alcohol care among this population. However, patient and system-level barriers must also be addressed to support the long-term success of DO-MoST specifically and alcohol-related care generally.
For individuals and families seeking recovery: Evidence suggests that Veterans are more likely to suffer from mental health issues than their non-Veteran counterparts, and alcohol is the most misused substance among Veterans. Engaging in alcohol-related support during and through medical-surgical care could improve both alcohol and medical-surgical outcomes. Veterans in this study felt open and receptive to discussing alcohol behaviors and participating in an intervention. Discussing alcohol use behaviors is likely to help and unlikely to hurt medical-surgical patient outcomes. If you or a loved one is engaged in medical-surgical care and are drinking regularly, exploring alcohol use patterns and alcohol’s impact on health, specifically related to the medical-surgical condition being treated, could lead to improved health.
For treatment professionals and treatment systems: Engaging Veterans who are in medical-surgical care in patient-led alcohol interventions may be an important opportunity to influence alcohol use behavior change among Veterans engaging in hazardous alcohol use. In general, Veterans in medical-surgical care were open to discussing alcohol use and thought the DO-MoST intervention, a motivational, patient-led alcohol intervention, was effective at addressing patient- and system-level barriers. However, improving access and availability of treatment and reducing stigma were some key barriers that continue to hinder treatment engagement. Exploring Veteran preferences in alcohol-related supports may improve overall help-seeking initiation and engagement.
For scientists: This qualitative study explored perceptions and experiences of Veterans that participated in DO-MoST and views on treatment barriers among clinical providers of care to medical-surgical patients. In general, findings supported medical-surgical care as an opportunity to increase alcohol behavior awareness and link to patient-selected treatments. Furthermore, the DO-MoST intervention was perceived to be effective at motivating behavior change and linking to alcohol supports. However, the effect size of the intervention and its statistical and practical significance has yet to be confirmed. Future investigations should explore the effectiveness of DO-MoST at improving alcohol and medical-surgical outcomes. Additional investigation is also needed to confirm experiences of Veterans that identify as female, non-binary, and races other than white. Future qualitative study may also purposively sample Veterans who had negative perceptions of DO-MoST in order to explore the counterfactual–discussing alcohol during medical-surgical care is not appropriate and DO-MoST is not effective. Ongoing evaluation of this intervention and long-term health outcomes may help facilitate immediate and lasting behavior change among Veterans.
For policy makers: The VA is the largest health care system in the US, and Veterans receiving medical-surgical care that also engage in hazardous drinking may benefit in compounding ways from a motivational, patient-led intervention. Veterans that have participated in such an intervention during medical-surgical care were open to discussing alcohol use and receptive to the intervention. Additional funding to support intervention evaluation and dissemination could have immediate and long-term health benefits as well as cost reductions in medical care. However, system-level barriers, including availability of preferred alcohol treatment and addiction-related stigma, were cited by patients and providers. Increasing funding for a variety of alcohol treatments could improve engagement and retention.