Is integrated treatment necessary for co-occurring disorders?
More than half of adults with posttraumatic stress disorder also have alcohol use disorder, and more than 1 in 10 with alcohol use disorder have posttraumatic stress disorder. Identifying the best course of treatment for adults with these commonly co-occurring disorders can be difficult. Which disorder should interventions target? Is integrated treatment the only option? This study explores whether single-focus treatments for alcohol use disorder and posttraumatic stress disorder lead to improvements in both among adults with these co-occurring disorders.
2 out of 3 adults in the US. that have had a posttraumatic stress disorder also have had an alcohol use disorder during their life. Additionally, 1 out of 10 adults that have had an alcohol use disorder have also had a posttraumatic stress disorder. Given the high co-occurrence of these two disorders, evidence identifying the best course or type of treatment would help clinical providers and those with these disorders make treatment decisions.
Conventional wisdom and practice suggest that alcohol use disorder and posttraumatic stress disorder should be treated separately through targeted treatments or through specifically designed interventions that integrate treatments for both trauma and alcohol use disorder. However, many clinics are under-resourced to develop, maintain, and staff specialized programs addressing both disorders. If a single-focus treatment could address both disorders, resources could be diverted to increasing the fidelity of that single-focus treatment rather than investing in training for new treatments.
This study sought to explore whether a single-focus treatment for posttraumatic stress disorder alone or for alcohol use disorder alone led to improvements in both types of outcomes among adults with co-occurring posttraumatic stress disorder and alcohol use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized control trial of adults that took place at an academic hospital-affiliated mental health clinic and a Veteran Affairs (VA)-based research clinic in the Pacific Northwest. Recruitment for the study began in November 2013, and all study interventions were completed by August 2018. Adults were recruited through ads in newspapers, flyers, and letters sent after identifying eligibility via medical records. Thus, individuals participating made the conscious decision to self-select into a treatment study, which included the eligibility criteria of having a desire to eliminate or reduce alcohol use. The study recruited 101 participants. Participants met DSM-5 criteria for posttraumatic stress disorder and alcohol use disorder, reported at least 2 heavy drinking days (5+/4+ standard drinks per day for men/women) or 2 weeks of heavy drinking (21+/14+ drinks per week for men/women) in the past month, have a desire to abstain or reduce alcohol use, be fluent in English, and be 18 or older. Individuals were excluded from study participation if they met any of the following criteria: having a psychotic or uncontrolled bipolar disorder, having attempted suicide or engaged in serious self-harm within the past 3 months or having suicidal ideation with a specific plan or intent within the past 2 months, being in a currently violent interpersonal relationship, experiencing alcohol withdrawal at the time of consent, having unstable psychiatric medication use within the past 3 months, having used a medication to treat alcohol use disorder (e.g., disulfiram, acamprosate) within the past month, or having participated in trauma-focused mental health treatment or behaviorally-focused alcohol treatment within the past month.
Participants were randomly assigned to one of three groups: cognitive processing therapy, relapse prevention, or assessment only.
Cognitive Processing Therapy is a treatment that aims to help clients modify their thoughts about the causes of traumatic events and their overly broad beliefs with worksheets and questioning techniques. The therapy focuses on teaching clients to challenge and change cognitions underlying their distressing experiences. Within cognitive processing therapy, alcohol use is considered an avoidance behavior (i.e., drinking to avoid experiencing unpleasant PTSD symptoms) and addressed by challenging alcohol-related maladaptive thought patterns.
Relapse prevention is a cognitive-behavioral therapy approach that focuses on helping individuals develop self-monitoring and coping skills to handle situations that may lead to excessive alcohol consumption. The goal is to prevent relapse by equipping individuals with the tools they need to manage their recovery. Relapse prevention addressed posttraumatic stress by encouraging participants to practice the skills they’re learning when they experience trauma-related symptoms – so that these PTSD-related experiences don’t “trigger” a drinking (or heavy drinking) episode.
Both treatments were 12 sessions long and of similar duration with participants attending one or two sessions per week for up to 20 weeks. The “assessment only” condition consisted of weekly brief (15min) phone calls from a study therapist to provide support/safety monitoring. Those that were initially assigned to the assessment only group were subsequently randomly assigned once more to one of the two active treatment groups – either cognitive processing therapy or relapse prevention after six weeks of receiving no treatment.
Participants completed validated assessments to measure changes in alcohol use and posttraumatic stress disorder severity at baseline, post-treatment, 3- and 12-month follow-up points. For alcohol use, the main outcomes were days of alcohol use and heavy drinking days (5+/4+ standard drinks for men/women). Posttraumatic stress disorder severity ranged from 0 – 80, with higher scores representing higher severity. Those that were first assigned to the assessment only condition were given an additional assessment following their six-week period of no treatment.
A total of 101 adults participated in the study. The average age was 42, and 56% of the participants identified as female while 53% identified as White. Over half (60%) were single, 33% had graduated college, 29% were veterans, and 38% were employed. About one in three (36%) reported their worst traumatic events as sexual assault, and another third (33%) reported their worst as physical assault. About one in three (39%) also meet criteria for another drug use disorder besides alcohol (other than tobacco).
WHAT DID THIS STUDY FIND?
Individuals in the assessment only condition made improvements prior to treatment.
Individuals assigned to the assessment only condition, which only included brief weekly phone calls for support/safety monitoring, showed improvements in both PTSD severity and heavy drinking days after the six-week period. However, those in both of the active treatment conditions experienced greater benefit on both PTSD severity and heavy drinking days than those in the assessment only condition.
Cognitive processing therapy and relapse prevention improved symptom severity and alcohol use to a similar degree.
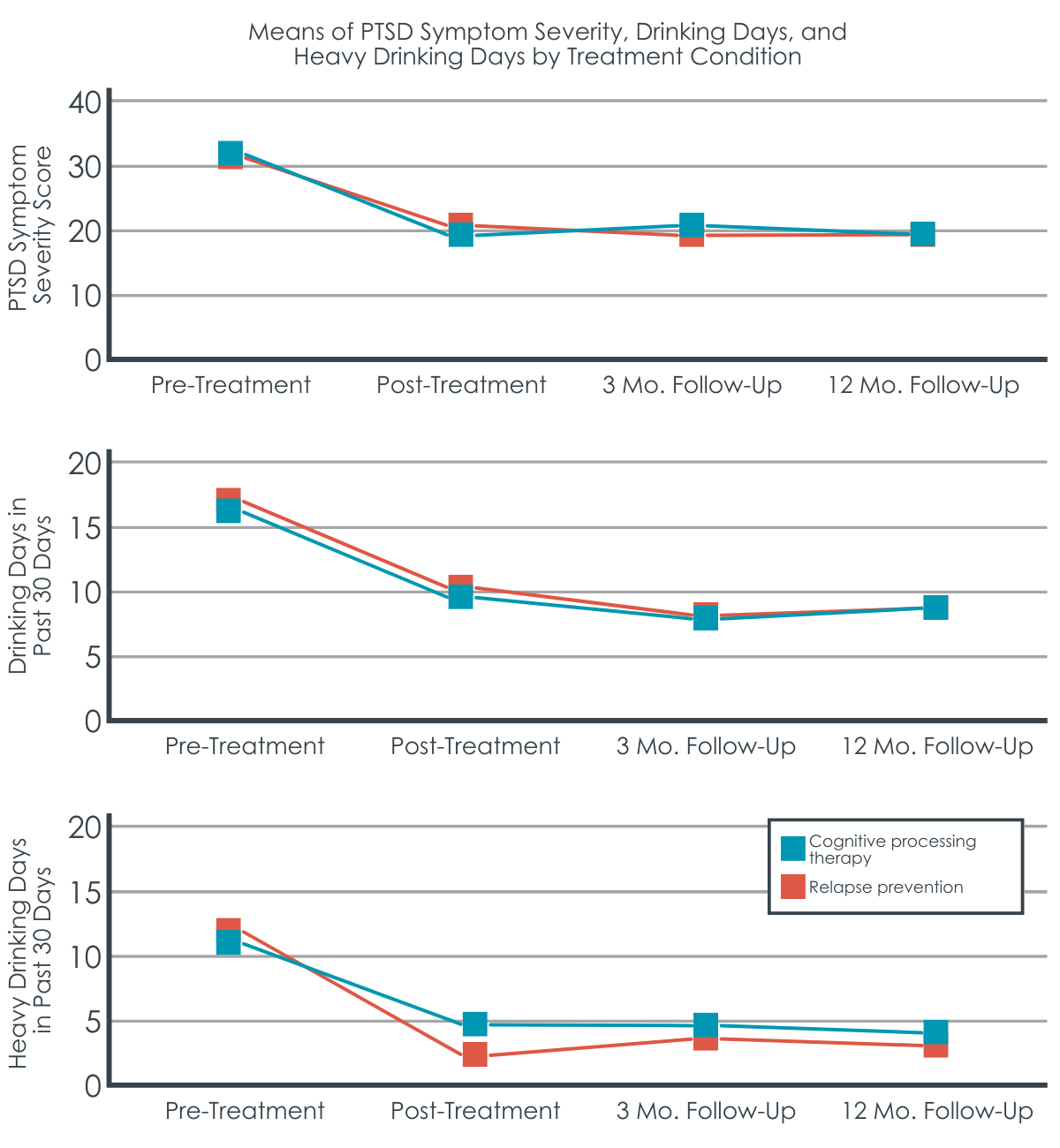
Participants in both conditions reported similar less severe PTSD symptoms and fewer heavy drinking days after receiving treatment. Overall, from baseline to 12 months after treatment, cognitive processing therapy led to a 47% decrease in PTSD severity, and relapse prevention led to a 35% decrease in severity. Those in cognitive processing therapy also reported a 73% reduction in days of heavy drinking at 12-month follow-up compared to baseline, and those in relapse prevention reported an 82% decrease in heavy drinking days. These benefits related to both treatment conditions occurred by end of treatment and were maintained through the 12-month follow-up.
Cognitive processing therapy and relapse prevention did not differ on PTSD severity immediately after treatment.
Both interventions resulted in similar improvements in PTSD severity and heavy drinking days immediately post-treatment. Participants in the cognitive processing therapy reported a 40% reduction in PTSD severity immediately after treatment, and those in the relapse prevention treatment saw a 37% reduction.
Relapse prevention had greater immediate reduction on heavy drinking than cognitive processing therapy.
Although both treatments led to reduced heavy drinking days, those receiving the more explicitly alcohol-focused relapse prevention treatment reported fewer heavy drinking days on average after treatment than those in cognitive processing therapy. Those in relapse prevention reported 77% fewer drinking days immediately following treatment compared to baseline, with past-month heavy drinking days reducing from 13 at baseline to 3 post-treatment. Those in the cognitive processing group reported a 54% reduction in the number of drinking days, from 17 days at baseline to 9 post-treatment. The number of drinking days was not significantly different between the two groups. Those in the cognitive processing group also reported a 59% reduction in the number of heavy drinking days, from 12 heavy drinking days at baseline to 5 post-treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 101 adults with co-occurring posttraumatic stress disorder and alcohol use disorder found that both a more explicitly trauma-focused cognitive processing therapy and a more explicitly focused alcohol use disorder focused relapse prevention treatment both reduced posttraumatic stress disorder severity to the same degree, and the relapse prevention treatment led to greater reductions in heavy drinking days compared to cognitive processing therapy. The findings suggest that the common belief that the two disorders require disorder-specific or integrated treatments to show improvements may not be true, at least when treatments are delivered according to manualized protocols.
Participants in both types of treatments saw benefits in the non-targeted disorder. Yet, those in the relapse prevention treatment saw greater reductions in their days of heavy drinking compared to participants in cognitive processing therapy. It is noteworthy to mention that only 55% of participants completed a minimum of 9 out of 12 therapy sessions and only 54% completed the 12-month follow-up. The modest sample size and the high rate of non-completion limit the study’s findings. Nevertheless, the study found that there was not differential dropout between treatments. This implies that, although the dropout rate was high, it was likely not associated with specific features of either treatment.
These findings highlight the complexity of co-occurring disorders and the misconception that individuals with co-occurring disorders always require specifically designed treatments for those with co-occurring disorders. This is good news as it may mean that for individuals suffering from both alcohol use disorder and PTSD who are seeking treatment and who cannot find an available program or clinician who has specific treatment expertise addressing both types of disorders, may nevertheless be able to find relief from both types of disorders by accessing either a PTSD specialist, or, by accessing an addiction relapse prevention treatment specialist.
Recently released data from 2021 reports that 19.4 million adults in the US have a substance use disorder co-occurring with another mental illness. Substance use, including alcohol, may lead to the onset of symptoms of another mental illness. Yet, mental illness may also precede and lead to substance use as a method to alleviate symptoms related to a mental illness (e.g., anxiety, depression). Which disorder manifests first, severity of each disorder, compounding effects of one disorder on the other, and even specific types of traumas may also impact how effective single-focused and integrated treatments are on improving outcomes for some individuals and this requires further study.
Additionally, as the study highlights, treatments that more explicitly target specific disorders (i.e., alcohol use disorder relapse prevention) may also address to some degree other aspects of co-occurring mental health challenges. Relapse prevention, for example, includes specific curricula surrounding trauma—framing trauma as a trigger for substance use which can be addressed through the implementation of coping skills learned through the relapse prevention program. The application of behavioral and coping skills (e.g., communication, self-efficacy) may address underlying aspects of mental illness regardless of the primary disorder.
This study found that both cognitive processing therapy and relapse prevention improved posttraumatic stress disorder severity and days of heavy drinking, with relapse prevention linked to greater reductions in heavy drinking compared to cognitive processing therapy. These findings suggest that, if there are barriers to accessing PTSD-specific care, empirically supported alcohol use disorder treatments like the relapse prevention approach used here may help improve PTSD symptoms as well. Although both treatments were associated with improvements in PTSD symptoms and heavy drinking, this study did not compare these disorder-specific treatments with an integrated treatment approach. An integrated treatment approach has been found to be more effective in reducing substance use among individuals with PTSD compared to standard, non-manualized treatments. However, reductions in both alcohol use and PTSD symptom severity with an integrated therapy are comparable to the results found in this study suggesting these individuals may benefit equally well from any of these types of integrated or non-integrated approaches. More research is needed to understand who may benefit most from different types of treatment and how specific disorder specific and demographic characteristics impact treatment outcomes.
The study had a relatively small sample. Thus, the study was underpowered to detect small to moderate effects, which means that they did not have enough participants to observe minor improvements in outcomes.
The low rate of treatment completion (55% completed at least 9 out of 12 sessions) reduces the credibility and confidence in the study’s findings. However, this level of session treatment completion is typical in such treatment studies and dropout was not different between the two types of treatments, which instills confidence in the results.
Nearly half (46%) did not complete the 12-month follow-up. The low follow-up completion rate further reduces the sample size, which reduces confidence in the effects found for the treatments at the 12-month follow-up.
BOTTOM LINE
This study found that among adults with co-occurring posttraumatic stress disorder and alcohol use disorder, a more explicitly trauma focused cognitive processing therapy and a more alcohol addiction focused relapse prevention did not differ on benefits in posttraumatic stress disorder severity, but participants in relapse prevention reported greater reductions in heavy drinking compared to their counterparts in cognitive processing therapy. These findings suggest that treatment targeting one type of disorder likely has spillover therapeutic benefits on other mental illness symptoms. Particularly for those with co-occurring alcohol use disorder and posttraumatic stress disorders, seeking treatment for alcohol use will likely provide tools that can be used to navigate triggers related to trauma in addition to helping eliminate or reduce heavy alcohol use. Additionally, treatments such as relapse prevention and cognitive processing therapy may each include at least some more minor components that are nevertheless sufficient to address behaviors and symptoms that are not explicitly targeted by that particular therapy (e.g., trauma in relapse prevention, and substance use in cognitive processing therapy).This may be good news for individuals who suffer from both types of disorders who cannot find practitioners or programs locally with expertise in both disorders; finding a clinician who can address at least one well, may also have positive effects on the other.
For individuals and families seeking recovery: Receiving alcohol use disorder treatments like relapse prevention has been found to improve drinking as well as severity of other disorders, such as posttraumatic stress disorder in this study. Although it can be difficult at times to identify the best course of treatment for someone with co-occurring disorders, this study demonstrates that a more addiction-focused relapse prevention therapy improved posttraumatic stress disorder severity just as well as a specially designed treatment for posttraumatic stress disorder, and relapse prevention was also more helpful at reducing heavy alcohol use. This is good news if you suffer from both types of disorders but cannot find practitioners or programs locally with expertise in both disorders; finding a clinician who can address at least one well, may also have positive effects on the other.
For treatment professionals and treatment systems: The study found that an alcohol use disorder treatment (relapse prevention) improved PTSD severity as effectively as the PTSD treatment (cognitive processing therapy) yet led to greater reductions in heavy drinking days. Although this study did not include a treatment specifically designed for adults with co-occurring disorder, both types of treatment include components that address mental health issues outside of the primary target (e.g., trauma in relapse prevention, and substance use in cognitive processing therapy) and resulted in magnitudes of effect similar to integrated treatments that have been specifically designed for those with co-occurring disorders. Applying either treatment effectively for those with co-occurring PTSD is likely to provide similar benefit for the targeted as well as non-targeted disorder. Additionally, given this study’s findings, treatment professionals and systems may benefit from supporting an individual’s personal preference in selection of one of these two types of treatment when available.
For scientists:This randomized control trial demonstrated that both unmodified PTSD focused cognitive processing therapy and addiction-focused relapse prevention led to similar and helpful improvements in posttraumatic stress disorder severity and heavy drinking, with relapse prevention leading to a greater reduction in heavy drinking days compared to cognitive processing therapy. These findings suggest that targeting either disorder among adults with co-occurring posttraumatic stress disorder and alcohol use disorder can lead to improvements to the same degree as existing treatments that focus on co-occurring disorders, with a potential preference for relapse prevention therapy if reductions in heavy drinking are a particular important goal. Future studies may explore how unique presentations of co-occurrence regarding disorder precedent, severity, and chronicity impact treatment.
For policy makers: The prevalence rate of adults with the co-occurrence of substance use disorders and another mental health illness is increasing, and understanding how existing treatments that may target a specific disorder can reduce symptom severity of other disorders is likely to benefit individuals with co-occurring disorders and relieve societal burden (e.g., medical cost, work hours). Additional funding to support the analysis of cross-treatment effects could improve the well-being of many individuals with co-occurring disorders that do not have access to integrated treatments and/or prefer specific treatment targets.
2 out of 3 adults in the US. that have had a posttraumatic stress disorder also have had an alcohol use disorder during their life. Additionally, 1 out of 10 adults that have had an alcohol use disorder have also had a posttraumatic stress disorder. Given the high co-occurrence of these two disorders, evidence identifying the best course or type of treatment would help clinical providers and those with these disorders make treatment decisions.
Conventional wisdom and practice suggest that alcohol use disorder and posttraumatic stress disorder should be treated separately through targeted treatments or through specifically designed interventions that integrate treatments for both trauma and alcohol use disorder. However, many clinics are under-resourced to develop, maintain, and staff specialized programs addressing both disorders. If a single-focus treatment could address both disorders, resources could be diverted to increasing the fidelity of that single-focus treatment rather than investing in training for new treatments.
This study sought to explore whether a single-focus treatment for posttraumatic stress disorder alone or for alcohol use disorder alone led to improvements in both types of outcomes among adults with co-occurring posttraumatic stress disorder and alcohol use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized control trial of adults that took place at an academic hospital-affiliated mental health clinic and a Veteran Affairs (VA)-based research clinic in the Pacific Northwest. Recruitment for the study began in November 2013, and all study interventions were completed by August 2018. Adults were recruited through ads in newspapers, flyers, and letters sent after identifying eligibility via medical records. Thus, individuals participating made the conscious decision to self-select into a treatment study, which included the eligibility criteria of having a desire to eliminate or reduce alcohol use. The study recruited 101 participants. Participants met DSM-5 criteria for posttraumatic stress disorder and alcohol use disorder, reported at least 2 heavy drinking days (5+/4+ standard drinks per day for men/women) or 2 weeks of heavy drinking (21+/14+ drinks per week for men/women) in the past month, have a desire to abstain or reduce alcohol use, be fluent in English, and be 18 or older. Individuals were excluded from study participation if they met any of the following criteria: having a psychotic or uncontrolled bipolar disorder, having attempted suicide or engaged in serious self-harm within the past 3 months or having suicidal ideation with a specific plan or intent within the past 2 months, being in a currently violent interpersonal relationship, experiencing alcohol withdrawal at the time of consent, having unstable psychiatric medication use within the past 3 months, having used a medication to treat alcohol use disorder (e.g., disulfiram, acamprosate) within the past month, or having participated in trauma-focused mental health treatment or behaviorally-focused alcohol treatment within the past month.
Participants were randomly assigned to one of three groups: cognitive processing therapy, relapse prevention, or assessment only.
Cognitive Processing Therapy is a treatment that aims to help clients modify their thoughts about the causes of traumatic events and their overly broad beliefs with worksheets and questioning techniques. The therapy focuses on teaching clients to challenge and change cognitions underlying their distressing experiences. Within cognitive processing therapy, alcohol use is considered an avoidance behavior (i.e., drinking to avoid experiencing unpleasant PTSD symptoms) and addressed by challenging alcohol-related maladaptive thought patterns.
Relapse prevention is a cognitive-behavioral therapy approach that focuses on helping individuals develop self-monitoring and coping skills to handle situations that may lead to excessive alcohol consumption. The goal is to prevent relapse by equipping individuals with the tools they need to manage their recovery. Relapse prevention addressed posttraumatic stress by encouraging participants to practice the skills they’re learning when they experience trauma-related symptoms – so that these PTSD-related experiences don’t “trigger” a drinking (or heavy drinking) episode.
Both treatments were 12 sessions long and of similar duration with participants attending one or two sessions per week for up to 20 weeks. The “assessment only” condition consisted of weekly brief (15min) phone calls from a study therapist to provide support/safety monitoring. Those that were initially assigned to the assessment only group were subsequently randomly assigned once more to one of the two active treatment groups – either cognitive processing therapy or relapse prevention after six weeks of receiving no treatment.
Participants completed validated assessments to measure changes in alcohol use and posttraumatic stress disorder severity at baseline, post-treatment, 3- and 12-month follow-up points. For alcohol use, the main outcomes were days of alcohol use and heavy drinking days (5+/4+ standard drinks for men/women). Posttraumatic stress disorder severity ranged from 0 – 80, with higher scores representing higher severity. Those that were first assigned to the assessment only condition were given an additional assessment following their six-week period of no treatment.
A total of 101 adults participated in the study. The average age was 42, and 56% of the participants identified as female while 53% identified as White. Over half (60%) were single, 33% had graduated college, 29% were veterans, and 38% were employed. About one in three (36%) reported their worst traumatic events as sexual assault, and another third (33%) reported their worst as physical assault. About one in three (39%) also meet criteria for another drug use disorder besides alcohol (other than tobacco).
WHAT DID THIS STUDY FIND?
Individuals in the assessment only condition made improvements prior to treatment.
Individuals assigned to the assessment only condition, which only included brief weekly phone calls for support/safety monitoring, showed improvements in both PTSD severity and heavy drinking days after the six-week period. However, those in both of the active treatment conditions experienced greater benefit on both PTSD severity and heavy drinking days than those in the assessment only condition.
Cognitive processing therapy and relapse prevention improved symptom severity and alcohol use to a similar degree.
Participants in both conditions reported similar less severe PTSD symptoms and fewer heavy drinking days after receiving treatment. Overall, from baseline to 12 months after treatment, cognitive processing therapy led to a 47% decrease in PTSD severity, and relapse prevention led to a 35% decrease in severity. Those in cognitive processing therapy also reported a 73% reduction in days of heavy drinking at 12-month follow-up compared to baseline, and those in relapse prevention reported an 82% decrease in heavy drinking days. These benefits related to both treatment conditions occurred by end of treatment and were maintained through the 12-month follow-up.
Cognitive processing therapy and relapse prevention did not differ on PTSD severity immediately after treatment.
Both interventions resulted in similar improvements in PTSD severity and heavy drinking days immediately post-treatment. Participants in the cognitive processing therapy reported a 40% reduction in PTSD severity immediately after treatment, and those in the relapse prevention treatment saw a 37% reduction.
Relapse prevention had greater immediate reduction on heavy drinking than cognitive processing therapy.
Although both treatments led to reduced heavy drinking days, those receiving the more explicitly alcohol-focused relapse prevention treatment reported fewer heavy drinking days on average after treatment than those in cognitive processing therapy. Those in relapse prevention reported 77% fewer drinking days immediately following treatment compared to baseline, with past-month heavy drinking days reducing from 13 at baseline to 3 post-treatment. Those in the cognitive processing group reported a 54% reduction in the number of drinking days, from 17 days at baseline to 9 post-treatment. The number of drinking days was not significantly different between the two groups. Those in the cognitive processing group also reported a 59% reduction in the number of heavy drinking days, from 12 heavy drinking days at baseline to 5 post-treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 101 adults with co-occurring posttraumatic stress disorder and alcohol use disorder found that both a more explicitly trauma-focused cognitive processing therapy and a more explicitly focused alcohol use disorder focused relapse prevention treatment both reduced posttraumatic stress disorder severity to the same degree, and the relapse prevention treatment led to greater reductions in heavy drinking days compared to cognitive processing therapy. The findings suggest that the common belief that the two disorders require disorder-specific or integrated treatments to show improvements may not be true, at least when treatments are delivered according to manualized protocols.
Participants in both types of treatments saw benefits in the non-targeted disorder. Yet, those in the relapse prevention treatment saw greater reductions in their days of heavy drinking compared to participants in cognitive processing therapy. It is noteworthy to mention that only 55% of participants completed a minimum of 9 out of 12 therapy sessions and only 54% completed the 12-month follow-up. The modest sample size and the high rate of non-completion limit the study’s findings. Nevertheless, the study found that there was not differential dropout between treatments. This implies that, although the dropout rate was high, it was likely not associated with specific features of either treatment.
These findings highlight the complexity of co-occurring disorders and the misconception that individuals with co-occurring disorders always require specifically designed treatments for those with co-occurring disorders. This is good news as it may mean that for individuals suffering from both alcohol use disorder and PTSD who are seeking treatment and who cannot find an available program or clinician who has specific treatment expertise addressing both types of disorders, may nevertheless be able to find relief from both types of disorders by accessing either a PTSD specialist, or, by accessing an addiction relapse prevention treatment specialist.
Recently released data from 2021 reports that 19.4 million adults in the US have a substance use disorder co-occurring with another mental illness. Substance use, including alcohol, may lead to the onset of symptoms of another mental illness. Yet, mental illness may also precede and lead to substance use as a method to alleviate symptoms related to a mental illness (e.g., anxiety, depression). Which disorder manifests first, severity of each disorder, compounding effects of one disorder on the other, and even specific types of traumas may also impact how effective single-focused and integrated treatments are on improving outcomes for some individuals and this requires further study.
Additionally, as the study highlights, treatments that more explicitly target specific disorders (i.e., alcohol use disorder relapse prevention) may also address to some degree other aspects of co-occurring mental health challenges. Relapse prevention, for example, includes specific curricula surrounding trauma—framing trauma as a trigger for substance use which can be addressed through the implementation of coping skills learned through the relapse prevention program. The application of behavioral and coping skills (e.g., communication, self-efficacy) may address underlying aspects of mental illness regardless of the primary disorder.
This study found that both cognitive processing therapy and relapse prevention improved posttraumatic stress disorder severity and days of heavy drinking, with relapse prevention linked to greater reductions in heavy drinking compared to cognitive processing therapy. These findings suggest that, if there are barriers to accessing PTSD-specific care, empirically supported alcohol use disorder treatments like the relapse prevention approach used here may help improve PTSD symptoms as well. Although both treatments were associated with improvements in PTSD symptoms and heavy drinking, this study did not compare these disorder-specific treatments with an integrated treatment approach. An integrated treatment approach has been found to be more effective in reducing substance use among individuals with PTSD compared to standard, non-manualized treatments. However, reductions in both alcohol use and PTSD symptom severity with an integrated therapy are comparable to the results found in this study suggesting these individuals may benefit equally well from any of these types of integrated or non-integrated approaches. More research is needed to understand who may benefit most from different types of treatment and how specific disorder specific and demographic characteristics impact treatment outcomes.
The study had a relatively small sample. Thus, the study was underpowered to detect small to moderate effects, which means that they did not have enough participants to observe minor improvements in outcomes.
The low rate of treatment completion (55% completed at least 9 out of 12 sessions) reduces the credibility and confidence in the study’s findings. However, this level of session treatment completion is typical in such treatment studies and dropout was not different between the two types of treatments, which instills confidence in the results.
Nearly half (46%) did not complete the 12-month follow-up. The low follow-up completion rate further reduces the sample size, which reduces confidence in the effects found for the treatments at the 12-month follow-up.
BOTTOM LINE
This study found that among adults with co-occurring posttraumatic stress disorder and alcohol use disorder, a more explicitly trauma focused cognitive processing therapy and a more alcohol addiction focused relapse prevention did not differ on benefits in posttraumatic stress disorder severity, but participants in relapse prevention reported greater reductions in heavy drinking compared to their counterparts in cognitive processing therapy. These findings suggest that treatment targeting one type of disorder likely has spillover therapeutic benefits on other mental illness symptoms. Particularly for those with co-occurring alcohol use disorder and posttraumatic stress disorders, seeking treatment for alcohol use will likely provide tools that can be used to navigate triggers related to trauma in addition to helping eliminate or reduce heavy alcohol use. Additionally, treatments such as relapse prevention and cognitive processing therapy may each include at least some more minor components that are nevertheless sufficient to address behaviors and symptoms that are not explicitly targeted by that particular therapy (e.g., trauma in relapse prevention, and substance use in cognitive processing therapy).This may be good news for individuals who suffer from both types of disorders who cannot find practitioners or programs locally with expertise in both disorders; finding a clinician who can address at least one well, may also have positive effects on the other.
For individuals and families seeking recovery: Receiving alcohol use disorder treatments like relapse prevention has been found to improve drinking as well as severity of other disorders, such as posttraumatic stress disorder in this study. Although it can be difficult at times to identify the best course of treatment for someone with co-occurring disorders, this study demonstrates that a more addiction-focused relapse prevention therapy improved posttraumatic stress disorder severity just as well as a specially designed treatment for posttraumatic stress disorder, and relapse prevention was also more helpful at reducing heavy alcohol use. This is good news if you suffer from both types of disorders but cannot find practitioners or programs locally with expertise in both disorders; finding a clinician who can address at least one well, may also have positive effects on the other.
For treatment professionals and treatment systems: The study found that an alcohol use disorder treatment (relapse prevention) improved PTSD severity as effectively as the PTSD treatment (cognitive processing therapy) yet led to greater reductions in heavy drinking days. Although this study did not include a treatment specifically designed for adults with co-occurring disorder, both types of treatment include components that address mental health issues outside of the primary target (e.g., trauma in relapse prevention, and substance use in cognitive processing therapy) and resulted in magnitudes of effect similar to integrated treatments that have been specifically designed for those with co-occurring disorders. Applying either treatment effectively for those with co-occurring PTSD is likely to provide similar benefit for the targeted as well as non-targeted disorder. Additionally, given this study’s findings, treatment professionals and systems may benefit from supporting an individual’s personal preference in selection of one of these two types of treatment when available.
For scientists:This randomized control trial demonstrated that both unmodified PTSD focused cognitive processing therapy and addiction-focused relapse prevention led to similar and helpful improvements in posttraumatic stress disorder severity and heavy drinking, with relapse prevention leading to a greater reduction in heavy drinking days compared to cognitive processing therapy. These findings suggest that targeting either disorder among adults with co-occurring posttraumatic stress disorder and alcohol use disorder can lead to improvements to the same degree as existing treatments that focus on co-occurring disorders, with a potential preference for relapse prevention therapy if reductions in heavy drinking are a particular important goal. Future studies may explore how unique presentations of co-occurrence regarding disorder precedent, severity, and chronicity impact treatment.
For policy makers: The prevalence rate of adults with the co-occurrence of substance use disorders and another mental health illness is increasing, and understanding how existing treatments that may target a specific disorder can reduce symptom severity of other disorders is likely to benefit individuals with co-occurring disorders and relieve societal burden (e.g., medical cost, work hours). Additional funding to support the analysis of cross-treatment effects could improve the well-being of many individuals with co-occurring disorders that do not have access to integrated treatments and/or prefer specific treatment targets.
2 out of 3 adults in the US. that have had a posttraumatic stress disorder also have had an alcohol use disorder during their life. Additionally, 1 out of 10 adults that have had an alcohol use disorder have also had a posttraumatic stress disorder. Given the high co-occurrence of these two disorders, evidence identifying the best course or type of treatment would help clinical providers and those with these disorders make treatment decisions.
Conventional wisdom and practice suggest that alcohol use disorder and posttraumatic stress disorder should be treated separately through targeted treatments or through specifically designed interventions that integrate treatments for both trauma and alcohol use disorder. However, many clinics are under-resourced to develop, maintain, and staff specialized programs addressing both disorders. If a single-focus treatment could address both disorders, resources could be diverted to increasing the fidelity of that single-focus treatment rather than investing in training for new treatments.
This study sought to explore whether a single-focus treatment for posttraumatic stress disorder alone or for alcohol use disorder alone led to improvements in both types of outcomes among adults with co-occurring posttraumatic stress disorder and alcohol use disorder.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized control trial of adults that took place at an academic hospital-affiliated mental health clinic and a Veteran Affairs (VA)-based research clinic in the Pacific Northwest. Recruitment for the study began in November 2013, and all study interventions were completed by August 2018. Adults were recruited through ads in newspapers, flyers, and letters sent after identifying eligibility via medical records. Thus, individuals participating made the conscious decision to self-select into a treatment study, which included the eligibility criteria of having a desire to eliminate or reduce alcohol use. The study recruited 101 participants. Participants met DSM-5 criteria for posttraumatic stress disorder and alcohol use disorder, reported at least 2 heavy drinking days (5+/4+ standard drinks per day for men/women) or 2 weeks of heavy drinking (21+/14+ drinks per week for men/women) in the past month, have a desire to abstain or reduce alcohol use, be fluent in English, and be 18 or older. Individuals were excluded from study participation if they met any of the following criteria: having a psychotic or uncontrolled bipolar disorder, having attempted suicide or engaged in serious self-harm within the past 3 months or having suicidal ideation with a specific plan or intent within the past 2 months, being in a currently violent interpersonal relationship, experiencing alcohol withdrawal at the time of consent, having unstable psychiatric medication use within the past 3 months, having used a medication to treat alcohol use disorder (e.g., disulfiram, acamprosate) within the past month, or having participated in trauma-focused mental health treatment or behaviorally-focused alcohol treatment within the past month.
Participants were randomly assigned to one of three groups: cognitive processing therapy, relapse prevention, or assessment only.
Cognitive Processing Therapy is a treatment that aims to help clients modify their thoughts about the causes of traumatic events and their overly broad beliefs with worksheets and questioning techniques. The therapy focuses on teaching clients to challenge and change cognitions underlying their distressing experiences. Within cognitive processing therapy, alcohol use is considered an avoidance behavior (i.e., drinking to avoid experiencing unpleasant PTSD symptoms) and addressed by challenging alcohol-related maladaptive thought patterns.
Relapse prevention is a cognitive-behavioral therapy approach that focuses on helping individuals develop self-monitoring and coping skills to handle situations that may lead to excessive alcohol consumption. The goal is to prevent relapse by equipping individuals with the tools they need to manage their recovery. Relapse prevention addressed posttraumatic stress by encouraging participants to practice the skills they’re learning when they experience trauma-related symptoms – so that these PTSD-related experiences don’t “trigger” a drinking (or heavy drinking) episode.
Both treatments were 12 sessions long and of similar duration with participants attending one or two sessions per week for up to 20 weeks. The “assessment only” condition consisted of weekly brief (15min) phone calls from a study therapist to provide support/safety monitoring. Those that were initially assigned to the assessment only group were subsequently randomly assigned once more to one of the two active treatment groups – either cognitive processing therapy or relapse prevention after six weeks of receiving no treatment.
Participants completed validated assessments to measure changes in alcohol use and posttraumatic stress disorder severity at baseline, post-treatment, 3- and 12-month follow-up points. For alcohol use, the main outcomes were days of alcohol use and heavy drinking days (5+/4+ standard drinks for men/women). Posttraumatic stress disorder severity ranged from 0 – 80, with higher scores representing higher severity. Those that were first assigned to the assessment only condition were given an additional assessment following their six-week period of no treatment.
A total of 101 adults participated in the study. The average age was 42, and 56% of the participants identified as female while 53% identified as White. Over half (60%) were single, 33% had graduated college, 29% were veterans, and 38% were employed. About one in three (36%) reported their worst traumatic events as sexual assault, and another third (33%) reported their worst as physical assault. About one in three (39%) also meet criteria for another drug use disorder besides alcohol (other than tobacco).
WHAT DID THIS STUDY FIND?
Individuals in the assessment only condition made improvements prior to treatment.
Individuals assigned to the assessment only condition, which only included brief weekly phone calls for support/safety monitoring, showed improvements in both PTSD severity and heavy drinking days after the six-week period. However, those in both of the active treatment conditions experienced greater benefit on both PTSD severity and heavy drinking days than those in the assessment only condition.
Cognitive processing therapy and relapse prevention improved symptom severity and alcohol use to a similar degree.
Participants in both conditions reported similar less severe PTSD symptoms and fewer heavy drinking days after receiving treatment. Overall, from baseline to 12 months after treatment, cognitive processing therapy led to a 47% decrease in PTSD severity, and relapse prevention led to a 35% decrease in severity. Those in cognitive processing therapy also reported a 73% reduction in days of heavy drinking at 12-month follow-up compared to baseline, and those in relapse prevention reported an 82% decrease in heavy drinking days. These benefits related to both treatment conditions occurred by end of treatment and were maintained through the 12-month follow-up.
Cognitive processing therapy and relapse prevention did not differ on PTSD severity immediately after treatment.
Both interventions resulted in similar improvements in PTSD severity and heavy drinking days immediately post-treatment. Participants in the cognitive processing therapy reported a 40% reduction in PTSD severity immediately after treatment, and those in the relapse prevention treatment saw a 37% reduction.
Relapse prevention had greater immediate reduction on heavy drinking than cognitive processing therapy.
Although both treatments led to reduced heavy drinking days, those receiving the more explicitly alcohol-focused relapse prevention treatment reported fewer heavy drinking days on average after treatment than those in cognitive processing therapy. Those in relapse prevention reported 77% fewer drinking days immediately following treatment compared to baseline, with past-month heavy drinking days reducing from 13 at baseline to 3 post-treatment. Those in the cognitive processing group reported a 54% reduction in the number of drinking days, from 17 days at baseline to 9 post-treatment. The number of drinking days was not significantly different between the two groups. Those in the cognitive processing group also reported a 59% reduction in the number of heavy drinking days, from 12 heavy drinking days at baseline to 5 post-treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study of 101 adults with co-occurring posttraumatic stress disorder and alcohol use disorder found that both a more explicitly trauma-focused cognitive processing therapy and a more explicitly focused alcohol use disorder focused relapse prevention treatment both reduced posttraumatic stress disorder severity to the same degree, and the relapse prevention treatment led to greater reductions in heavy drinking days compared to cognitive processing therapy. The findings suggest that the common belief that the two disorders require disorder-specific or integrated treatments to show improvements may not be true, at least when treatments are delivered according to manualized protocols.
Participants in both types of treatments saw benefits in the non-targeted disorder. Yet, those in the relapse prevention treatment saw greater reductions in their days of heavy drinking compared to participants in cognitive processing therapy. It is noteworthy to mention that only 55% of participants completed a minimum of 9 out of 12 therapy sessions and only 54% completed the 12-month follow-up. The modest sample size and the high rate of non-completion limit the study’s findings. Nevertheless, the study found that there was not differential dropout between treatments. This implies that, although the dropout rate was high, it was likely not associated with specific features of either treatment.
These findings highlight the complexity of co-occurring disorders and the misconception that individuals with co-occurring disorders always require specifically designed treatments for those with co-occurring disorders. This is good news as it may mean that for individuals suffering from both alcohol use disorder and PTSD who are seeking treatment and who cannot find an available program or clinician who has specific treatment expertise addressing both types of disorders, may nevertheless be able to find relief from both types of disorders by accessing either a PTSD specialist, or, by accessing an addiction relapse prevention treatment specialist.
Recently released data from 2021 reports that 19.4 million adults in the US have a substance use disorder co-occurring with another mental illness. Substance use, including alcohol, may lead to the onset of symptoms of another mental illness. Yet, mental illness may also precede and lead to substance use as a method to alleviate symptoms related to a mental illness (e.g., anxiety, depression). Which disorder manifests first, severity of each disorder, compounding effects of one disorder on the other, and even specific types of traumas may also impact how effective single-focused and integrated treatments are on improving outcomes for some individuals and this requires further study.
Additionally, as the study highlights, treatments that more explicitly target specific disorders (i.e., alcohol use disorder relapse prevention) may also address to some degree other aspects of co-occurring mental health challenges. Relapse prevention, for example, includes specific curricula surrounding trauma—framing trauma as a trigger for substance use which can be addressed through the implementation of coping skills learned through the relapse prevention program. The application of behavioral and coping skills (e.g., communication, self-efficacy) may address underlying aspects of mental illness regardless of the primary disorder.
This study found that both cognitive processing therapy and relapse prevention improved posttraumatic stress disorder severity and days of heavy drinking, with relapse prevention linked to greater reductions in heavy drinking compared to cognitive processing therapy. These findings suggest that, if there are barriers to accessing PTSD-specific care, empirically supported alcohol use disorder treatments like the relapse prevention approach used here may help improve PTSD symptoms as well. Although both treatments were associated with improvements in PTSD symptoms and heavy drinking, this study did not compare these disorder-specific treatments with an integrated treatment approach. An integrated treatment approach has been found to be more effective in reducing substance use among individuals with PTSD compared to standard, non-manualized treatments. However, reductions in both alcohol use and PTSD symptom severity with an integrated therapy are comparable to the results found in this study suggesting these individuals may benefit equally well from any of these types of integrated or non-integrated approaches. More research is needed to understand who may benefit most from different types of treatment and how specific disorder specific and demographic characteristics impact treatment outcomes.
The study had a relatively small sample. Thus, the study was underpowered to detect small to moderate effects, which means that they did not have enough participants to observe minor improvements in outcomes.
The low rate of treatment completion (55% completed at least 9 out of 12 sessions) reduces the credibility and confidence in the study’s findings. However, this level of session treatment completion is typical in such treatment studies and dropout was not different between the two types of treatments, which instills confidence in the results.
Nearly half (46%) did not complete the 12-month follow-up. The low follow-up completion rate further reduces the sample size, which reduces confidence in the effects found for the treatments at the 12-month follow-up.
BOTTOM LINE
This study found that among adults with co-occurring posttraumatic stress disorder and alcohol use disorder, a more explicitly trauma focused cognitive processing therapy and a more alcohol addiction focused relapse prevention did not differ on benefits in posttraumatic stress disorder severity, but participants in relapse prevention reported greater reductions in heavy drinking compared to their counterparts in cognitive processing therapy. These findings suggest that treatment targeting one type of disorder likely has spillover therapeutic benefits on other mental illness symptoms. Particularly for those with co-occurring alcohol use disorder and posttraumatic stress disorders, seeking treatment for alcohol use will likely provide tools that can be used to navigate triggers related to trauma in addition to helping eliminate or reduce heavy alcohol use. Additionally, treatments such as relapse prevention and cognitive processing therapy may each include at least some more minor components that are nevertheless sufficient to address behaviors and symptoms that are not explicitly targeted by that particular therapy (e.g., trauma in relapse prevention, and substance use in cognitive processing therapy).This may be good news for individuals who suffer from both types of disorders who cannot find practitioners or programs locally with expertise in both disorders; finding a clinician who can address at least one well, may also have positive effects on the other.
For individuals and families seeking recovery: Receiving alcohol use disorder treatments like relapse prevention has been found to improve drinking as well as severity of other disorders, such as posttraumatic stress disorder in this study. Although it can be difficult at times to identify the best course of treatment for someone with co-occurring disorders, this study demonstrates that a more addiction-focused relapse prevention therapy improved posttraumatic stress disorder severity just as well as a specially designed treatment for posttraumatic stress disorder, and relapse prevention was also more helpful at reducing heavy alcohol use. This is good news if you suffer from both types of disorders but cannot find practitioners or programs locally with expertise in both disorders; finding a clinician who can address at least one well, may also have positive effects on the other.
For treatment professionals and treatment systems: The study found that an alcohol use disorder treatment (relapse prevention) improved PTSD severity as effectively as the PTSD treatment (cognitive processing therapy) yet led to greater reductions in heavy drinking days. Although this study did not include a treatment specifically designed for adults with co-occurring disorder, both types of treatment include components that address mental health issues outside of the primary target (e.g., trauma in relapse prevention, and substance use in cognitive processing therapy) and resulted in magnitudes of effect similar to integrated treatments that have been specifically designed for those with co-occurring disorders. Applying either treatment effectively for those with co-occurring PTSD is likely to provide similar benefit for the targeted as well as non-targeted disorder. Additionally, given this study’s findings, treatment professionals and systems may benefit from supporting an individual’s personal preference in selection of one of these two types of treatment when available.
For scientists:This randomized control trial demonstrated that both unmodified PTSD focused cognitive processing therapy and addiction-focused relapse prevention led to similar and helpful improvements in posttraumatic stress disorder severity and heavy drinking, with relapse prevention leading to a greater reduction in heavy drinking days compared to cognitive processing therapy. These findings suggest that targeting either disorder among adults with co-occurring posttraumatic stress disorder and alcohol use disorder can lead to improvements to the same degree as existing treatments that focus on co-occurring disorders, with a potential preference for relapse prevention therapy if reductions in heavy drinking are a particular important goal. Future studies may explore how unique presentations of co-occurrence regarding disorder precedent, severity, and chronicity impact treatment.
For policy makers: The prevalence rate of adults with the co-occurrence of substance use disorders and another mental health illness is increasing, and understanding how existing treatments that may target a specific disorder can reduce symptom severity of other disorders is likely to benefit individuals with co-occurring disorders and relieve societal burden (e.g., medical cost, work hours). Additional funding to support the analysis of cross-treatment effects could improve the well-being of many individuals with co-occurring disorders that do not have access to integrated treatments and/or prefer specific treatment targets.