Online mutual-help meetings: Who attends and do they benefit?
The closure of in-person meetings at the beginning of the COVID-19 pandemic brought digital recovery supports like online mutual-help meetings into the mainstream. This study of individuals with lifetime alcohol use disorder conducted pre-COVID examined factors associated with attending meetings online and whether online mutual-help attendance was associated with improved likelihood of abstinence.
Although online mutual-help groups have existed for some time, the closure of in-person meetings at the beginning of the COVID-19 pandemic has resulted in more people engaging with these groups. It is a longstanding reality that only a small minority of people with substance use disorders receive treatment. More easily accessible online mutual-help groups and other online recovery support services have the potential to address systemic barriers to treatment access, including lack of childcare, the need to continue working, transportation, and cost.
In parts of the country, the only available mutual-help meetings are 12-step recovery groups such as Alcoholics Anonymous. While research strongly supports the effectiveness of Alcoholics Anonymous (AA) for alcohol use disorder, with some evidence suggesting 12-step groups are effective for cocaine and methamphetamine use disorders, 12-steps groups may not be the best option for all individuals. Other mutual-help groups such as Self-Management and Recovery Training (SMART), Women for Sobriety, LifeRing Secular Recovery, Refuge Recovery, Celebrate Recovery, or Harm Reduction Works might be a better fit for these individuals philosophically or supportive of non-abstinence recovery goals, and are also all available online. As such, remote access through the internet allows people in recovery to access these resources when no in-person meetings exist in their area. Similarly, culturally informed addiction treatment or recovery support offered by professionals of color is another critical absence in large sections of the country. Online mutual-help groups for people of color (“affinity groups”) may help address this issue as well.
Researchers have suggested that online meetings support recovery in similar ways to in-person meetings. Anecdotal reports, not to mention the scale of their utilization, indicate that people find them helpful. There appears to be minimal risks for harmful interactions in online meeting participation. However, we currently have little data on who attends online meetings, their level of effectiveness compared to in-person meetings, how people combine online and in-person supports, and the mechanisms through which they support change. We also lack sufficient research on whether some platforms or points of accessing online meetings are more effective than others. This study examined the demographics, substance use and recovery characteristics, and primary mutual-help group affiliation of online recovery group attendees and the association of online meeting attendance with substance use outcomes.
HOW WAS THIS STUDY CONDUCTED?
Researchers reanalyzed data collected in 2015-16 for the Peer Alternative in Addiction study, which compared the effectiveness of mutual-help organizations such as AA, Women for Sobriety, LifeRing Secular Recovery, and Self-Management and Recovery Training (SMART). The original study, conducted before the COVID-19 pandemic, included 647 U.S. adults over the age of 18 with lifetime alcohol use disorder. Participants were recruited through working with the national leaderships of SMART and LifeRing and, for 12-step members, online through the website “In the Rooms.” (In the Rooms is a website where members, who can sign up for a free account, gain access to online meetings as well as features like blogs, chat rooms, and direct messaging with other members.) Study participants completed an initial survey (“baseline”) and then were followed up at 6 months (with 81% responding) and 12 months (with 86% percent responding). At baseline, 62 percent of survey respondents had attended at least one online mutual-help meeting in their lifetime and 36 percent had done so in the last 30 days.
The original study collected information on demographics, substance use and recovery, and the ways that participants engaged with mutual-help groups. For demographics, participants were asked about gender, race, ethnicity, marital status, education, employment, annual income, and whether they lived in urban, rural, or suburban areas. For substance use and recovery characteristics, participants were asked how recently they had used alcohol, how recently they had used other substances, and their alcohol recovery goal (total abstinence forever vs. drink after abstinence period/occasionally). For mutual-help group characteristics, participants were asked the number of meetings they had attended in the last 30 days, the types of groups they attended, their “primary group” (AA, LifeRing, SMART etc.), how involved they were with their primary group (including whether they had a home group/regular meeting, how regularly they attended their primary group, and their level of participation in group activities), their satisfaction with the primary group, and about primary group cohesion (for example, the extent to which the felt like they belonged or were valued).
In this new analysis, the study team looked at three questions. First, they used statistical tests to establish whether associations exist between demographics, substance use/recovery characteristics, or mutual-help utilization and online meeting attendance. Second, they created a model that allowed them to compare how well baseline characteristics such as recent alcohol and drug use, alcohol recovery goal, alcohol use severity, and alcohol abstinence self-efficacy predicted online mutual-help attendance. Third, they created a different model to test whether the association between online mutual-help attendance and abstinence was the same at baseline, 6 months, and 12 months, or whether this association changed at these different points in time.
WHAT DID THIS STUDY FIND?
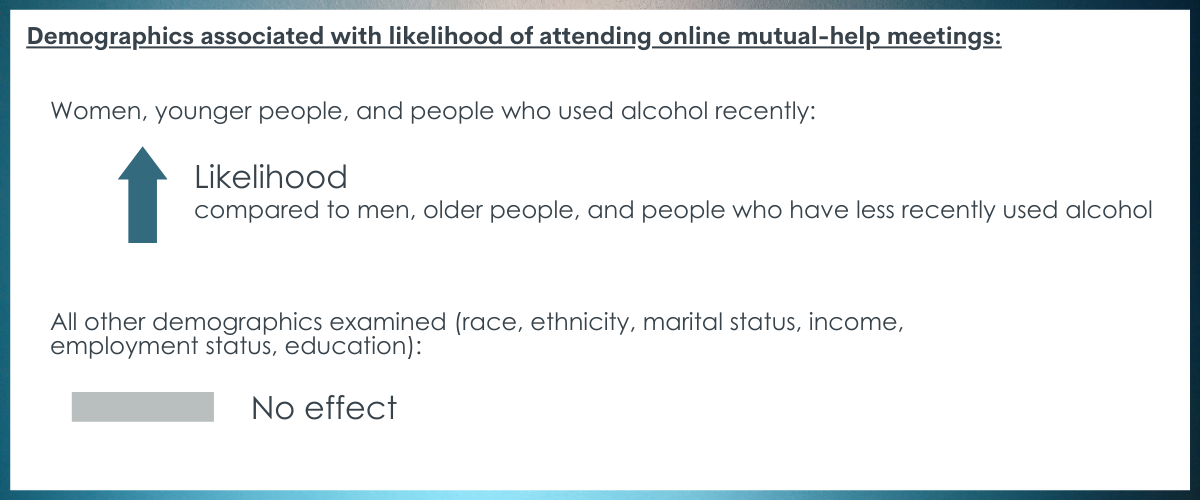
Women, younger people, and people who used alcohol recently were more likely to attend online meetings.
The analysis found that meeting attendance was less likely among men than women. On the whole, participants who attended online meetings were younger than those who had not. Otherwise, demographics characteristics such as race, ethnicity, marital status, income, employment status, and education were not associated with increased likelihood of online meeting attendance. At baseline, participants who used alcohol in the past 30 days, and from 30 days to 1 year in the past, were more likely to attend online meetings than those who last drank over 1 year before. Regarding other substance use, participants who used other substances within the past 30 days to 1 year were more likely to attend online meetings than those whose last episode of use was over 5 years before. In addition, other substance use from 1 to 5 years ago was associated with greater odds of online meetings attendance than use over 5 years in the past.
Online attendance was associated with severity of alcohol problems and 12-step affiliation, but no association existed between online attendance and recovery goal.
In contrast to participants who did not attend online meetings, participants who attended online meetings had greater severity of alcohol use and alcohol problems and were less confident about their ability to resist drinking heavily. Current alcohol recovery goal—lifetime time absence versus some form or reduced or controlled drinking—was not associated with higher odds of online meeting attendance. Participants who attended more than one mutual-help group were more likely to attend on-line meetings. Additionally, participants whose primary mutual-help-group was 12-step meetings or Women for Sobriety were also more likely to attend online meetings in comparison to those who identified SMART or LifeRing as their primary group. Involvement in their primary group was lower among participants who attended online meetings.
Despite lower likelihood for abstinence at baseline, participants in online meetings may have comparable abstinence at 6, 12 months.
At baseline, participants who attended online meetings were less likely to be abstinent from alcohol. At 6 months, however, there was increased odds for online participants to be abstinent. At 12 months online meeting attendees had similar rates of abstinence compared to those who did not attend an online meeting (i.e., those only attending in-person or those who did not attend any meetings). However, this change in rates of abstinence over time may be an artifact of the statistical models used by the researchers. When they included the type of primary mutual-help group and attendance of multiple groups in their model, the association between online group attendance and lower abstinence rates remained, while the increased odds of abstinence at 6 and 12 months disappeared.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This secondary analysis of data from a 2015 study provides insights into what factors might predict online meeting attendance. Although not representative of current online meeting attendance, these insights can be combined with data from other studies to help guide both researchers examining the effectiveness of online mutual-help meetings and providers who want to support clients accessing recovery supports online.
Even before the COVID-19 pandemic, a majority of participants in the study had attended an online mutual-help meeting. While the number of online meeting attendees in this study probably reflected their recruitment of 12-step study participants (the majority of participants) from the website “In the Rooms,” the fact that the attendance was consistent across race, ethnicity, marital status, income, employment status, and education is notable and encouraging.
Given the persistent low numbers of people with substance use disorders that receive any type of treatment, online mutual-help meetings may help address existing barriers to care, for example employment, childcare, transportation, and the high cost of addiction treatment. At the same time, it is important to remember that 1 in 4 Americans do not have access to broadband internet and, even among those who do, not everyone has access to a safe or otherwise suitable environment where they can utilize online recovery supports. Consistent with other research on tele-healthand online supports, this study found that women and younger people were more likely to attend online meetings. Women, culturally, may have more domestic responsibilities (e.g., childcare, family meal preparation) that makes online participation particularly convenient and time-saving. This finding is also consistent with studies that show that men are less likely in general to seek support or mental health challenges than women and women approach health issues utilizing multiple sources. Men and older adults may benefit from targeted education about online recovery supports and, in the case of older adults, technical assistance.
Other important findings from this study include that people who attend online meetings are more likely to have drunk alcohol or consumed drugs recently, have more severe drinking problems, and have less confidence in meeting their drinking goals. The study authors interpret these findings to mean that online resources might be particularly attractive to people in early recovery, who are seeking out resources and trying different options to build connections. On this basis, providers might suggest online meetings as a low-threshold recovery support to individuals seeking recovery or early in their recovery process. At the same time, more recent or severe use does not necessarily indicate that a person is in early recovery. Other researchers have suggested the greater anonymity of online spaces may allow individuals pursuing harm reduction goals (moderate use; abstinence from one substance combined with moderate use of other) to participate in mutual-help meetings without worrying about judgement from people practicing more traditional, abstinence-only recovery, although many organizations such as SMART Recovery support non-abstinence goals in their meetings whether in person or online. Similarly, the greater anonymity offered by online meetings (not turning on one’s camera; attending meeting out of one’s geographical area) may also allow people returning to mutual-help group participation after a reoccurrence of use who are feeling guilt or shame. Further research is needed to see whether the association between online meeting attendance and recent/more severe drinking and substance use generalizes to other populations and what, if any, implications it has for recovery support and clinical care.
While attendees of online meetings were more likely to have drunk recently, the researcher’s analysis found that those attending online meetings have increased odds of abstinence at 6 months and equivalent odds of abstinence to other study participants at 12 months (although the increased likelihood of abstinence at 12 months was not large enough to be distinguishable from a chance effect). In other words, it appears that online meeting attendees may achieve similar rates of abstinence as other study participants not attending online meetings over time. However, this convergence disappeared when the model included primary mutual-help affiliation and the attendance of more than one type of group, with 12-step membership predicting higher odds of 6- and 12-month abstinence.
It is not entirely clear what this means. It may be an effect particular to the study’s sample. Participants from LifeRing and SMART were recruited from the general population of members with the aid of national organizations. Because of the historic culture of anonymity, participants from 12-step organization were recruited from an online meeting platform, In the Rooms. What may have happened is that 12-step affiliated participants were both more likely to attend meeting online (since they were recruited from the online resource,“In the Rooms”) and they had higher rates of abstinence in this study. It also should be remembered that not all study participants had abstinence as their stated recovery goal, therefore lower rates of abstinence among non-12-step group members that attend online meetings may not represent worse outcomes/. Rather, they may be in keeping with their initial goal.
Based on research into in-person mutual-help meetings, there are potential disadvantages to attending online meetings solely. Active involvement in meetings—for example, getting a sponsor, socializing with other people in recovery outside of meetings, or joining a home group—generally results in better substance related outcomes than meeting attendance alone. Developing these types of supportive connections may be more difficult online. The benefits of mutual-help meetings are in large part explained by peer-to-peer social interaction. In online group therapy, a possible parallel to online mutual-help meetings, group connection may be harder to develop. While more research is needed, it may be that individuals who have previous experience with in-person recovery groups and are more stably in remission are better able to adapt to the ways online groups support recovery goals. In turn, individuals who have only attended online meetings may benefit from groups that have professional facilitation and off-line components.
Finally, it is worth noting that online mutual-help groups (much like their in-person counterparts) will vary greatly in focus, format, culture, and demographic composition. No best practices exist for mutual-help groups that hold across different spaces; nor is there a mechanism or governance body to report negative experiences. When making referrals, clinicians should familiarize themselves with the different online options available and consider recommending meetings offered through the official sites of mutual-help organizations or those where facilitators and other safety monitors uphold community guidelines.
As the authors recognize, this study was unable to guarantee that its samples were representative of the large populations of the mutual-help groups in question. More research is needed to determine to what extent these finds generalize.
This study was conducted before the COVID-19 pandemic and the increased utilization of online mutual-help meetings caused by the shutdown of in-person meetings. Further research is needed to understand how this cultural shift may have affected who is attending online meetings and how they are utilizing them for recovery supports.
BOTTOM LINE
This secondary analysis of data from a 2015 study provides insights into what factors might predict online meeting attendance. The majority of study participants had attended an online mutual-help meeting, reflecting the fact that online meetings had become an increasingly popular form of recovery support before COVID-19. Echoing other research on tele-health and similar services, online meeting attendees in this study were more likely to be younger and female. Although it may not generalize to other populations, attendees in this study were also more likely to have drank or used substances recently, more likely to attend more than one type of mutual-help group (AA, LifeRing, SMART, etc.), and more likely to have problems of greater severity. It may be that individuals early in recovery find online mutual-help meetings to be a more accessible, “lower threshold” form of recovery support. However, further researcher is needed on online meeting attendance to understand what factors explain this association or if it generalizes to other populations.
For individuals and families seeking recovery: Online mutual-help meetings are now part of many people’s recovery programs. For many people in recovery, they have provided greater access to meetings and allowed them to work around challenges related to work schedule, childcare, transport, and disability access. While 12-step groups are the only available type of mutual-help meeting in much of the country, online meetings give people in or seeking help for their recovery access to multiple other options that may better fit their recovery preferences, philosophy, or goals, such as SMART, LifeRing, Women in Sobriety, All Recovery Meetings, and Harm Reduction Works. This may be especially true for atheists/agnostics who may not connect with the spiritual basis of 12-step philosophy and individuals pursuing moderation or Harm Reduction goals. At the same time, people in recovery should be aware that the effectiveness of mutual-help groups appears to be connected to active involvement (such as getting a sponsor, service, and socializing), developing recovery supportive social networks, and group accountability. It may be more difficult to develop these types of connections through online meeting attendance alone. While more research is needed,people in early recovery may benefit more from combining online meetings and active participation in in-person groups than from attending online meetings alone.
For treatment professionals and treatment systems: Online mutual-help meetings are becoming an increasingly popular option for recovery support, in no small part because their accessibility through the internet lets individuals work around obstacles to traditional treatment and recovery support services (employment, the lack of childcare, transport, and cost). Initial evidence indicates that women and younger people are more likely to utilize online recovery support. It may be that additional efforts are needed to inform men and older adults of these resources and support them in becoming familiar with their format. This study also raises the possibility that people early in recovery might find it easier to engage in online meetings before trying traditional meetings. At the same time, there are reasons to suspect that online meeting attendance alone may not have the same benefits as either traditional meetings or combining online and traditional meetings. The benefits of mutual-help meetings are in large part explained by peer-to-peer social interaction. Recovery supportive social networks may be harder to develop online. Finally, it is worth noting that, just like in person meetings, online mutual-help groups will vary in focus, format, culture, and demographic composition. When making referrals, treatment professionals should familiarize themselves with the different online options available and consider recommending meetings offered through the official sites of mutual-help organizations, such as the SMART website, or platforms like Unity Recovery, where facilitators uphold community guidelines.
For scientists:This article contributes to a small, but growing, body of research into online mutual aid meetings. Based on a secondary analysis of a 2015 study of mutual-help groups (AA, SMART, LifeRing, Women for Sobriety), the authors find that online attendance is more likely among women and younger people, people who attended more than one type of mutual held group, people who had consumed alcohol and other substances more recently, people with more sever alcohol problems, and people with less confidence of maintaining abstinence. Further research is needed to see whether these associations generalize to other populations, especially after the widespread shift to utilizing online mutual-help meetings during COVID-19. Especially notable is the finding that online meeting attendance in this sample is associated with more recent use, which may suggest that people in early recovery find online meetings more accessible than in-person meetings. More research is needed on who attends online meetings, their level of effectiveness overall as well as their effectiveness compared to in-person meetings specifically, how people combine online and in-person supports, the mechanisms through which they support change, and whether some platforms or points of access are more effective than others.
For policy makers: The beginning of COVID-19 witnessed the rapid and unplanned closure of in-person mutual help meetings. Although available before the pandemic, online mutual-help meetings provided people with an alternative source of support and allowed many to access peer-to-peer support for the first time. Although the data is currently limited,many people report finding online mutual aid meetings helpful and there appear to be few risks to accessing support in this format. This article suggests that people in early recovery may find online meetings more accessible and easier to access than more traditional, in-person meetings. At the same time, there are reasons to suspect that online meeting attendance alone may not have the same benefits as either attending traditional in-person meetings or combining online and traditional meetings. We currently have little data on who attends online meetings, their level of effectiveness compared to in-person meetings, and whether some platforms or points of access are more effective than others. Given the large number of people who are now utilizing these resources, this is a crucial research area to support. Finally, it is important to remember that 1 in 4 Americans do not have access to broadband internet and people in lower income strata, as well as Black and Latino individuals, are less likely to have broadband access. Encouraging increased reliance on online recovery supports, while failing to expand access to traditional in-person recovery supports, may ameliorate some issues of access while accentuating other disparities. Given this disparity in broadband access, the need for widespread broadband infrastructure has taken on outsized importance with the mainstreaming of online mutual-help meetings as well as more formal telehealth services.
Although online mutual-help groups have existed for some time, the closure of in-person meetings at the beginning of the COVID-19 pandemic has resulted in more people engaging with these groups. It is a longstanding reality that only a small minority of people with substance use disorders receive treatment. More easily accessible online mutual-help groups and other online recovery support services have the potential to address systemic barriers to treatment access, including lack of childcare, the need to continue working, transportation, and cost.
In parts of the country, the only available mutual-help meetings are 12-step recovery groups such as Alcoholics Anonymous. While research strongly supports the effectiveness of Alcoholics Anonymous (AA) for alcohol use disorder, with some evidence suggesting 12-step groups are effective for cocaine and methamphetamine use disorders, 12-steps groups may not be the best option for all individuals. Other mutual-help groups such as Self-Management and Recovery Training (SMART), Women for Sobriety, LifeRing Secular Recovery, Refuge Recovery, Celebrate Recovery, or Harm Reduction Works might be a better fit for these individuals philosophically or supportive of non-abstinence recovery goals, and are also all available online. As such, remote access through the internet allows people in recovery to access these resources when no in-person meetings exist in their area. Similarly, culturally informed addiction treatment or recovery support offered by professionals of color is another critical absence in large sections of the country. Online mutual-help groups for people of color (“affinity groups”) may help address this issue as well.
Researchers have suggested that online meetings support recovery in similar ways to in-person meetings. Anecdotal reports, not to mention the scale of their utilization, indicate that people find them helpful. There appears to be minimal risks for harmful interactions in online meeting participation. However, we currently have little data on who attends online meetings, their level of effectiveness compared to in-person meetings, how people combine online and in-person supports, and the mechanisms through which they support change. We also lack sufficient research on whether some platforms or points of accessing online meetings are more effective than others. This study examined the demographics, substance use and recovery characteristics, and primary mutual-help group affiliation of online recovery group attendees and the association of online meeting attendance with substance use outcomes.
HOW WAS THIS STUDY CONDUCTED?
Researchers reanalyzed data collected in 2015-16 for the Peer Alternative in Addiction study, which compared the effectiveness of mutual-help organizations such as AA, Women for Sobriety, LifeRing Secular Recovery, and Self-Management and Recovery Training (SMART). The original study, conducted before the COVID-19 pandemic, included 647 U.S. adults over the age of 18 with lifetime alcohol use disorder. Participants were recruited through working with the national leaderships of SMART and LifeRing and, for 12-step members, online through the website “In the Rooms.” (In the Rooms is a website where members, who can sign up for a free account, gain access to online meetings as well as features like blogs, chat rooms, and direct messaging with other members.) Study participants completed an initial survey (“baseline”) and then were followed up at 6 months (with 81% responding) and 12 months (with 86% percent responding). At baseline, 62 percent of survey respondents had attended at least one online mutual-help meeting in their lifetime and 36 percent had done so in the last 30 days.
The original study collected information on demographics, substance use and recovery, and the ways that participants engaged with mutual-help groups. For demographics, participants were asked about gender, race, ethnicity, marital status, education, employment, annual income, and whether they lived in urban, rural, or suburban areas. For substance use and recovery characteristics, participants were asked how recently they had used alcohol, how recently they had used other substances, and their alcohol recovery goal (total abstinence forever vs. drink after abstinence period/occasionally). For mutual-help group characteristics, participants were asked the number of meetings they had attended in the last 30 days, the types of groups they attended, their “primary group” (AA, LifeRing, SMART etc.), how involved they were with their primary group (including whether they had a home group/regular meeting, how regularly they attended their primary group, and their level of participation in group activities), their satisfaction with the primary group, and about primary group cohesion (for example, the extent to which the felt like they belonged or were valued).
In this new analysis, the study team looked at three questions. First, they used statistical tests to establish whether associations exist between demographics, substance use/recovery characteristics, or mutual-help utilization and online meeting attendance. Second, they created a model that allowed them to compare how well baseline characteristics such as recent alcohol and drug use, alcohol recovery goal, alcohol use severity, and alcohol abstinence self-efficacy predicted online mutual-help attendance. Third, they created a different model to test whether the association between online mutual-help attendance and abstinence was the same at baseline, 6 months, and 12 months, or whether this association changed at these different points in time.
WHAT DID THIS STUDY FIND?
Women, younger people, and people who used alcohol recently were more likely to attend online meetings.
The analysis found that meeting attendance was less likely among men than women. On the whole, participants who attended online meetings were younger than those who had not. Otherwise, demographics characteristics such as race, ethnicity, marital status, income, employment status, and education were not associated with increased likelihood of online meeting attendance. At baseline, participants who used alcohol in the past 30 days, and from 30 days to 1 year in the past, were more likely to attend online meetings than those who last drank over 1 year before. Regarding other substance use, participants who used other substances within the past 30 days to 1 year were more likely to attend online meetings than those whose last episode of use was over 5 years before. In addition, other substance use from 1 to 5 years ago was associated with greater odds of online meetings attendance than use over 5 years in the past.
Online attendance was associated with severity of alcohol problems and 12-step affiliation, but no association existed between online attendance and recovery goal.
In contrast to participants who did not attend online meetings, participants who attended online meetings had greater severity of alcohol use and alcohol problems and were less confident about their ability to resist drinking heavily. Current alcohol recovery goal—lifetime time absence versus some form or reduced or controlled drinking—was not associated with higher odds of online meeting attendance. Participants who attended more than one mutual-help group were more likely to attend on-line meetings. Additionally, participants whose primary mutual-help-group was 12-step meetings or Women for Sobriety were also more likely to attend online meetings in comparison to those who identified SMART or LifeRing as their primary group. Involvement in their primary group was lower among participants who attended online meetings.
Despite lower likelihood for abstinence at baseline, participants in online meetings may have comparable abstinence at 6, 12 months.
At baseline, participants who attended online meetings were less likely to be abstinent from alcohol. At 6 months, however, there was increased odds for online participants to be abstinent. At 12 months online meeting attendees had similar rates of abstinence compared to those who did not attend an online meeting (i.e., those only attending in-person or those who did not attend any meetings). However, this change in rates of abstinence over time may be an artifact of the statistical models used by the researchers. When they included the type of primary mutual-help group and attendance of multiple groups in their model, the association between online group attendance and lower abstinence rates remained, while the increased odds of abstinence at 6 and 12 months disappeared.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This secondary analysis of data from a 2015 study provides insights into what factors might predict online meeting attendance. Although not representative of current online meeting attendance, these insights can be combined with data from other studies to help guide both researchers examining the effectiveness of online mutual-help meetings and providers who want to support clients accessing recovery supports online.
Even before the COVID-19 pandemic, a majority of participants in the study had attended an online mutual-help meeting. While the number of online meeting attendees in this study probably reflected their recruitment of 12-step study participants (the majority of participants) from the website “In the Rooms,” the fact that the attendance was consistent across race, ethnicity, marital status, income, employment status, and education is notable and encouraging.
Given the persistent low numbers of people with substance use disorders that receive any type of treatment, online mutual-help meetings may help address existing barriers to care, for example employment, childcare, transportation, and the high cost of addiction treatment. At the same time, it is important to remember that 1 in 4 Americans do not have access to broadband internet and, even among those who do, not everyone has access to a safe or otherwise suitable environment where they can utilize online recovery supports. Consistent with other research on tele-healthand online supports, this study found that women and younger people were more likely to attend online meetings. Women, culturally, may have more domestic responsibilities (e.g., childcare, family meal preparation) that makes online participation particularly convenient and time-saving. This finding is also consistent with studies that show that men are less likely in general to seek support or mental health challenges than women and women approach health issues utilizing multiple sources. Men and older adults may benefit from targeted education about online recovery supports and, in the case of older adults, technical assistance.
Other important findings from this study include that people who attend online meetings are more likely to have drunk alcohol or consumed drugs recently, have more severe drinking problems, and have less confidence in meeting their drinking goals. The study authors interpret these findings to mean that online resources might be particularly attractive to people in early recovery, who are seeking out resources and trying different options to build connections. On this basis, providers might suggest online meetings as a low-threshold recovery support to individuals seeking recovery or early in their recovery process. At the same time, more recent or severe use does not necessarily indicate that a person is in early recovery. Other researchers have suggested the greater anonymity of online spaces may allow individuals pursuing harm reduction goals (moderate use; abstinence from one substance combined with moderate use of other) to participate in mutual-help meetings without worrying about judgement from people practicing more traditional, abstinence-only recovery, although many organizations such as SMART Recovery support non-abstinence goals in their meetings whether in person or online. Similarly, the greater anonymity offered by online meetings (not turning on one’s camera; attending meeting out of one’s geographical area) may also allow people returning to mutual-help group participation after a reoccurrence of use who are feeling guilt or shame. Further research is needed to see whether the association between online meeting attendance and recent/more severe drinking and substance use generalizes to other populations and what, if any, implications it has for recovery support and clinical care.
While attendees of online meetings were more likely to have drunk recently, the researcher’s analysis found that those attending online meetings have increased odds of abstinence at 6 months and equivalent odds of abstinence to other study participants at 12 months (although the increased likelihood of abstinence at 12 months was not large enough to be distinguishable from a chance effect). In other words, it appears that online meeting attendees may achieve similar rates of abstinence as other study participants not attending online meetings over time. However, this convergence disappeared when the model included primary mutual-help affiliation and the attendance of more than one type of group, with 12-step membership predicting higher odds of 6- and 12-month abstinence.
It is not entirely clear what this means. It may be an effect particular to the study’s sample. Participants from LifeRing and SMART were recruited from the general population of members with the aid of national organizations. Because of the historic culture of anonymity, participants from 12-step organization were recruited from an online meeting platform, In the Rooms. What may have happened is that 12-step affiliated participants were both more likely to attend meeting online (since they were recruited from the online resource,“In the Rooms”) and they had higher rates of abstinence in this study. It also should be remembered that not all study participants had abstinence as their stated recovery goal, therefore lower rates of abstinence among non-12-step group members that attend online meetings may not represent worse outcomes/. Rather, they may be in keeping with their initial goal.
Based on research into in-person mutual-help meetings, there are potential disadvantages to attending online meetings solely. Active involvement in meetings—for example, getting a sponsor, socializing with other people in recovery outside of meetings, or joining a home group—generally results in better substance related outcomes than meeting attendance alone. Developing these types of supportive connections may be more difficult online. The benefits of mutual-help meetings are in large part explained by peer-to-peer social interaction. In online group therapy, a possible parallel to online mutual-help meetings, group connection may be harder to develop. While more research is needed, it may be that individuals who have previous experience with in-person recovery groups and are more stably in remission are better able to adapt to the ways online groups support recovery goals. In turn, individuals who have only attended online meetings may benefit from groups that have professional facilitation and off-line components.
Finally, it is worth noting that online mutual-help groups (much like their in-person counterparts) will vary greatly in focus, format, culture, and demographic composition. No best practices exist for mutual-help groups that hold across different spaces; nor is there a mechanism or governance body to report negative experiences. When making referrals, clinicians should familiarize themselves with the different online options available and consider recommending meetings offered through the official sites of mutual-help organizations or those where facilitators and other safety monitors uphold community guidelines.
As the authors recognize, this study was unable to guarantee that its samples were representative of the large populations of the mutual-help groups in question. More research is needed to determine to what extent these finds generalize.
This study was conducted before the COVID-19 pandemic and the increased utilization of online mutual-help meetings caused by the shutdown of in-person meetings. Further research is needed to understand how this cultural shift may have affected who is attending online meetings and how they are utilizing them for recovery supports.
BOTTOM LINE
This secondary analysis of data from a 2015 study provides insights into what factors might predict online meeting attendance. The majority of study participants had attended an online mutual-help meeting, reflecting the fact that online meetings had become an increasingly popular form of recovery support before COVID-19. Echoing other research on tele-health and similar services, online meeting attendees in this study were more likely to be younger and female. Although it may not generalize to other populations, attendees in this study were also more likely to have drank or used substances recently, more likely to attend more than one type of mutual-help group (AA, LifeRing, SMART, etc.), and more likely to have problems of greater severity. It may be that individuals early in recovery find online mutual-help meetings to be a more accessible, “lower threshold” form of recovery support. However, further researcher is needed on online meeting attendance to understand what factors explain this association or if it generalizes to other populations.
For individuals and families seeking recovery: Online mutual-help meetings are now part of many people’s recovery programs. For many people in recovery, they have provided greater access to meetings and allowed them to work around challenges related to work schedule, childcare, transport, and disability access. While 12-step groups are the only available type of mutual-help meeting in much of the country, online meetings give people in or seeking help for their recovery access to multiple other options that may better fit their recovery preferences, philosophy, or goals, such as SMART, LifeRing, Women in Sobriety, All Recovery Meetings, and Harm Reduction Works. This may be especially true for atheists/agnostics who may not connect with the spiritual basis of 12-step philosophy and individuals pursuing moderation or Harm Reduction goals. At the same time, people in recovery should be aware that the effectiveness of mutual-help groups appears to be connected to active involvement (such as getting a sponsor, service, and socializing), developing recovery supportive social networks, and group accountability. It may be more difficult to develop these types of connections through online meeting attendance alone. While more research is needed,people in early recovery may benefit more from combining online meetings and active participation in in-person groups than from attending online meetings alone.
For treatment professionals and treatment systems: Online mutual-help meetings are becoming an increasingly popular option for recovery support, in no small part because their accessibility through the internet lets individuals work around obstacles to traditional treatment and recovery support services (employment, the lack of childcare, transport, and cost). Initial evidence indicates that women and younger people are more likely to utilize online recovery support. It may be that additional efforts are needed to inform men and older adults of these resources and support them in becoming familiar with their format. This study also raises the possibility that people early in recovery might find it easier to engage in online meetings before trying traditional meetings. At the same time, there are reasons to suspect that online meeting attendance alone may not have the same benefits as either traditional meetings or combining online and traditional meetings. The benefits of mutual-help meetings are in large part explained by peer-to-peer social interaction. Recovery supportive social networks may be harder to develop online. Finally, it is worth noting that, just like in person meetings, online mutual-help groups will vary in focus, format, culture, and demographic composition. When making referrals, treatment professionals should familiarize themselves with the different online options available and consider recommending meetings offered through the official sites of mutual-help organizations, such as the SMART website, or platforms like Unity Recovery, where facilitators uphold community guidelines.
For scientists:This article contributes to a small, but growing, body of research into online mutual aid meetings. Based on a secondary analysis of a 2015 study of mutual-help groups (AA, SMART, LifeRing, Women for Sobriety), the authors find that online attendance is more likely among women and younger people, people who attended more than one type of mutual held group, people who had consumed alcohol and other substances more recently, people with more sever alcohol problems, and people with less confidence of maintaining abstinence. Further research is needed to see whether these associations generalize to other populations, especially after the widespread shift to utilizing online mutual-help meetings during COVID-19. Especially notable is the finding that online meeting attendance in this sample is associated with more recent use, which may suggest that people in early recovery find online meetings more accessible than in-person meetings. More research is needed on who attends online meetings, their level of effectiveness overall as well as their effectiveness compared to in-person meetings specifically, how people combine online and in-person supports, the mechanisms through which they support change, and whether some platforms or points of access are more effective than others.
For policy makers: The beginning of COVID-19 witnessed the rapid and unplanned closure of in-person mutual help meetings. Although available before the pandemic, online mutual-help meetings provided people with an alternative source of support and allowed many to access peer-to-peer support for the first time. Although the data is currently limited,many people report finding online mutual aid meetings helpful and there appear to be few risks to accessing support in this format. This article suggests that people in early recovery may find online meetings more accessible and easier to access than more traditional, in-person meetings. At the same time, there are reasons to suspect that online meeting attendance alone may not have the same benefits as either attending traditional in-person meetings or combining online and traditional meetings. We currently have little data on who attends online meetings, their level of effectiveness compared to in-person meetings, and whether some platforms or points of access are more effective than others. Given the large number of people who are now utilizing these resources, this is a crucial research area to support. Finally, it is important to remember that 1 in 4 Americans do not have access to broadband internet and people in lower income strata, as well as Black and Latino individuals, are less likely to have broadband access. Encouraging increased reliance on online recovery supports, while failing to expand access to traditional in-person recovery supports, may ameliorate some issues of access while accentuating other disparities. Given this disparity in broadband access, the need for widespread broadband infrastructure has taken on outsized importance with the mainstreaming of online mutual-help meetings as well as more formal telehealth services.
Although online mutual-help groups have existed for some time, the closure of in-person meetings at the beginning of the COVID-19 pandemic has resulted in more people engaging with these groups. It is a longstanding reality that only a small minority of people with substance use disorders receive treatment. More easily accessible online mutual-help groups and other online recovery support services have the potential to address systemic barriers to treatment access, including lack of childcare, the need to continue working, transportation, and cost.
In parts of the country, the only available mutual-help meetings are 12-step recovery groups such as Alcoholics Anonymous. While research strongly supports the effectiveness of Alcoholics Anonymous (AA) for alcohol use disorder, with some evidence suggesting 12-step groups are effective for cocaine and methamphetamine use disorders, 12-steps groups may not be the best option for all individuals. Other mutual-help groups such as Self-Management and Recovery Training (SMART), Women for Sobriety, LifeRing Secular Recovery, Refuge Recovery, Celebrate Recovery, or Harm Reduction Works might be a better fit for these individuals philosophically or supportive of non-abstinence recovery goals, and are also all available online. As such, remote access through the internet allows people in recovery to access these resources when no in-person meetings exist in their area. Similarly, culturally informed addiction treatment or recovery support offered by professionals of color is another critical absence in large sections of the country. Online mutual-help groups for people of color (“affinity groups”) may help address this issue as well.
Researchers have suggested that online meetings support recovery in similar ways to in-person meetings. Anecdotal reports, not to mention the scale of their utilization, indicate that people find them helpful. There appears to be minimal risks for harmful interactions in online meeting participation. However, we currently have little data on who attends online meetings, their level of effectiveness compared to in-person meetings, how people combine online and in-person supports, and the mechanisms through which they support change. We also lack sufficient research on whether some platforms or points of accessing online meetings are more effective than others. This study examined the demographics, substance use and recovery characteristics, and primary mutual-help group affiliation of online recovery group attendees and the association of online meeting attendance with substance use outcomes.
HOW WAS THIS STUDY CONDUCTED?
Researchers reanalyzed data collected in 2015-16 for the Peer Alternative in Addiction study, which compared the effectiveness of mutual-help organizations such as AA, Women for Sobriety, LifeRing Secular Recovery, and Self-Management and Recovery Training (SMART). The original study, conducted before the COVID-19 pandemic, included 647 U.S. adults over the age of 18 with lifetime alcohol use disorder. Participants were recruited through working with the national leaderships of SMART and LifeRing and, for 12-step members, online through the website “In the Rooms.” (In the Rooms is a website where members, who can sign up for a free account, gain access to online meetings as well as features like blogs, chat rooms, and direct messaging with other members.) Study participants completed an initial survey (“baseline”) and then were followed up at 6 months (with 81% responding) and 12 months (with 86% percent responding). At baseline, 62 percent of survey respondents had attended at least one online mutual-help meeting in their lifetime and 36 percent had done so in the last 30 days.
The original study collected information on demographics, substance use and recovery, and the ways that participants engaged with mutual-help groups. For demographics, participants were asked about gender, race, ethnicity, marital status, education, employment, annual income, and whether they lived in urban, rural, or suburban areas. For substance use and recovery characteristics, participants were asked how recently they had used alcohol, how recently they had used other substances, and their alcohol recovery goal (total abstinence forever vs. drink after abstinence period/occasionally). For mutual-help group characteristics, participants were asked the number of meetings they had attended in the last 30 days, the types of groups they attended, their “primary group” (AA, LifeRing, SMART etc.), how involved they were with their primary group (including whether they had a home group/regular meeting, how regularly they attended their primary group, and their level of participation in group activities), their satisfaction with the primary group, and about primary group cohesion (for example, the extent to which the felt like they belonged or were valued).
In this new analysis, the study team looked at three questions. First, they used statistical tests to establish whether associations exist between demographics, substance use/recovery characteristics, or mutual-help utilization and online meeting attendance. Second, they created a model that allowed them to compare how well baseline characteristics such as recent alcohol and drug use, alcohol recovery goal, alcohol use severity, and alcohol abstinence self-efficacy predicted online mutual-help attendance. Third, they created a different model to test whether the association between online mutual-help attendance and abstinence was the same at baseline, 6 months, and 12 months, or whether this association changed at these different points in time.
WHAT DID THIS STUDY FIND?
Women, younger people, and people who used alcohol recently were more likely to attend online meetings.
The analysis found that meeting attendance was less likely among men than women. On the whole, participants who attended online meetings were younger than those who had not. Otherwise, demographics characteristics such as race, ethnicity, marital status, income, employment status, and education were not associated with increased likelihood of online meeting attendance. At baseline, participants who used alcohol in the past 30 days, and from 30 days to 1 year in the past, were more likely to attend online meetings than those who last drank over 1 year before. Regarding other substance use, participants who used other substances within the past 30 days to 1 year were more likely to attend online meetings than those whose last episode of use was over 5 years before. In addition, other substance use from 1 to 5 years ago was associated with greater odds of online meetings attendance than use over 5 years in the past.
Online attendance was associated with severity of alcohol problems and 12-step affiliation, but no association existed between online attendance and recovery goal.
In contrast to participants who did not attend online meetings, participants who attended online meetings had greater severity of alcohol use and alcohol problems and were less confident about their ability to resist drinking heavily. Current alcohol recovery goal—lifetime time absence versus some form or reduced or controlled drinking—was not associated with higher odds of online meeting attendance. Participants who attended more than one mutual-help group were more likely to attend on-line meetings. Additionally, participants whose primary mutual-help-group was 12-step meetings or Women for Sobriety were also more likely to attend online meetings in comparison to those who identified SMART or LifeRing as their primary group. Involvement in their primary group was lower among participants who attended online meetings.
Despite lower likelihood for abstinence at baseline, participants in online meetings may have comparable abstinence at 6, 12 months.
At baseline, participants who attended online meetings were less likely to be abstinent from alcohol. At 6 months, however, there was increased odds for online participants to be abstinent. At 12 months online meeting attendees had similar rates of abstinence compared to those who did not attend an online meeting (i.e., those only attending in-person or those who did not attend any meetings). However, this change in rates of abstinence over time may be an artifact of the statistical models used by the researchers. When they included the type of primary mutual-help group and attendance of multiple groups in their model, the association between online group attendance and lower abstinence rates remained, while the increased odds of abstinence at 6 and 12 months disappeared.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This secondary analysis of data from a 2015 study provides insights into what factors might predict online meeting attendance. Although not representative of current online meeting attendance, these insights can be combined with data from other studies to help guide both researchers examining the effectiveness of online mutual-help meetings and providers who want to support clients accessing recovery supports online.
Even before the COVID-19 pandemic, a majority of participants in the study had attended an online mutual-help meeting. While the number of online meeting attendees in this study probably reflected their recruitment of 12-step study participants (the majority of participants) from the website “In the Rooms,” the fact that the attendance was consistent across race, ethnicity, marital status, income, employment status, and education is notable and encouraging.
Given the persistent low numbers of people with substance use disorders that receive any type of treatment, online mutual-help meetings may help address existing barriers to care, for example employment, childcare, transportation, and the high cost of addiction treatment. At the same time, it is important to remember that 1 in 4 Americans do not have access to broadband internet and, even among those who do, not everyone has access to a safe or otherwise suitable environment where they can utilize online recovery supports. Consistent with other research on tele-healthand online supports, this study found that women and younger people were more likely to attend online meetings. Women, culturally, may have more domestic responsibilities (e.g., childcare, family meal preparation) that makes online participation particularly convenient and time-saving. This finding is also consistent with studies that show that men are less likely in general to seek support or mental health challenges than women and women approach health issues utilizing multiple sources. Men and older adults may benefit from targeted education about online recovery supports and, in the case of older adults, technical assistance.
Other important findings from this study include that people who attend online meetings are more likely to have drunk alcohol or consumed drugs recently, have more severe drinking problems, and have less confidence in meeting their drinking goals. The study authors interpret these findings to mean that online resources might be particularly attractive to people in early recovery, who are seeking out resources and trying different options to build connections. On this basis, providers might suggest online meetings as a low-threshold recovery support to individuals seeking recovery or early in their recovery process. At the same time, more recent or severe use does not necessarily indicate that a person is in early recovery. Other researchers have suggested the greater anonymity of online spaces may allow individuals pursuing harm reduction goals (moderate use; abstinence from one substance combined with moderate use of other) to participate in mutual-help meetings without worrying about judgement from people practicing more traditional, abstinence-only recovery, although many organizations such as SMART Recovery support non-abstinence goals in their meetings whether in person or online. Similarly, the greater anonymity offered by online meetings (not turning on one’s camera; attending meeting out of one’s geographical area) may also allow people returning to mutual-help group participation after a reoccurrence of use who are feeling guilt or shame. Further research is needed to see whether the association between online meeting attendance and recent/more severe drinking and substance use generalizes to other populations and what, if any, implications it has for recovery support and clinical care.
While attendees of online meetings were more likely to have drunk recently, the researcher’s analysis found that those attending online meetings have increased odds of abstinence at 6 months and equivalent odds of abstinence to other study participants at 12 months (although the increased likelihood of abstinence at 12 months was not large enough to be distinguishable from a chance effect). In other words, it appears that online meeting attendees may achieve similar rates of abstinence as other study participants not attending online meetings over time. However, this convergence disappeared when the model included primary mutual-help affiliation and the attendance of more than one type of group, with 12-step membership predicting higher odds of 6- and 12-month abstinence.
It is not entirely clear what this means. It may be an effect particular to the study’s sample. Participants from LifeRing and SMART were recruited from the general population of members with the aid of national organizations. Because of the historic culture of anonymity, participants from 12-step organization were recruited from an online meeting platform, In the Rooms. What may have happened is that 12-step affiliated participants were both more likely to attend meeting online (since they were recruited from the online resource,“In the Rooms”) and they had higher rates of abstinence in this study. It also should be remembered that not all study participants had abstinence as their stated recovery goal, therefore lower rates of abstinence among non-12-step group members that attend online meetings may not represent worse outcomes/. Rather, they may be in keeping with their initial goal.
Based on research into in-person mutual-help meetings, there are potential disadvantages to attending online meetings solely. Active involvement in meetings—for example, getting a sponsor, socializing with other people in recovery outside of meetings, or joining a home group—generally results in better substance related outcomes than meeting attendance alone. Developing these types of supportive connections may be more difficult online. The benefits of mutual-help meetings are in large part explained by peer-to-peer social interaction. In online group therapy, a possible parallel to online mutual-help meetings, group connection may be harder to develop. While more research is needed, it may be that individuals who have previous experience with in-person recovery groups and are more stably in remission are better able to adapt to the ways online groups support recovery goals. In turn, individuals who have only attended online meetings may benefit from groups that have professional facilitation and off-line components.
Finally, it is worth noting that online mutual-help groups (much like their in-person counterparts) will vary greatly in focus, format, culture, and demographic composition. No best practices exist for mutual-help groups that hold across different spaces; nor is there a mechanism or governance body to report negative experiences. When making referrals, clinicians should familiarize themselves with the different online options available and consider recommending meetings offered through the official sites of mutual-help organizations or those where facilitators and other safety monitors uphold community guidelines.
As the authors recognize, this study was unable to guarantee that its samples were representative of the large populations of the mutual-help groups in question. More research is needed to determine to what extent these finds generalize.
This study was conducted before the COVID-19 pandemic and the increased utilization of online mutual-help meetings caused by the shutdown of in-person meetings. Further research is needed to understand how this cultural shift may have affected who is attending online meetings and how they are utilizing them for recovery supports.
BOTTOM LINE
This secondary analysis of data from a 2015 study provides insights into what factors might predict online meeting attendance. The majority of study participants had attended an online mutual-help meeting, reflecting the fact that online meetings had become an increasingly popular form of recovery support before COVID-19. Echoing other research on tele-health and similar services, online meeting attendees in this study were more likely to be younger and female. Although it may not generalize to other populations, attendees in this study were also more likely to have drank or used substances recently, more likely to attend more than one type of mutual-help group (AA, LifeRing, SMART, etc.), and more likely to have problems of greater severity. It may be that individuals early in recovery find online mutual-help meetings to be a more accessible, “lower threshold” form of recovery support. However, further researcher is needed on online meeting attendance to understand what factors explain this association or if it generalizes to other populations.
For individuals and families seeking recovery: Online mutual-help meetings are now part of many people’s recovery programs. For many people in recovery, they have provided greater access to meetings and allowed them to work around challenges related to work schedule, childcare, transport, and disability access. While 12-step groups are the only available type of mutual-help meeting in much of the country, online meetings give people in or seeking help for their recovery access to multiple other options that may better fit their recovery preferences, philosophy, or goals, such as SMART, LifeRing, Women in Sobriety, All Recovery Meetings, and Harm Reduction Works. This may be especially true for atheists/agnostics who may not connect with the spiritual basis of 12-step philosophy and individuals pursuing moderation or Harm Reduction goals. At the same time, people in recovery should be aware that the effectiveness of mutual-help groups appears to be connected to active involvement (such as getting a sponsor, service, and socializing), developing recovery supportive social networks, and group accountability. It may be more difficult to develop these types of connections through online meeting attendance alone. While more research is needed,people in early recovery may benefit more from combining online meetings and active participation in in-person groups than from attending online meetings alone.
For treatment professionals and treatment systems: Online mutual-help meetings are becoming an increasingly popular option for recovery support, in no small part because their accessibility through the internet lets individuals work around obstacles to traditional treatment and recovery support services (employment, the lack of childcare, transport, and cost). Initial evidence indicates that women and younger people are more likely to utilize online recovery support. It may be that additional efforts are needed to inform men and older adults of these resources and support them in becoming familiar with their format. This study also raises the possibility that people early in recovery might find it easier to engage in online meetings before trying traditional meetings. At the same time, there are reasons to suspect that online meeting attendance alone may not have the same benefits as either traditional meetings or combining online and traditional meetings. The benefits of mutual-help meetings are in large part explained by peer-to-peer social interaction. Recovery supportive social networks may be harder to develop online. Finally, it is worth noting that, just like in person meetings, online mutual-help groups will vary in focus, format, culture, and demographic composition. When making referrals, treatment professionals should familiarize themselves with the different online options available and consider recommending meetings offered through the official sites of mutual-help organizations, such as the SMART website, or platforms like Unity Recovery, where facilitators uphold community guidelines.
For scientists:This article contributes to a small, but growing, body of research into online mutual aid meetings. Based on a secondary analysis of a 2015 study of mutual-help groups (AA, SMART, LifeRing, Women for Sobriety), the authors find that online attendance is more likely among women and younger people, people who attended more than one type of mutual held group, people who had consumed alcohol and other substances more recently, people with more sever alcohol problems, and people with less confidence of maintaining abstinence. Further research is needed to see whether these associations generalize to other populations, especially after the widespread shift to utilizing online mutual-help meetings during COVID-19. Especially notable is the finding that online meeting attendance in this sample is associated with more recent use, which may suggest that people in early recovery find online meetings more accessible than in-person meetings. More research is needed on who attends online meetings, their level of effectiveness overall as well as their effectiveness compared to in-person meetings specifically, how people combine online and in-person supports, the mechanisms through which they support change, and whether some platforms or points of access are more effective than others.
For policy makers: The beginning of COVID-19 witnessed the rapid and unplanned closure of in-person mutual help meetings. Although available before the pandemic, online mutual-help meetings provided people with an alternative source of support and allowed many to access peer-to-peer support for the first time. Although the data is currently limited,many people report finding online mutual aid meetings helpful and there appear to be few risks to accessing support in this format. This article suggests that people in early recovery may find online meetings more accessible and easier to access than more traditional, in-person meetings. At the same time, there are reasons to suspect that online meeting attendance alone may not have the same benefits as either attending traditional in-person meetings or combining online and traditional meetings. We currently have little data on who attends online meetings, their level of effectiveness compared to in-person meetings, and whether some platforms or points of access are more effective than others. Given the large number of people who are now utilizing these resources, this is a crucial research area to support. Finally, it is important to remember that 1 in 4 Americans do not have access to broadband internet and people in lower income strata, as well as Black and Latino individuals, are less likely to have broadband access. Encouraging increased reliance on online recovery supports, while failing to expand access to traditional in-person recovery supports, may ameliorate some issues of access while accentuating other disparities. Given this disparity in broadband access, the need for widespread broadband infrastructure has taken on outsized importance with the mainstreaming of online mutual-help meetings as well as more formal telehealth services.