Scaling up SMART Recovery online meetings during COVID-19
COVID-19 sparked a rapid change in how recovery services were provided. Mutual-help organizations were required to shift from in-person to almost exclusively online meetings. With support from the Australian government, SMART Recovery Australia dramatically increased online groups in ways that participants experienced as welcoming and beneficial.
Mutual-help organizations are a highly ubiquitous community recovery resource that leverage peer-to-peer connections to help individuals with substance use disorders and other addiction-related problems. Twelve-step mutual help organizations such as Alcoholics Anonymous and Narcotics Anonymous have been providing support to individuals for nearly a century, and secular and other or non-twelve step organizations such as SMART Recovery and LifeRing emerged in the 1990’s. Attendance at mutual-help organizations is the most common form of help-seeking among individuals with a current or past substance use problem, and there is a growing body of research supporting the use mutual-help organizations such as Alcoholics Anonymous and SMART Recovery.
The public health response (i.e., social distancing) during the COVID-19 pandemic limited in-person treatment and recovery support services for many. Although social distancing reduces the spread of communicable infections, the constrained access to substance use disorder and recovery services can have other negative side effects such increased isolation and notable declines in mental health for some, particularly those in addiction recovery. To help respond to the needs of individuals in or seeking recovery, mutual-help organizations transitioned during the pandemic from in-person to online formats.
This study focused on SMART Recovery, a program that incorporates principles from evidence-based cognitive behavioral therapy and motivational interviewing techniques to promote positive change among individuals experiencing substance use problems or behavioral addictions (e.g., gambling). Facilitators who have been trained in the SMART Recovery method lead the groups, and attendance is completely free (apart from voluntary contributions) as is the case with most other mutual-help organizations. SMART Recovery Australia received a federal grant from the Commonwealth Government of Australia to scale up online meetings during the COVID-19 pandemic. The scaling up of online offerings was designed to increase access to recovery support, and third-party delivery would likely increase the probability of sustaining online meetings after the funded grant period. The study evaluated SMART Recovery Australia’s success at scaling up online mutual-help in response to the COVID-19 pandemic as well as perceptions of participation among online meeting participants.
HOW WAS THIS STUDY CONDUCTED?
This study was an evaluation of SMART Recovery Australia’s scaling up of online meetings during the COVID-19 pandemic (July 1st, 2020 – August 31st, 2021), which was supported by a grant from the Australian government. The grant supported existing SMART groups’ move to an online format, training new SMART facilitators, outreach to third-party organizations (e.g., treatment centers), support setting up and navigating the online platform (Zoom), making calls following the first online group meeting, and creating new support materials such as a PowerPoint slideshow outlining the structure of online groups.
The program aimed to increase the number of online meetings from 6 to 100 and for 80% of groups to be delivered by third-party providers such as facilitators within private health and social care organizations. This study used participant questionnaires, administrative logs, and analytics from Zoom (the online meeting platform used) to investigate the 12-month scaling up effort and the 2 months after funding ended.
A link to the online participant questionnaire was presented at the end of every meeting, though participants could only respond to the survey once throughout the study period (even if they attended multiple meetings). The questionnaire was developed by the research team to capture how participants perceived SMART online meeting engagement, experience, and contribution to recovery as well as their basic demographic information. Participants were asked their level of agreement with a 5-point scale ranging from ‘Strongly Disagree’ to ‘Strongly Agree’ on questions related to their engagement, experience, and SMART’s contribution to their recovery. Administrative logs provided data on the number of trained facilitators and their affiliation (SMART Recovery Australia staff, SMART Recovery Australia volunteer, or third-party providers including staff from treatment programs) and the number of new meetings. Zoom analytics provided information on the number of meetings provided, number of meeting log-ins (totaled across meetings, not unique cases), average number of attendees per meeting, and average number of meetings delivered per month. A new group was considered established if they offered at least 2 meetings during the study period.
A total of 1052 individuals completed the questionnaire. About half identified as male (52%) or female (47%) with about 2% identifying as transgender male, transgender female, or non-binary/indeterminate. Almost all (90%) were between the ages of 25 and 64 with 6% aged 24 or younger and 4% aged 65 or older. A small number (<3%) identified as Aboriginal but not Torres Strait Islander or both Aboriginal and Torres Strait Islander, and about 71% lived in a major city. Alcohol use (72%) was most common behavior that prompted meeting attendance followed by tobacco use (13%), methamphetamine use (13%), cannabis use (13%), and other drug use (e.g., including opioids; 18%). About a third (35%) of participants listed other process-related behaviors such as food, gambling, and sex as the primary behavior that prompted group attendance. Over a third (39%) identified multiple behaviors as the reason for attending SMART Recovery.
WHAT DID THIS STUDY FIND?
The program substantially increased new online groups.
Pre-pandemic, SMART Recovery Australia had 6 online groups. During the 12 months of the program, 126 new online groups were established. This surpassed the program’s goal of 100. In any one month during the program, there was an average of 232 online meetings with an average of 3479 total (i.e., not unique) meeting attendees. At each meeting, there was an average of 14 attendees, and each group met 16 times on average. Among participants that completed questionnaires, 93% ‘Agreed’ or ‘Strongly Agreed’ that they felt welcome at the online meeting, and 91% ‘Agreed’ or ‘Strongly Agreed’ that they felt supported and understood by others attending the meeting. At the end of the program period, 76% of meetings were delivered by third-party providers. Also, 13.4% of the offered meetings were “identity” groups specifically for women, men, young people, family and friends, people of Aboriginal and/or Torres Strait Islander, and Korean language speakers. The number of active online groups and meetings was similar during the 2-month follow-up period compared to the initial 12 months, suggesting that efforts to scale up were maintained over this short follow-up.
Over half of participants felt online meetings were ‘better’ or ‘much better’ than in-person meetings.
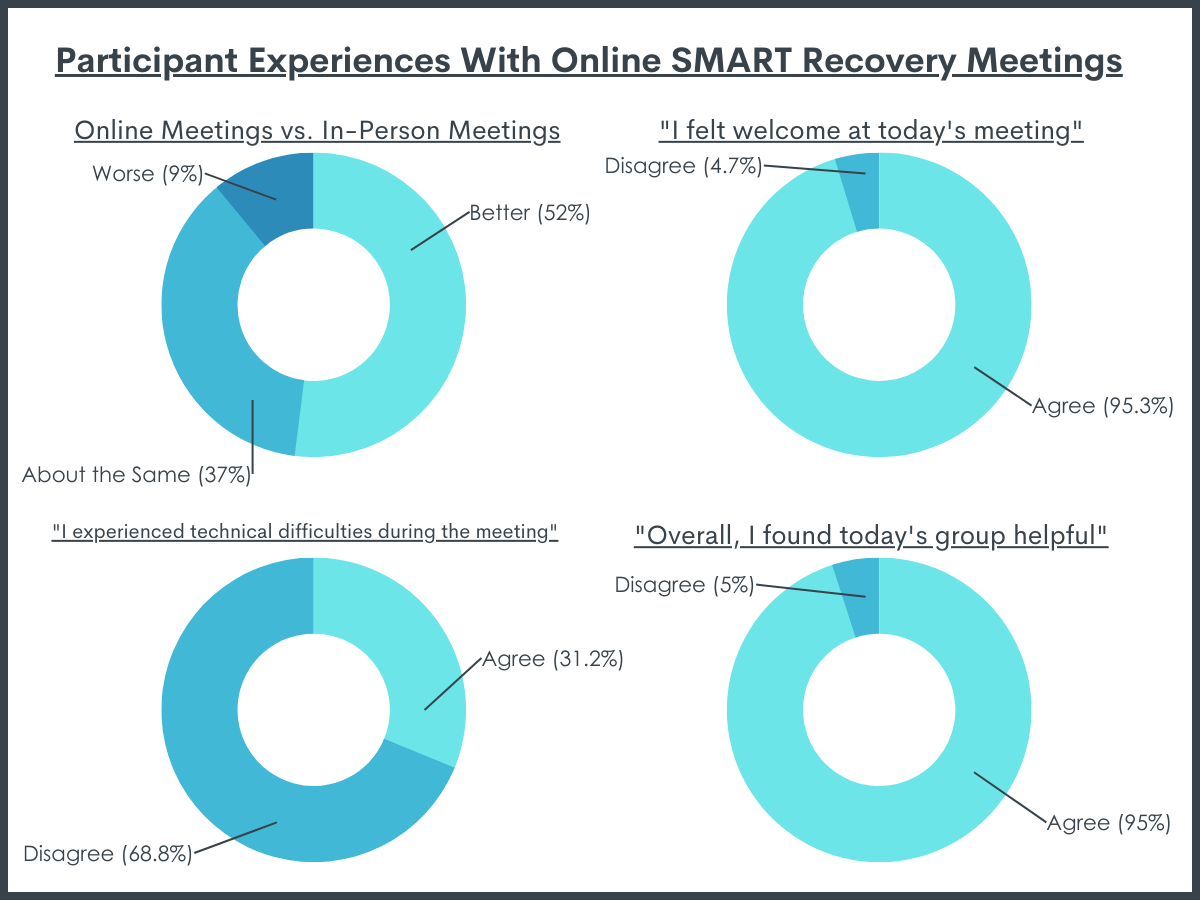
A subset of 345 participants had previously attended an in-person SMART Recovery meeting before the COVID-19 pandemic. Of those, 52% felt that the online meetings were ‘better’ (26%) or ‘much better’ (26%) than in-person meetings, and another 37% felt they were ‘about the same’. So, 89% of respondents that attended in-person meetings pre-pandemic thought the online meetings were about the same if not better than those in-person meetings. Among all 1052 survey respondents, 85% felt the online groups made a positive contribution to their recovery. Additionally, 90% listed the online groups as helpful, and 92% also shared they intended to continue SMART Recovery. Although 92% of participants felt the meetings were well facilitated, 21% of participants reported ‘agree’ or ‘strongly agree’ to having experienced technical difficulties.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study evaluated SMART Recovery Australia’s scaling up of online meetings during the COVID-19 pandemic. The program aimed to increase the number of online groups offered as well as the number of trained third-party SMART Recovery facilitators. The evaluation incorporated participant questionnaires, Zoom analytics, and administrative logs to assess perceived helpfulness of the online meetings, how many meetings were available and how many people attended, and how many trained facilitators were eligible to lead SMART groups.
This study found that 126 new online SMART Recovery groups were established and the participants who completed a survey, overall, felt the online meetings were welcoming, well-facilitated, and beneficial for their recovery. Among a subset of participants that had attended in-person meetings, over 80% perceived online meetings to be at least as helpful or even better than those in-person meetings. We do not know whether the actual elements of the Zoom experience are directly therapeutic or whether these ratings are confounded with factors related to the convivence of Zoom (e.g., lack of need to travel to meetings).
Australia responded to COVID-19 restrictions by making grants available to support recovery resources. SMART Recovery Australia subsequently received funding to support scaling up online groups. The perceived helpfulness of the online meetings and the expansive growth of online offerings suggest that Australia and SMART Recovery’s response may serve as a successful example of how to respond to public health crises that require social distancing and greater social isolation, such as COVID-19.
This study also suggests that for many experienced SMART members, online meetings may be as good or better than in-person meetings. If future research with more rigorous methods (e.g., randomized control trial that compares substance use and other recovery outcomes across the two modes of delivery) confirms these findings, then online meetings may be an effective alternative to in-person meetings. Results would also need to be replicated during a time when in-person meetings are offered at the same frequency as during non-COVID times. This study was conducted during a time when in-person options were not available. Yet, online meetings may increase access to recovery supports for individuals unable or uncomfortable attending in-person meetings. Research can help examine engagement with online supports going forward, now that in-person meetings are becoming more widely available. Future research and practice will also benefit from incorporating an equity lens. About one in four American adults do not have access to broadband internet at home. Those identifying as Black or Latinx and those with lower levels of education or income are less likely to have access.
In addition, 20% of the online meeting attendees who completed a survey experienced some technical difficulties with the online meeting. Although technology may increase access and availability of recovery supports, if individuals are unable to use the technology, then online meetings may not reach individuals in need and could even increase stress for those attempting to attend. There may be a need to develop brief trainings or “on-boarding” to build capacity for attendance and comfort with the online format.
The results from the participants questionnaires are subject to self-selection and social desirability bias. It is possible that individuals with less desirable experiences with online meetings did not stay until the end of the meeting when the link to the questionnaire was provided or did not elect to complete the questionnaire. Similarly, respondents that did complete the questionnaires may have been more motivated to engage with SMART and complete the questionnaire. Individuals who did complete the survey may also feel pressure to report positive experiences.
This study used a questionnaire that was developed by the research team and for which participants self-reported their experiences. The findings may be skewed positive due to the nature of the questions being asked. Also, since the study did not use standardized measures for the assessment of recovery or quality of life, the validity of the results is uncertain.
The number of unique meeting attendees was almost certainly less than the total number of log-ins during the study period. A smaller group of individuals may make up a disproportionately large share of meeting log-ins. A small group may have attended multiple meetings every week for the duration while others may only have attended one meeting. The number of unique individuals served by this effort to scale up SMART online meetings cannot be determined from the study data.
About 46% of participants that completed questionnaires had just attended their first SMART Recovery meeting. Thus, it is unknown if they continued attending online groups or working on their problem behaviors.
BOTTOM LINE
Overall, this study suggests that scaling up online SMART Recovery meetings in Australia during the COVID-19 pandemic was feasible, and attendees who completed a survey felt positively about their experience. Staff support enabled SMART facilitators to be trained virtually and start new online groups. There were 126 new online SMART Recovery groups, and there were 2,786 online meetings offered during the 12-month program period. Most participants who had attended in-person meetings prior to the pandemic felt that online meetings were about the same or better than in-person meetings. Results suggest that SMART Recovery Australia provided support perceived as valuable by its members and new attendees during the COVID-19 pandemic and there was clearly a demand for these meetings. SMART Recovery Australia responded to the COVID-19 pandemic in what appears to be a helpful way. However, more research is needed on whether SMART meeting attendance, both in-person and online, promotes improved substance use and other recovery outcomes.
For individuals and families seeking recovery: Online mutual-help groups may have mitigated some of the negative consequences of COVID-19 for individuals with substance use disorder or other process addictions in Australia. Although many of the public health measures taken during the pandemic are no longer in place, many mutual-help groups continue to host online meetings. Most mutual-help organizations maintain a national or local website that provides a database of in-person and online meetings. If you or a loved one are seeking recovery, attending online support meetings such as SMART Recovery may be a viable alternative to in-person meetings.
For treatment professionals and treatment systems: This evaluation study showed that SMART Recovery Australia was able to increase the number of online groups and trained facilitators during the COVID-19 pandemic. Moreover, most participants that previously attended in-person meetings and completed a survey found the online meetings to be about the same or better than in-person meetings. More research is needed to determine the impact of SMART Recovery, both in-person and online, on substance use and other recovery outcomes.
For scientists:The current study attempted to characterize meeting attendance and participant experiences in response to SMART Recovery Australia’s efforts to scale up online meetings during the COVID-19 pandemic. While the study found SMART Recovery Australia to have started 126 new online groups and the online groups were perceived to contribute to individuals’ recovery, future studies need to allow for a direct comparison between online and in-person meetings. These studies may feature a randomized control group design or an ex post-facto design with matching (e.g., pair-wise matching, propensity score matching). Investigation is also needed to elucidate differences between online and no meeting attendance. Additional methodological approaches will help to inform clinical and public health recommendations regarding online recovery support meetings. Furthermore, future studies should use validated measures of recovery outcomes (e.g., frequency and amount of substance use, quality of life, life satisfaction, recovery capital, etc.).
For policy makers: Given the potential of online meetings to increase access to mutual-help organizations, continuing to support policies that improve access to necessary infrastructure (e.g., high-speed internet) and the funding of digital recovery research is needed to test whether individuals with substance use disorders and other process addictions benefit from online meeting participation.
Mutual-help organizations are a highly ubiquitous community recovery resource that leverage peer-to-peer connections to help individuals with substance use disorders and other addiction-related problems. Twelve-step mutual help organizations such as Alcoholics Anonymous and Narcotics Anonymous have been providing support to individuals for nearly a century, and secular and other or non-twelve step organizations such as SMART Recovery and LifeRing emerged in the 1990’s. Attendance at mutual-help organizations is the most common form of help-seeking among individuals with a current or past substance use problem, and there is a growing body of research supporting the use mutual-help organizations such as Alcoholics Anonymous and SMART Recovery.
The public health response (i.e., social distancing) during the COVID-19 pandemic limited in-person treatment and recovery support services for many. Although social distancing reduces the spread of communicable infections, the constrained access to substance use disorder and recovery services can have other negative side effects such increased isolation and notable declines in mental health for some, particularly those in addiction recovery. To help respond to the needs of individuals in or seeking recovery, mutual-help organizations transitioned during the pandemic from in-person to online formats.
This study focused on SMART Recovery, a program that incorporates principles from evidence-based cognitive behavioral therapy and motivational interviewing techniques to promote positive change among individuals experiencing substance use problems or behavioral addictions (e.g., gambling). Facilitators who have been trained in the SMART Recovery method lead the groups, and attendance is completely free (apart from voluntary contributions) as is the case with most other mutual-help organizations. SMART Recovery Australia received a federal grant from the Commonwealth Government of Australia to scale up online meetings during the COVID-19 pandemic. The scaling up of online offerings was designed to increase access to recovery support, and third-party delivery would likely increase the probability of sustaining online meetings after the funded grant period. The study evaluated SMART Recovery Australia’s success at scaling up online mutual-help in response to the COVID-19 pandemic as well as perceptions of participation among online meeting participants.
HOW WAS THIS STUDY CONDUCTED?
This study was an evaluation of SMART Recovery Australia’s scaling up of online meetings during the COVID-19 pandemic (July 1st, 2020 – August 31st, 2021), which was supported by a grant from the Australian government. The grant supported existing SMART groups’ move to an online format, training new SMART facilitators, outreach to third-party organizations (e.g., treatment centers), support setting up and navigating the online platform (Zoom), making calls following the first online group meeting, and creating new support materials such as a PowerPoint slideshow outlining the structure of online groups.
The program aimed to increase the number of online meetings from 6 to 100 and for 80% of groups to be delivered by third-party providers such as facilitators within private health and social care organizations. This study used participant questionnaires, administrative logs, and analytics from Zoom (the online meeting platform used) to investigate the 12-month scaling up effort and the 2 months after funding ended.
A link to the online participant questionnaire was presented at the end of every meeting, though participants could only respond to the survey once throughout the study period (even if they attended multiple meetings). The questionnaire was developed by the research team to capture how participants perceived SMART online meeting engagement, experience, and contribution to recovery as well as their basic demographic information. Participants were asked their level of agreement with a 5-point scale ranging from ‘Strongly Disagree’ to ‘Strongly Agree’ on questions related to their engagement, experience, and SMART’s contribution to their recovery. Administrative logs provided data on the number of trained facilitators and their affiliation (SMART Recovery Australia staff, SMART Recovery Australia volunteer, or third-party providers including staff from treatment programs) and the number of new meetings. Zoom analytics provided information on the number of meetings provided, number of meeting log-ins (totaled across meetings, not unique cases), average number of attendees per meeting, and average number of meetings delivered per month. A new group was considered established if they offered at least 2 meetings during the study period.
A total of 1052 individuals completed the questionnaire. About half identified as male (52%) or female (47%) with about 2% identifying as transgender male, transgender female, or non-binary/indeterminate. Almost all (90%) were between the ages of 25 and 64 with 6% aged 24 or younger and 4% aged 65 or older. A small number (<3%) identified as Aboriginal but not Torres Strait Islander or both Aboriginal and Torres Strait Islander, and about 71% lived in a major city. Alcohol use (72%) was most common behavior that prompted meeting attendance followed by tobacco use (13%), methamphetamine use (13%), cannabis use (13%), and other drug use (e.g., including opioids; 18%). About a third (35%) of participants listed other process-related behaviors such as food, gambling, and sex as the primary behavior that prompted group attendance. Over a third (39%) identified multiple behaviors as the reason for attending SMART Recovery.
WHAT DID THIS STUDY FIND?
The program substantially increased new online groups.
Pre-pandemic, SMART Recovery Australia had 6 online groups. During the 12 months of the program, 126 new online groups were established. This surpassed the program’s goal of 100. In any one month during the program, there was an average of 232 online meetings with an average of 3479 total (i.e., not unique) meeting attendees. At each meeting, there was an average of 14 attendees, and each group met 16 times on average. Among participants that completed questionnaires, 93% ‘Agreed’ or ‘Strongly Agreed’ that they felt welcome at the online meeting, and 91% ‘Agreed’ or ‘Strongly Agreed’ that they felt supported and understood by others attending the meeting. At the end of the program period, 76% of meetings were delivered by third-party providers. Also, 13.4% of the offered meetings were “identity” groups specifically for women, men, young people, family and friends, people of Aboriginal and/or Torres Strait Islander, and Korean language speakers. The number of active online groups and meetings was similar during the 2-month follow-up period compared to the initial 12 months, suggesting that efforts to scale up were maintained over this short follow-up.
Over half of participants felt online meetings were ‘better’ or ‘much better’ than in-person meetings.
A subset of 345 participants had previously attended an in-person SMART Recovery meeting before the COVID-19 pandemic. Of those, 52% felt that the online meetings were ‘better’ (26%) or ‘much better’ (26%) than in-person meetings, and another 37% felt they were ‘about the same’. So, 89% of respondents that attended in-person meetings pre-pandemic thought the online meetings were about the same if not better than those in-person meetings. Among all 1052 survey respondents, 85% felt the online groups made a positive contribution to their recovery. Additionally, 90% listed the online groups as helpful, and 92% also shared they intended to continue SMART Recovery. Although 92% of participants felt the meetings were well facilitated, 21% of participants reported ‘agree’ or ‘strongly agree’ to having experienced technical difficulties.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study evaluated SMART Recovery Australia’s scaling up of online meetings during the COVID-19 pandemic. The program aimed to increase the number of online groups offered as well as the number of trained third-party SMART Recovery facilitators. The evaluation incorporated participant questionnaires, Zoom analytics, and administrative logs to assess perceived helpfulness of the online meetings, how many meetings were available and how many people attended, and how many trained facilitators were eligible to lead SMART groups.
This study found that 126 new online SMART Recovery groups were established and the participants who completed a survey, overall, felt the online meetings were welcoming, well-facilitated, and beneficial for their recovery. Among a subset of participants that had attended in-person meetings, over 80% perceived online meetings to be at least as helpful or even better than those in-person meetings. We do not know whether the actual elements of the Zoom experience are directly therapeutic or whether these ratings are confounded with factors related to the convivence of Zoom (e.g., lack of need to travel to meetings).
Australia responded to COVID-19 restrictions by making grants available to support recovery resources. SMART Recovery Australia subsequently received funding to support scaling up online groups. The perceived helpfulness of the online meetings and the expansive growth of online offerings suggest that Australia and SMART Recovery’s response may serve as a successful example of how to respond to public health crises that require social distancing and greater social isolation, such as COVID-19.
This study also suggests that for many experienced SMART members, online meetings may be as good or better than in-person meetings. If future research with more rigorous methods (e.g., randomized control trial that compares substance use and other recovery outcomes across the two modes of delivery) confirms these findings, then online meetings may be an effective alternative to in-person meetings. Results would also need to be replicated during a time when in-person meetings are offered at the same frequency as during non-COVID times. This study was conducted during a time when in-person options were not available. Yet, online meetings may increase access to recovery supports for individuals unable or uncomfortable attending in-person meetings. Research can help examine engagement with online supports going forward, now that in-person meetings are becoming more widely available. Future research and practice will also benefit from incorporating an equity lens. About one in four American adults do not have access to broadband internet at home. Those identifying as Black or Latinx and those with lower levels of education or income are less likely to have access.
In addition, 20% of the online meeting attendees who completed a survey experienced some technical difficulties with the online meeting. Although technology may increase access and availability of recovery supports, if individuals are unable to use the technology, then online meetings may not reach individuals in need and could even increase stress for those attempting to attend. There may be a need to develop brief trainings or “on-boarding” to build capacity for attendance and comfort with the online format.
The results from the participants questionnaires are subject to self-selection and social desirability bias. It is possible that individuals with less desirable experiences with online meetings did not stay until the end of the meeting when the link to the questionnaire was provided or did not elect to complete the questionnaire. Similarly, respondents that did complete the questionnaires may have been more motivated to engage with SMART and complete the questionnaire. Individuals who did complete the survey may also feel pressure to report positive experiences.
This study used a questionnaire that was developed by the research team and for which participants self-reported their experiences. The findings may be skewed positive due to the nature of the questions being asked. Also, since the study did not use standardized measures for the assessment of recovery or quality of life, the validity of the results is uncertain.
The number of unique meeting attendees was almost certainly less than the total number of log-ins during the study period. A smaller group of individuals may make up a disproportionately large share of meeting log-ins. A small group may have attended multiple meetings every week for the duration while others may only have attended one meeting. The number of unique individuals served by this effort to scale up SMART online meetings cannot be determined from the study data.
About 46% of participants that completed questionnaires had just attended their first SMART Recovery meeting. Thus, it is unknown if they continued attending online groups or working on their problem behaviors.
BOTTOM LINE
Overall, this study suggests that scaling up online SMART Recovery meetings in Australia during the COVID-19 pandemic was feasible, and attendees who completed a survey felt positively about their experience. Staff support enabled SMART facilitators to be trained virtually and start new online groups. There were 126 new online SMART Recovery groups, and there were 2,786 online meetings offered during the 12-month program period. Most participants who had attended in-person meetings prior to the pandemic felt that online meetings were about the same or better than in-person meetings. Results suggest that SMART Recovery Australia provided support perceived as valuable by its members and new attendees during the COVID-19 pandemic and there was clearly a demand for these meetings. SMART Recovery Australia responded to the COVID-19 pandemic in what appears to be a helpful way. However, more research is needed on whether SMART meeting attendance, both in-person and online, promotes improved substance use and other recovery outcomes.
For individuals and families seeking recovery: Online mutual-help groups may have mitigated some of the negative consequences of COVID-19 for individuals with substance use disorder or other process addictions in Australia. Although many of the public health measures taken during the pandemic are no longer in place, many mutual-help groups continue to host online meetings. Most mutual-help organizations maintain a national or local website that provides a database of in-person and online meetings. If you or a loved one are seeking recovery, attending online support meetings such as SMART Recovery may be a viable alternative to in-person meetings.
For treatment professionals and treatment systems: This evaluation study showed that SMART Recovery Australia was able to increase the number of online groups and trained facilitators during the COVID-19 pandemic. Moreover, most participants that previously attended in-person meetings and completed a survey found the online meetings to be about the same or better than in-person meetings. More research is needed to determine the impact of SMART Recovery, both in-person and online, on substance use and other recovery outcomes.
For scientists:The current study attempted to characterize meeting attendance and participant experiences in response to SMART Recovery Australia’s efforts to scale up online meetings during the COVID-19 pandemic. While the study found SMART Recovery Australia to have started 126 new online groups and the online groups were perceived to contribute to individuals’ recovery, future studies need to allow for a direct comparison between online and in-person meetings. These studies may feature a randomized control group design or an ex post-facto design with matching (e.g., pair-wise matching, propensity score matching). Investigation is also needed to elucidate differences between online and no meeting attendance. Additional methodological approaches will help to inform clinical and public health recommendations regarding online recovery support meetings. Furthermore, future studies should use validated measures of recovery outcomes (e.g., frequency and amount of substance use, quality of life, life satisfaction, recovery capital, etc.).
For policy makers: Given the potential of online meetings to increase access to mutual-help organizations, continuing to support policies that improve access to necessary infrastructure (e.g., high-speed internet) and the funding of digital recovery research is needed to test whether individuals with substance use disorders and other process addictions benefit from online meeting participation.
Mutual-help organizations are a highly ubiquitous community recovery resource that leverage peer-to-peer connections to help individuals with substance use disorders and other addiction-related problems. Twelve-step mutual help organizations such as Alcoholics Anonymous and Narcotics Anonymous have been providing support to individuals for nearly a century, and secular and other or non-twelve step organizations such as SMART Recovery and LifeRing emerged in the 1990’s. Attendance at mutual-help organizations is the most common form of help-seeking among individuals with a current or past substance use problem, and there is a growing body of research supporting the use mutual-help organizations such as Alcoholics Anonymous and SMART Recovery.
The public health response (i.e., social distancing) during the COVID-19 pandemic limited in-person treatment and recovery support services for many. Although social distancing reduces the spread of communicable infections, the constrained access to substance use disorder and recovery services can have other negative side effects such increased isolation and notable declines in mental health for some, particularly those in addiction recovery. To help respond to the needs of individuals in or seeking recovery, mutual-help organizations transitioned during the pandemic from in-person to online formats.
This study focused on SMART Recovery, a program that incorporates principles from evidence-based cognitive behavioral therapy and motivational interviewing techniques to promote positive change among individuals experiencing substance use problems or behavioral addictions (e.g., gambling). Facilitators who have been trained in the SMART Recovery method lead the groups, and attendance is completely free (apart from voluntary contributions) as is the case with most other mutual-help organizations. SMART Recovery Australia received a federal grant from the Commonwealth Government of Australia to scale up online meetings during the COVID-19 pandemic. The scaling up of online offerings was designed to increase access to recovery support, and third-party delivery would likely increase the probability of sustaining online meetings after the funded grant period. The study evaluated SMART Recovery Australia’s success at scaling up online mutual-help in response to the COVID-19 pandemic as well as perceptions of participation among online meeting participants.
HOW WAS THIS STUDY CONDUCTED?
This study was an evaluation of SMART Recovery Australia’s scaling up of online meetings during the COVID-19 pandemic (July 1st, 2020 – August 31st, 2021), which was supported by a grant from the Australian government. The grant supported existing SMART groups’ move to an online format, training new SMART facilitators, outreach to third-party organizations (e.g., treatment centers), support setting up and navigating the online platform (Zoom), making calls following the first online group meeting, and creating new support materials such as a PowerPoint slideshow outlining the structure of online groups.
The program aimed to increase the number of online meetings from 6 to 100 and for 80% of groups to be delivered by third-party providers such as facilitators within private health and social care organizations. This study used participant questionnaires, administrative logs, and analytics from Zoom (the online meeting platform used) to investigate the 12-month scaling up effort and the 2 months after funding ended.
A link to the online participant questionnaire was presented at the end of every meeting, though participants could only respond to the survey once throughout the study period (even if they attended multiple meetings). The questionnaire was developed by the research team to capture how participants perceived SMART online meeting engagement, experience, and contribution to recovery as well as their basic demographic information. Participants were asked their level of agreement with a 5-point scale ranging from ‘Strongly Disagree’ to ‘Strongly Agree’ on questions related to their engagement, experience, and SMART’s contribution to their recovery. Administrative logs provided data on the number of trained facilitators and their affiliation (SMART Recovery Australia staff, SMART Recovery Australia volunteer, or third-party providers including staff from treatment programs) and the number of new meetings. Zoom analytics provided information on the number of meetings provided, number of meeting log-ins (totaled across meetings, not unique cases), average number of attendees per meeting, and average number of meetings delivered per month. A new group was considered established if they offered at least 2 meetings during the study period.
A total of 1052 individuals completed the questionnaire. About half identified as male (52%) or female (47%) with about 2% identifying as transgender male, transgender female, or non-binary/indeterminate. Almost all (90%) were between the ages of 25 and 64 with 6% aged 24 or younger and 4% aged 65 or older. A small number (<3%) identified as Aboriginal but not Torres Strait Islander or both Aboriginal and Torres Strait Islander, and about 71% lived in a major city. Alcohol use (72%) was most common behavior that prompted meeting attendance followed by tobacco use (13%), methamphetamine use (13%), cannabis use (13%), and other drug use (e.g., including opioids; 18%). About a third (35%) of participants listed other process-related behaviors such as food, gambling, and sex as the primary behavior that prompted group attendance. Over a third (39%) identified multiple behaviors as the reason for attending SMART Recovery.
WHAT DID THIS STUDY FIND?
The program substantially increased new online groups.
Pre-pandemic, SMART Recovery Australia had 6 online groups. During the 12 months of the program, 126 new online groups were established. This surpassed the program’s goal of 100. In any one month during the program, there was an average of 232 online meetings with an average of 3479 total (i.e., not unique) meeting attendees. At each meeting, there was an average of 14 attendees, and each group met 16 times on average. Among participants that completed questionnaires, 93% ‘Agreed’ or ‘Strongly Agreed’ that they felt welcome at the online meeting, and 91% ‘Agreed’ or ‘Strongly Agreed’ that they felt supported and understood by others attending the meeting. At the end of the program period, 76% of meetings were delivered by third-party providers. Also, 13.4% of the offered meetings were “identity” groups specifically for women, men, young people, family and friends, people of Aboriginal and/or Torres Strait Islander, and Korean language speakers. The number of active online groups and meetings was similar during the 2-month follow-up period compared to the initial 12 months, suggesting that efforts to scale up were maintained over this short follow-up.
Over half of participants felt online meetings were ‘better’ or ‘much better’ than in-person meetings.
A subset of 345 participants had previously attended an in-person SMART Recovery meeting before the COVID-19 pandemic. Of those, 52% felt that the online meetings were ‘better’ (26%) or ‘much better’ (26%) than in-person meetings, and another 37% felt they were ‘about the same’. So, 89% of respondents that attended in-person meetings pre-pandemic thought the online meetings were about the same if not better than those in-person meetings. Among all 1052 survey respondents, 85% felt the online groups made a positive contribution to their recovery. Additionally, 90% listed the online groups as helpful, and 92% also shared they intended to continue SMART Recovery. Although 92% of participants felt the meetings were well facilitated, 21% of participants reported ‘agree’ or ‘strongly agree’ to having experienced technical difficulties.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study evaluated SMART Recovery Australia’s scaling up of online meetings during the COVID-19 pandemic. The program aimed to increase the number of online groups offered as well as the number of trained third-party SMART Recovery facilitators. The evaluation incorporated participant questionnaires, Zoom analytics, and administrative logs to assess perceived helpfulness of the online meetings, how many meetings were available and how many people attended, and how many trained facilitators were eligible to lead SMART groups.
This study found that 126 new online SMART Recovery groups were established and the participants who completed a survey, overall, felt the online meetings were welcoming, well-facilitated, and beneficial for their recovery. Among a subset of participants that had attended in-person meetings, over 80% perceived online meetings to be at least as helpful or even better than those in-person meetings. We do not know whether the actual elements of the Zoom experience are directly therapeutic or whether these ratings are confounded with factors related to the convivence of Zoom (e.g., lack of need to travel to meetings).
Australia responded to COVID-19 restrictions by making grants available to support recovery resources. SMART Recovery Australia subsequently received funding to support scaling up online groups. The perceived helpfulness of the online meetings and the expansive growth of online offerings suggest that Australia and SMART Recovery’s response may serve as a successful example of how to respond to public health crises that require social distancing and greater social isolation, such as COVID-19.
This study also suggests that for many experienced SMART members, online meetings may be as good or better than in-person meetings. If future research with more rigorous methods (e.g., randomized control trial that compares substance use and other recovery outcomes across the two modes of delivery) confirms these findings, then online meetings may be an effective alternative to in-person meetings. Results would also need to be replicated during a time when in-person meetings are offered at the same frequency as during non-COVID times. This study was conducted during a time when in-person options were not available. Yet, online meetings may increase access to recovery supports for individuals unable or uncomfortable attending in-person meetings. Research can help examine engagement with online supports going forward, now that in-person meetings are becoming more widely available. Future research and practice will also benefit from incorporating an equity lens. About one in four American adults do not have access to broadband internet at home. Those identifying as Black or Latinx and those with lower levels of education or income are less likely to have access.
In addition, 20% of the online meeting attendees who completed a survey experienced some technical difficulties with the online meeting. Although technology may increase access and availability of recovery supports, if individuals are unable to use the technology, then online meetings may not reach individuals in need and could even increase stress for those attempting to attend. There may be a need to develop brief trainings or “on-boarding” to build capacity for attendance and comfort with the online format.
The results from the participants questionnaires are subject to self-selection and social desirability bias. It is possible that individuals with less desirable experiences with online meetings did not stay until the end of the meeting when the link to the questionnaire was provided or did not elect to complete the questionnaire. Similarly, respondents that did complete the questionnaires may have been more motivated to engage with SMART and complete the questionnaire. Individuals who did complete the survey may also feel pressure to report positive experiences.
This study used a questionnaire that was developed by the research team and for which participants self-reported their experiences. The findings may be skewed positive due to the nature of the questions being asked. Also, since the study did not use standardized measures for the assessment of recovery or quality of life, the validity of the results is uncertain.
The number of unique meeting attendees was almost certainly less than the total number of log-ins during the study period. A smaller group of individuals may make up a disproportionately large share of meeting log-ins. A small group may have attended multiple meetings every week for the duration while others may only have attended one meeting. The number of unique individuals served by this effort to scale up SMART online meetings cannot be determined from the study data.
About 46% of participants that completed questionnaires had just attended their first SMART Recovery meeting. Thus, it is unknown if they continued attending online groups or working on their problem behaviors.
BOTTOM LINE
Overall, this study suggests that scaling up online SMART Recovery meetings in Australia during the COVID-19 pandemic was feasible, and attendees who completed a survey felt positively about their experience. Staff support enabled SMART facilitators to be trained virtually and start new online groups. There were 126 new online SMART Recovery groups, and there were 2,786 online meetings offered during the 12-month program period. Most participants who had attended in-person meetings prior to the pandemic felt that online meetings were about the same or better than in-person meetings. Results suggest that SMART Recovery Australia provided support perceived as valuable by its members and new attendees during the COVID-19 pandemic and there was clearly a demand for these meetings. SMART Recovery Australia responded to the COVID-19 pandemic in what appears to be a helpful way. However, more research is needed on whether SMART meeting attendance, both in-person and online, promotes improved substance use and other recovery outcomes.
For individuals and families seeking recovery: Online mutual-help groups may have mitigated some of the negative consequences of COVID-19 for individuals with substance use disorder or other process addictions in Australia. Although many of the public health measures taken during the pandemic are no longer in place, many mutual-help groups continue to host online meetings. Most mutual-help organizations maintain a national or local website that provides a database of in-person and online meetings. If you or a loved one are seeking recovery, attending online support meetings such as SMART Recovery may be a viable alternative to in-person meetings.
For treatment professionals and treatment systems: This evaluation study showed that SMART Recovery Australia was able to increase the number of online groups and trained facilitators during the COVID-19 pandemic. Moreover, most participants that previously attended in-person meetings and completed a survey found the online meetings to be about the same or better than in-person meetings. More research is needed to determine the impact of SMART Recovery, both in-person and online, on substance use and other recovery outcomes.
For scientists:The current study attempted to characterize meeting attendance and participant experiences in response to SMART Recovery Australia’s efforts to scale up online meetings during the COVID-19 pandemic. While the study found SMART Recovery Australia to have started 126 new online groups and the online groups were perceived to contribute to individuals’ recovery, future studies need to allow for a direct comparison between online and in-person meetings. These studies may feature a randomized control group design or an ex post-facto design with matching (e.g., pair-wise matching, propensity score matching). Investigation is also needed to elucidate differences between online and no meeting attendance. Additional methodological approaches will help to inform clinical and public health recommendations regarding online recovery support meetings. Furthermore, future studies should use validated measures of recovery outcomes (e.g., frequency and amount of substance use, quality of life, life satisfaction, recovery capital, etc.).
For policy makers: Given the potential of online meetings to increase access to mutual-help organizations, continuing to support policies that improve access to necessary infrastructure (e.g., high-speed internet) and the funding of digital recovery research is needed to test whether individuals with substance use disorders and other process addictions benefit from online meeting participation.