
How well does online CBT stack up with CBT delivered in-person?
The COVID-19 pandemic has highlighted ongoing barriers to alcohol use disorder treatment engagement, leading to widespread adoption of internet-delivered treatments and digital recovery support services. Interventions leveraging these digital technologies have emerged as one strategy for expanding alcohol use disorder treatment access to those who may otherwise not receive it. One important question, therefore, is how a treatment does when delivered online versus in-person. In this study individuals were randomly assigned to either internet-delivered cognitive behavioral therapy (online CBT) or face-to-face cognitive behavioral therapy (in-person CBT) for alcohol use disorder. The online CBT participants were tested specifically to see if they had comparable outcomes (i.e., did not have inferior outcomes to in-person participants; a “non-inferiority” trial) with some intriguing results found.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Harmful alcohol use is among the leading causes of premature death worldwide and accounts for approximately 5% of the world’s disease burden as measured by disability-adjusted life years (i.e., the number of years lost due to disability, illness, or premature death). Alcohol policy interventions aimed at reducing alcohol-related harms throughout the world include limiting alcohol availability, restricting alcohol advertising, increasing taxes on alcohol, and of course, identifying gaps in, and expanding access to, alcohol use disorder treatment. Yet, researchers estimate that, worldwide, only 7.1% of individuals with substance use disorder (including alcohol use disorder) and a recognized treatment need received even minimally adequate treatment. Many efforts to reduce disease burden and death attributed to alcohol use disorder have therefore been focused on increasing access to treatment.
One-way providers have worked to expand treatment access to individuals with alcohol use disorder is through the use of digital technologies. With telemedicine, for example, treatment reach is improved because individuals can use online communication tools such as video conferencing and/or text chat to engage in treatment. Individuals may also engage in treatment without directly interacting with a clinician, where engagement is self-directed and the treatment modules are automated.
Another approach may be a hybrid of these two, such that patients can engage on their own with treatment modules while a clinician helps support their engagement using online communication tools. Although research has shown that some internet-delivered treatments can help patients reduce their alcohol use, questions remain about how internet-delivered treatments compare to interventions that are delivered in-person. The current study addresses this research gap by examining whether cognitive behavioral therapy delivered by a provider over the internet (iCBT) is non-inferior to (i.e., is as effective as) CBT that is delivered in person (face-to-face CBT) for treating alcohol use disorder in adults.
HOW WAS THIS STUDY CONDUCTED?
This study was a randomized controlled non-inferiority trial with 301 participants who were assigned to receive either internet-delivered CBT (iCBT; n = 150) or face-to-face CBT (n = 151). Both iCBT and face-to-face CBT participants received CBT treatment from a study therapist. Participants were followed up 3- and 6-months after being randomized in order to assess various alcohol-related outcomes. Participants were 301 Swedish adults who had an alcohol use disorder as determined by the International Classification of Disease (ICD-10) and the Alcohol Use Disorders Identification Test (AUDIT). Non-inferiority trials are a way to compare new treatments to existing treatments that are known to be effective in order to determine if the new treatment is as good as the existing one.
Participants in both treatment groups completed five modules of CBT over a 3-month period. The CBT intervention was consistent with other empirically-supported CBT approaches for substance use disorder. The intervention incorporated self-help materials used in prior internet-based treatment, and incorporated exercises and content based on relapse prevention, motivational interviewing, and behavioral self-control.
The CBT program was divided into five primary units: 1) motivation, 2) drinking goal and self-control, 3) behavioral analysis of drinking and risk situations, 4) general problem solving, and 5) preventing relapse.
Study therapists used the same program and materials in both conditions, with the difference being that the treatment and materials in the iCBT condition were delivered online, including all communication between the therapist and patient. For the in-person condition, the treatment and materials were delivered entirely in-person with paper (i.e., hard copy) content. The same 8 study therapists provided treatment to both iCBT and face-to-face participants.
The primary outcome in this study was the difference in alcohol consumption between treatment groups as measured by the total number of standard drinks consumed in the previous week at the 6-month follow up. Past week alcohol consumption was self-reported using the Timeline Followback and used the Swedish definition of one standard drink which contains 12 grams of pure alcohol per drink (the United States’ “standard drink” has 14g of pure alcohol and thus the Swedish “drink” has slightly less alcohol). This outcome was also assessed at the 3-month follow-up, which was also the end of treatment.
Secondary outcomes (measured at both the 3- and 6-month follow-ups) included the number of non-drinking days, number of binge-drinking days (defined as days with 4+ drinks/day for men and 3+/day for women), problematic alcohol use as determined by the AUDIT, health-related quality of life, and other measures of psychological wellbeing including depression and general anxiety disorder. The research team also measured the strength and effect of the therapeutic relationship between the participant and provider via the Working Alliance Inventory and Session Rating Scale.
The researchers in this study used an intent-to-treat approach, meaning that all participants who were randomized were included in the analyses, even if they did not receive the allocated intervention.
Importantly, this study was also a non-inferiority trial. To determine whether online CBT with a therapist was comparable (i.e., non-inferior/as good as) to the well-established in-person CBT, they used prior research and accepted methods to identify the non-inferiority “thresholds” in this study. That is, they conducted a series of steps to identify how close therapist-facilitated online CBT outcomes needed to be relative to in-person CBT in order to be considered “non-inferior”. The results below are described within this non-inferiority framework.
Regarding participant demographic characteristics, over half (62%) were male and the majority of participants were either married or cohabitating (70.7% iCBT, 66.9% face-to-face), college educated (66.7% iCBT, 68.9% face-to-face), and employed (82.7% iCBT, 82.1% face-to-face).
WHAT DID THIS STUDY FIND?
The difference in past week alcohol consumption at the 3- and 6-month follow-up demonstrated that iCBT was non-inferior to (i.e., not worse than) face-to-face CBT.
Researchers in this study used a margin of 5 standard drinks to determine if iCBT was non-inferior to face-to-face CBT. In other words, the interventions would only be considered differentially effective if there was a difference in alcohol consumption outcomes of more than 5 standard drinks. When controlling for baseline alcohol consumption, the researchers found that the difference in past-week alcohol consumption in the iCBT group was non-inferior to (i.e., not worse than) the face-to-face group at both 3- and 6-month follow-up (see Figure 1). Another way of saying this is that the iCBT group performed as well despite receiving the CBT from a therapist over the internet, rather than in person.
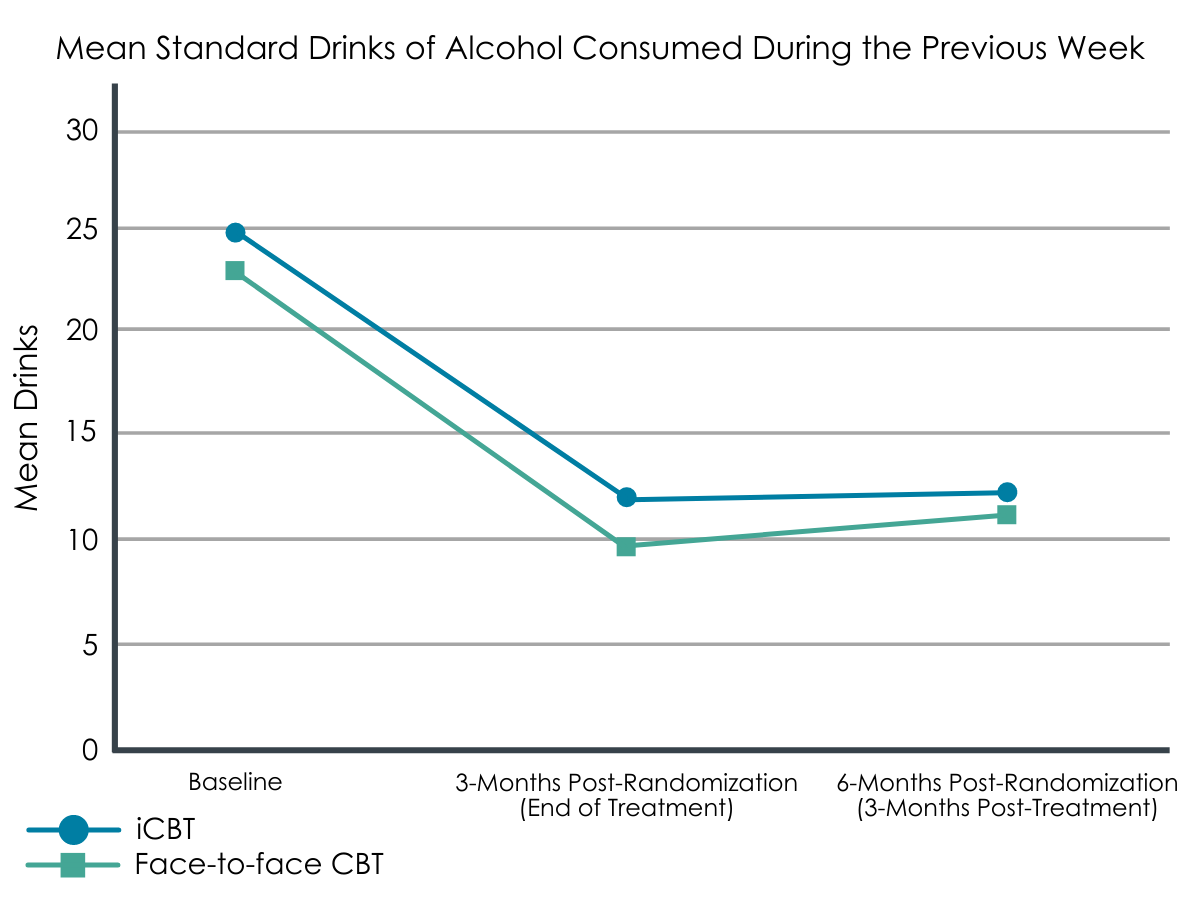
Figure 1.
iCBT was found to be non-inferior to (i.e., not worse than) face-to-face CBT on all secondary outcomes except for number of binge drinking days and harmful/hazardous alcohol use at the 6-month follow-up.
At the 6-month follow-up, iCBT was found to be non-inferior (i.e., not worse than) face-to-face CBT in terms of number of non-drinking days, number of DSM-5 alcohol use disorder criteria met, and on measures of depression, general anxiety disorder, and health related quality of life. However, iCBT was found to be inferior (i.e., worse than) face-to-face CBT in terms of number of binge drinking days and harmful/hazardous alcohol use at the 6-month follow-up. Of note, at the 3-month follow-up, iCBT was non-inferior (i.e., not worse than) face-to-face CBT on all secondary outcomes (i.e., harmful/hazardous alcohol use, number of DSM-5 alcohol use disorder criteria met, number of binge drinking days, number of non-drinking days, general anxiety disorder scores, and health related quality of life) with the exception of depression scores, where iCBT was found to be inferior to face-to-face CBT.
Face-to-face CBT participants completed more CBT treatments and rated the working alliance as stronger than participants in the iCBT group.
Overall, participants in the face-to-face group completed more CBT treatment modules than those in the therapist-facilitated online iCBT group, and also rated the strength and effect of the therapeutic relationship (i.e., the working alliance) as stronger. In terms of participants’ subjective experience with each treatment, compared to the in-person group, iCBT participants were less likely to consider the approach an “effective option for changing their drinking” and reported a “less personal” treatment experience, on average.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team found the online therapist-facilitated iCBT to be non-inferior (i.e., not worse than) in-person CBT on the primary outcome of past week alcohol consumption at the 6-month follow up, as well as the secondary outcome of past week alcohol consumption at the 3-month follow up. This means that upon treatment completion (i.e., the 3-month follow-up) and 3 months after finishing treatment (i.e., the 6-month follow-up), participants in both the intervention and the comparison condition were drinking at similar, reduced rates when compared to their baseline levels of drinking. This suggests that therapist-delivered CBT conducted over the internet may be as effective as CBT that is delivered in person in terms of total reductions in past week alcohol consumption. The research team also found that iCBT did as well as face-to-face CBT in terms of increasing non-drinking/abstinent days at the 6-month follow-up.
An important difference was observed, however, as iCBT was found to be inferior to face-to-face CBT on 1) harmful or hazardous alcohol use and 2) number of binge drinking days at the 6-month follow-up. These findings suggest that while participants in the iCBT and face-to-face group had similar numbers of non-drinking days and drinks in the past week, on the days when they did drink, iCBT participants drank more heavily and hazardously. Of note, this suggests there may be a more protective effect against more dangerous alcohol use patterns that is produced by ongoing in-person therapist interactions. It is plausible that in-person therapist interactions may help reduce these more dangerous drinking patterns by providing a stronger therapeutic alliance and greater accountability and helping patients to attend more sessions.
Indeed, overall, participants in the face-to-face group completed more treatment modules than those in the iCBT group. Participants in the iCBT group also viewed their treatment as less personal than those in the face-to-face group, and a smaller proportion of those in the iCBT group viewed the treatment as effective when compared to the face-to-face participants. Participants in the face-to-face group also rated the strength and effect of their therapeutic relationship with their treatment provider as stronger than those in the iCBT condition. Together these differences may have enabled participants in the face-to-face group to employ additional strategies or feel more comfortable reaching out for assistance on days when they did drink, thereby reducing the likelihood of heavy or hazardous drinking relative to the iCBT participants. For both researchers and providers, focusing specifically on ways to strengthen the working alliance between providers and patients who work together virtually could potentially help improve the effects of internet-delivered treatment, as well as patients’ satisfaction with and engagement in treatment.
Not to be forgotten among the above-mentioned results is that the research team also demonstrated non-inferiority for health-related quality of life, general anxiety disorder, and number of DSM-V alcohol use disorder criteria met at both the 3- and 6-month follow-ups (meaning that the iCBT was not worse than face-to-face treatment on all of these outcomes at both timepoints). These results indicate that therapist-facilitated iCBT may have more therapeutic similarities with face-to-face treatment that extend beyond alcohol use patterns and is a viable alternative to face-to-face treatment, particularly when internet-delivered treatment is the only option for specialized care.
From a broader public health perspective, this is particularly advantageous given that the reach of online treatments combined with its effectiveness has the potential to have a substantial impact on the overall health burden of alcohol use disorder. This is particularly true if the alternative to internet-delivered delivered is no treatment at all.
While internet-delivered treatments are a promising option for helping to bridge treatment gaps for people who may otherwise lack alcohol use disorder treatment access, not all internet-treatments are created – or delivered – equally. The results from this study should not be taken as an indication of the effectiveness of all internet-delivered therapies, which vary in their composition, pacing and intensity, and style and structure, all of which may influence their efficacy. This study also compared one specific type of CBT delivered either virtually using a therapist or face-to-face among a sample of largely employed, college educated, housed, married/cohabitating individuals with a demonstrated interest in internet delivered treatment. Efficacy in other populations may differ.
- LIMITATIONS
-
- Despite demonstrating that iCBT was non-inferior to face-to-face CBT in terms of past week alcohol consumption at the 3- and 6-month follow-ups, the five-drink non-inferiority limit may be considered too liberal and, as the authors report, is higher than what is typically used in evaluations of brief-interventions or face-to-face interventions used in community and primary care settings.
- The majority of participants in this study were well-educated, employed, had stable living situations and had demonstrated an interest in internet-based treatment. Efficacy of iCBT in other populations needs further testing.
- Attrition in this study was high: 33% of participants did not complete the 3-month follow up and 43% did not complete the 6-month follow up. Of note, although there were no differences in attrition between treatment groups at the 3- or 6-month follow-up, those who did not complete the 6-month follow up had higher general anxiety disorder scores at baseline compared to those who did complete the 6-month follow up. Once again, this somewhat limits the confidence that can be placed in these estimates of treatment efficacy. Results should be interpreted with caution given follow-up data were missing for a large portion of the sample.
BOTTOM LINE
Only a small minority of individuals with alcohol use disorder in need of treatment actually receive it. Accessing specialized alcohol use disorder treatment is a problem that prevents many people from getting the help they need.
This study found that internet-delivered CBT was therapeutically similar to face-to-face treatment for some abstinence and other alcohol-related outcomes as well as indices measuring quality of life, but results were mixed when it came to harmful or hazardous alcohol use, and number of binge-drinking days. Additionally, iCBT participants completed fewer CBT modules and the working alliance was rated as less strong in the iCBT group than in the face-to-face group.
Nonetheless, internet-delivered treatments remain an important way to help expand alcohol use disorder treatment access and, in some cases, may help reduce alcohol harms. Future research on strategies to improve the working alliance virtually could help improve internet-delivered treatment adherence and efficacy and, in turn, improve alcohol-related outcomes.
- For individuals and families seeking recovery: Accessing specialized treatment remains a challenge for individuals with alcohol use disorder and their families. Internet-delivered treatments are one way to expand specialized alcohol use disorder treatment to individuals who may otherwise lack access and can help some people reduce their drinking and other alcohol use disorder symptoms. Individuals and their families should be aware, however, that there are different types of internet-delivered treatments and are encouraged to talk to their providers about what types of treatments may be right for them.
- For treatment professionals and treatment systems: Internet delivered treatment may be beneficial for some patients, particularly those who may otherwise lack access to specialized alcohol use disorder treatment. Treatment providers should also be aware that some patients who receive internet-delivered treatment may view the therapeutic relationship as weaker than they would receiving in person treatment, which could impact treatment adherence and effectiveness. Given that the COVID-19 pandemic has led to a widespread shift to internet-delivered treatments, by focusing on virtual and individualized strategies, providers may be able to strengthen the working alliance and thereby improve patient outcomes.
- For scientists: The COVID-19 pandemic has highlighted ongoing barriers to alcohol use disorder treatment engagement, leading to the widespread adoption of internet-delivered treatments and digital recovery support services. Additional research is needed to assess which elements of internet-delivered treatment are most effective, which would benefit from further refinement and enhancement, and how such treatments may be combined with community-based digital recovery support services to improve outcomes. Research focused on identifying for whom internet-delivered therapy works best and strategies for strengthening the working alliance virtually can also help to strengthen the scientific literature in this area.
- For policy makers: Similar to SUD treatments delivered in person, internet-delivered treatments vary in their composition, style and frequency, and providers will need to determine what types of treatments are appropriate for which patients. Ensuring that alcohol use disorder treatments are available, accessible, and covered by insurance regardless of whether they are provided in-person or via the internet could help expand treatment access to more patients in need of treatment.
CITATIONS
Johansson, M., Sinadinovic, K., Gajecki, M., Lindner, P., Berman, A. H., Hermansson, U., & Andréasson, S. (2020). Internet-based therapy versus face-to-face therapy for alcohol use disorder, a randomized controlled non-inferiority trial. Addiction, [Epub ahead of print]. Doi: 10.1111/add.15270
