Mutual-help groups and medications for Opioid Use Disorder: Does attendance lead to greater medication continuance?
Keeping patients in opioid use disorder medication treatment is challenging, with two-thirds dropping out by 6 months. This study investigated the relationship between attendance at widely available mutual-help groups and successful completion of opioid use disorder medication treatment in a national sample.
Use of recovery support services like mutual-help groups are one of the factors associated with improved treatment retention and completion among individuals receiving treatment for substance use disorders broadly, and for opioid use disorder more specifically. However, it is unclear whether the benefits of mutual-help groups for treatment retention exist in the context of opioid use disorder medication treatment. Participation in 12-step mutual help groups like Narcotics Anonymous is associated with improved outcomes including retention for those taking the agonist medication buprenorphine, though some may also encounter negative messaging around their use of medication. Determining the role of individual patient/treatment factors, like mutual-help group participation, on medication treatment outcomes could ultimately help identify facilitators and supports for opioid use disorder treatment retention, completion, and sustained recovery. This study used national data and machine-learning models to evaluate the relationship between mutual-help group attendance and successful completion of opioid use disorder medication treatment in the United States.
HOW WAS THIS STUDY CONDUCTED?
This study used a machine-learning model to estimate the causal relationship between mutual-help group attendance and completion of opioid use disorder medication treatment, among a national sample. The influence of individual patient factors on treatment completion was also assessed.
Data were obtained from the Treatment Episode Data Set: Discharges (TEDS-D), which provides information on patients (e.g., demographics, substance use and treatment history) who received addiction treatment at publicly-funded facilities in the United States between 2015 and 2019. Data were collected at the time of a patient’s treatment admission and again at treatment discharge.
All patients included in the analyses (n=157,885) received a minimum of 30-days of outpatient, residential, or inpatient treatment for a primary opioid use disorder, and had methadone, buprenorphine, or naltrexone documented in their individual treatment plans. Mutual-help group participation was defined as attendance at any substance use disorder mutual-help group meeting (e.g., Alcoholics Anonymous, Narcotics Anonymous) 1 or more times in the 30 days before treatment discharge. Treatment completion status was assessed in 2 categories: 1) treatment completed: patient completed all parts of the treatment plan/program at the time of discharge; 2) treatment not completed: patient dropped out of treatment before the plan/program was completed or treatment was terminated early by the treatment facility. The use of medication treatment was not assessed beyond discharge, nor was the time in treatment specified by the plan to achieve completion. Some individuals may have transitioned to private healthcare facilities, which were not assessed here. Thus, successful treatment completion was defined as discharge from a publicly-funded outpatient, inpatient, or residential treatment facility, where a patient received medication treatment and discharge timing was appropriate from their clinician’s perspective.
Analyses excluded data from states (i.e. California, Alabama, Delaware, and Michigan) and individual patient records with substantial missing data on mutual-help group participation. Of the 2,533,964 patients who had a primary opioid use disorder in the data set, 12.8% received medication treatment and had available data on mutual-help group participation. Additional patient records were removed when key variables of interest were missing – ultimately, 6.23% of the original patient records were included in the analyses (n=157,885).
Machine learning approaches were used to select an ideal matched comparison group that minimizes bias and variance of the average effect when comparing mutual-help attendees to their respective matched non-attendee. Baseline characteristics driving selection of comparison group participants included demographics, treatment setting and referral source, frequency and route of primary substance use, non-opioid substance use, number of prior treatment episodes, and co-occurring mental health disorders. Subsequent analyses also assessed the extent to which these individual patient factors informing the selection of the matched comparison group and mutual-help participation were associated with treatment completion.
Among the final sample, 25% of patients completed treatment and 31% attended a mutual-help group meeting on 1 or more occasions. Patients were primarily non-Hispanic White (74%) and a little over half were men (60%). Forty-one percent of the sample was between the ages of 25 and 34 years old.
WHAT DID THIS STUDY FIND?
Mutual-help group attendance was associated with increased rates of treatment completion
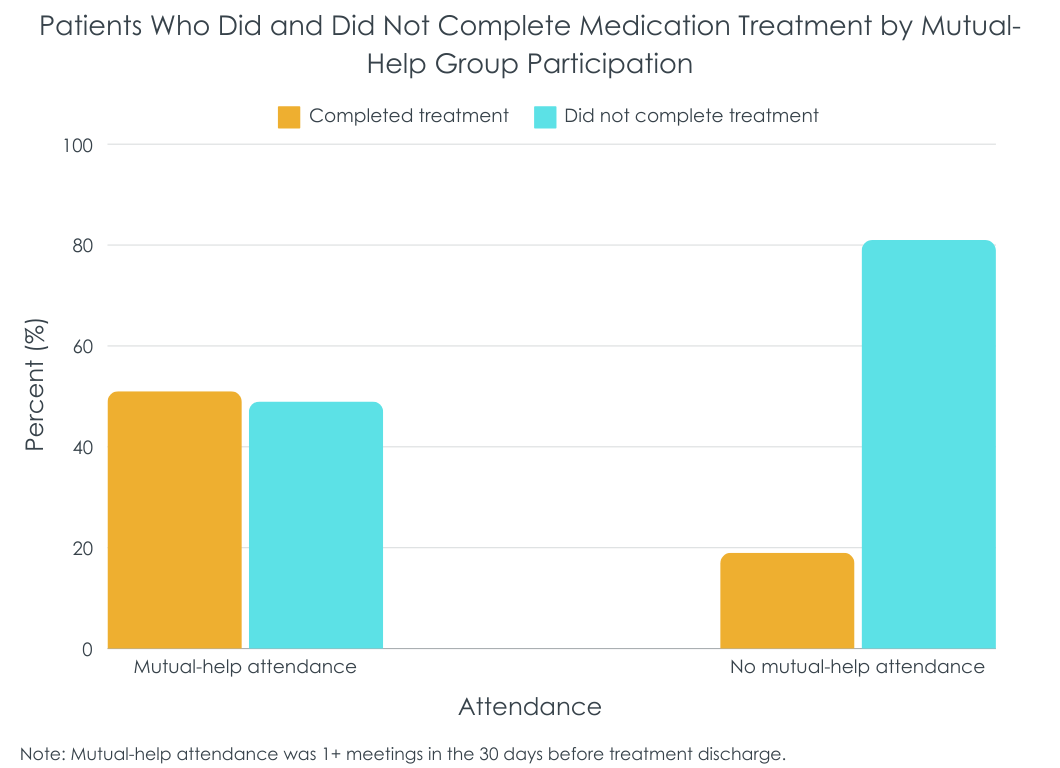
Patients who attended 1 or more mutual-help group meetings were more likely to successfully complete medication treatment than those who didn’t attend mutual-help meetings. Relative to the matched control group of non-attendees, mutual-help attendance was associated with a 26% increase in treatment completion rates (see figure below).
Meeting attendance was the strongest predictor of treatment completion
Individuals who had the highest likelihood of completing treatment were college educated (1.2 times more likely than high-school educated patients), non-Hispanic White and Black patients (1.8 and 1.0 times more likely than Hispanic patients), who had not used substances in the month prior to treatment admission (2.0 times more likely than patients engaged in daily use), were referred to treatment by the criminal justice system (1.9 times more likely that patients self-referred to treatment), and had attended 1 or more mutual-help meetings in the month prior to treatment discharge (3.1 times more likely than patients who didn’t attend a mutual-help meeting).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study showed that while many individual patient factors are associated with greater odds of treatment completion for patients taking opioid use disorder medications including the agonists buprenorphine and methadone as well as the antagonist naltrexone, attendance at 1 or more mutual-help group meetings in the 30 days prior to treatment discharge appears to be one of the strongest predictors. Mutual-help group linkages might be a promising option to help address less than favorable medication treatment completion rates across the US. For example, mutual-help groups are known to enhance recovery-oriented social support, which might help individuals engage with like-minded people to promote recovery-supportive thoughts and behaviors that support treatment engagement and completion.
It is clear that not everyone involved in mutual-help groups, or people with opioid use disorder more generally, are universally in favor of using medications to treat opioid use disorder. So, if mutual-help group participation does actually play a positive true causal role in improving the likelihood that a patient would continue to take their medication, it may have been due to the fact that such patients are participating in “medication friendly” groups, or are associating with other attendees who are supportive of medication continuation. Though the exact mechanisms underlying potential benefits to medication treatment completion are unclear in this study, mutual-help group participation may be a good option for individuals who are looking to support their medication treatment and recovery goals.
Importantly, not all mutual-help groups or chapters openly welcome individuals who are receiving medication treatment, particularly opioid agonist medication treatments (e.g., methadone, buprenorphine), because some consider the use of these medications as in conflict to their abstinence-based organizational models. Given the variability in medication attitudes across different mutual-help groups and different group chapters, additional research is needed for a more fine-grained analysis of the differential benefits of various mutual-help organizations for supporting medication treatment completion and preventing dropout. Medication type (agonist vs. antagonist), formulation (extended-release vs. daily dosing), and dose are also important factors when examining the effects related to mutual-help participation and opioid use disorder medication outcomes.
It is also worth highlighting that this study defined mutual-help group attendance as attendance at 1 or more meetings, and it is therefore unclear what the optimal ‘dose’ of mutual-help attendance might be for individuals who are receiving medication treatment. Active involvement in mutual-help groups, such as working with a sponsor/trusted member and socializing with other members outside the meetings, more strongly predicts substance use compared to attendance alone. The study’s approach to measuring treatment completion also requires additional context. It cannot be determined, for example, how long individuals received medications, nor which medication (of buprenorphine, methadone, or naltrexone) was taken. It may improve the utility of future studies examining mutual-help and opioid use disorder medications to add more precision in how these key variables are measured and operationally defined.
Because this was a cross-sectional study, it is unclear if those participating in mutual-help groups during treatment were also attending these groups prior to initiating treatment. Perhaps most significantly, individuals engaging in mutual-help organizations before and during treatment may represent a group with greater general motivation for treatment and recovery, who happen to use recovery support services in addition to medication treatment as part of their recovery pathways. In other words, they could be reaching out for anything that might help them. Indeed, this study found that other factors potentially associated with recovery motivation predicted treatment completion (e.g., no substance use in the month prior to treatment). Therefore, the directionality of the relationship between meeting attendance and treatment completion is hard to determine. It is possible that current recovery motivation may be driving increases in both medication use and mutual-help participation. Future research will clarify the role of motivation in the relationship between mutual-help group attendance and treatment retention, and whether initiating medication treatment and mutual-help groups at the same time produces similar benefits for treatment retention.
This study did not include privately-funded treatment facilities. Thus, findings may differ for patients receiving medication treatment from private primary care practices and community health centers.
This study excluded states with a high prevalence of missing data on patients’ mutual-help group participation, demanding additional research in these regions of the US. The type of medication treatment was also not considered in this study and additional research is needed to determine how this influences participation in mutual-help groups and treatment retention.
Because this was a cross-sectional study, it is unclear if those who attended mutual-help meetings were already engaged in these groups prior to medication treatment. Thus, findings could reflect baseline differences in patient motivation as opposed to causal effects of mutual-help meeting attendance in improving medication continuation. Additionally, this study assessed treatment completion among individuals who were receiving medication as part of their treatment plans and the researchers did not follow individuals who transitioned to medication treatment at privately funded primary care facilities. Thus, it is unclear how specific treatment plans and goals (e.g., planned duration of medication use in the context of a broader treatment program) affected outcomes, and whether treatment goals were affected beyond discharge from the publicly-funded facilities assessed in this study.
BOTTOM LINE
For individuals taking opioid use disorder medication, any mutual-help attendance in the 30-days before treatment discharge was the strongest predictor of successfully completing treatment. The study was cross-sectional, however, and there remains the potential that patient motivation accounted for the benefit of mutual-help despite the use of machine learning to create a rigorous comparison condition of non-attendees. While linkages to mutual-help for patients taking opioid use disorder medication could help improve retention and outcomes, longitudinal, experimental studies are needed.
For individuals and families seeking recovery: Attending mutual-help meetings during opioid use disorder treatment could be a good option for people who are looking to support their treatment and recovery goals. Individuals and families interested in mutual-help organizations are encouraged to explore onlineresources to learn about the various organizations and chapters near them, and to attend different meetings to find the right fit. Individuals receiving medication treatment are also encouraged to speak with their treatment providers about ways that they might be able to enhance their ability and willingness to continue treatment, as appropriate.
For treatment professionals and treatment systems: Findings highlight the potential for mutual-help organizations to support treatment completion among patients receiving opioid use disorder medication treatment as part of their treatment plan. Given that this cross-sectional study did not evaluate the influence of patient motivation, type of medication treatment (buprenorphine, methadone, Vivitrol), or type of mutual-help group (12-step, secular, etc.) on study outcomes, additional rigorous research is needed to clarify their role in treatment-service outcomes.
For scientists: Additional research is needed to examine the direct effects of mutual-help group participation on opioid use disorder medication treatment progress and outcomes. Randomized controlled trials and prospective studies are needed to determine the effects of different types of mutual-help organizations (e.g., 12-step, secular) and other recovery support services on medication treatment retention. Future studies should also examine the influence of service-use histories (e.g., pre-treatment use of mutual-help), patient motivation for treatment/recovery, type of medication (buprenorphine, methadone, extended-release naltrexone) and treatment facility (e.g., public, private), and additional patient-level factors (e.g., change in mental/physical health symptoms) on study outcomes.
For policy makers: Of those who discontinue opioid use disorder medication treatments like buprenorphine, about one-quarter discontinue within 1 month and two-thirds by 6 months. Since these medications are most effective when taken over longer periods of time, funding for research to identify best practices for enhancing treatment retention in the context of medication treatment may improve patient outcomes. Mutual-help organization linkage to, and active participation particularly in, medication friendly groups or participants could enhance the duration and benefits of medications for opioid use disorder.
Use of recovery support services like mutual-help groups are one of the factors associated with improved treatment retention and completion among individuals receiving treatment for substance use disorders broadly, and for opioid use disorder more specifically. However, it is unclear whether the benefits of mutual-help groups for treatment retention exist in the context of opioid use disorder medication treatment. Participation in 12-step mutual help groups like Narcotics Anonymous is associated with improved outcomes including retention for those taking the agonist medication buprenorphine, though some may also encounter negative messaging around their use of medication. Determining the role of individual patient/treatment factors, like mutual-help group participation, on medication treatment outcomes could ultimately help identify facilitators and supports for opioid use disorder treatment retention, completion, and sustained recovery. This study used national data and machine-learning models to evaluate the relationship between mutual-help group attendance and successful completion of opioid use disorder medication treatment in the United States.
HOW WAS THIS STUDY CONDUCTED?
This study used a machine-learning model to estimate the causal relationship between mutual-help group attendance and completion of opioid use disorder medication treatment, among a national sample. The influence of individual patient factors on treatment completion was also assessed.
Data were obtained from the Treatment Episode Data Set: Discharges (TEDS-D), which provides information on patients (e.g., demographics, substance use and treatment history) who received addiction treatment at publicly-funded facilities in the United States between 2015 and 2019. Data were collected at the time of a patient’s treatment admission and again at treatment discharge.
All patients included in the analyses (n=157,885) received a minimum of 30-days of outpatient, residential, or inpatient treatment for a primary opioid use disorder, and had methadone, buprenorphine, or naltrexone documented in their individual treatment plans. Mutual-help group participation was defined as attendance at any substance use disorder mutual-help group meeting (e.g., Alcoholics Anonymous, Narcotics Anonymous) 1 or more times in the 30 days before treatment discharge. Treatment completion status was assessed in 2 categories: 1) treatment completed: patient completed all parts of the treatment plan/program at the time of discharge; 2) treatment not completed: patient dropped out of treatment before the plan/program was completed or treatment was terminated early by the treatment facility. The use of medication treatment was not assessed beyond discharge, nor was the time in treatment specified by the plan to achieve completion. Some individuals may have transitioned to private healthcare facilities, which were not assessed here. Thus, successful treatment completion was defined as discharge from a publicly-funded outpatient, inpatient, or residential treatment facility, where a patient received medication treatment and discharge timing was appropriate from their clinician’s perspective.
Analyses excluded data from states (i.e. California, Alabama, Delaware, and Michigan) and individual patient records with substantial missing data on mutual-help group participation. Of the 2,533,964 patients who had a primary opioid use disorder in the data set, 12.8% received medication treatment and had available data on mutual-help group participation. Additional patient records were removed when key variables of interest were missing – ultimately, 6.23% of the original patient records were included in the analyses (n=157,885).
Machine learning approaches were used to select an ideal matched comparison group that minimizes bias and variance of the average effect when comparing mutual-help attendees to their respective matched non-attendee. Baseline characteristics driving selection of comparison group participants included demographics, treatment setting and referral source, frequency and route of primary substance use, non-opioid substance use, number of prior treatment episodes, and co-occurring mental health disorders. Subsequent analyses also assessed the extent to which these individual patient factors informing the selection of the matched comparison group and mutual-help participation were associated with treatment completion.
Among the final sample, 25% of patients completed treatment and 31% attended a mutual-help group meeting on 1 or more occasions. Patients were primarily non-Hispanic White (74%) and a little over half were men (60%). Forty-one percent of the sample was between the ages of 25 and 34 years old.
WHAT DID THIS STUDY FIND?
Mutual-help group attendance was associated with increased rates of treatment completion
Patients who attended 1 or more mutual-help group meetings were more likely to successfully complete medication treatment than those who didn’t attend mutual-help meetings. Relative to the matched control group of non-attendees, mutual-help attendance was associated with a 26% increase in treatment completion rates (see figure below).
Meeting attendance was the strongest predictor of treatment completion
Individuals who had the highest likelihood of completing treatment were college educated (1.2 times more likely than high-school educated patients), non-Hispanic White and Black patients (1.8 and 1.0 times more likely than Hispanic patients), who had not used substances in the month prior to treatment admission (2.0 times more likely than patients engaged in daily use), were referred to treatment by the criminal justice system (1.9 times more likely that patients self-referred to treatment), and had attended 1 or more mutual-help meetings in the month prior to treatment discharge (3.1 times more likely than patients who didn’t attend a mutual-help meeting).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study showed that while many individual patient factors are associated with greater odds of treatment completion for patients taking opioid use disorder medications including the agonists buprenorphine and methadone as well as the antagonist naltrexone, attendance at 1 or more mutual-help group meetings in the 30 days prior to treatment discharge appears to be one of the strongest predictors. Mutual-help group linkages might be a promising option to help address less than favorable medication treatment completion rates across the US. For example, mutual-help groups are known to enhance recovery-oriented social support, which might help individuals engage with like-minded people to promote recovery-supportive thoughts and behaviors that support treatment engagement and completion.
It is clear that not everyone involved in mutual-help groups, or people with opioid use disorder more generally, are universally in favor of using medications to treat opioid use disorder. So, if mutual-help group participation does actually play a positive true causal role in improving the likelihood that a patient would continue to take their medication, it may have been due to the fact that such patients are participating in “medication friendly” groups, or are associating with other attendees who are supportive of medication continuation. Though the exact mechanisms underlying potential benefits to medication treatment completion are unclear in this study, mutual-help group participation may be a good option for individuals who are looking to support their medication treatment and recovery goals.
Importantly, not all mutual-help groups or chapters openly welcome individuals who are receiving medication treatment, particularly opioid agonist medication treatments (e.g., methadone, buprenorphine), because some consider the use of these medications as in conflict to their abstinence-based organizational models. Given the variability in medication attitudes across different mutual-help groups and different group chapters, additional research is needed for a more fine-grained analysis of the differential benefits of various mutual-help organizations for supporting medication treatment completion and preventing dropout. Medication type (agonist vs. antagonist), formulation (extended-release vs. daily dosing), and dose are also important factors when examining the effects related to mutual-help participation and opioid use disorder medication outcomes.
It is also worth highlighting that this study defined mutual-help group attendance as attendance at 1 or more meetings, and it is therefore unclear what the optimal ‘dose’ of mutual-help attendance might be for individuals who are receiving medication treatment. Active involvement in mutual-help groups, such as working with a sponsor/trusted member and socializing with other members outside the meetings, more strongly predicts substance use compared to attendance alone. The study’s approach to measuring treatment completion also requires additional context. It cannot be determined, for example, how long individuals received medications, nor which medication (of buprenorphine, methadone, or naltrexone) was taken. It may improve the utility of future studies examining mutual-help and opioid use disorder medications to add more precision in how these key variables are measured and operationally defined.
Because this was a cross-sectional study, it is unclear if those participating in mutual-help groups during treatment were also attending these groups prior to initiating treatment. Perhaps most significantly, individuals engaging in mutual-help organizations before and during treatment may represent a group with greater general motivation for treatment and recovery, who happen to use recovery support services in addition to medication treatment as part of their recovery pathways. In other words, they could be reaching out for anything that might help them. Indeed, this study found that other factors potentially associated with recovery motivation predicted treatment completion (e.g., no substance use in the month prior to treatment). Therefore, the directionality of the relationship between meeting attendance and treatment completion is hard to determine. It is possible that current recovery motivation may be driving increases in both medication use and mutual-help participation. Future research will clarify the role of motivation in the relationship between mutual-help group attendance and treatment retention, and whether initiating medication treatment and mutual-help groups at the same time produces similar benefits for treatment retention.
This study did not include privately-funded treatment facilities. Thus, findings may differ for patients receiving medication treatment from private primary care practices and community health centers.
This study excluded states with a high prevalence of missing data on patients’ mutual-help group participation, demanding additional research in these regions of the US. The type of medication treatment was also not considered in this study and additional research is needed to determine how this influences participation in mutual-help groups and treatment retention.
Because this was a cross-sectional study, it is unclear if those who attended mutual-help meetings were already engaged in these groups prior to medication treatment. Thus, findings could reflect baseline differences in patient motivation as opposed to causal effects of mutual-help meeting attendance in improving medication continuation. Additionally, this study assessed treatment completion among individuals who were receiving medication as part of their treatment plans and the researchers did not follow individuals who transitioned to medication treatment at privately funded primary care facilities. Thus, it is unclear how specific treatment plans and goals (e.g., planned duration of medication use in the context of a broader treatment program) affected outcomes, and whether treatment goals were affected beyond discharge from the publicly-funded facilities assessed in this study.
BOTTOM LINE
For individuals taking opioid use disorder medication, any mutual-help attendance in the 30-days before treatment discharge was the strongest predictor of successfully completing treatment. The study was cross-sectional, however, and there remains the potential that patient motivation accounted for the benefit of mutual-help despite the use of machine learning to create a rigorous comparison condition of non-attendees. While linkages to mutual-help for patients taking opioid use disorder medication could help improve retention and outcomes, longitudinal, experimental studies are needed.
For individuals and families seeking recovery: Attending mutual-help meetings during opioid use disorder treatment could be a good option for people who are looking to support their treatment and recovery goals. Individuals and families interested in mutual-help organizations are encouraged to explore onlineresources to learn about the various organizations and chapters near them, and to attend different meetings to find the right fit. Individuals receiving medication treatment are also encouraged to speak with their treatment providers about ways that they might be able to enhance their ability and willingness to continue treatment, as appropriate.
For treatment professionals and treatment systems: Findings highlight the potential for mutual-help organizations to support treatment completion among patients receiving opioid use disorder medication treatment as part of their treatment plan. Given that this cross-sectional study did not evaluate the influence of patient motivation, type of medication treatment (buprenorphine, methadone, Vivitrol), or type of mutual-help group (12-step, secular, etc.) on study outcomes, additional rigorous research is needed to clarify their role in treatment-service outcomes.
For scientists: Additional research is needed to examine the direct effects of mutual-help group participation on opioid use disorder medication treatment progress and outcomes. Randomized controlled trials and prospective studies are needed to determine the effects of different types of mutual-help organizations (e.g., 12-step, secular) and other recovery support services on medication treatment retention. Future studies should also examine the influence of service-use histories (e.g., pre-treatment use of mutual-help), patient motivation for treatment/recovery, type of medication (buprenorphine, methadone, extended-release naltrexone) and treatment facility (e.g., public, private), and additional patient-level factors (e.g., change in mental/physical health symptoms) on study outcomes.
For policy makers: Of those who discontinue opioid use disorder medication treatments like buprenorphine, about one-quarter discontinue within 1 month and two-thirds by 6 months. Since these medications are most effective when taken over longer periods of time, funding for research to identify best practices for enhancing treatment retention in the context of medication treatment may improve patient outcomes. Mutual-help organization linkage to, and active participation particularly in, medication friendly groups or participants could enhance the duration and benefits of medications for opioid use disorder.
Use of recovery support services like mutual-help groups are one of the factors associated with improved treatment retention and completion among individuals receiving treatment for substance use disorders broadly, and for opioid use disorder more specifically. However, it is unclear whether the benefits of mutual-help groups for treatment retention exist in the context of opioid use disorder medication treatment. Participation in 12-step mutual help groups like Narcotics Anonymous is associated with improved outcomes including retention for those taking the agonist medication buprenorphine, though some may also encounter negative messaging around their use of medication. Determining the role of individual patient/treatment factors, like mutual-help group participation, on medication treatment outcomes could ultimately help identify facilitators and supports for opioid use disorder treatment retention, completion, and sustained recovery. This study used national data and machine-learning models to evaluate the relationship between mutual-help group attendance and successful completion of opioid use disorder medication treatment in the United States.
HOW WAS THIS STUDY CONDUCTED?
This study used a machine-learning model to estimate the causal relationship between mutual-help group attendance and completion of opioid use disorder medication treatment, among a national sample. The influence of individual patient factors on treatment completion was also assessed.
Data were obtained from the Treatment Episode Data Set: Discharges (TEDS-D), which provides information on patients (e.g., demographics, substance use and treatment history) who received addiction treatment at publicly-funded facilities in the United States between 2015 and 2019. Data were collected at the time of a patient’s treatment admission and again at treatment discharge.
All patients included in the analyses (n=157,885) received a minimum of 30-days of outpatient, residential, or inpatient treatment for a primary opioid use disorder, and had methadone, buprenorphine, or naltrexone documented in their individual treatment plans. Mutual-help group participation was defined as attendance at any substance use disorder mutual-help group meeting (e.g., Alcoholics Anonymous, Narcotics Anonymous) 1 or more times in the 30 days before treatment discharge. Treatment completion status was assessed in 2 categories: 1) treatment completed: patient completed all parts of the treatment plan/program at the time of discharge; 2) treatment not completed: patient dropped out of treatment before the plan/program was completed or treatment was terminated early by the treatment facility. The use of medication treatment was not assessed beyond discharge, nor was the time in treatment specified by the plan to achieve completion. Some individuals may have transitioned to private healthcare facilities, which were not assessed here. Thus, successful treatment completion was defined as discharge from a publicly-funded outpatient, inpatient, or residential treatment facility, where a patient received medication treatment and discharge timing was appropriate from their clinician’s perspective.
Analyses excluded data from states (i.e. California, Alabama, Delaware, and Michigan) and individual patient records with substantial missing data on mutual-help group participation. Of the 2,533,964 patients who had a primary opioid use disorder in the data set, 12.8% received medication treatment and had available data on mutual-help group participation. Additional patient records were removed when key variables of interest were missing – ultimately, 6.23% of the original patient records were included in the analyses (n=157,885).
Machine learning approaches were used to select an ideal matched comparison group that minimizes bias and variance of the average effect when comparing mutual-help attendees to their respective matched non-attendee. Baseline characteristics driving selection of comparison group participants included demographics, treatment setting and referral source, frequency and route of primary substance use, non-opioid substance use, number of prior treatment episodes, and co-occurring mental health disorders. Subsequent analyses also assessed the extent to which these individual patient factors informing the selection of the matched comparison group and mutual-help participation were associated with treatment completion.
Among the final sample, 25% of patients completed treatment and 31% attended a mutual-help group meeting on 1 or more occasions. Patients were primarily non-Hispanic White (74%) and a little over half were men (60%). Forty-one percent of the sample was between the ages of 25 and 34 years old.
WHAT DID THIS STUDY FIND?
Mutual-help group attendance was associated with increased rates of treatment completion
Patients who attended 1 or more mutual-help group meetings were more likely to successfully complete medication treatment than those who didn’t attend mutual-help meetings. Relative to the matched control group of non-attendees, mutual-help attendance was associated with a 26% increase in treatment completion rates (see figure below).
Meeting attendance was the strongest predictor of treatment completion
Individuals who had the highest likelihood of completing treatment were college educated (1.2 times more likely than high-school educated patients), non-Hispanic White and Black patients (1.8 and 1.0 times more likely than Hispanic patients), who had not used substances in the month prior to treatment admission (2.0 times more likely than patients engaged in daily use), were referred to treatment by the criminal justice system (1.9 times more likely that patients self-referred to treatment), and had attended 1 or more mutual-help meetings in the month prior to treatment discharge (3.1 times more likely than patients who didn’t attend a mutual-help meeting).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study showed that while many individual patient factors are associated with greater odds of treatment completion for patients taking opioid use disorder medications including the agonists buprenorphine and methadone as well as the antagonist naltrexone, attendance at 1 or more mutual-help group meetings in the 30 days prior to treatment discharge appears to be one of the strongest predictors. Mutual-help group linkages might be a promising option to help address less than favorable medication treatment completion rates across the US. For example, mutual-help groups are known to enhance recovery-oriented social support, which might help individuals engage with like-minded people to promote recovery-supportive thoughts and behaviors that support treatment engagement and completion.
It is clear that not everyone involved in mutual-help groups, or people with opioid use disorder more generally, are universally in favor of using medications to treat opioid use disorder. So, if mutual-help group participation does actually play a positive true causal role in improving the likelihood that a patient would continue to take their medication, it may have been due to the fact that such patients are participating in “medication friendly” groups, or are associating with other attendees who are supportive of medication continuation. Though the exact mechanisms underlying potential benefits to medication treatment completion are unclear in this study, mutual-help group participation may be a good option for individuals who are looking to support their medication treatment and recovery goals.
Importantly, not all mutual-help groups or chapters openly welcome individuals who are receiving medication treatment, particularly opioid agonist medication treatments (e.g., methadone, buprenorphine), because some consider the use of these medications as in conflict to their abstinence-based organizational models. Given the variability in medication attitudes across different mutual-help groups and different group chapters, additional research is needed for a more fine-grained analysis of the differential benefits of various mutual-help organizations for supporting medication treatment completion and preventing dropout. Medication type (agonist vs. antagonist), formulation (extended-release vs. daily dosing), and dose are also important factors when examining the effects related to mutual-help participation and opioid use disorder medication outcomes.
It is also worth highlighting that this study defined mutual-help group attendance as attendance at 1 or more meetings, and it is therefore unclear what the optimal ‘dose’ of mutual-help attendance might be for individuals who are receiving medication treatment. Active involvement in mutual-help groups, such as working with a sponsor/trusted member and socializing with other members outside the meetings, more strongly predicts substance use compared to attendance alone. The study’s approach to measuring treatment completion also requires additional context. It cannot be determined, for example, how long individuals received medications, nor which medication (of buprenorphine, methadone, or naltrexone) was taken. It may improve the utility of future studies examining mutual-help and opioid use disorder medications to add more precision in how these key variables are measured and operationally defined.
Because this was a cross-sectional study, it is unclear if those participating in mutual-help groups during treatment were also attending these groups prior to initiating treatment. Perhaps most significantly, individuals engaging in mutual-help organizations before and during treatment may represent a group with greater general motivation for treatment and recovery, who happen to use recovery support services in addition to medication treatment as part of their recovery pathways. In other words, they could be reaching out for anything that might help them. Indeed, this study found that other factors potentially associated with recovery motivation predicted treatment completion (e.g., no substance use in the month prior to treatment). Therefore, the directionality of the relationship between meeting attendance and treatment completion is hard to determine. It is possible that current recovery motivation may be driving increases in both medication use and mutual-help participation. Future research will clarify the role of motivation in the relationship between mutual-help group attendance and treatment retention, and whether initiating medication treatment and mutual-help groups at the same time produces similar benefits for treatment retention.
This study did not include privately-funded treatment facilities. Thus, findings may differ for patients receiving medication treatment from private primary care practices and community health centers.
This study excluded states with a high prevalence of missing data on patients’ mutual-help group participation, demanding additional research in these regions of the US. The type of medication treatment was also not considered in this study and additional research is needed to determine how this influences participation in mutual-help groups and treatment retention.
Because this was a cross-sectional study, it is unclear if those who attended mutual-help meetings were already engaged in these groups prior to medication treatment. Thus, findings could reflect baseline differences in patient motivation as opposed to causal effects of mutual-help meeting attendance in improving medication continuation. Additionally, this study assessed treatment completion among individuals who were receiving medication as part of their treatment plans and the researchers did not follow individuals who transitioned to medication treatment at privately funded primary care facilities. Thus, it is unclear how specific treatment plans and goals (e.g., planned duration of medication use in the context of a broader treatment program) affected outcomes, and whether treatment goals were affected beyond discharge from the publicly-funded facilities assessed in this study.
BOTTOM LINE
For individuals taking opioid use disorder medication, any mutual-help attendance in the 30-days before treatment discharge was the strongest predictor of successfully completing treatment. The study was cross-sectional, however, and there remains the potential that patient motivation accounted for the benefit of mutual-help despite the use of machine learning to create a rigorous comparison condition of non-attendees. While linkages to mutual-help for patients taking opioid use disorder medication could help improve retention and outcomes, longitudinal, experimental studies are needed.
For individuals and families seeking recovery: Attending mutual-help meetings during opioid use disorder treatment could be a good option for people who are looking to support their treatment and recovery goals. Individuals and families interested in mutual-help organizations are encouraged to explore onlineresources to learn about the various organizations and chapters near them, and to attend different meetings to find the right fit. Individuals receiving medication treatment are also encouraged to speak with their treatment providers about ways that they might be able to enhance their ability and willingness to continue treatment, as appropriate.
For treatment professionals and treatment systems: Findings highlight the potential for mutual-help organizations to support treatment completion among patients receiving opioid use disorder medication treatment as part of their treatment plan. Given that this cross-sectional study did not evaluate the influence of patient motivation, type of medication treatment (buprenorphine, methadone, Vivitrol), or type of mutual-help group (12-step, secular, etc.) on study outcomes, additional rigorous research is needed to clarify their role in treatment-service outcomes.
For scientists: Additional research is needed to examine the direct effects of mutual-help group participation on opioid use disorder medication treatment progress and outcomes. Randomized controlled trials and prospective studies are needed to determine the effects of different types of mutual-help organizations (e.g., 12-step, secular) and other recovery support services on medication treatment retention. Future studies should also examine the influence of service-use histories (e.g., pre-treatment use of mutual-help), patient motivation for treatment/recovery, type of medication (buprenorphine, methadone, extended-release naltrexone) and treatment facility (e.g., public, private), and additional patient-level factors (e.g., change in mental/physical health symptoms) on study outcomes.
For policy makers: Of those who discontinue opioid use disorder medication treatments like buprenorphine, about one-quarter discontinue within 1 month and two-thirds by 6 months. Since these medications are most effective when taken over longer periods of time, funding for research to identify best practices for enhancing treatment retention in the context of medication treatment may improve patient outcomes. Mutual-help organization linkage to, and active participation particularly in, medication friendly groups or participants could enhance the duration and benefits of medications for opioid use disorder.