Greater mutual-help benefit for Black vs. White individuals with opioid use disorder helps offset treatment completion disadvantage
Research that identifies strategies to address the disadvantages faced by racial and ethnic minorities in substance use disorder care can improve health equity for these marginalized groups. This study examined whether mutual-help participation improved opioid use disorder treatment completion for men and women of differing races and ethnicities.
Whereas mutual-help participation has been looked at to some degree in populations with opioid use disorder little research has examined the impact of so called “intersectionality” on mutual-help participation (i.e., the intersection of demographic variables like race/ethnicity, sex/gender, age and so on with mutual-help participation and benefits) and treatment, despite documented disparities in substance use treatment completion among Black, Latinx, and Indigenous populations when compared to White groups in the U.S. There are some people who believe that 12-step meetings cater only to White, middle-class men, raising concerns about potential racial/ethnic and/or sex disparities in mutual-help participation.
A prior review of 19 studies, however, showed weak evidence for differences. Most studies in the review showed no racial/ethnic differences in mutual-help attendance, with some evidence weekly suggestive of disparities for Latinx immigrants, women, and adolescents, as well as Black women and adolescents. The review concluded that overall, studies were “dated” and “inconsistent”, highlighting the need for additional research in this area.
This study sought to help further our understanding of the role mutual-help group participation can play in opioid use disorder treatment and whether such benefits are equitable across specific gender and racial/ethnic groups.
HOW WAS THIS STUDY CONDUCTED?
The researchers used a large publicly available SAMHSA data set to examine nearly 200,000 adults (N = 199,779) in outpatient or intensive outpatient opioid use treatment from 2015-2017 and their treatment completion outcomes. Participants’ clinical data upon discharge were used to examine the association between mutual-help participation in the 30 days prior to discharge and treatment completion status, as well as to examine group differences by race/ethnicity and sex.
Participants were included in this study if they were adults (18 years of age or older), participated in at least 30 days of outpatient or intensive outpatient treatment (IOP), and their reported primary substance upon admission was opioids. Participants were excluded if they were in another type of substance use treatment (e.g., residential), were in treatment for fewer than 30 days, or their reported primary substance was something other than opioids. Because the researchers were interested in the specific role of mutual-help groups in the community (as opposed to mutual help group participation within a residential treatment setting), the study only included participants in outpatient treatment or intensive outpatient treatment who had no record of prior treatment episodes. Participants who had missing responses for variables of interest were also excluded from the study.
Large publicly available data sets, like the SAMSHA data set used in the current study, often heavily rely on reports of clinic administrative data, meaning, data may be entered by treatment staff or providers, rather than asking patients directly. In the current study, to assess self-help participation, the study asked, “Did the participant participate in self-help groups in the 30 days prior to discharge?” Response options were: treatment completed, dropped out of treatment, terminated by facility, transferred to another treatment program or facility, incarcerated, death, or other. The researchers then grouped participants into “successful” (i.e., treatment completed) or “unsuccessful” (i.e., dropped out of treatment or terminated by facility) treatment completion groups. Participants with discharge statuses of a) transferred to another treatment program or facility, b) incarcerated, c) death, or d) other were excluded from this study.
The researchers used reports of participants’ race, ethnicity, and sex in the data to create 10 groups: American Indian/Alaska Native (AI/ AN) men, AI/AN women, Asian/Pacific Islander (PI) men, Asian/PI women, Black men, Black women, Hispanic men, Hispanic women, White men, and White women. Hispanic men and women included individuals of all racial identities who indicated their ethnicity as Hispanic. Individuals in all other racial categories include individuals who indicated their ethnicity as non-Hispanic.
First, the researchers tested the association between mutual-help participation and treatment completion by race/ethnicity, while controlling for participants’ education, length of stay in treatment, employment status at discharge, and age at admission, to see if a) the effect of mutual-help participation was associated independently with greater rates of treatment completion, and b) if this effect differed by race/ethnicity. In the second analysis, the researchers examined differences in the association between mutual-help participation and treatment completion by race/ethnicity and sex, while controlling for the same demographic and clinical factors. This kind of analysis is intended to help clarify if there are specific differences in the effect of mutual-help participation on treatment completion for, say, American Indian/Alaskan Native women compared to another specific group, like, Hispanic men, while accounting for other differences that could affect treatment completion (i.e., education, length of stay in treatment, employment status at discharge, and age at admission).
Participants in this study were mostly White, with White women accounting for 33.2% of the sample and White men accounting for 43.4% of the sample. Fewer participants were Black men (7.9%), Black women (4.3%), Hispanic men (4.9%), and Hispanic women (2.8%). American
Indian/Alaskan Native (AI/AN) and Asian/Pacific Islander (PI) men and women each accounted for less than 1% of the sample, respectively. The sample was mostly younger to middle aged, with 65% falling between ages 25-44. Almost half of the sample had completed high school (48.4%), and only 36% were employed (part or full-time) at time of discharge from treatment. Participants’ length of stay in treatment varied from 30 days to more than 1 year.
A majority of these patients with primary opioid use disorder did not participate in any mutual-help (self-help) (71.4%) and did not “successfully” complete treatment (i.e., dropped out of treatment or treatment was terminated by the facility, 62.4%). Although still quite low, the highest rates of treatment completion were among White men (40.9%), Asian/PI men (39.2%), White women (38.4%), and Hispanic men (37.5%), followed by Hispanic women (34.3%) and Asian/PI women (33.6%). The lowest treatment completion rates were among AI/AN men (31.2%), Black men (28.7%), AI/AN women (27.1%), and Black women (23.4%).
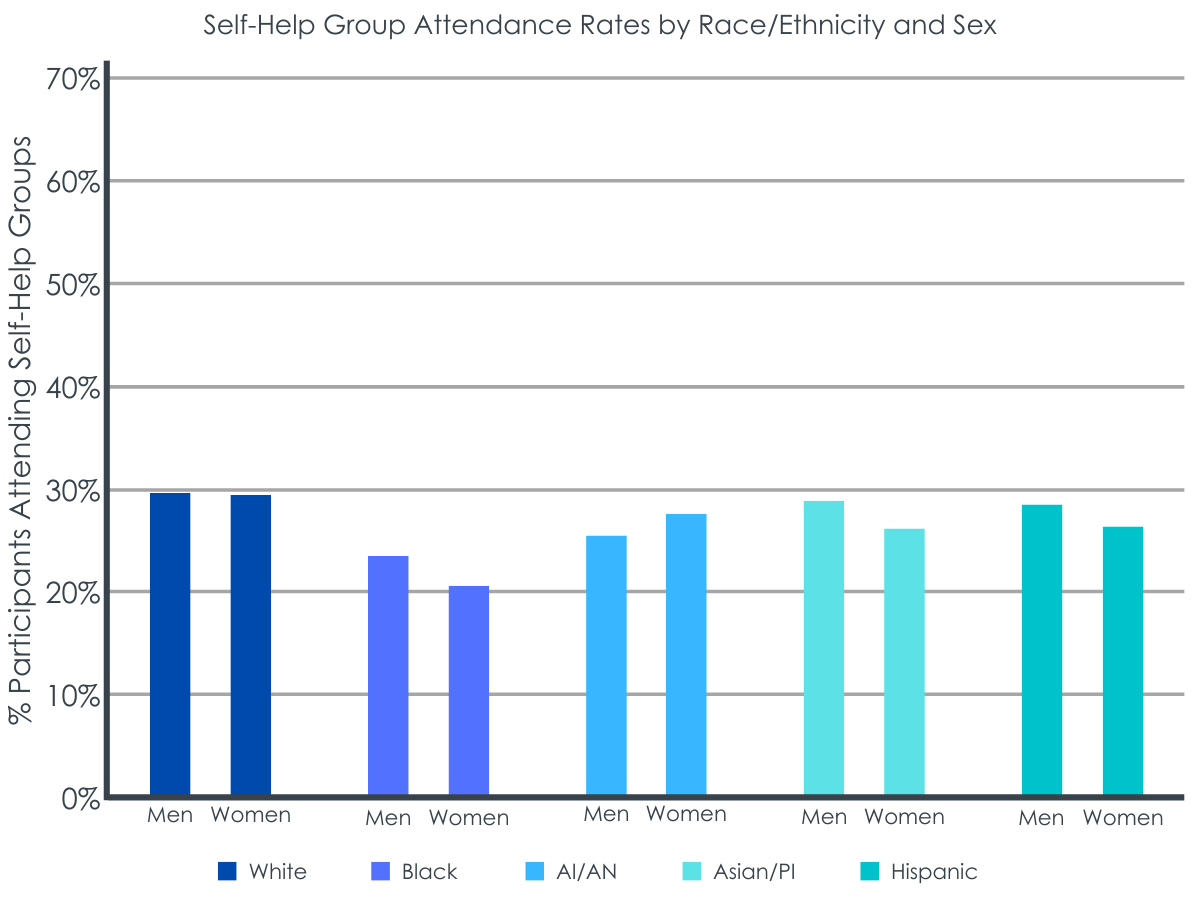
The highest rates of mutual-help group attendance were among White men (29.6%), White women (29.5%), Asian/PI men (29.0%), Hispanic men (28.1%), and AI/AN women (27.4%), followed by Hispanic women (26.3%), Asian/PI women (26.1%), and AI/AN men (25.6%). The lowest rates of mutual-help group attendance were among Black men (23.7%) and Black women (20.8%).
WHAT DID THIS STUDY FIND?
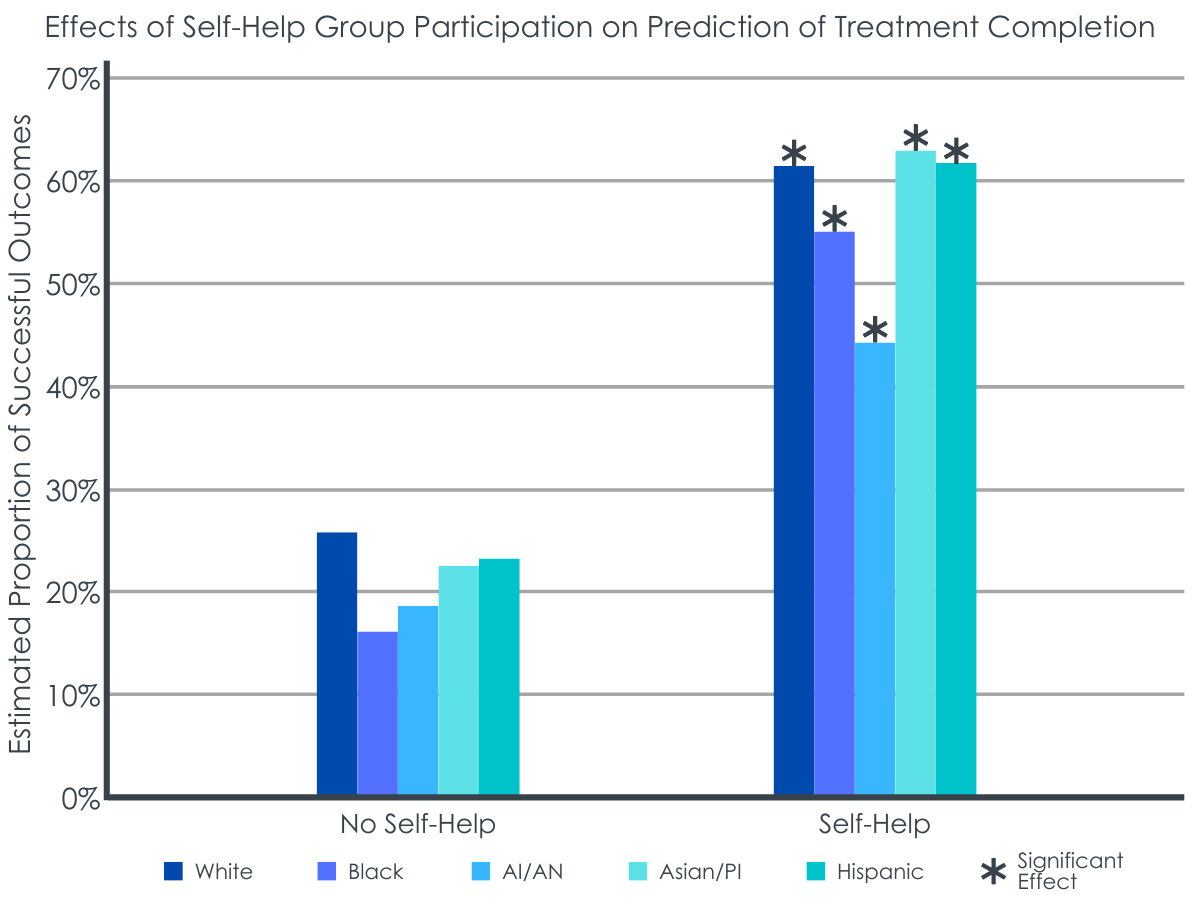
Mutual-help attendance overall was associated with treatment completion.
Controlling for the interaction of race/ethnicity, sex, and mutual-help participation, mutual-help participation was independently associated with treatment completion, with those who attended mutual-help meetings having 4.5 times greater odds of completing treatment compared to no mutual-help meeting participation in the 30 days prior to discharge, while controlling for demographic and clinical characteristics.
Black men and Black women benefitted more from mutual-help participation than other groups.
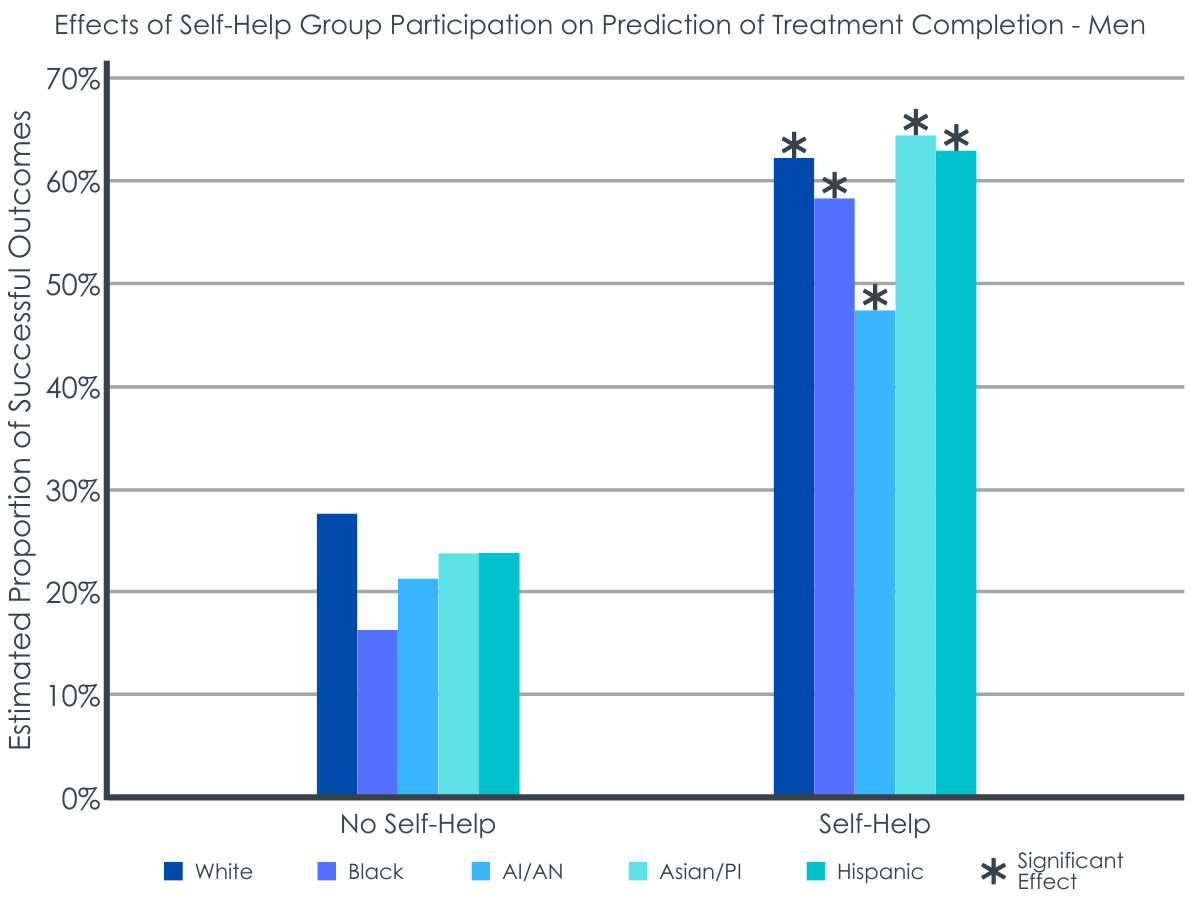
Despite the lower mutual-help participation among Black men and women, Black men showed the largest positive association between mutual-help group participation and treatment completion compared to men of other races/ethnicities. The largest difference was between Black men and White men. Compared to White men, the association between mutual-help participation and treatment completion was about 50% stronger for Black men. In other words, there was a larger difference in treatment completion rates between Black men who did and Black men who did not attend mutual-help prior to treatment discharge, than between White men who did and did not attend mutual-help prior to treatment discharge. However, White men had higher rates of treatment completion, overall, irrespective of mutual-help attendance.
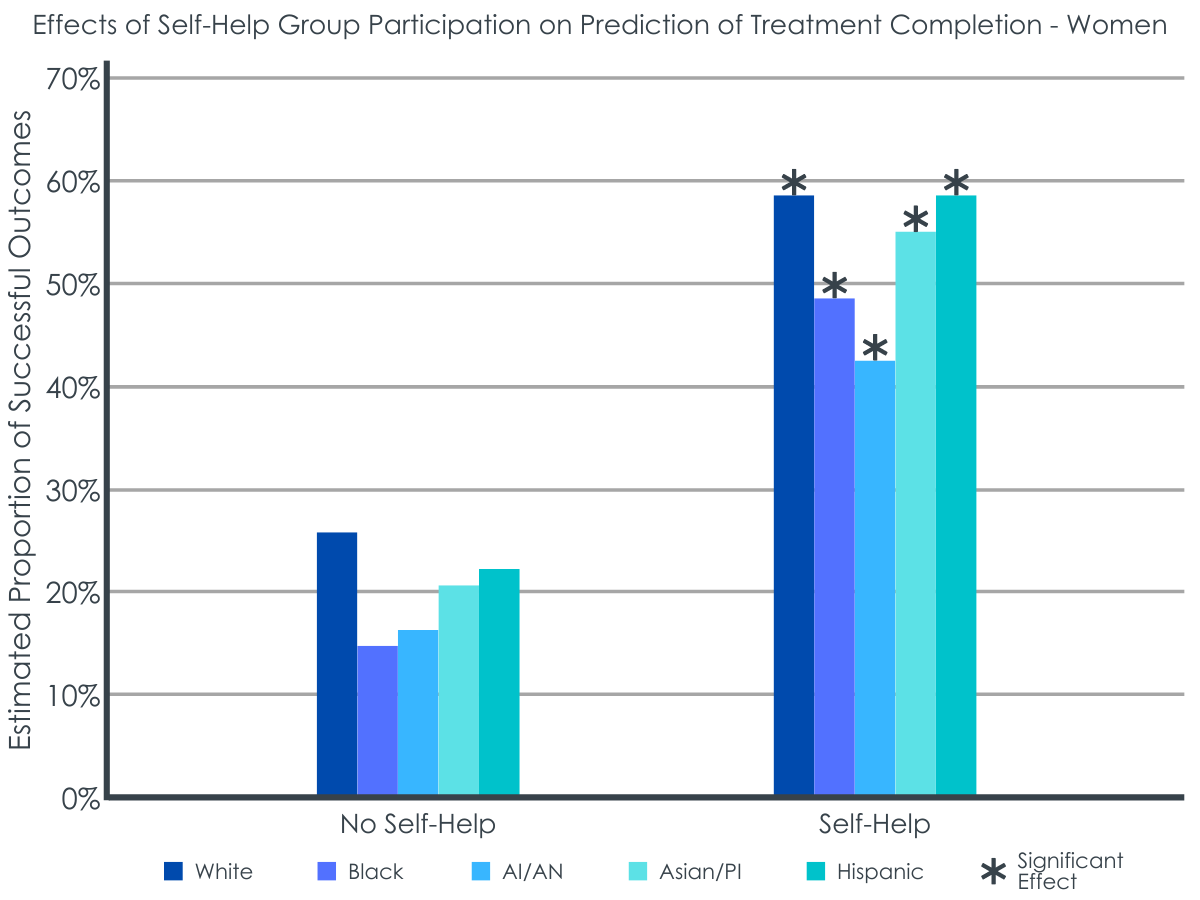
Similarly, among women, Black women as well as Hispanic women benefitted more from mutual-help participation than White women and American Indian/Alaskan Native women. The largest difference was between Black women and American Indian/Alaskan Native women. Compared to American Indian/Alaskan Native women, the association between mutual-help participation and treatment completion was 47% stronger for Black women. There were no differences in the benefits of attending mutual-help on treatment completion outcomes between White, American Indian/Alaskan Native, and Asian/Pacific Islander women.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For all racial, ethnic, and sex groups in this study, the study participants – comprised of outpatients with primary opioid use disorder – were more likely to complete treatment if they had attended mutual-help in the 30 days prior to discharge compared to participants who did not attend. From the current study, it cannot be concluded if greater mutual-help participation played a causative role in helping people to complete their treatment. It might be the case that that these individuals simply were more motivated to change thus were looking wherever they could to find support including from mutual-help organizations as well as treatment. There is good evidence however, that while this might be true, there is also a causative role in mutual-help participation improving treatment adherence and improving outcomes. Mutual-help attendance may well provide support and resources for individuals in opioid use treatment to help them reach their treatment goals. This is consistent with a body of literature that shows Alcoholics Anonymous produces comparable rates of alcohol abstinence to first line clinical treatments, and higher levels of 12-step involvement is associated with greater abstinence for individuals with other drug use problems. This may be somewhat surprising given reports of negative attitudes in 12-step towards individuals taking medications for opioid use disorder, including refusals to sponsor (act as a recovery mentor) people utilizing opioid use disorder medications. That said, the researchers of this study did not report the degree of opioid use disorder medication usage that might have influenced such participation. Mutual-help groups other than 12-step-based ones exist (e.g., SMART Recovery, Women for Sobriety, Recovery Dharma). Even within 12-step, all groups are autonomous and may have differing norms, customs, and attitudes regarding medication. This variety means that some individual mutual-help meetings may have more positive attitudes towards opioid use disorder medications than others. The researchers may not have had access to information about the types of mutual-help groups participants attended and did not report if participants were taking medications for opioid use disorder as noted above. Both of these factors could have had an unknown influence on the study results. Nonetheless, initial research on individuals with opioid use disorder who received or were receiving opioid use disorder medications has shown that both medication engagement and mutual-help participation are independently associated with opioid abstinence, which is consistent with the results found here.
Black men, Black women, and Hispanic women benefited more from mutual-help attendance than their respective White counterparts, and mutual-help attendance was equally beneficial among American Indian/Alaskan Native, Asian/Pacific Islander, and White women. Other research shows racial/ethnic disparities in substance use treatment completion are largely explained by socioeconomic factors that indicate that different racial/ethnic groups face different levels of barriers influencing the likelihood of successfully finishing a particular phase of treatment. Logistical barriers to treatment completion, for example, such as difficulties with finding treatment, paying or qualifying for treatment, obtaining transportation, and handling family and work responsibilities, may be somewhat mitigated for mutual-help group participation specifically because meetings are free and widely available (i.e., located in accessible community settings and online), and operate independently of governmental and professional healthcare institutions. Thus, marginalized people with more disadvantages and less access to recovery capital (potentially such as Black men, Black women, and Hispanic women in the current study) may benefit more from being able to flexibly use this free, community-based resource than individuals with greater structural advantages (such as White men and women in the current study) who are perhaps more able to access professional care.
Although Black men and women, and Hispanic women, showed greater benefits of mutual-help attendance in completing treatment relative to their White counterparts, Black men (28.7% completed treatment, 23.7% attended mutual help) and Black women (23.4% completed treatment, 20.8% attended mutual help) had the lowest treatment completion and mutual-help attendance rates.
The highest treatment completion and mutual-help attendance rates were among White individuals and men (White men 40.9%, White women 38.4%, Asian/PI men 39.2%, Hispanic men 37.5% completed treatment; White men 29.6%, White women 29.5%, Asian/PI men 29.0%, Hispanic men 28.1% attended mutual help).
In addition to logistical barriers, marginalized groups may experience cultural barriers to completing treatment, such as a lack of culturally adapted treatments, a lack of group representation among clients and staff, and potential experiences of discrimination. Similar cultural barriers may exist for participating in mutual-help groups, such as a lack of representation of a person’s marginalized identity within a given mutual help group’s founding, history, membership, and/or leadership; mismatch between a given mutual help group’s philosophy, values, or practices with a person’s own culture; or a person experiencing heightened scrutiny, prejudice, and discrimination within a given mutual-help group.
However, given the higher rates of treatment completion and mutual-help attendance among Whites relative to Black participants, the greater benefits of mutual-help attendance for Black men and women could be a statistical artifact – meaning they had more room to benefit from mutual-help attendance when compared White participants. More research is needed to clarify this.
The measure of mutual-help attendance in the current study lacked details about the type of mutual help groups attended and frequency participants attended, which limits some of what we can interpret from the study results. Mutual-help attendance was defined by a ‘yes’/’no’ response to the question: “Did the participant participate in self-help groups in the 30 days prior to discharge?” This provides no information about what kinds of mutual-help groups participants attended, how many times a participant attended mutual-help meetings over the course of treatment, or how involved they were in a particular group. Research suggests that being actively involved (e.g., having a sponsor) in mutual-help is a stronger predictor of beneficial outcomes versus attendance alone, which cannot be disentangled from attendance in the current study. However, it may be a reasonable assumption that participants who were categorized into the mutual-help participation group were probably more than one-time attendees assuming treatment providers would be unlikely to indicate ‘yes’ if a patient had only attended mutual-help once in the 30 days prior to treatment completion. Although, ultimately we do not know.
All measures in the current study were likely derived from clinic administrative reporting, meaning data could be reported by clinic administrative staff or treatment providers, but not the participants themselves. Reports of clinic data could be susceptible to bias from treatment providers or may not necessarily reflect how participants view themselves or their experience in treatment.
Participants categorized as Hispanic included individuals of all racial identities who indicated their ethnicity as Hispanic. Individuals in all other racial categories included individuals who indicated their ethnicity as non-Hispanic. While this is a strength in the study for participants who may identify with none of the racial categories typically provided on e.g., U.S. census survey, this creates a limitation for Afrolatinx/e individuals who are Black and Hispanic. Afrolatinx individuals may experience differing mutual-help attendance and treatment completion rates than a White Hispanic person, or a Hispanic person who identifies with neither Black or White race, but this cannot be ascertained in the current study.
BOTTOM LINE
In a sample of almost 200,000 adults in outpatient opioid use treatment from 2015-2017, mutual-help attendance in the 30-days prior to discharge was associated with greater treatment completion rates across racial/ethnic and sex groups. Among men, Black men appeared to benefit the most from mutual-help group participation in terms of completing treatment compared to men of other races/ethnicities. Among women, Black women and Hispanic women benefitted more from mutual-help attendance than White women and American Indian/Alaskan Native women.
For individuals and families seeking recovery: Placing these findings in context with other studies, contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups may be a cost-effective way build social support for racially/ethnically diverse men and women and help them maintain abstinence from various substances. Participating in mutual-help groups may help individuals in outpatient treatment for opioid use achieve their treatment goals. Mutual-help may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital.
For treatment professionals and treatment systems: Placing these findings in context with other studies, contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups are a cost-effective way build social support for racially/ethnically diverse men and women and maintain abstinence from various substances. Participating in mutual-help groups may help individuals in outpatient treatment for opioid use achieve their treatment goals. Mutual-help participation may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital. Encouraging patients to try mutual-help towards the end of outpatient opioid treatment may assist in treatment completion.
For scientists: Findings from this dataset (N = 199,779) from the 2015–2017 SAMHSA Treatment Episode Dataset–Discharge (TEDS-D) suggest that participating in mutual-help in the 30 days prior to discharge from outpatient or intensive outpatient treatment for opioid use is associated with greater treatment completion rates. Controlling for the interaction of race/ethnicity and sex, there was a significant main effect for mutual-help participation on treatment completion, such that mutual-help participation was associated with 4.5 times greater odds of completing treatment compared to no mutual-help participation in the 30 days prior to discharge. Black men, Black women, and Hispanic women showed a stronger relative association between mutual-help attendance and treatment completion compared to other racial/ethnic groups. Compared to White men, the association between mutual-help participation and treatment completion was about 50% stronger for Black men. Compared to American Indian/Alaskan Native women, the association between mutual-help participation and treatment completion was 47% stronger for Black women. The highest rates of treatment completion and mutual-help attendance were among White men and women; thus, it is unclear if the greater benefits observed for Black men and women were a statistical artifact of having more room to benefit, or a real mutual-help benefit based on potential differences in structural advantages and recovery capital between Black participants and other racial/ethnic groups. Future research should measure the frequency, quality, and intensity of mutual-help group participation for individuals in treatment for opioid use to disentangle these benefits.
For policy makers: Contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups may be a cost-effective way to support treatment goals and build social support for racially/ethnically diverse men and women and maintain abstinence from various substances. Mutual-help may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital. Continued funding for research examining community-based recovery supports would help to disentangle racial/ethnic and sex disparities in substance use treatment and support clinical practice and public health guidelines to reduce inequities.
Whereas mutual-help participation has been looked at to some degree in populations with opioid use disorder little research has examined the impact of so called “intersectionality” on mutual-help participation (i.e., the intersection of demographic variables like race/ethnicity, sex/gender, age and so on with mutual-help participation and benefits) and treatment, despite documented disparities in substance use treatment completion among Black, Latinx, and Indigenous populations when compared to White groups in the U.S. There are some people who believe that 12-step meetings cater only to White, middle-class men, raising concerns about potential racial/ethnic and/or sex disparities in mutual-help participation.
A prior review of 19 studies, however, showed weak evidence for differences. Most studies in the review showed no racial/ethnic differences in mutual-help attendance, with some evidence weekly suggestive of disparities for Latinx immigrants, women, and adolescents, as well as Black women and adolescents. The review concluded that overall, studies were “dated” and “inconsistent”, highlighting the need for additional research in this area.
This study sought to help further our understanding of the role mutual-help group participation can play in opioid use disorder treatment and whether such benefits are equitable across specific gender and racial/ethnic groups.
HOW WAS THIS STUDY CONDUCTED?
The researchers used a large publicly available SAMHSA data set to examine nearly 200,000 adults (N = 199,779) in outpatient or intensive outpatient opioid use treatment from 2015-2017 and their treatment completion outcomes. Participants’ clinical data upon discharge were used to examine the association between mutual-help participation in the 30 days prior to discharge and treatment completion status, as well as to examine group differences by race/ethnicity and sex.
Participants were included in this study if they were adults (18 years of age or older), participated in at least 30 days of outpatient or intensive outpatient treatment (IOP), and their reported primary substance upon admission was opioids. Participants were excluded if they were in another type of substance use treatment (e.g., residential), were in treatment for fewer than 30 days, or their reported primary substance was something other than opioids. Because the researchers were interested in the specific role of mutual-help groups in the community (as opposed to mutual help group participation within a residential treatment setting), the study only included participants in outpatient treatment or intensive outpatient treatment who had no record of prior treatment episodes. Participants who had missing responses for variables of interest were also excluded from the study.
Large publicly available data sets, like the SAMSHA data set used in the current study, often heavily rely on reports of clinic administrative data, meaning, data may be entered by treatment staff or providers, rather than asking patients directly. In the current study, to assess self-help participation, the study asked, “Did the participant participate in self-help groups in the 30 days prior to discharge?” Response options were: treatment completed, dropped out of treatment, terminated by facility, transferred to another treatment program or facility, incarcerated, death, or other. The researchers then grouped participants into “successful” (i.e., treatment completed) or “unsuccessful” (i.e., dropped out of treatment or terminated by facility) treatment completion groups. Participants with discharge statuses of a) transferred to another treatment program or facility, b) incarcerated, c) death, or d) other were excluded from this study.
The researchers used reports of participants’ race, ethnicity, and sex in the data to create 10 groups: American Indian/Alaska Native (AI/ AN) men, AI/AN women, Asian/Pacific Islander (PI) men, Asian/PI women, Black men, Black women, Hispanic men, Hispanic women, White men, and White women. Hispanic men and women included individuals of all racial identities who indicated their ethnicity as Hispanic. Individuals in all other racial categories include individuals who indicated their ethnicity as non-Hispanic.
First, the researchers tested the association between mutual-help participation and treatment completion by race/ethnicity, while controlling for participants’ education, length of stay in treatment, employment status at discharge, and age at admission, to see if a) the effect of mutual-help participation was associated independently with greater rates of treatment completion, and b) if this effect differed by race/ethnicity. In the second analysis, the researchers examined differences in the association between mutual-help participation and treatment completion by race/ethnicity and sex, while controlling for the same demographic and clinical factors. This kind of analysis is intended to help clarify if there are specific differences in the effect of mutual-help participation on treatment completion for, say, American Indian/Alaskan Native women compared to another specific group, like, Hispanic men, while accounting for other differences that could affect treatment completion (i.e., education, length of stay in treatment, employment status at discharge, and age at admission).
Participants in this study were mostly White, with White women accounting for 33.2% of the sample and White men accounting for 43.4% of the sample. Fewer participants were Black men (7.9%), Black women (4.3%), Hispanic men (4.9%), and Hispanic women (2.8%). American
Indian/Alaskan Native (AI/AN) and Asian/Pacific Islander (PI) men and women each accounted for less than 1% of the sample, respectively. The sample was mostly younger to middle aged, with 65% falling between ages 25-44. Almost half of the sample had completed high school (48.4%), and only 36% were employed (part or full-time) at time of discharge from treatment. Participants’ length of stay in treatment varied from 30 days to more than 1 year.
A majority of these patients with primary opioid use disorder did not participate in any mutual-help (self-help) (71.4%) and did not “successfully” complete treatment (i.e., dropped out of treatment or treatment was terminated by the facility, 62.4%). Although still quite low, the highest rates of treatment completion were among White men (40.9%), Asian/PI men (39.2%), White women (38.4%), and Hispanic men (37.5%), followed by Hispanic women (34.3%) and Asian/PI women (33.6%). The lowest treatment completion rates were among AI/AN men (31.2%), Black men (28.7%), AI/AN women (27.1%), and Black women (23.4%).
The highest rates of mutual-help group attendance were among White men (29.6%), White women (29.5%), Asian/PI men (29.0%), Hispanic men (28.1%), and AI/AN women (27.4%), followed by Hispanic women (26.3%), Asian/PI women (26.1%), and AI/AN men (25.6%). The lowest rates of mutual-help group attendance were among Black men (23.7%) and Black women (20.8%).
WHAT DID THIS STUDY FIND?
Mutual-help attendance overall was associated with treatment completion.
Controlling for the interaction of race/ethnicity, sex, and mutual-help participation, mutual-help participation was independently associated with treatment completion, with those who attended mutual-help meetings having 4.5 times greater odds of completing treatment compared to no mutual-help meeting participation in the 30 days prior to discharge, while controlling for demographic and clinical characteristics.
Black men and Black women benefitted more from mutual-help participation than other groups.
Despite the lower mutual-help participation among Black men and women, Black men showed the largest positive association between mutual-help group participation and treatment completion compared to men of other races/ethnicities. The largest difference was between Black men and White men. Compared to White men, the association between mutual-help participation and treatment completion was about 50% stronger for Black men. In other words, there was a larger difference in treatment completion rates between Black men who did and Black men who did not attend mutual-help prior to treatment discharge, than between White men who did and did not attend mutual-help prior to treatment discharge. However, White men had higher rates of treatment completion, overall, irrespective of mutual-help attendance.
Similarly, among women, Black women as well as Hispanic women benefitted more from mutual-help participation than White women and American Indian/Alaskan Native women. The largest difference was between Black women and American Indian/Alaskan Native women. Compared to American Indian/Alaskan Native women, the association between mutual-help participation and treatment completion was 47% stronger for Black women. There were no differences in the benefits of attending mutual-help on treatment completion outcomes between White, American Indian/Alaskan Native, and Asian/Pacific Islander women.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For all racial, ethnic, and sex groups in this study, the study participants – comprised of outpatients with primary opioid use disorder – were more likely to complete treatment if they had attended mutual-help in the 30 days prior to discharge compared to participants who did not attend. From the current study, it cannot be concluded if greater mutual-help participation played a causative role in helping people to complete their treatment. It might be the case that that these individuals simply were more motivated to change thus were looking wherever they could to find support including from mutual-help organizations as well as treatment. There is good evidence however, that while this might be true, there is also a causative role in mutual-help participation improving treatment adherence and improving outcomes. Mutual-help attendance may well provide support and resources for individuals in opioid use treatment to help them reach their treatment goals. This is consistent with a body of literature that shows Alcoholics Anonymous produces comparable rates of alcohol abstinence to first line clinical treatments, and higher levels of 12-step involvement is associated with greater abstinence for individuals with other drug use problems. This may be somewhat surprising given reports of negative attitudes in 12-step towards individuals taking medications for opioid use disorder, including refusals to sponsor (act as a recovery mentor) people utilizing opioid use disorder medications. That said, the researchers of this study did not report the degree of opioid use disorder medication usage that might have influenced such participation. Mutual-help groups other than 12-step-based ones exist (e.g., SMART Recovery, Women for Sobriety, Recovery Dharma). Even within 12-step, all groups are autonomous and may have differing norms, customs, and attitudes regarding medication. This variety means that some individual mutual-help meetings may have more positive attitudes towards opioid use disorder medications than others. The researchers may not have had access to information about the types of mutual-help groups participants attended and did not report if participants were taking medications for opioid use disorder as noted above. Both of these factors could have had an unknown influence on the study results. Nonetheless, initial research on individuals with opioid use disorder who received or were receiving opioid use disorder medications has shown that both medication engagement and mutual-help participation are independently associated with opioid abstinence, which is consistent with the results found here.
Black men, Black women, and Hispanic women benefited more from mutual-help attendance than their respective White counterparts, and mutual-help attendance was equally beneficial among American Indian/Alaskan Native, Asian/Pacific Islander, and White women. Other research shows racial/ethnic disparities in substance use treatment completion are largely explained by socioeconomic factors that indicate that different racial/ethnic groups face different levels of barriers influencing the likelihood of successfully finishing a particular phase of treatment. Logistical barriers to treatment completion, for example, such as difficulties with finding treatment, paying or qualifying for treatment, obtaining transportation, and handling family and work responsibilities, may be somewhat mitigated for mutual-help group participation specifically because meetings are free and widely available (i.e., located in accessible community settings and online), and operate independently of governmental and professional healthcare institutions. Thus, marginalized people with more disadvantages and less access to recovery capital (potentially such as Black men, Black women, and Hispanic women in the current study) may benefit more from being able to flexibly use this free, community-based resource than individuals with greater structural advantages (such as White men and women in the current study) who are perhaps more able to access professional care.
Although Black men and women, and Hispanic women, showed greater benefits of mutual-help attendance in completing treatment relative to their White counterparts, Black men (28.7% completed treatment, 23.7% attended mutual help) and Black women (23.4% completed treatment, 20.8% attended mutual help) had the lowest treatment completion and mutual-help attendance rates.
The highest treatment completion and mutual-help attendance rates were among White individuals and men (White men 40.9%, White women 38.4%, Asian/PI men 39.2%, Hispanic men 37.5% completed treatment; White men 29.6%, White women 29.5%, Asian/PI men 29.0%, Hispanic men 28.1% attended mutual help).
In addition to logistical barriers, marginalized groups may experience cultural barriers to completing treatment, such as a lack of culturally adapted treatments, a lack of group representation among clients and staff, and potential experiences of discrimination. Similar cultural barriers may exist for participating in mutual-help groups, such as a lack of representation of a person’s marginalized identity within a given mutual help group’s founding, history, membership, and/or leadership; mismatch between a given mutual help group’s philosophy, values, or practices with a person’s own culture; or a person experiencing heightened scrutiny, prejudice, and discrimination within a given mutual-help group.
However, given the higher rates of treatment completion and mutual-help attendance among Whites relative to Black participants, the greater benefits of mutual-help attendance for Black men and women could be a statistical artifact – meaning they had more room to benefit from mutual-help attendance when compared White participants. More research is needed to clarify this.
The measure of mutual-help attendance in the current study lacked details about the type of mutual help groups attended and frequency participants attended, which limits some of what we can interpret from the study results. Mutual-help attendance was defined by a ‘yes’/’no’ response to the question: “Did the participant participate in self-help groups in the 30 days prior to discharge?” This provides no information about what kinds of mutual-help groups participants attended, how many times a participant attended mutual-help meetings over the course of treatment, or how involved they were in a particular group. Research suggests that being actively involved (e.g., having a sponsor) in mutual-help is a stronger predictor of beneficial outcomes versus attendance alone, which cannot be disentangled from attendance in the current study. However, it may be a reasonable assumption that participants who were categorized into the mutual-help participation group were probably more than one-time attendees assuming treatment providers would be unlikely to indicate ‘yes’ if a patient had only attended mutual-help once in the 30 days prior to treatment completion. Although, ultimately we do not know.
All measures in the current study were likely derived from clinic administrative reporting, meaning data could be reported by clinic administrative staff or treatment providers, but not the participants themselves. Reports of clinic data could be susceptible to bias from treatment providers or may not necessarily reflect how participants view themselves or their experience in treatment.
Participants categorized as Hispanic included individuals of all racial identities who indicated their ethnicity as Hispanic. Individuals in all other racial categories included individuals who indicated their ethnicity as non-Hispanic. While this is a strength in the study for participants who may identify with none of the racial categories typically provided on e.g., U.S. census survey, this creates a limitation for Afrolatinx/e individuals who are Black and Hispanic. Afrolatinx individuals may experience differing mutual-help attendance and treatment completion rates than a White Hispanic person, or a Hispanic person who identifies with neither Black or White race, but this cannot be ascertained in the current study.
BOTTOM LINE
In a sample of almost 200,000 adults in outpatient opioid use treatment from 2015-2017, mutual-help attendance in the 30-days prior to discharge was associated with greater treatment completion rates across racial/ethnic and sex groups. Among men, Black men appeared to benefit the most from mutual-help group participation in terms of completing treatment compared to men of other races/ethnicities. Among women, Black women and Hispanic women benefitted more from mutual-help attendance than White women and American Indian/Alaskan Native women.
For individuals and families seeking recovery: Placing these findings in context with other studies, contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups may be a cost-effective way build social support for racially/ethnically diverse men and women and help them maintain abstinence from various substances. Participating in mutual-help groups may help individuals in outpatient treatment for opioid use achieve their treatment goals. Mutual-help may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital.
For treatment professionals and treatment systems: Placing these findings in context with other studies, contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups are a cost-effective way build social support for racially/ethnically diverse men and women and maintain abstinence from various substances. Participating in mutual-help groups may help individuals in outpatient treatment for opioid use achieve their treatment goals. Mutual-help participation may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital. Encouraging patients to try mutual-help towards the end of outpatient opioid treatment may assist in treatment completion.
For scientists: Findings from this dataset (N = 199,779) from the 2015–2017 SAMHSA Treatment Episode Dataset–Discharge (TEDS-D) suggest that participating in mutual-help in the 30 days prior to discharge from outpatient or intensive outpatient treatment for opioid use is associated with greater treatment completion rates. Controlling for the interaction of race/ethnicity and sex, there was a significant main effect for mutual-help participation on treatment completion, such that mutual-help participation was associated with 4.5 times greater odds of completing treatment compared to no mutual-help participation in the 30 days prior to discharge. Black men, Black women, and Hispanic women showed a stronger relative association between mutual-help attendance and treatment completion compared to other racial/ethnic groups. Compared to White men, the association between mutual-help participation and treatment completion was about 50% stronger for Black men. Compared to American Indian/Alaskan Native women, the association between mutual-help participation and treatment completion was 47% stronger for Black women. The highest rates of treatment completion and mutual-help attendance were among White men and women; thus, it is unclear if the greater benefits observed for Black men and women were a statistical artifact of having more room to benefit, or a real mutual-help benefit based on potential differences in structural advantages and recovery capital between Black participants and other racial/ethnic groups. Future research should measure the frequency, quality, and intensity of mutual-help group participation for individuals in treatment for opioid use to disentangle these benefits.
For policy makers: Contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups may be a cost-effective way to support treatment goals and build social support for racially/ethnically diverse men and women and maintain abstinence from various substances. Mutual-help may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital. Continued funding for research examining community-based recovery supports would help to disentangle racial/ethnic and sex disparities in substance use treatment and support clinical practice and public health guidelines to reduce inequities.
Whereas mutual-help participation has been looked at to some degree in populations with opioid use disorder little research has examined the impact of so called “intersectionality” on mutual-help participation (i.e., the intersection of demographic variables like race/ethnicity, sex/gender, age and so on with mutual-help participation and benefits) and treatment, despite documented disparities in substance use treatment completion among Black, Latinx, and Indigenous populations when compared to White groups in the U.S. There are some people who believe that 12-step meetings cater only to White, middle-class men, raising concerns about potential racial/ethnic and/or sex disparities in mutual-help participation.
A prior review of 19 studies, however, showed weak evidence for differences. Most studies in the review showed no racial/ethnic differences in mutual-help attendance, with some evidence weekly suggestive of disparities for Latinx immigrants, women, and adolescents, as well as Black women and adolescents. The review concluded that overall, studies were “dated” and “inconsistent”, highlighting the need for additional research in this area.
This study sought to help further our understanding of the role mutual-help group participation can play in opioid use disorder treatment and whether such benefits are equitable across specific gender and racial/ethnic groups.
HOW WAS THIS STUDY CONDUCTED?
The researchers used a large publicly available SAMHSA data set to examine nearly 200,000 adults (N = 199,779) in outpatient or intensive outpatient opioid use treatment from 2015-2017 and their treatment completion outcomes. Participants’ clinical data upon discharge were used to examine the association between mutual-help participation in the 30 days prior to discharge and treatment completion status, as well as to examine group differences by race/ethnicity and sex.
Participants were included in this study if they were adults (18 years of age or older), participated in at least 30 days of outpatient or intensive outpatient treatment (IOP), and their reported primary substance upon admission was opioids. Participants were excluded if they were in another type of substance use treatment (e.g., residential), were in treatment for fewer than 30 days, or their reported primary substance was something other than opioids. Because the researchers were interested in the specific role of mutual-help groups in the community (as opposed to mutual help group participation within a residential treatment setting), the study only included participants in outpatient treatment or intensive outpatient treatment who had no record of prior treatment episodes. Participants who had missing responses for variables of interest were also excluded from the study.
Large publicly available data sets, like the SAMSHA data set used in the current study, often heavily rely on reports of clinic administrative data, meaning, data may be entered by treatment staff or providers, rather than asking patients directly. In the current study, to assess self-help participation, the study asked, “Did the participant participate in self-help groups in the 30 days prior to discharge?” Response options were: treatment completed, dropped out of treatment, terminated by facility, transferred to another treatment program or facility, incarcerated, death, or other. The researchers then grouped participants into “successful” (i.e., treatment completed) or “unsuccessful” (i.e., dropped out of treatment or terminated by facility) treatment completion groups. Participants with discharge statuses of a) transferred to another treatment program or facility, b) incarcerated, c) death, or d) other were excluded from this study.
The researchers used reports of participants’ race, ethnicity, and sex in the data to create 10 groups: American Indian/Alaska Native (AI/ AN) men, AI/AN women, Asian/Pacific Islander (PI) men, Asian/PI women, Black men, Black women, Hispanic men, Hispanic women, White men, and White women. Hispanic men and women included individuals of all racial identities who indicated their ethnicity as Hispanic. Individuals in all other racial categories include individuals who indicated their ethnicity as non-Hispanic.
First, the researchers tested the association between mutual-help participation and treatment completion by race/ethnicity, while controlling for participants’ education, length of stay in treatment, employment status at discharge, and age at admission, to see if a) the effect of mutual-help participation was associated independently with greater rates of treatment completion, and b) if this effect differed by race/ethnicity. In the second analysis, the researchers examined differences in the association between mutual-help participation and treatment completion by race/ethnicity and sex, while controlling for the same demographic and clinical factors. This kind of analysis is intended to help clarify if there are specific differences in the effect of mutual-help participation on treatment completion for, say, American Indian/Alaskan Native women compared to another specific group, like, Hispanic men, while accounting for other differences that could affect treatment completion (i.e., education, length of stay in treatment, employment status at discharge, and age at admission).
Participants in this study were mostly White, with White women accounting for 33.2% of the sample and White men accounting for 43.4% of the sample. Fewer participants were Black men (7.9%), Black women (4.3%), Hispanic men (4.9%), and Hispanic women (2.8%). American
Indian/Alaskan Native (AI/AN) and Asian/Pacific Islander (PI) men and women each accounted for less than 1% of the sample, respectively. The sample was mostly younger to middle aged, with 65% falling between ages 25-44. Almost half of the sample had completed high school (48.4%), and only 36% were employed (part or full-time) at time of discharge from treatment. Participants’ length of stay in treatment varied from 30 days to more than 1 year.
A majority of these patients with primary opioid use disorder did not participate in any mutual-help (self-help) (71.4%) and did not “successfully” complete treatment (i.e., dropped out of treatment or treatment was terminated by the facility, 62.4%). Although still quite low, the highest rates of treatment completion were among White men (40.9%), Asian/PI men (39.2%), White women (38.4%), and Hispanic men (37.5%), followed by Hispanic women (34.3%) and Asian/PI women (33.6%). The lowest treatment completion rates were among AI/AN men (31.2%), Black men (28.7%), AI/AN women (27.1%), and Black women (23.4%).
The highest rates of mutual-help group attendance were among White men (29.6%), White women (29.5%), Asian/PI men (29.0%), Hispanic men (28.1%), and AI/AN women (27.4%), followed by Hispanic women (26.3%), Asian/PI women (26.1%), and AI/AN men (25.6%). The lowest rates of mutual-help group attendance were among Black men (23.7%) and Black women (20.8%).
WHAT DID THIS STUDY FIND?
Mutual-help attendance overall was associated with treatment completion.
Controlling for the interaction of race/ethnicity, sex, and mutual-help participation, mutual-help participation was independently associated with treatment completion, with those who attended mutual-help meetings having 4.5 times greater odds of completing treatment compared to no mutual-help meeting participation in the 30 days prior to discharge, while controlling for demographic and clinical characteristics.
Black men and Black women benefitted more from mutual-help participation than other groups.
Despite the lower mutual-help participation among Black men and women, Black men showed the largest positive association between mutual-help group participation and treatment completion compared to men of other races/ethnicities. The largest difference was between Black men and White men. Compared to White men, the association between mutual-help participation and treatment completion was about 50% stronger for Black men. In other words, there was a larger difference in treatment completion rates between Black men who did and Black men who did not attend mutual-help prior to treatment discharge, than between White men who did and did not attend mutual-help prior to treatment discharge. However, White men had higher rates of treatment completion, overall, irrespective of mutual-help attendance.
Similarly, among women, Black women as well as Hispanic women benefitted more from mutual-help participation than White women and American Indian/Alaskan Native women. The largest difference was between Black women and American Indian/Alaskan Native women. Compared to American Indian/Alaskan Native women, the association between mutual-help participation and treatment completion was 47% stronger for Black women. There were no differences in the benefits of attending mutual-help on treatment completion outcomes between White, American Indian/Alaskan Native, and Asian/Pacific Islander women.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
For all racial, ethnic, and sex groups in this study, the study participants – comprised of outpatients with primary opioid use disorder – were more likely to complete treatment if they had attended mutual-help in the 30 days prior to discharge compared to participants who did not attend. From the current study, it cannot be concluded if greater mutual-help participation played a causative role in helping people to complete their treatment. It might be the case that that these individuals simply were more motivated to change thus were looking wherever they could to find support including from mutual-help organizations as well as treatment. There is good evidence however, that while this might be true, there is also a causative role in mutual-help participation improving treatment adherence and improving outcomes. Mutual-help attendance may well provide support and resources for individuals in opioid use treatment to help them reach their treatment goals. This is consistent with a body of literature that shows Alcoholics Anonymous produces comparable rates of alcohol abstinence to first line clinical treatments, and higher levels of 12-step involvement is associated with greater abstinence for individuals with other drug use problems. This may be somewhat surprising given reports of negative attitudes in 12-step towards individuals taking medications for opioid use disorder, including refusals to sponsor (act as a recovery mentor) people utilizing opioid use disorder medications. That said, the researchers of this study did not report the degree of opioid use disorder medication usage that might have influenced such participation. Mutual-help groups other than 12-step-based ones exist (e.g., SMART Recovery, Women for Sobriety, Recovery Dharma). Even within 12-step, all groups are autonomous and may have differing norms, customs, and attitudes regarding medication. This variety means that some individual mutual-help meetings may have more positive attitudes towards opioid use disorder medications than others. The researchers may not have had access to information about the types of mutual-help groups participants attended and did not report if participants were taking medications for opioid use disorder as noted above. Both of these factors could have had an unknown influence on the study results. Nonetheless, initial research on individuals with opioid use disorder who received or were receiving opioid use disorder medications has shown that both medication engagement and mutual-help participation are independently associated with opioid abstinence, which is consistent with the results found here.
Black men, Black women, and Hispanic women benefited more from mutual-help attendance than their respective White counterparts, and mutual-help attendance was equally beneficial among American Indian/Alaskan Native, Asian/Pacific Islander, and White women. Other research shows racial/ethnic disparities in substance use treatment completion are largely explained by socioeconomic factors that indicate that different racial/ethnic groups face different levels of barriers influencing the likelihood of successfully finishing a particular phase of treatment. Logistical barriers to treatment completion, for example, such as difficulties with finding treatment, paying or qualifying for treatment, obtaining transportation, and handling family and work responsibilities, may be somewhat mitigated for mutual-help group participation specifically because meetings are free and widely available (i.e., located in accessible community settings and online), and operate independently of governmental and professional healthcare institutions. Thus, marginalized people with more disadvantages and less access to recovery capital (potentially such as Black men, Black women, and Hispanic women in the current study) may benefit more from being able to flexibly use this free, community-based resource than individuals with greater structural advantages (such as White men and women in the current study) who are perhaps more able to access professional care.
Although Black men and women, and Hispanic women, showed greater benefits of mutual-help attendance in completing treatment relative to their White counterparts, Black men (28.7% completed treatment, 23.7% attended mutual help) and Black women (23.4% completed treatment, 20.8% attended mutual help) had the lowest treatment completion and mutual-help attendance rates.
The highest treatment completion and mutual-help attendance rates were among White individuals and men (White men 40.9%, White women 38.4%, Asian/PI men 39.2%, Hispanic men 37.5% completed treatment; White men 29.6%, White women 29.5%, Asian/PI men 29.0%, Hispanic men 28.1% attended mutual help).
In addition to logistical barriers, marginalized groups may experience cultural barriers to completing treatment, such as a lack of culturally adapted treatments, a lack of group representation among clients and staff, and potential experiences of discrimination. Similar cultural barriers may exist for participating in mutual-help groups, such as a lack of representation of a person’s marginalized identity within a given mutual help group’s founding, history, membership, and/or leadership; mismatch between a given mutual help group’s philosophy, values, or practices with a person’s own culture; or a person experiencing heightened scrutiny, prejudice, and discrimination within a given mutual-help group.
However, given the higher rates of treatment completion and mutual-help attendance among Whites relative to Black participants, the greater benefits of mutual-help attendance for Black men and women could be a statistical artifact – meaning they had more room to benefit from mutual-help attendance when compared White participants. More research is needed to clarify this.
The measure of mutual-help attendance in the current study lacked details about the type of mutual help groups attended and frequency participants attended, which limits some of what we can interpret from the study results. Mutual-help attendance was defined by a ‘yes’/’no’ response to the question: “Did the participant participate in self-help groups in the 30 days prior to discharge?” This provides no information about what kinds of mutual-help groups participants attended, how many times a participant attended mutual-help meetings over the course of treatment, or how involved they were in a particular group. Research suggests that being actively involved (e.g., having a sponsor) in mutual-help is a stronger predictor of beneficial outcomes versus attendance alone, which cannot be disentangled from attendance in the current study. However, it may be a reasonable assumption that participants who were categorized into the mutual-help participation group were probably more than one-time attendees assuming treatment providers would be unlikely to indicate ‘yes’ if a patient had only attended mutual-help once in the 30 days prior to treatment completion. Although, ultimately we do not know.
All measures in the current study were likely derived from clinic administrative reporting, meaning data could be reported by clinic administrative staff or treatment providers, but not the participants themselves. Reports of clinic data could be susceptible to bias from treatment providers or may not necessarily reflect how participants view themselves or their experience in treatment.
Participants categorized as Hispanic included individuals of all racial identities who indicated their ethnicity as Hispanic. Individuals in all other racial categories included individuals who indicated their ethnicity as non-Hispanic. While this is a strength in the study for participants who may identify with none of the racial categories typically provided on e.g., U.S. census survey, this creates a limitation for Afrolatinx/e individuals who are Black and Hispanic. Afrolatinx individuals may experience differing mutual-help attendance and treatment completion rates than a White Hispanic person, or a Hispanic person who identifies with neither Black or White race, but this cannot be ascertained in the current study.
BOTTOM LINE
In a sample of almost 200,000 adults in outpatient opioid use treatment from 2015-2017, mutual-help attendance in the 30-days prior to discharge was associated with greater treatment completion rates across racial/ethnic and sex groups. Among men, Black men appeared to benefit the most from mutual-help group participation in terms of completing treatment compared to men of other races/ethnicities. Among women, Black women and Hispanic women benefitted more from mutual-help attendance than White women and American Indian/Alaskan Native women.
For individuals and families seeking recovery: Placing these findings in context with other studies, contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups may be a cost-effective way build social support for racially/ethnically diverse men and women and help them maintain abstinence from various substances. Participating in mutual-help groups may help individuals in outpatient treatment for opioid use achieve their treatment goals. Mutual-help may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital.
For treatment professionals and treatment systems: Placing these findings in context with other studies, contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups are a cost-effective way build social support for racially/ethnically diverse men and women and maintain abstinence from various substances. Participating in mutual-help groups may help individuals in outpatient treatment for opioid use achieve their treatment goals. Mutual-help participation may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital. Encouraging patients to try mutual-help towards the end of outpatient opioid treatment may assist in treatment completion.
For scientists: Findings from this dataset (N = 199,779) from the 2015–2017 SAMHSA Treatment Episode Dataset–Discharge (TEDS-D) suggest that participating in mutual-help in the 30 days prior to discharge from outpatient or intensive outpatient treatment for opioid use is associated with greater treatment completion rates. Controlling for the interaction of race/ethnicity and sex, there was a significant main effect for mutual-help participation on treatment completion, such that mutual-help participation was associated with 4.5 times greater odds of completing treatment compared to no mutual-help participation in the 30 days prior to discharge. Black men, Black women, and Hispanic women showed a stronger relative association between mutual-help attendance and treatment completion compared to other racial/ethnic groups. Compared to White men, the association between mutual-help participation and treatment completion was about 50% stronger for Black men. Compared to American Indian/Alaskan Native women, the association between mutual-help participation and treatment completion was 47% stronger for Black women. The highest rates of treatment completion and mutual-help attendance were among White men and women; thus, it is unclear if the greater benefits observed for Black men and women were a statistical artifact of having more room to benefit, or a real mutual-help benefit based on potential differences in structural advantages and recovery capital between Black participants and other racial/ethnic groups. Future research should measure the frequency, quality, and intensity of mutual-help group participation for individuals in treatment for opioid use to disentangle these benefits.
For policy makers: Contrary to the idea that 12-step mutual-help organizations cater only to White, middle-class men with alcohol use disorder, mutual-help groups may be a cost-effective way to support treatment goals and build social support for racially/ethnically diverse men and women and maintain abstinence from various substances. Mutual-help may be especially beneficial for individuals experiencing greater economic barriers or disadvantages in building recovery capital. Continued funding for research examining community-based recovery supports would help to disentangle racial/ethnic and sex disparities in substance use treatment and support clinical practice and public health guidelines to reduce inequities.