In the US, AA and other 12-step groups are the longest running and most widely available mutual-help options, though beginning in the 1970s, other mutual-help organizations began to emerge. SMART Recovery, based on motivational and CBT strategies, is one of the most well-known. Some people with alcohol use disorder opt to use SMART, some use AA, some actually use both, and some use neither. This study investigated characteristics associated with these different recovery pathway choices.
For people with alcohol use disorder, mutual-help organizations have the highest rates of engagement across professional and non-professional services. Participation in the 12-step mutual-help organization, Alcoholics Anonymous (AA), produces benefits as large as other addiction-focused interventions while, on average, producing higher rates of sustained abstinence and remission over time. As a community-based organization, it is also very cost-effective, with estimated US-wide treatment cost reductions alone totaling $10 billion compared to other treatments (e.g., cognitive behavioral therapies, motivations enhancement therapies).
Over the last 50 years, there has been a rise in other mutual-help organizations such as Self-Management and Recovery Training or “SMART” Recovery (hereafter SMART). SMART is a mutual-help organization that integrates motivational and cognitive-behavioral clinical approaches, but adapted for a community-based setting. SMART meetings are led by a trained facilitator who may or may not have lived experience in recovery, which is different from most other mutual-help organizations which are entirely peer-led (e.g., AA). Another difference between SMART and most other mutual-help organizations is that SMART is open to anyone with any kind of substance use or behavioral addiction rather than alcohol and other drug use more specifically as is the case for the most popular 12-step groups. Other key differences between SMART and most other mutual-help organizations include an explicit omission of any spiritual or religious content in the approach (people with spiritual and religious backgrounds are welcome and encouraged to attend) and the lack of a social network or “fellowship” cultural norm. Many individuals go to 2 or more types of mutual-help organizations. Thus it is important also to understand how those who attend both SMART and AA might differ from those who attend only one or the other.
As evidence for SMART grows, it will be important to know who is most likely to be drawn to this recovery support option. The current study investigated who chooses to engage in SMART compared to AA, Both AA and SMART, or Neither.
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional analysis that compared 361 adult participants that self-selected into one of four recovery paths: SMART (20.8%), AA (20.2%), both (14.7%), or neither (44.3%). Participants had started a new alcohol use disorder recovery attempt in the past 90 days or were planning to start one in the next 14 days. Those who attended (or were planning to attend) SMART-only, AA-only, or both were categorized accordingly. A fourth group included those that had not attended either SMART or AA in the last 90 days and did not intend to in the subsequent 14 days. Participants were recruited between January 2019 and January 2022 as part of a larger 2-year prospective study of alcohol use disorder recovery pathways. They were recruited at SMART meetings, outpatient treatment, and several community recruitment sources (e.g., ResearchMatch, Facebook, Reddit, newspaper).
All participants reported a primary alcohol use problem, met DSM-5 alcohol use disorder criteria, and consumed alcohol in the past 90 days. They resided in either New England or San Diego. For the assessment, participants provided information spanning demographics, clinical outcomes, and other recovery-related variables. Of all 361 participants, just over half were female (52%) and almost three-quarters were White (74%). The average age was 46, and 36% were married, engaged, or living with partner as if married. Close to half were employed full-time (42%) and had completed a bachelor’s degree or higher (50%).
WHAT DID THIS STUDY FIND?
Demographics of SMART-only participants were different from AA-only participants
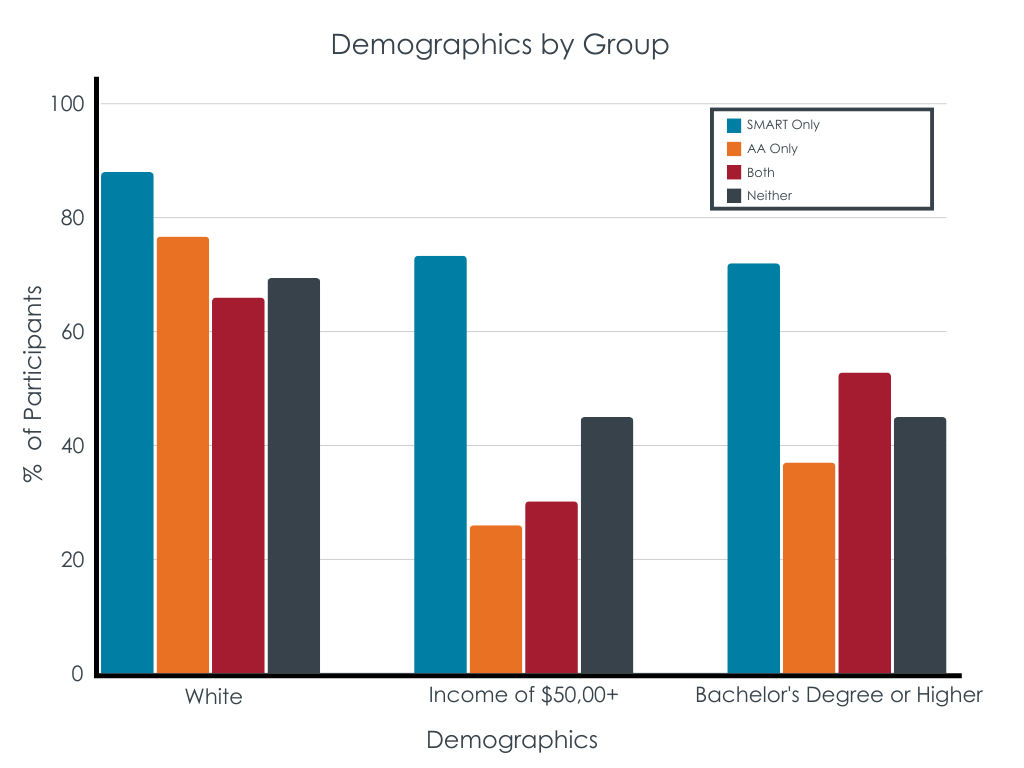
Compared to the AA-only, Both, and Neither groups, those in the SMART-only group were more likely to be White (88% versus 77% or less), to have higher incomes (73% with an annual income of $50,000 or more versus 45% or less), and to have higher levels of education (72% with a bachelor’s degree or higher versus 52% or less). Those in the SMART-only group were also more likely to be in a committed relationship (53% versus 36% or less). Other differences emerged that were more nuanced such as those in the SMART-only group were less likely to be female (40%) compared to participants in the Neither group (60%) but not the AA-only or Both groups.
Clinical characteristics of SMART participants were somewhat different from AA participants
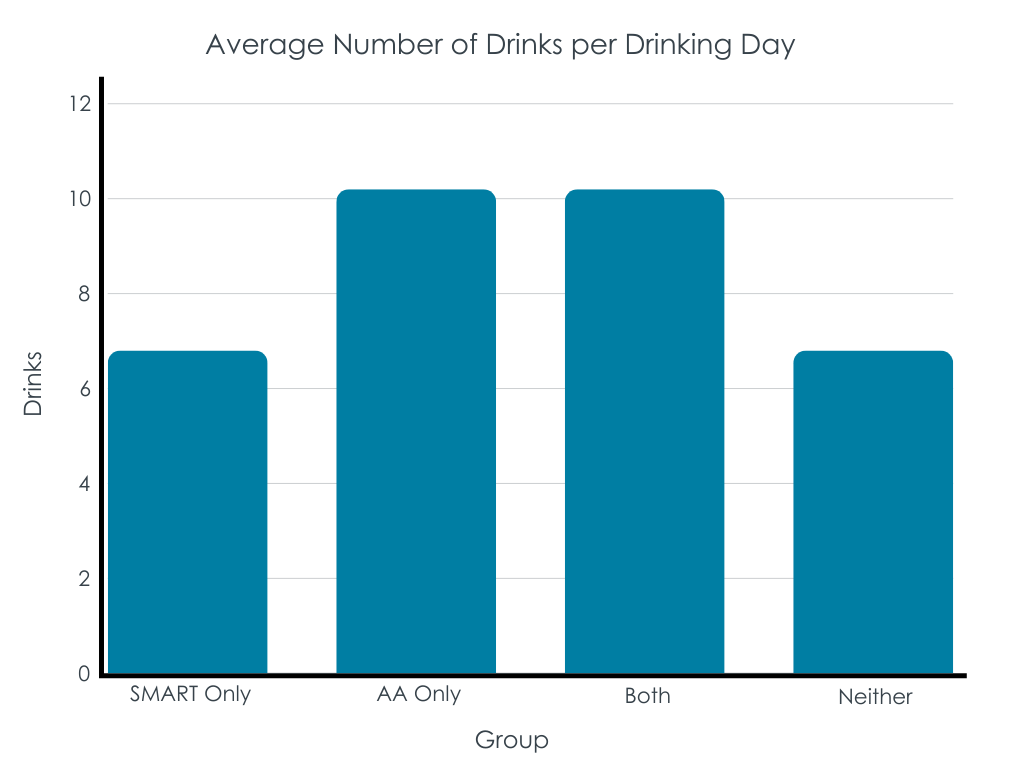
Individuals in the SMART-only group had similar alcohol use disorder severity compared to the AA-only and Both groups, but they had higher severity compared to the Neither group. Those in the SMART and Neither groups reported fewer drinks per drinking day in contrast to the AA-only and Both groups. The frequency of other substance use did not differ across the groups nor did the proportion of participations reporting a prior psychiatric diagnosis. Those in the SMART-only group were less likely to have a history of formal treatment compared to the AA and Both groups.
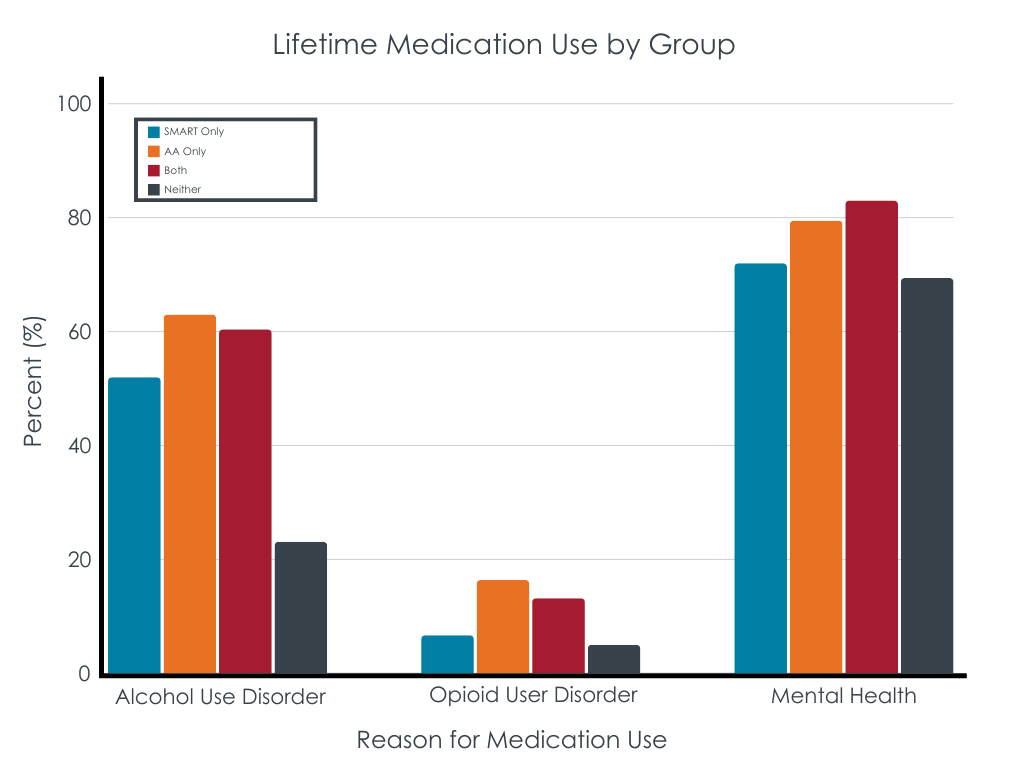
More than 52% of participants in the SMART-only, AA-only, and Both groups reported use of medications for alcohol use disorder in their lifetime, with no differences between these groups. Fewer participants in the Neither group (23%) reported medications for alcohol use disorder. Similarly, use of medications for opioid use disorder was low (9%) in all groups, yet medications for mental health problems was high across all groups (74%). Medication use for opioid use disorder and mental health problems did not differ across groups.
SMART participants were less likely than AA attendees to use other recovery support services
Individuals in the SMART-only group were less likely to report having lived in a recovery residence compared to the AA-only and Both groups. They were also less likely to have attended a recovery community center or recovery community organization. However, SMART and AA-only groups did not differ in their recovery capital, abstinence self-efficacy, or commitment to sobriety. Those choosing to attend neither SMART nor AA did report less recovery resource use. Those in the SMART and Neither groups were less likely than the AA and Both groups to have criminal justice involvement as well.
Nearly all participants had previous experience with the mutual-help organization they chose for this recovery attempt—98% of those attending AA had been previously and 91% of those attending SMART had done so previously. Those in SMART were less likely to have attended Narcotics Anonymous previously compared to those in the AA or Both groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Community-based recovery supports, such as mutual-help organizations (e.g., SMART) and recovery community organizations, are expanding. Apart from extensive research showing benefit from AA participation, there is little research on other mutual-help organizations to inform clinical recommendations. As new types of support and services like SMART continue to grow, clinicians and community members will benefit from knowing who is most likely to engage and to benefit from different types of support. This study finds that individuals with alcohol use disorder making a new recovery attempt that chose to attend SMART rather than AA, Both, or Neither were different across demographic, clinical, and recovery-related characteristics. Adults who engaged in SMART were more likely to be White, psychosocially stable, and economically advantaged. They also reported lower alcohol use intensity, less formal treatment and use of recovery support services, and fewer legal problems. These findings suggest that individuals starting a new recovery attempt with more initial recovery assets overall may find aspects of SMART more appealing compared to other mutual-help organizations (e.g., AA).
Furthermore, the findings suggest that SMART may fill a specific need for some. For example, many individuals chose to attend both SMART and AA, which may mean they provide unique but complementary offerings. For example, one possibility is that AA may better provide access to a recovery-supportive social network and help individuals develop recovery coping skills that leverage these social connections while SMART may help individuals develop recovery coping skills they can deploy on their own, independent of social support.
The study was cross-sectional; thus, no conclusions can be made about the effect of SMART compared to the other recovery pathways examined.
Recruitment for this study occurred in Boston, MA and San Diego, CA. Findings may be limited to these regions. Recruitment also occurred during COVID-19, which may have impacted participation in mutual-help organizations in unknown ways.
This study compared individuals choosing SMART, AA, both, or neither. Findings may differ across other mutual-help organizations (e.g., Narcotics Anonymous) or across an individual’s recovery journey. For example, someone may begin their recovery attempt attending AA but choose to switch and attend solely SMART later.
BOTTOM LINE
This cross-sectional study investigated demographic, clinical, and recovery-related characteristics among adults making a recovery attempt and choosing either to attend SMART-only, AA-only, both, or neither. The study found that those choosing to engage SMART-only were more likely to be White, psychosocially stable, economically advantaged, have less formal treatment and recovery support services use, and have fewer legal problems. The findings suggest that aspects of SMART may be appealing to adults with less intensive drinking, treatment, and legal histories, and who possess more initial recovery assets. Furthermore, differences also suggests that SMART fills an important niche in a recovery ecosystem, expanding the range of possible supports among those with alcohol and other drug problems. Future study is warranted to determine what unique benefits SMART confers and for whom.
For individuals and families seeking recovery: Adults choosing to engage SMART-only compared to AA-only, both, or neither were likely to be more affluent, White, have lower alcohol use intensity, and have less formal treatment and legal histories. If you or a loved one is making a new recovery attempt, mutual-help organizations like SMART and AA may be places to find support on your recovery journey. The best plan is likely to consist of sampling several meetings of each to see which one suits you the best, or you may end up utilizing both, capitalizing on the strengths of each.
For treatment professionals and treatment systems: Adults choosing to attend SMART-only compared to AA-only, both, or neither were more likely to be affluent, White, have lower alcohol use intensity, and have less formal treatment or legal involvement. Although this study was cross-sectional and cannot inform conclusions about the effects of these mutual-help organizations, it is likely beneficial to help individuals understand the menu of recovery supports available in the community and gives clues as to who may be best suited to try which particular options.
For scientists:Adults making a new recovery attempt and choosing to attend SMART-only compared to AA- only, both, or neither were more likely to be affluent, White, have lower alcohol use intensity, and have less formal treatment. However, the study cannot determine if the self-selected recovery path was beneficial for an individual or for those choosing that recovery pathway generally. Thus, future longitudinal studies that examine these recovery pathways over time will shed light on how well the different recovery pathways work for whom. Additionally, expanding recruitment to other regions may account for regional differences in mutual-help organization availability and culture.
For policy makers: SMART is one mutual-help organization that may have unique components that appeal to certain individuals—thus filling an important niche in the recovery ecosystem. Additional funding to facilitate SMART meetings as well as investigate its longtime effects would benefit adults seeking or in recovery from alcohol and other drug problems.
For people with alcohol use disorder, mutual-help organizations have the highest rates of engagement across professional and non-professional services. Participation in the 12-step mutual-help organization, Alcoholics Anonymous (AA), produces benefits as large as other addiction-focused interventions while, on average, producing higher rates of sustained abstinence and remission over time. As a community-based organization, it is also very cost-effective, with estimated US-wide treatment cost reductions alone totaling $10 billion compared to other treatments (e.g., cognitive behavioral therapies, motivations enhancement therapies).
Over the last 50 years, there has been a rise in other mutual-help organizations such as Self-Management and Recovery Training or “SMART” Recovery (hereafter SMART). SMART is a mutual-help organization that integrates motivational and cognitive-behavioral clinical approaches, but adapted for a community-based setting. SMART meetings are led by a trained facilitator who may or may not have lived experience in recovery, which is different from most other mutual-help organizations which are entirely peer-led (e.g., AA). Another difference between SMART and most other mutual-help organizations is that SMART is open to anyone with any kind of substance use or behavioral addiction rather than alcohol and other drug use more specifically as is the case for the most popular 12-step groups. Other key differences between SMART and most other mutual-help organizations include an explicit omission of any spiritual or religious content in the approach (people with spiritual and religious backgrounds are welcome and encouraged to attend) and the lack of a social network or “fellowship” cultural norm. Many individuals go to 2 or more types of mutual-help organizations. Thus it is important also to understand how those who attend both SMART and AA might differ from those who attend only one or the other.
As evidence for SMART grows, it will be important to know who is most likely to be drawn to this recovery support option. The current study investigated who chooses to engage in SMART compared to AA, Both AA and SMART, or Neither.
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional analysis that compared 361 adult participants that self-selected into one of four recovery paths: SMART (20.8%), AA (20.2%), both (14.7%), or neither (44.3%). Participants had started a new alcohol use disorder recovery attempt in the past 90 days or were planning to start one in the next 14 days. Those who attended (or were planning to attend) SMART-only, AA-only, or both were categorized accordingly. A fourth group included those that had not attended either SMART or AA in the last 90 days and did not intend to in the subsequent 14 days. Participants were recruited between January 2019 and January 2022 as part of a larger 2-year prospective study of alcohol use disorder recovery pathways. They were recruited at SMART meetings, outpatient treatment, and several community recruitment sources (e.g., ResearchMatch, Facebook, Reddit, newspaper).
All participants reported a primary alcohol use problem, met DSM-5 alcohol use disorder criteria, and consumed alcohol in the past 90 days. They resided in either New England or San Diego. For the assessment, participants provided information spanning demographics, clinical outcomes, and other recovery-related variables. Of all 361 participants, just over half were female (52%) and almost three-quarters were White (74%). The average age was 46, and 36% were married, engaged, or living with partner as if married. Close to half were employed full-time (42%) and had completed a bachelor’s degree or higher (50%).
WHAT DID THIS STUDY FIND?
Demographics of SMART-only participants were different from AA-only participants
Compared to the AA-only, Both, and Neither groups, those in the SMART-only group were more likely to be White (88% versus 77% or less), to have higher incomes (73% with an annual income of $50,000 or more versus 45% or less), and to have higher levels of education (72% with a bachelor’s degree or higher versus 52% or less). Those in the SMART-only group were also more likely to be in a committed relationship (53% versus 36% or less). Other differences emerged that were more nuanced such as those in the SMART-only group were less likely to be female (40%) compared to participants in the Neither group (60%) but not the AA-only or Both groups.
Clinical characteristics of SMART participants were somewhat different from AA participants
Individuals in the SMART-only group had similar alcohol use disorder severity compared to the AA-only and Both groups, but they had higher severity compared to the Neither group. Those in the SMART and Neither groups reported fewer drinks per drinking day in contrast to the AA-only and Both groups. The frequency of other substance use did not differ across the groups nor did the proportion of participations reporting a prior psychiatric diagnosis. Those in the SMART-only group were less likely to have a history of formal treatment compared to the AA and Both groups.
More than 52% of participants in the SMART-only, AA-only, and Both groups reported use of medications for alcohol use disorder in their lifetime, with no differences between these groups. Fewer participants in the Neither group (23%) reported medications for alcohol use disorder. Similarly, use of medications for opioid use disorder was low (9%) in all groups, yet medications for mental health problems was high across all groups (74%). Medication use for opioid use disorder and mental health problems did not differ across groups.
SMART participants were less likely than AA attendees to use other recovery support services
Individuals in the SMART-only group were less likely to report having lived in a recovery residence compared to the AA-only and Both groups. They were also less likely to have attended a recovery community center or recovery community organization. However, SMART and AA-only groups did not differ in their recovery capital, abstinence self-efficacy, or commitment to sobriety. Those choosing to attend neither SMART nor AA did report less recovery resource use. Those in the SMART and Neither groups were less likely than the AA and Both groups to have criminal justice involvement as well.
Nearly all participants had previous experience with the mutual-help organization they chose for this recovery attempt—98% of those attending AA had been previously and 91% of those attending SMART had done so previously. Those in SMART were less likely to have attended Narcotics Anonymous previously compared to those in the AA or Both groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Community-based recovery supports, such as mutual-help organizations (e.g., SMART) and recovery community organizations, are expanding. Apart from extensive research showing benefit from AA participation, there is little research on other mutual-help organizations to inform clinical recommendations. As new types of support and services like SMART continue to grow, clinicians and community members will benefit from knowing who is most likely to engage and to benefit from different types of support. This study finds that individuals with alcohol use disorder making a new recovery attempt that chose to attend SMART rather than AA, Both, or Neither were different across demographic, clinical, and recovery-related characteristics. Adults who engaged in SMART were more likely to be White, psychosocially stable, and economically advantaged. They also reported lower alcohol use intensity, less formal treatment and use of recovery support services, and fewer legal problems. These findings suggest that individuals starting a new recovery attempt with more initial recovery assets overall may find aspects of SMART more appealing compared to other mutual-help organizations (e.g., AA).
Furthermore, the findings suggest that SMART may fill a specific need for some. For example, many individuals chose to attend both SMART and AA, which may mean they provide unique but complementary offerings. For example, one possibility is that AA may better provide access to a recovery-supportive social network and help individuals develop recovery coping skills that leverage these social connections while SMART may help individuals develop recovery coping skills they can deploy on their own, independent of social support.
The study was cross-sectional; thus, no conclusions can be made about the effect of SMART compared to the other recovery pathways examined.
Recruitment for this study occurred in Boston, MA and San Diego, CA. Findings may be limited to these regions. Recruitment also occurred during COVID-19, which may have impacted participation in mutual-help organizations in unknown ways.
This study compared individuals choosing SMART, AA, both, or neither. Findings may differ across other mutual-help organizations (e.g., Narcotics Anonymous) or across an individual’s recovery journey. For example, someone may begin their recovery attempt attending AA but choose to switch and attend solely SMART later.
BOTTOM LINE
This cross-sectional study investigated demographic, clinical, and recovery-related characteristics among adults making a recovery attempt and choosing either to attend SMART-only, AA-only, both, or neither. The study found that those choosing to engage SMART-only were more likely to be White, psychosocially stable, economically advantaged, have less formal treatment and recovery support services use, and have fewer legal problems. The findings suggest that aspects of SMART may be appealing to adults with less intensive drinking, treatment, and legal histories, and who possess more initial recovery assets. Furthermore, differences also suggests that SMART fills an important niche in a recovery ecosystem, expanding the range of possible supports among those with alcohol and other drug problems. Future study is warranted to determine what unique benefits SMART confers and for whom.
For individuals and families seeking recovery: Adults choosing to engage SMART-only compared to AA-only, both, or neither were likely to be more affluent, White, have lower alcohol use intensity, and have less formal treatment and legal histories. If you or a loved one is making a new recovery attempt, mutual-help organizations like SMART and AA may be places to find support on your recovery journey. The best plan is likely to consist of sampling several meetings of each to see which one suits you the best, or you may end up utilizing both, capitalizing on the strengths of each.
For treatment professionals and treatment systems: Adults choosing to attend SMART-only compared to AA-only, both, or neither were more likely to be affluent, White, have lower alcohol use intensity, and have less formal treatment or legal involvement. Although this study was cross-sectional and cannot inform conclusions about the effects of these mutual-help organizations, it is likely beneficial to help individuals understand the menu of recovery supports available in the community and gives clues as to who may be best suited to try which particular options.
For scientists:Adults making a new recovery attempt and choosing to attend SMART-only compared to AA- only, both, or neither were more likely to be affluent, White, have lower alcohol use intensity, and have less formal treatment. However, the study cannot determine if the self-selected recovery path was beneficial for an individual or for those choosing that recovery pathway generally. Thus, future longitudinal studies that examine these recovery pathways over time will shed light on how well the different recovery pathways work for whom. Additionally, expanding recruitment to other regions may account for regional differences in mutual-help organization availability and culture.
For policy makers: SMART is one mutual-help organization that may have unique components that appeal to certain individuals—thus filling an important niche in the recovery ecosystem. Additional funding to facilitate SMART meetings as well as investigate its longtime effects would benefit adults seeking or in recovery from alcohol and other drug problems.
For people with alcohol use disorder, mutual-help organizations have the highest rates of engagement across professional and non-professional services. Participation in the 12-step mutual-help organization, Alcoholics Anonymous (AA), produces benefits as large as other addiction-focused interventions while, on average, producing higher rates of sustained abstinence and remission over time. As a community-based organization, it is also very cost-effective, with estimated US-wide treatment cost reductions alone totaling $10 billion compared to other treatments (e.g., cognitive behavioral therapies, motivations enhancement therapies).
Over the last 50 years, there has been a rise in other mutual-help organizations such as Self-Management and Recovery Training or “SMART” Recovery (hereafter SMART). SMART is a mutual-help organization that integrates motivational and cognitive-behavioral clinical approaches, but adapted for a community-based setting. SMART meetings are led by a trained facilitator who may or may not have lived experience in recovery, which is different from most other mutual-help organizations which are entirely peer-led (e.g., AA). Another difference between SMART and most other mutual-help organizations is that SMART is open to anyone with any kind of substance use or behavioral addiction rather than alcohol and other drug use more specifically as is the case for the most popular 12-step groups. Other key differences between SMART and most other mutual-help organizations include an explicit omission of any spiritual or religious content in the approach (people with spiritual and religious backgrounds are welcome and encouraged to attend) and the lack of a social network or “fellowship” cultural norm. Many individuals go to 2 or more types of mutual-help organizations. Thus it is important also to understand how those who attend both SMART and AA might differ from those who attend only one or the other.
As evidence for SMART grows, it will be important to know who is most likely to be drawn to this recovery support option. The current study investigated who chooses to engage in SMART compared to AA, Both AA and SMART, or Neither.
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional analysis that compared 361 adult participants that self-selected into one of four recovery paths: SMART (20.8%), AA (20.2%), both (14.7%), or neither (44.3%). Participants had started a new alcohol use disorder recovery attempt in the past 90 days or were planning to start one in the next 14 days. Those who attended (or were planning to attend) SMART-only, AA-only, or both were categorized accordingly. A fourth group included those that had not attended either SMART or AA in the last 90 days and did not intend to in the subsequent 14 days. Participants were recruited between January 2019 and January 2022 as part of a larger 2-year prospective study of alcohol use disorder recovery pathways. They were recruited at SMART meetings, outpatient treatment, and several community recruitment sources (e.g., ResearchMatch, Facebook, Reddit, newspaper).
All participants reported a primary alcohol use problem, met DSM-5 alcohol use disorder criteria, and consumed alcohol in the past 90 days. They resided in either New England or San Diego. For the assessment, participants provided information spanning demographics, clinical outcomes, and other recovery-related variables. Of all 361 participants, just over half were female (52%) and almost three-quarters were White (74%). The average age was 46, and 36% were married, engaged, or living with partner as if married. Close to half were employed full-time (42%) and had completed a bachelor’s degree or higher (50%).
WHAT DID THIS STUDY FIND?
Demographics of SMART-only participants were different from AA-only participants
Compared to the AA-only, Both, and Neither groups, those in the SMART-only group were more likely to be White (88% versus 77% or less), to have higher incomes (73% with an annual income of $50,000 or more versus 45% or less), and to have higher levels of education (72% with a bachelor’s degree or higher versus 52% or less). Those in the SMART-only group were also more likely to be in a committed relationship (53% versus 36% or less). Other differences emerged that were more nuanced such as those in the SMART-only group were less likely to be female (40%) compared to participants in the Neither group (60%) but not the AA-only or Both groups.
Clinical characteristics of SMART participants were somewhat different from AA participants
Individuals in the SMART-only group had similar alcohol use disorder severity compared to the AA-only and Both groups, but they had higher severity compared to the Neither group. Those in the SMART and Neither groups reported fewer drinks per drinking day in contrast to the AA-only and Both groups. The frequency of other substance use did not differ across the groups nor did the proportion of participations reporting a prior psychiatric diagnosis. Those in the SMART-only group were less likely to have a history of formal treatment compared to the AA and Both groups.
More than 52% of participants in the SMART-only, AA-only, and Both groups reported use of medications for alcohol use disorder in their lifetime, with no differences between these groups. Fewer participants in the Neither group (23%) reported medications for alcohol use disorder. Similarly, use of medications for opioid use disorder was low (9%) in all groups, yet medications for mental health problems was high across all groups (74%). Medication use for opioid use disorder and mental health problems did not differ across groups.
SMART participants were less likely than AA attendees to use other recovery support services
Individuals in the SMART-only group were less likely to report having lived in a recovery residence compared to the AA-only and Both groups. They were also less likely to have attended a recovery community center or recovery community organization. However, SMART and AA-only groups did not differ in their recovery capital, abstinence self-efficacy, or commitment to sobriety. Those choosing to attend neither SMART nor AA did report less recovery resource use. Those in the SMART and Neither groups were less likely than the AA and Both groups to have criminal justice involvement as well.
Nearly all participants had previous experience with the mutual-help organization they chose for this recovery attempt—98% of those attending AA had been previously and 91% of those attending SMART had done so previously. Those in SMART were less likely to have attended Narcotics Anonymous previously compared to those in the AA or Both groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Community-based recovery supports, such as mutual-help organizations (e.g., SMART) and recovery community organizations, are expanding. Apart from extensive research showing benefit from AA participation, there is little research on other mutual-help organizations to inform clinical recommendations. As new types of support and services like SMART continue to grow, clinicians and community members will benefit from knowing who is most likely to engage and to benefit from different types of support. This study finds that individuals with alcohol use disorder making a new recovery attempt that chose to attend SMART rather than AA, Both, or Neither were different across demographic, clinical, and recovery-related characteristics. Adults who engaged in SMART were more likely to be White, psychosocially stable, and economically advantaged. They also reported lower alcohol use intensity, less formal treatment and use of recovery support services, and fewer legal problems. These findings suggest that individuals starting a new recovery attempt with more initial recovery assets overall may find aspects of SMART more appealing compared to other mutual-help organizations (e.g., AA).
Furthermore, the findings suggest that SMART may fill a specific need for some. For example, many individuals chose to attend both SMART and AA, which may mean they provide unique but complementary offerings. For example, one possibility is that AA may better provide access to a recovery-supportive social network and help individuals develop recovery coping skills that leverage these social connections while SMART may help individuals develop recovery coping skills they can deploy on their own, independent of social support.
The study was cross-sectional; thus, no conclusions can be made about the effect of SMART compared to the other recovery pathways examined.
Recruitment for this study occurred in Boston, MA and San Diego, CA. Findings may be limited to these regions. Recruitment also occurred during COVID-19, which may have impacted participation in mutual-help organizations in unknown ways.
This study compared individuals choosing SMART, AA, both, or neither. Findings may differ across other mutual-help organizations (e.g., Narcotics Anonymous) or across an individual’s recovery journey. For example, someone may begin their recovery attempt attending AA but choose to switch and attend solely SMART later.
BOTTOM LINE
This cross-sectional study investigated demographic, clinical, and recovery-related characteristics among adults making a recovery attempt and choosing either to attend SMART-only, AA-only, both, or neither. The study found that those choosing to engage SMART-only were more likely to be White, psychosocially stable, economically advantaged, have less formal treatment and recovery support services use, and have fewer legal problems. The findings suggest that aspects of SMART may be appealing to adults with less intensive drinking, treatment, and legal histories, and who possess more initial recovery assets. Furthermore, differences also suggests that SMART fills an important niche in a recovery ecosystem, expanding the range of possible supports among those with alcohol and other drug problems. Future study is warranted to determine what unique benefits SMART confers and for whom.
For individuals and families seeking recovery: Adults choosing to engage SMART-only compared to AA-only, both, or neither were likely to be more affluent, White, have lower alcohol use intensity, and have less formal treatment and legal histories. If you or a loved one is making a new recovery attempt, mutual-help organizations like SMART and AA may be places to find support on your recovery journey. The best plan is likely to consist of sampling several meetings of each to see which one suits you the best, or you may end up utilizing both, capitalizing on the strengths of each.
For treatment professionals and treatment systems: Adults choosing to attend SMART-only compared to AA-only, both, or neither were more likely to be affluent, White, have lower alcohol use intensity, and have less formal treatment or legal involvement. Although this study was cross-sectional and cannot inform conclusions about the effects of these mutual-help organizations, it is likely beneficial to help individuals understand the menu of recovery supports available in the community and gives clues as to who may be best suited to try which particular options.
For scientists:Adults making a new recovery attempt and choosing to attend SMART-only compared to AA- only, both, or neither were more likely to be affluent, White, have lower alcohol use intensity, and have less formal treatment. However, the study cannot determine if the self-selected recovery path was beneficial for an individual or for those choosing that recovery pathway generally. Thus, future longitudinal studies that examine these recovery pathways over time will shed light on how well the different recovery pathways work for whom. Additionally, expanding recruitment to other regions may account for regional differences in mutual-help organization availability and culture.
For policy makers: SMART is one mutual-help organization that may have unique components that appeal to certain individuals—thus filling an important niche in the recovery ecosystem. Additional funding to facilitate SMART meetings as well as investigate its longtime effects would benefit adults seeking or in recovery from alcohol and other drug problems.