Does stimulant use reduce the benefits of medication for opioid use disorder?
Stimulant use – methamphetamine use especially – is rapidly increasing among people with opioid use disorder, which may impact chances of remission. Using data from 2 randomized controlled trials, this study examined whether ongoing stimulant use after starting medication for opioid use disorder impacted return to opioid use. It also tested if the effect of stimulant use on medication outcomes depended on which medication someone was taking – buprenorphine or extended-release naltrexone.
Illicit opioid use remains a significant public health concern, while opioid use disorder is associated with more substantial psychosocial challenges and barriers to recovery relative to other substance use disorders. Medications for opioid use disorder, such as buprenorphine and extended-release naltrexone, are first-line treatments to reduce opioid overdose-related mortality and return to illicit opioid use. The most commonly used medication for opioid use disorder, buprenorphine (often prescribed in formulation with naloxone and known by the brand name “Suboxone”) binds to opioid receptor sites in the brain but is slower acting and less potent than opioids like heroin, resulting in reductions in craving and withdrawal symptoms while simultaneously blocking other opioids used while the medication is active. Extended-release naltrexone is a monthly injection (known by the brand name “Vivitrol”) that blocks the pleasurable effects of opioids.
Even though these medications are effective, only an estimated 18% of people in 2022 diagnosed with opioid use disorder had taken an opioid use disorder medication that they were prescribed, with initiation rates higher for those prescribed buprenorphine compared to extended-release naltrexone. Further, rates of discontinuation among those who begin medications for opioid use disorder are high (e.g., 65% within 6 months), and so identification of factors that increase adherence to medication for opioid use disorder may increase the overall impact of this approach.
In recent years, there has been a rapid increase in methamphetamine use among people with opioid use disorder, fueling concerns of an emerging “twin epidemic”. In a nationally representative sample, rates of co-use increased from 9.0% in 2015 to 30.2% in 2017. In some regions, such as West Virginia, these increases may be even greater. For those at risk for co-use of these drugs, continued use of stimulants may be risky for individuals in opioid use disorder recovery because 1) methamphetamine use may trigger cravings for opioids among those who used opioids to counteract the negative effects of stimulants; or 2) stimulant use may increase likelihood of exposure to opioid use (e.g., in social settings). For people attempting recovery from opioid use disorder, particularly those using medications for opioid use disorder, continued stimulant use may therefore represent a risk factor for return to use.
This study examined whether ongoing stimulant use influences rates of return to illicit opioid use after the start of medications for opioid use disorder. The study also explored whether the influence of stimulants was different depending upon whether the individual was receiving buprenorphine or extended-release naltrexone.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of longitudinal data using a pooled sample from two National Drug Abuse Treatment Clinical Trials Network randomized clinical trials designed to compare the effectiveness of buprenorphine and extended-release naltrexone. Both clinical trials recruited adults aged 18 years of age or older who met criteria for opioid use disorder seeking treatment for opioid dependence and willing to accept “agonist-based” or “antagonist-based” therapy.
In the first trial, participants were recruited from voluntary opioid treatment programs. In the second trial, participants were recruited at 5 HIV treatment clinics across 5 states. In both trials, participants were randomized to receive either buprenorphine or extended-release naltrexone.
Only participants who received at least one dose of the medication to which they were assigned were included in this study. Researchers collected follow up data regarding daily stimulant or opioid use using the timeline follow-back over approximately 24 weeks. The researchers also collected urine drug screens weekly (Trial 1) or monthly (Trial 2). From the data collected, researchers created indicators of past 7 day stimulant use, return to opioid use (defined as the day in which illicit opioids were used for the first time following initiation of medication for opioid use disorder), and relapse to illicit opioid use, which was operationally defined as meeting one of the following conditions: (1) illicit opioid use for 7 or more days in a row or (2) 4 consecutive weeks of at least 1 day of illicit opioid use per week.
The researchers first descriptively examined rates of return to illicit opioid use and explored stimulant use as a predictor of return to illicit opioid use. Next, researchers examined differences in return to use between buprenorphine and extended-release naltrexone. Researchers then examined stimulant use as a predictor of relapse to illicit opioid use and tested whether there were differences between medications.
The first study randomized 570 participants, and the second study randomized 114. Of the 684 who were randomized, a total of 528 participants initiated medication for opioid use disorder as part of trial participation and were included in the analyses. The sample was primarily between 30 and 49 years of age (49%), male (69%), and non-Hispanic White (66%). Four in five used tobacco every day and 67% reported daily injection drug use.
WHAT DID THIS STUDY FIND?
Stimulant use associated with return to any illicit opioid use
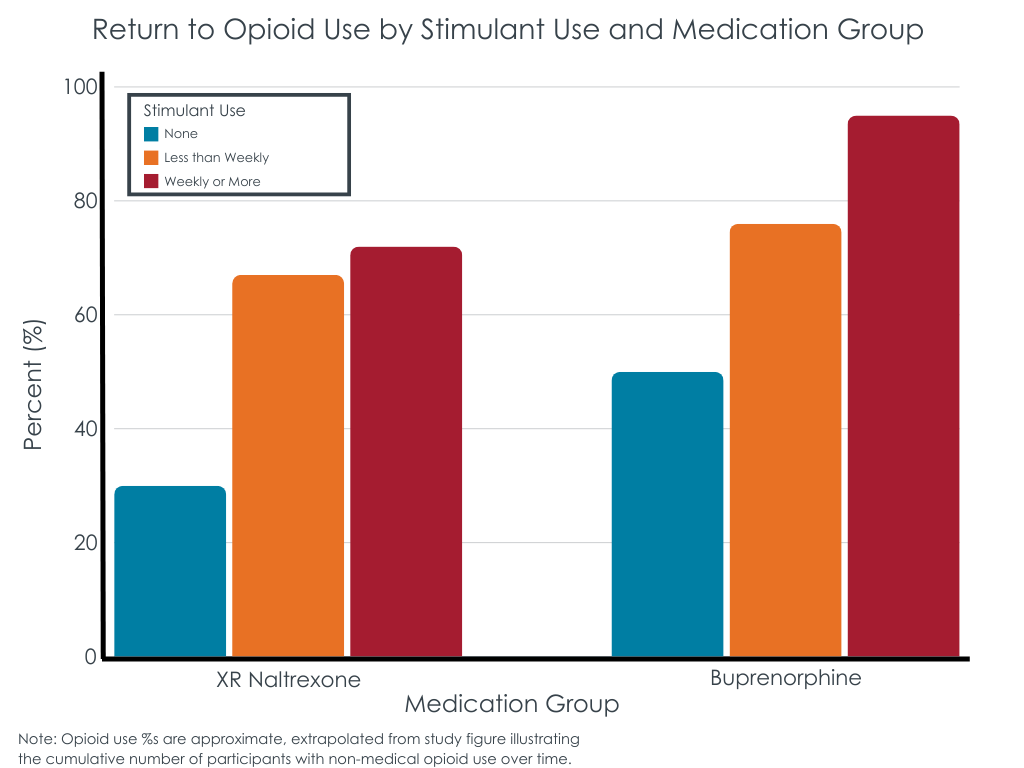
In both trials, participants were less likely to successfully initiate extended-release naltrexone compared to buprenorphine. Buprenorphine and extended-release naltrexone groups were equally likely to report stimulant use, with 47% reporting simulant use after initiation, overall. Buprenorphine participants, however, were more likely to return to any illicit opioid use (67%) compared to those receiving extended-release naltrexone (46%).
On any given day, compared to no stimulant use, stimulant use was associated with a 9-fold increase in likelihood that the participant also reported their first day of illicit opioid use. This added risk associated with stimulant use was lower for the extended-release naltrexone group (~4.5 times greater) relative to the buprenorphine group (~13 times greater).
At the week-level, the results were also consistent: each additional day of past week stimulant use was associated with an additional 27% increase in the risk of return to illicit opioid use that week, with higher rates for buprenorphine (42% increase) relative to extended-release naltrexone (10% increase). Urine drug test results supported the evidence above suggesting that stimulants were associated with return to illicit opioid use (2.8 times more likely); however, there were not any difference between the two medications for opioid use disorder.
Stimulant use associated with relapse to ongoing illicit opioid use
Among those who used illicit opioids at least once during the study period, 66% met criteria for relapse to ongoing illicit opioid use. Those reporting weekly or greater stimulant use following their first use of opioids had 2.3 times greater odds of relapsing to ongoing use. The differences in this effect between extended-release naltrexone and buprenorphine was not statistically significant, however, the findings trended in the same direction, with higher odds of return to ongoing illicit opioid use for those initiated on buprenorphine compared to those initiated on extended-release naltrexone.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The current study provides evidence that stimulant use after initiation of medications for opioid use disorder is associated with worse opioid use outcomes. These findings are of particular significance given the epidemiological trend of increasing rates of stimulant use among people who use opioids. Although partial opioid agonists or antagonists such as buprenorphine and extended-release naltrexone are safe and helpful treatments for opioid use disorder, up to 2/3 discontinue within 6 months after initiation. Stimulant use may be one reason for such low rates of medication adherence, given that in some regions almost half of people who use opioids are now reporting stimulant use. Those who use both stimulants and opioids may also represent a qualitatively distinct class of people with opioid use disorder that are characteristically more severe and also co-use other substance as well. In this case, stimulant use would not necessarily be the “cause” of increased risk, but rather one indicator of a larger index of “severity”.
Consistent with previous research, those randomized to extended-release naltrexone were less likely to successfully initiate treatment compared to buprenorphine; however, among those that did initiate, those in the extended-release naltrexone group were less likely to return to use or relapse to ongoing illicit opioid use after using stimulants compared to those in the buprenorphine group.
Overall, these results suggest that initiating people who use stimulants on extended-release naltrexone may result in improved clinical outcomes. However, this also introduces a clinical conundrum, in which those who plan to continue to use stimulants after initiation of medications for opioid use disorder would most benefit from a medication (extended-release naltrexone) that would be more difficult to initiate. This juxtaposition between greater benefit from extended-release naltrexone but more challenging initiation compared to buprenorphine has also been demonstrated with other populations with opioid use disorder, such as people experiencing homelessness.
Understanding reasons for poorer initiation rates for extended-release naltrexone is an important step to increase its clinical value. This phenomenon may be in part explained by the fact that extended-release naltrexone requires a 7-day abstinence period to initiate. Other researchers conducting clinical trials for extended-release naltrexone have hypothesized that those who inject heroin or co-use opioids with cocaine or other stimulants may be more likely to have more severe withdrawal symptoms in general which may interfere with initiation of extended-release naltrexone. Supporting this premise, there are greater rates of successful initiation of extended-release naltrexone among people in an inpatient setting compared to an outpatient setting. For people starting recovery from opioid use disorder who are likely to continue stimulant use following initiation of an opioid use disorder, it may be advisable to initiate extended-release naltrexone in an inpatient setting during the withdrawal period to enhance their chances of successful sustained remission. More research is needed to identify factors that reduce initiation to improve sustained recovery for this critical and growing population.
Finally, given high rates of stimulant use among people with opioid use disorder in this study, research is needed on strategies to supplement medications with empirically-supported interventions to prevent or address stimulant use. This approach has been successfully established when treating other forms of substance use disorder. For example, studies have demonstrated that empirically-supported treatments such as cognitive-behavior therapy and contingency management help to address concomitant cocaine use for individuals receiving methadone maintenance for opioid use disorder.
The two trials recruited from voluntary opioid treatment programs and HIV clinics, which may not be representative of the general population of people with opioid use disorder.
By design, only participants who received at least one dose of the medication to which they were assigned were included in this study.
BOTTOM LINE
Almost half of people used stimulants following initiation onto a medication for opioid use disorder under optimal conditions – a rigorous clinical trial. Stimulant use was associated with increased risk of return to opioid use and relapse to ongoing illicit opioid use; however, the risk was greater for those who received buprenorphine relative to extended-release naltrexone. It is unclear whether stimulant use is a direct causal factor in elevated risk for opioid use, a marker for greater opioid use disorder severity, or whether its use reflects psychological factors such as lower motivation for stopping substance use or lack of concern for adverse consequences.
For individuals and families seeking recovery: If you or a family member are seeking help for opioid use disorder and are likely to continue stimulant use following initiation of an opioid use disorder, extended-release naltrexone may result in better outcomes than buprenorphine. However, initiation on extended-release naltrexone requires an initial period of abstinence which may be difficult for some, and initiating in an inpatient setting during the withdrawal period may increase chances of successful sustained remission. Sustained recovery may be more likely when medication for opioid use disorder is paired with treatments or recovery support services that are known to be effective for treating or managing other substance use disorder including but not limited to stimulant use disorder.
For treatment professionals and treatment systems: Awareness of other substance use, and stimulant use in particular, among those initiating medications for opioid use disorder may help providers identify a critical issue that interferes with successful remission. The current study also supports calls for increased personalized medicine for substance use disorder, which pairs treatments with patients idiosyncratically based upon patient-level factors. Understanding patient characteristics may maximize treatment efficacy. For example, the current study suggests that those currently using stimulants while starting a recovery attempt from opioid use disorder may be more likely to succeed with extended-release naltrexone, assuming that the early initiation period can be effectively managed and risk for treatment drop out is mitigated. Initiation of pharmacotherapy may also be improved when paired with other treatments or recovery support services, given the high prevalence and compounding risk of stimulant use.
For scientists:More research is necessary to understand the reasons for the association between stimulant use and return to use following initiation on medications for opioid use. Additional research to identify patient-level characteristics that may influence outcomes may inform trials testing the efficacy of personalized medicine approaches to enhance initiation on medications for opioid use disorder. In other words, this study suggests that those using stimulants may be more likely to succeed at remission from opioid use disorder when prescribed extended-release naltrexone, assuming the risk for treatment drop out is mitigated. Future studies examining factors associated with initiation on extended-release naltrexone may help reduce dropout in this critical initiation period. However, studies measuring the additive benefit of medications for opioid use disorder with other treatments or recovery support services may also improve rates of initiation and sustained recovery in this co-use population.
For policy makers: The current study highlights individual level characteristics that interfere with treatment efficacy. High dropout rates may indicate that a medication for opioid use disorder has not been adequately tailored to an individual’s unique clinical profile. More research and policy development is needed to continue to understand factors influencing treatment efficacy, which may ultimately result in personalized medicine approaches. The value of medication may also be improved if policy encouraged pairing pharmacotherapy with other treatments or recovery support services, given the high prevalence and compounding risk of stimulant use.
Illicit opioid use remains a significant public health concern, while opioid use disorder is associated with more substantial psychosocial challenges and barriers to recovery relative to other substance use disorders. Medications for opioid use disorder, such as buprenorphine and extended-release naltrexone, are first-line treatments to reduce opioid overdose-related mortality and return to illicit opioid use. The most commonly used medication for opioid use disorder, buprenorphine (often prescribed in formulation with naloxone and known by the brand name “Suboxone”) binds to opioid receptor sites in the brain but is slower acting and less potent than opioids like heroin, resulting in reductions in craving and withdrawal symptoms while simultaneously blocking other opioids used while the medication is active. Extended-release naltrexone is a monthly injection (known by the brand name “Vivitrol”) that blocks the pleasurable effects of opioids.
Even though these medications are effective, only an estimated 18% of people in 2022 diagnosed with opioid use disorder had taken an opioid use disorder medication that they were prescribed, with initiation rates higher for those prescribed buprenorphine compared to extended-release naltrexone. Further, rates of discontinuation among those who begin medications for opioid use disorder are high (e.g., 65% within 6 months), and so identification of factors that increase adherence to medication for opioid use disorder may increase the overall impact of this approach.
In recent years, there has been a rapid increase in methamphetamine use among people with opioid use disorder, fueling concerns of an emerging “twin epidemic”. In a nationally representative sample, rates of co-use increased from 9.0% in 2015 to 30.2% in 2017. In some regions, such as West Virginia, these increases may be even greater. For those at risk for co-use of these drugs, continued use of stimulants may be risky for individuals in opioid use disorder recovery because 1) methamphetamine use may trigger cravings for opioids among those who used opioids to counteract the negative effects of stimulants; or 2) stimulant use may increase likelihood of exposure to opioid use (e.g., in social settings). For people attempting recovery from opioid use disorder, particularly those using medications for opioid use disorder, continued stimulant use may therefore represent a risk factor for return to use.
This study examined whether ongoing stimulant use influences rates of return to illicit opioid use after the start of medications for opioid use disorder. The study also explored whether the influence of stimulants was different depending upon whether the individual was receiving buprenorphine or extended-release naltrexone.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of longitudinal data using a pooled sample from two National Drug Abuse Treatment Clinical Trials Network randomized clinical trials designed to compare the effectiveness of buprenorphine and extended-release naltrexone. Both clinical trials recruited adults aged 18 years of age or older who met criteria for opioid use disorder seeking treatment for opioid dependence and willing to accept “agonist-based” or “antagonist-based” therapy.
In the first trial, participants were recruited from voluntary opioid treatment programs. In the second trial, participants were recruited at 5 HIV treatment clinics across 5 states. In both trials, participants were randomized to receive either buprenorphine or extended-release naltrexone.
Only participants who received at least one dose of the medication to which they were assigned were included in this study. Researchers collected follow up data regarding daily stimulant or opioid use using the timeline follow-back over approximately 24 weeks. The researchers also collected urine drug screens weekly (Trial 1) or monthly (Trial 2). From the data collected, researchers created indicators of past 7 day stimulant use, return to opioid use (defined as the day in which illicit opioids were used for the first time following initiation of medication for opioid use disorder), and relapse to illicit opioid use, which was operationally defined as meeting one of the following conditions: (1) illicit opioid use for 7 or more days in a row or (2) 4 consecutive weeks of at least 1 day of illicit opioid use per week.
The researchers first descriptively examined rates of return to illicit opioid use and explored stimulant use as a predictor of return to illicit opioid use. Next, researchers examined differences in return to use between buprenorphine and extended-release naltrexone. Researchers then examined stimulant use as a predictor of relapse to illicit opioid use and tested whether there were differences between medications.
The first study randomized 570 participants, and the second study randomized 114. Of the 684 who were randomized, a total of 528 participants initiated medication for opioid use disorder as part of trial participation and were included in the analyses. The sample was primarily between 30 and 49 years of age (49%), male (69%), and non-Hispanic White (66%). Four in five used tobacco every day and 67% reported daily injection drug use.
WHAT DID THIS STUDY FIND?
Stimulant use associated with return to any illicit opioid use
In both trials, participants were less likely to successfully initiate extended-release naltrexone compared to buprenorphine. Buprenorphine and extended-release naltrexone groups were equally likely to report stimulant use, with 47% reporting simulant use after initiation, overall. Buprenorphine participants, however, were more likely to return to any illicit opioid use (67%) compared to those receiving extended-release naltrexone (46%).
On any given day, compared to no stimulant use, stimulant use was associated with a 9-fold increase in likelihood that the participant also reported their first day of illicit opioid use. This added risk associated with stimulant use was lower for the extended-release naltrexone group (~4.5 times greater) relative to the buprenorphine group (~13 times greater).
At the week-level, the results were also consistent: each additional day of past week stimulant use was associated with an additional 27% increase in the risk of return to illicit opioid use that week, with higher rates for buprenorphine (42% increase) relative to extended-release naltrexone (10% increase). Urine drug test results supported the evidence above suggesting that stimulants were associated with return to illicit opioid use (2.8 times more likely); however, there were not any difference between the two medications for opioid use disorder.
Stimulant use associated with relapse to ongoing illicit opioid use
Among those who used illicit opioids at least once during the study period, 66% met criteria for relapse to ongoing illicit opioid use. Those reporting weekly or greater stimulant use following their first use of opioids had 2.3 times greater odds of relapsing to ongoing use. The differences in this effect between extended-release naltrexone and buprenorphine was not statistically significant, however, the findings trended in the same direction, with higher odds of return to ongoing illicit opioid use for those initiated on buprenorphine compared to those initiated on extended-release naltrexone.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The current study provides evidence that stimulant use after initiation of medications for opioid use disorder is associated with worse opioid use outcomes. These findings are of particular significance given the epidemiological trend of increasing rates of stimulant use among people who use opioids. Although partial opioid agonists or antagonists such as buprenorphine and extended-release naltrexone are safe and helpful treatments for opioid use disorder, up to 2/3 discontinue within 6 months after initiation. Stimulant use may be one reason for such low rates of medication adherence, given that in some regions almost half of people who use opioids are now reporting stimulant use. Those who use both stimulants and opioids may also represent a qualitatively distinct class of people with opioid use disorder that are characteristically more severe and also co-use other substance as well. In this case, stimulant use would not necessarily be the “cause” of increased risk, but rather one indicator of a larger index of “severity”.
Consistent with previous research, those randomized to extended-release naltrexone were less likely to successfully initiate treatment compared to buprenorphine; however, among those that did initiate, those in the extended-release naltrexone group were less likely to return to use or relapse to ongoing illicit opioid use after using stimulants compared to those in the buprenorphine group.
Overall, these results suggest that initiating people who use stimulants on extended-release naltrexone may result in improved clinical outcomes. However, this also introduces a clinical conundrum, in which those who plan to continue to use stimulants after initiation of medications for opioid use disorder would most benefit from a medication (extended-release naltrexone) that would be more difficult to initiate. This juxtaposition between greater benefit from extended-release naltrexone but more challenging initiation compared to buprenorphine has also been demonstrated with other populations with opioid use disorder, such as people experiencing homelessness.
Understanding reasons for poorer initiation rates for extended-release naltrexone is an important step to increase its clinical value. This phenomenon may be in part explained by the fact that extended-release naltrexone requires a 7-day abstinence period to initiate. Other researchers conducting clinical trials for extended-release naltrexone have hypothesized that those who inject heroin or co-use opioids with cocaine or other stimulants may be more likely to have more severe withdrawal symptoms in general which may interfere with initiation of extended-release naltrexone. Supporting this premise, there are greater rates of successful initiation of extended-release naltrexone among people in an inpatient setting compared to an outpatient setting. For people starting recovery from opioid use disorder who are likely to continue stimulant use following initiation of an opioid use disorder, it may be advisable to initiate extended-release naltrexone in an inpatient setting during the withdrawal period to enhance their chances of successful sustained remission. More research is needed to identify factors that reduce initiation to improve sustained recovery for this critical and growing population.
Finally, given high rates of stimulant use among people with opioid use disorder in this study, research is needed on strategies to supplement medications with empirically-supported interventions to prevent or address stimulant use. This approach has been successfully established when treating other forms of substance use disorder. For example, studies have demonstrated that empirically-supported treatments such as cognitive-behavior therapy and contingency management help to address concomitant cocaine use for individuals receiving methadone maintenance for opioid use disorder.
The two trials recruited from voluntary opioid treatment programs and HIV clinics, which may not be representative of the general population of people with opioid use disorder.
By design, only participants who received at least one dose of the medication to which they were assigned were included in this study.
BOTTOM LINE
Almost half of people used stimulants following initiation onto a medication for opioid use disorder under optimal conditions – a rigorous clinical trial. Stimulant use was associated with increased risk of return to opioid use and relapse to ongoing illicit opioid use; however, the risk was greater for those who received buprenorphine relative to extended-release naltrexone. It is unclear whether stimulant use is a direct causal factor in elevated risk for opioid use, a marker for greater opioid use disorder severity, or whether its use reflects psychological factors such as lower motivation for stopping substance use or lack of concern for adverse consequences.
For individuals and families seeking recovery: If you or a family member are seeking help for opioid use disorder and are likely to continue stimulant use following initiation of an opioid use disorder, extended-release naltrexone may result in better outcomes than buprenorphine. However, initiation on extended-release naltrexone requires an initial period of abstinence which may be difficult for some, and initiating in an inpatient setting during the withdrawal period may increase chances of successful sustained remission. Sustained recovery may be more likely when medication for opioid use disorder is paired with treatments or recovery support services that are known to be effective for treating or managing other substance use disorder including but not limited to stimulant use disorder.
For treatment professionals and treatment systems: Awareness of other substance use, and stimulant use in particular, among those initiating medications for opioid use disorder may help providers identify a critical issue that interferes with successful remission. The current study also supports calls for increased personalized medicine for substance use disorder, which pairs treatments with patients idiosyncratically based upon patient-level factors. Understanding patient characteristics may maximize treatment efficacy. For example, the current study suggests that those currently using stimulants while starting a recovery attempt from opioid use disorder may be more likely to succeed with extended-release naltrexone, assuming that the early initiation period can be effectively managed and risk for treatment drop out is mitigated. Initiation of pharmacotherapy may also be improved when paired with other treatments or recovery support services, given the high prevalence and compounding risk of stimulant use.
For scientists:More research is necessary to understand the reasons for the association between stimulant use and return to use following initiation on medications for opioid use. Additional research to identify patient-level characteristics that may influence outcomes may inform trials testing the efficacy of personalized medicine approaches to enhance initiation on medications for opioid use disorder. In other words, this study suggests that those using stimulants may be more likely to succeed at remission from opioid use disorder when prescribed extended-release naltrexone, assuming the risk for treatment drop out is mitigated. Future studies examining factors associated with initiation on extended-release naltrexone may help reduce dropout in this critical initiation period. However, studies measuring the additive benefit of medications for opioid use disorder with other treatments or recovery support services may also improve rates of initiation and sustained recovery in this co-use population.
For policy makers: The current study highlights individual level characteristics that interfere with treatment efficacy. High dropout rates may indicate that a medication for opioid use disorder has not been adequately tailored to an individual’s unique clinical profile. More research and policy development is needed to continue to understand factors influencing treatment efficacy, which may ultimately result in personalized medicine approaches. The value of medication may also be improved if policy encouraged pairing pharmacotherapy with other treatments or recovery support services, given the high prevalence and compounding risk of stimulant use.
Illicit opioid use remains a significant public health concern, while opioid use disorder is associated with more substantial psychosocial challenges and barriers to recovery relative to other substance use disorders. Medications for opioid use disorder, such as buprenorphine and extended-release naltrexone, are first-line treatments to reduce opioid overdose-related mortality and return to illicit opioid use. The most commonly used medication for opioid use disorder, buprenorphine (often prescribed in formulation with naloxone and known by the brand name “Suboxone”) binds to opioid receptor sites in the brain but is slower acting and less potent than opioids like heroin, resulting in reductions in craving and withdrawal symptoms while simultaneously blocking other opioids used while the medication is active. Extended-release naltrexone is a monthly injection (known by the brand name “Vivitrol”) that blocks the pleasurable effects of opioids.
Even though these medications are effective, only an estimated 18% of people in 2022 diagnosed with opioid use disorder had taken an opioid use disorder medication that they were prescribed, with initiation rates higher for those prescribed buprenorphine compared to extended-release naltrexone. Further, rates of discontinuation among those who begin medications for opioid use disorder are high (e.g., 65% within 6 months), and so identification of factors that increase adherence to medication for opioid use disorder may increase the overall impact of this approach.
In recent years, there has been a rapid increase in methamphetamine use among people with opioid use disorder, fueling concerns of an emerging “twin epidemic”. In a nationally representative sample, rates of co-use increased from 9.0% in 2015 to 30.2% in 2017. In some regions, such as West Virginia, these increases may be even greater. For those at risk for co-use of these drugs, continued use of stimulants may be risky for individuals in opioid use disorder recovery because 1) methamphetamine use may trigger cravings for opioids among those who used opioids to counteract the negative effects of stimulants; or 2) stimulant use may increase likelihood of exposure to opioid use (e.g., in social settings). For people attempting recovery from opioid use disorder, particularly those using medications for opioid use disorder, continued stimulant use may therefore represent a risk factor for return to use.
This study examined whether ongoing stimulant use influences rates of return to illicit opioid use after the start of medications for opioid use disorder. The study also explored whether the influence of stimulants was different depending upon whether the individual was receiving buprenorphine or extended-release naltrexone.
HOW WAS THIS STUDY CONDUCTED?
This was a secondary analysis of longitudinal data using a pooled sample from two National Drug Abuse Treatment Clinical Trials Network randomized clinical trials designed to compare the effectiveness of buprenorphine and extended-release naltrexone. Both clinical trials recruited adults aged 18 years of age or older who met criteria for opioid use disorder seeking treatment for opioid dependence and willing to accept “agonist-based” or “antagonist-based” therapy.
In the first trial, participants were recruited from voluntary opioid treatment programs. In the second trial, participants were recruited at 5 HIV treatment clinics across 5 states. In both trials, participants were randomized to receive either buprenorphine or extended-release naltrexone.
Only participants who received at least one dose of the medication to which they were assigned were included in this study. Researchers collected follow up data regarding daily stimulant or opioid use using the timeline follow-back over approximately 24 weeks. The researchers also collected urine drug screens weekly (Trial 1) or monthly (Trial 2). From the data collected, researchers created indicators of past 7 day stimulant use, return to opioid use (defined as the day in which illicit opioids were used for the first time following initiation of medication for opioid use disorder), and relapse to illicit opioid use, which was operationally defined as meeting one of the following conditions: (1) illicit opioid use for 7 or more days in a row or (2) 4 consecutive weeks of at least 1 day of illicit opioid use per week.
The researchers first descriptively examined rates of return to illicit opioid use and explored stimulant use as a predictor of return to illicit opioid use. Next, researchers examined differences in return to use between buprenorphine and extended-release naltrexone. Researchers then examined stimulant use as a predictor of relapse to illicit opioid use and tested whether there were differences between medications.
The first study randomized 570 participants, and the second study randomized 114. Of the 684 who were randomized, a total of 528 participants initiated medication for opioid use disorder as part of trial participation and were included in the analyses. The sample was primarily between 30 and 49 years of age (49%), male (69%), and non-Hispanic White (66%). Four in five used tobacco every day and 67% reported daily injection drug use.
WHAT DID THIS STUDY FIND?
Stimulant use associated with return to any illicit opioid use
In both trials, participants were less likely to successfully initiate extended-release naltrexone compared to buprenorphine. Buprenorphine and extended-release naltrexone groups were equally likely to report stimulant use, with 47% reporting simulant use after initiation, overall. Buprenorphine participants, however, were more likely to return to any illicit opioid use (67%) compared to those receiving extended-release naltrexone (46%).
On any given day, compared to no stimulant use, stimulant use was associated with a 9-fold increase in likelihood that the participant also reported their first day of illicit opioid use. This added risk associated with stimulant use was lower for the extended-release naltrexone group (~4.5 times greater) relative to the buprenorphine group (~13 times greater).
At the week-level, the results were also consistent: each additional day of past week stimulant use was associated with an additional 27% increase in the risk of return to illicit opioid use that week, with higher rates for buprenorphine (42% increase) relative to extended-release naltrexone (10% increase). Urine drug test results supported the evidence above suggesting that stimulants were associated with return to illicit opioid use (2.8 times more likely); however, there were not any difference between the two medications for opioid use disorder.
Stimulant use associated with relapse to ongoing illicit opioid use
Among those who used illicit opioids at least once during the study period, 66% met criteria for relapse to ongoing illicit opioid use. Those reporting weekly or greater stimulant use following their first use of opioids had 2.3 times greater odds of relapsing to ongoing use. The differences in this effect between extended-release naltrexone and buprenorphine was not statistically significant, however, the findings trended in the same direction, with higher odds of return to ongoing illicit opioid use for those initiated on buprenorphine compared to those initiated on extended-release naltrexone.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The current study provides evidence that stimulant use after initiation of medications for opioid use disorder is associated with worse opioid use outcomes. These findings are of particular significance given the epidemiological trend of increasing rates of stimulant use among people who use opioids. Although partial opioid agonists or antagonists such as buprenorphine and extended-release naltrexone are safe and helpful treatments for opioid use disorder, up to 2/3 discontinue within 6 months after initiation. Stimulant use may be one reason for such low rates of medication adherence, given that in some regions almost half of people who use opioids are now reporting stimulant use. Those who use both stimulants and opioids may also represent a qualitatively distinct class of people with opioid use disorder that are characteristically more severe and also co-use other substance as well. In this case, stimulant use would not necessarily be the “cause” of increased risk, but rather one indicator of a larger index of “severity”.
Consistent with previous research, those randomized to extended-release naltrexone were less likely to successfully initiate treatment compared to buprenorphine; however, among those that did initiate, those in the extended-release naltrexone group were less likely to return to use or relapse to ongoing illicit opioid use after using stimulants compared to those in the buprenorphine group.
Overall, these results suggest that initiating people who use stimulants on extended-release naltrexone may result in improved clinical outcomes. However, this also introduces a clinical conundrum, in which those who plan to continue to use stimulants after initiation of medications for opioid use disorder would most benefit from a medication (extended-release naltrexone) that would be more difficult to initiate. This juxtaposition between greater benefit from extended-release naltrexone but more challenging initiation compared to buprenorphine has also been demonstrated with other populations with opioid use disorder, such as people experiencing homelessness.
Understanding reasons for poorer initiation rates for extended-release naltrexone is an important step to increase its clinical value. This phenomenon may be in part explained by the fact that extended-release naltrexone requires a 7-day abstinence period to initiate. Other researchers conducting clinical trials for extended-release naltrexone have hypothesized that those who inject heroin or co-use opioids with cocaine or other stimulants may be more likely to have more severe withdrawal symptoms in general which may interfere with initiation of extended-release naltrexone. Supporting this premise, there are greater rates of successful initiation of extended-release naltrexone among people in an inpatient setting compared to an outpatient setting. For people starting recovery from opioid use disorder who are likely to continue stimulant use following initiation of an opioid use disorder, it may be advisable to initiate extended-release naltrexone in an inpatient setting during the withdrawal period to enhance their chances of successful sustained remission. More research is needed to identify factors that reduce initiation to improve sustained recovery for this critical and growing population.
Finally, given high rates of stimulant use among people with opioid use disorder in this study, research is needed on strategies to supplement medications with empirically-supported interventions to prevent or address stimulant use. This approach has been successfully established when treating other forms of substance use disorder. For example, studies have demonstrated that empirically-supported treatments such as cognitive-behavior therapy and contingency management help to address concomitant cocaine use for individuals receiving methadone maintenance for opioid use disorder.
The two trials recruited from voluntary opioid treatment programs and HIV clinics, which may not be representative of the general population of people with opioid use disorder.
By design, only participants who received at least one dose of the medication to which they were assigned were included in this study.
BOTTOM LINE
Almost half of people used stimulants following initiation onto a medication for opioid use disorder under optimal conditions – a rigorous clinical trial. Stimulant use was associated with increased risk of return to opioid use and relapse to ongoing illicit opioid use; however, the risk was greater for those who received buprenorphine relative to extended-release naltrexone. It is unclear whether stimulant use is a direct causal factor in elevated risk for opioid use, a marker for greater opioid use disorder severity, or whether its use reflects psychological factors such as lower motivation for stopping substance use or lack of concern for adverse consequences.
For individuals and families seeking recovery: If you or a family member are seeking help for opioid use disorder and are likely to continue stimulant use following initiation of an opioid use disorder, extended-release naltrexone may result in better outcomes than buprenorphine. However, initiation on extended-release naltrexone requires an initial period of abstinence which may be difficult for some, and initiating in an inpatient setting during the withdrawal period may increase chances of successful sustained remission. Sustained recovery may be more likely when medication for opioid use disorder is paired with treatments or recovery support services that are known to be effective for treating or managing other substance use disorder including but not limited to stimulant use disorder.
For treatment professionals and treatment systems: Awareness of other substance use, and stimulant use in particular, among those initiating medications for opioid use disorder may help providers identify a critical issue that interferes with successful remission. The current study also supports calls for increased personalized medicine for substance use disorder, which pairs treatments with patients idiosyncratically based upon patient-level factors. Understanding patient characteristics may maximize treatment efficacy. For example, the current study suggests that those currently using stimulants while starting a recovery attempt from opioid use disorder may be more likely to succeed with extended-release naltrexone, assuming that the early initiation period can be effectively managed and risk for treatment drop out is mitigated. Initiation of pharmacotherapy may also be improved when paired with other treatments or recovery support services, given the high prevalence and compounding risk of stimulant use.
For scientists:More research is necessary to understand the reasons for the association between stimulant use and return to use following initiation on medications for opioid use. Additional research to identify patient-level characteristics that may influence outcomes may inform trials testing the efficacy of personalized medicine approaches to enhance initiation on medications for opioid use disorder. In other words, this study suggests that those using stimulants may be more likely to succeed at remission from opioid use disorder when prescribed extended-release naltrexone, assuming the risk for treatment drop out is mitigated. Future studies examining factors associated with initiation on extended-release naltrexone may help reduce dropout in this critical initiation period. However, studies measuring the additive benefit of medications for opioid use disorder with other treatments or recovery support services may also improve rates of initiation and sustained recovery in this co-use population.
For policy makers: The current study highlights individual level characteristics that interfere with treatment efficacy. High dropout rates may indicate that a medication for opioid use disorder has not been adequately tailored to an individual’s unique clinical profile. More research and policy development is needed to continue to understand factors influencing treatment efficacy, which may ultimately result in personalized medicine approaches. The value of medication may also be improved if policy encouraged pairing pharmacotherapy with other treatments or recovery support services, given the high prevalence and compounding risk of stimulant use.