OB-GYNs Say Opioid Use Disorders During Pregnancy Provide Opportunities for Life-changing Interventions
Opioid misuse during pregnancy and the postpartum period does not always constitute a medical emergency, but it can provide opportunities for excellent healthcare for mother, fetus, and infant. This clinical opinion piece reviews the major considerations for OB-GYNs who care for opioid-using women…
The opioid epidemic has resulted in hundreds of thousands of preventable deaths and has received national attention by the world’s most powerful political figures. Opioid use and opioid use disorder affects all walks of life including pregnant and postpartum women. The prevalence of opioid use disorder during pregnancy increased by 127%, from 1.7 per 1,000 delivery admissions in 1998 to 3.9 per 1,000 delivery admissions in 2011. More recently, almost 1% of pregnant women reported non-medical use of opioids in the past 30 days.
Pregnancy presents providers with a window of opportunity to screen for substance use disorders, offer brief intervention, and refer women to specialized treatment. In this clinical opinion piece, OB-GYNs (doctors who specialize in women’s health) with expertise in the treatment of opioid use disorder during pregnancy review clinical care issues associated with illicit and prescribed opioid use in the pregnant and postpartum period and outline the major responsibilities of OB-GYNs.
HOW WAS THIS STUDY CONDUCTED?
This summary highlights formal conclusions from the proceedings of the Expert Meeting on Perinatal Illicit Drug Abuse that was convened by the US Centers for Disease Control and Prevention (CDC).
WHAT DID THIS STUDY FIND?
This clinical opinion piece outlines the following points regarding clinical care issues that are related to opioid use and opioid use disorder in the prenatal, triage (emergency department), and postpartum phases of care.
PRENATAL CARE
Building rapport can enable useful communication in a population that may be reluctant to disclose their history. This can be done by permitting the patient to speak uninterrupted, summarizing what the patient said using their words, maintaining eye contact, active listening such as nodding, and asking clarifying questions. These common elements of good, person-centered, counseling, help build trust and patients’ engagement with care.
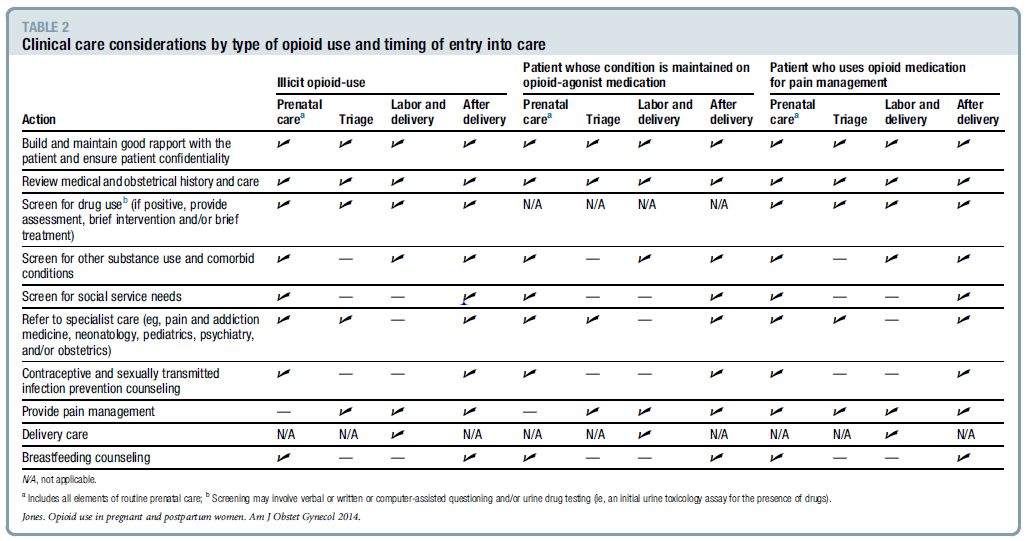
Actions of clinical care by type of opioid use and point of entry into care are described in Table 1. Specifically, across the top of Table 1 lists the type of opioid use such as illicit, maintenance treatment, and pain management and the point of patient entry including prenatal, triage, labor and delivery, and after delivery. Coordinate care (not hand-off care) with a pain or addiction medicine practitioner. Obstetric providers should ensure that referral agencies accept the patients insurance and are accessible.
Inform patients that neonatal abstinence syndrome, which occurs when a fetus is exposed to drugs, is an expected and treatable condition. Neonatal abstinence syndrome is characterized by hyperirritability of the central nervous system, dysfunction in the autonomic nervous system, gastrointestinal tract, and respiratory system. Discuss the signs and the anticipated maternal and newborn infant length of hospital stays.
If a patient is maintained on an opioid agonist, continue the maintenance and enhance pain management for acute needs. Pain management should be based on clinical assessment and not on the prescribed maintenance dose of medication.
There is a need to avoid partial agonist/antagonist intravenous treatments to reduce labor pain. Labor epidural or combined spinal/epidural forms of pain management typically works well. Practitioners should advise patients that the expectation of total pain control may be not achievable despite the use of analgesia due to increased pain sensitivity from long-term opioid use.
For patients who use illicit benzodiazepines (common in patients who use opioids), treatment to prevent benzodiazepine withdrawal may be indicated.
POSTPARTUM CARE
Breastfeeding is compatible with the low levels of methadone or buprenorphine that are present in breast milk.
The patient should be encouraged to postpone transitioning off opioid agonist or partial agonist treatments until she is living in a home that does not have drug-related activity, the infant sleeps through the night, breastfeeding is completed, and until she has built enough recovery resources (“recovery capital”) to help sustain remission. For some patients, long-term opioid agonist treatment may be best – scientific evidence, clinical needs, and patient motivation must all be considered in helping these patients maintain opioid abstinence.
Actions of Clinical Care by Type of Opioid Use (illicit, maintenance treatment, or pain management) and Point of Entry into Care.
WHY IS THIS STUDY IMPORTANT
This clinical opinion piece raised some key points regarding obstetric care for opioid using women during pregnancy and postpartum periods. The goal is to provide excellent healthcare to women who use opioids by increasing their willingness to seek and receive the needed medical and social support services.
OB-GYNs who acquire the knowledge, skills, and specialty support maximize their chances of providing high quality evidenced–based care to this growing population.
This is a clinical opinion piece, and is limited by its reliance on the expertise of the authors. In this case, the authors incorporated references to many peer-reviewed studies to both explain and support their clinical advice which mostly focused on the patient-provider relationship and the role of medications.
The opinion piece did not address ways to help facilitate patient participation in recovery supportive social networks and environments, such mutual help organizations, which are empirically shown to be associated with higher rates of treatment engagement and abstinence when used with medication.
NEXT STEPS
Given that both clinicians and patients have unanswered questions regarding the expected duration of pharmacological treatment, more research should be done to inform this question for pregnant and postpartum populations.
BOTTOM LINE
For individuals & families seeking recovery: This opinion piece reviewed clinical care issues for pregnant and postpartum women. It is important to have open communication with your provider and discuss any use of opioids so they can give you treatment options that best support the health of you, your fetus, and newborn.
For scientists: This clinical opinion article encourages OB-GYNs to screen for substance use disorders in pregnant and postpartum women and coordinate care when indicated. This population may have complex psychosocial and environmental factors or co-occurring psychiatric conditions. Although screening for substance use disorder is a well-developed test, more work could be done to help clinicians swiftly navigate and prioritize the maze of other factors that could be critical for the patient’s needs.
For policy makers: This opinion piece reviews clinical care issues that are related to illicit and prescribed opioid use among pregnant women and women in the postpartum period. The authors suggest that OB-GYNs have an ethical obligation to screen, assess, and provide a brief interventions and referral to treatment for patients with an opioid use disorder. Consider prioritizing policies and funding that motivate and facilitate obstetric providers to screen and coordinate care for pregnant and postpartum patients who use opioids.
For treatment professionals and treatment systems: This clinical opinion piece outlines major responsibilities of OB-GYNs who treat women who use opioids. Encourage your patients to seek regular obstetric care if they are pregnant. Treatment providers should coordinate care plans with OB-GYNs throughout the prenatal, labor and delivery, and postpartum periods to help support remission and recovery.
The opioid epidemic has resulted in hundreds of thousands of preventable deaths and has received national attention by the world’s most powerful political figures. Opioid use and opioid use disorder affects all walks of life including pregnant and postpartum women. The prevalence of opioid use disorder during pregnancy increased by 127%, from 1.7 per 1,000 delivery admissions in 1998 to 3.9 per 1,000 delivery admissions in 2011. More recently, almost 1% of pregnant women reported non-medical use of opioids in the past 30 days.
Pregnancy presents providers with a window of opportunity to screen for substance use disorders, offer brief intervention, and refer women to specialized treatment. In this clinical opinion piece, OB-GYNs (doctors who specialize in women’s health) with expertise in the treatment of opioid use disorder during pregnancy review clinical care issues associated with illicit and prescribed opioid use in the pregnant and postpartum period and outline the major responsibilities of OB-GYNs.
HOW WAS THIS STUDY CONDUCTED?
This summary highlights formal conclusions from the proceedings of the Expert Meeting on Perinatal Illicit Drug Abuse that was convened by the US Centers for Disease Control and Prevention (CDC).
WHAT DID THIS STUDY FIND?
This clinical opinion piece outlines the following points regarding clinical care issues that are related to opioid use and opioid use disorder in the prenatal, triage (emergency department), and postpartum phases of care.
PRENATAL CARE
Building rapport can enable useful communication in a population that may be reluctant to disclose their history. This can be done by permitting the patient to speak uninterrupted, summarizing what the patient said using their words, maintaining eye contact, active listening such as nodding, and asking clarifying questions. These common elements of good, person-centered, counseling, help build trust and patients’ engagement with care.
Actions of clinical care by type of opioid use and point of entry into care are described in Table 1. Specifically, across the top of Table 1 lists the type of opioid use such as illicit, maintenance treatment, and pain management and the point of patient entry including prenatal, triage, labor and delivery, and after delivery. Coordinate care (not hand-off care) with a pain or addiction medicine practitioner. Obstetric providers should ensure that referral agencies accept the patients insurance and are accessible.
Inform patients that neonatal abstinence syndrome, which occurs when a fetus is exposed to drugs, is an expected and treatable condition. Neonatal abstinence syndrome is characterized by hyperirritability of the central nervous system, dysfunction in the autonomic nervous system, gastrointestinal tract, and respiratory system. Discuss the signs and the anticipated maternal and newborn infant length of hospital stays.
If a patient is maintained on an opioid agonist, continue the maintenance and enhance pain management for acute needs. Pain management should be based on clinical assessment and not on the prescribed maintenance dose of medication.
There is a need to avoid partial agonist/antagonist intravenous treatments to reduce labor pain. Labor epidural or combined spinal/epidural forms of pain management typically works well. Practitioners should advise patients that the expectation of total pain control may be not achievable despite the use of analgesia due to increased pain sensitivity from long-term opioid use.
For patients who use illicit benzodiazepines (common in patients who use opioids), treatment to prevent benzodiazepine withdrawal may be indicated.
POSTPARTUM CARE
Breastfeeding is compatible with the low levels of methadone or buprenorphine that are present in breast milk.
The patient should be encouraged to postpone transitioning off opioid agonist or partial agonist treatments until she is living in a home that does not have drug-related activity, the infant sleeps through the night, breastfeeding is completed, and until she has built enough recovery resources (“recovery capital”) to help sustain remission. For some patients, long-term opioid agonist treatment may be best – scientific evidence, clinical needs, and patient motivation must all be considered in helping these patients maintain opioid abstinence.
Actions of Clinical Care by Type of Opioid Use (illicit, maintenance treatment, or pain management) and Point of Entry into Care.
WHY IS THIS STUDY IMPORTANT
This clinical opinion piece raised some key points regarding obstetric care for opioid using women during pregnancy and postpartum periods. The goal is to provide excellent healthcare to women who use opioids by increasing their willingness to seek and receive the needed medical and social support services.
OB-GYNs who acquire the knowledge, skills, and specialty support maximize their chances of providing high quality evidenced–based care to this growing population.
This is a clinical opinion piece, and is limited by its reliance on the expertise of the authors. In this case, the authors incorporated references to many peer-reviewed studies to both explain and support their clinical advice which mostly focused on the patient-provider relationship and the role of medications.
The opinion piece did not address ways to help facilitate patient participation in recovery supportive social networks and environments, such mutual help organizations, which are empirically shown to be associated with higher rates of treatment engagement and abstinence when used with medication.
NEXT STEPS
Given that both clinicians and patients have unanswered questions regarding the expected duration of pharmacological treatment, more research should be done to inform this question for pregnant and postpartum populations.
BOTTOM LINE
For individuals & families seeking recovery: This opinion piece reviewed clinical care issues for pregnant and postpartum women. It is important to have open communication with your provider and discuss any use of opioids so they can give you treatment options that best support the health of you, your fetus, and newborn.
For scientists: This clinical opinion article encourages OB-GYNs to screen for substance use disorders in pregnant and postpartum women and coordinate care when indicated. This population may have complex psychosocial and environmental factors or co-occurring psychiatric conditions. Although screening for substance use disorder is a well-developed test, more work could be done to help clinicians swiftly navigate and prioritize the maze of other factors that could be critical for the patient’s needs.
For policy makers: This opinion piece reviews clinical care issues that are related to illicit and prescribed opioid use among pregnant women and women in the postpartum period. The authors suggest that OB-GYNs have an ethical obligation to screen, assess, and provide a brief interventions and referral to treatment for patients with an opioid use disorder. Consider prioritizing policies and funding that motivate and facilitate obstetric providers to screen and coordinate care for pregnant and postpartum patients who use opioids.
For treatment professionals and treatment systems: This clinical opinion piece outlines major responsibilities of OB-GYNs who treat women who use opioids. Encourage your patients to seek regular obstetric care if they are pregnant. Treatment providers should coordinate care plans with OB-GYNs throughout the prenatal, labor and delivery, and postpartum periods to help support remission and recovery.
The opioid epidemic has resulted in hundreds of thousands of preventable deaths and has received national attention by the world’s most powerful political figures. Opioid use and opioid use disorder affects all walks of life including pregnant and postpartum women. The prevalence of opioid use disorder during pregnancy increased by 127%, from 1.7 per 1,000 delivery admissions in 1998 to 3.9 per 1,000 delivery admissions in 2011. More recently, almost 1% of pregnant women reported non-medical use of opioids in the past 30 days.
Pregnancy presents providers with a window of opportunity to screen for substance use disorders, offer brief intervention, and refer women to specialized treatment. In this clinical opinion piece, OB-GYNs (doctors who specialize in women’s health) with expertise in the treatment of opioid use disorder during pregnancy review clinical care issues associated with illicit and prescribed opioid use in the pregnant and postpartum period and outline the major responsibilities of OB-GYNs.
HOW WAS THIS STUDY CONDUCTED?
This summary highlights formal conclusions from the proceedings of the Expert Meeting on Perinatal Illicit Drug Abuse that was convened by the US Centers for Disease Control and Prevention (CDC).
WHAT DID THIS STUDY FIND?
This clinical opinion piece outlines the following points regarding clinical care issues that are related to opioid use and opioid use disorder in the prenatal, triage (emergency department), and postpartum phases of care.
PRENATAL CARE
Building rapport can enable useful communication in a population that may be reluctant to disclose their history. This can be done by permitting the patient to speak uninterrupted, summarizing what the patient said using their words, maintaining eye contact, active listening such as nodding, and asking clarifying questions. These common elements of good, person-centered, counseling, help build trust and patients’ engagement with care.
Actions of clinical care by type of opioid use and point of entry into care are described in Table 1. Specifically, across the top of Table 1 lists the type of opioid use such as illicit, maintenance treatment, and pain management and the point of patient entry including prenatal, triage, labor and delivery, and after delivery. Coordinate care (not hand-off care) with a pain or addiction medicine practitioner. Obstetric providers should ensure that referral agencies accept the patients insurance and are accessible.
Inform patients that neonatal abstinence syndrome, which occurs when a fetus is exposed to drugs, is an expected and treatable condition. Neonatal abstinence syndrome is characterized by hyperirritability of the central nervous system, dysfunction in the autonomic nervous system, gastrointestinal tract, and respiratory system. Discuss the signs and the anticipated maternal and newborn infant length of hospital stays.
If a patient is maintained on an opioid agonist, continue the maintenance and enhance pain management for acute needs. Pain management should be based on clinical assessment and not on the prescribed maintenance dose of medication.
There is a need to avoid partial agonist/antagonist intravenous treatments to reduce labor pain. Labor epidural or combined spinal/epidural forms of pain management typically works well. Practitioners should advise patients that the expectation of total pain control may be not achievable despite the use of analgesia due to increased pain sensitivity from long-term opioid use.
For patients who use illicit benzodiazepines (common in patients who use opioids), treatment to prevent benzodiazepine withdrawal may be indicated.
POSTPARTUM CARE
Breastfeeding is compatible with the low levels of methadone or buprenorphine that are present in breast milk.
The patient should be encouraged to postpone transitioning off opioid agonist or partial agonist treatments until she is living in a home that does not have drug-related activity, the infant sleeps through the night, breastfeeding is completed, and until she has built enough recovery resources (“recovery capital”) to help sustain remission. For some patients, long-term opioid agonist treatment may be best – scientific evidence, clinical needs, and patient motivation must all be considered in helping these patients maintain opioid abstinence.
Actions of Clinical Care by Type of Opioid Use (illicit, maintenance treatment, or pain management) and Point of Entry into Care.
WHY IS THIS STUDY IMPORTANT
This clinical opinion piece raised some key points regarding obstetric care for opioid using women during pregnancy and postpartum periods. The goal is to provide excellent healthcare to women who use opioids by increasing their willingness to seek and receive the needed medical and social support services.
OB-GYNs who acquire the knowledge, skills, and specialty support maximize their chances of providing high quality evidenced–based care to this growing population.
This is a clinical opinion piece, and is limited by its reliance on the expertise of the authors. In this case, the authors incorporated references to many peer-reviewed studies to both explain and support their clinical advice which mostly focused on the patient-provider relationship and the role of medications.
The opinion piece did not address ways to help facilitate patient participation in recovery supportive social networks and environments, such mutual help organizations, which are empirically shown to be associated with higher rates of treatment engagement and abstinence when used with medication.
NEXT STEPS
Given that both clinicians and patients have unanswered questions regarding the expected duration of pharmacological treatment, more research should be done to inform this question for pregnant and postpartum populations.
BOTTOM LINE
For individuals & families seeking recovery: This opinion piece reviewed clinical care issues for pregnant and postpartum women. It is important to have open communication with your provider and discuss any use of opioids so they can give you treatment options that best support the health of you, your fetus, and newborn.
For scientists: This clinical opinion article encourages OB-GYNs to screen for substance use disorders in pregnant and postpartum women and coordinate care when indicated. This population may have complex psychosocial and environmental factors or co-occurring psychiatric conditions. Although screening for substance use disorder is a well-developed test, more work could be done to help clinicians swiftly navigate and prioritize the maze of other factors that could be critical for the patient’s needs.
For policy makers: This opinion piece reviews clinical care issues that are related to illicit and prescribed opioid use among pregnant women and women in the postpartum period. The authors suggest that OB-GYNs have an ethical obligation to screen, assess, and provide a brief interventions and referral to treatment for patients with an opioid use disorder. Consider prioritizing policies and funding that motivate and facilitate obstetric providers to screen and coordinate care for pregnant and postpartum patients who use opioids.
For treatment professionals and treatment systems: This clinical opinion piece outlines major responsibilities of OB-GYNs who treat women who use opioids. Encourage your patients to seek regular obstetric care if they are pregnant. Treatment providers should coordinate care plans with OB-GYNs throughout the prenatal, labor and delivery, and postpartum periods to help support remission and recovery.