
It’s a Family Affair: Treatments for Parents to Increase Skill & Well-being
Parents of teens with substance use problems often experience a great deal of stress, which may, in turn, lead to less effective coping when faced with difficult situations. This study tested whether interventions designed specifically for parents can help increase their coping skills and decrease their levels of stress.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
When an individual has a substance use disorder, it can be a source of great stress for family and friends. For teens and young adults, perhaps no family member or friend experiences greater stress than their parents. Importantly though, studies have shown that family members, often called “concerned significant others”, can develop skills to react in helpful ways to their loved that makes it more likely for them to get into treatment. In addition to working with concerned significant others to help engage individuals in treatment, their mental health is an important target in its own right. In this study, McGillicuddy and colleagues tested an intervention designed to improve coping skills for parents and other guardians of teens with substance use problems who are not in treatment against family-focused 12-step facilitation (i.e., to Al-Anon and Nar-Anon).
HOW WAS THIS STUDY CONDUCTED?
Study authors randomized 85 parents and guardians (hereafter referred to as parents) of 12-21 year old individuals (17 years old, on average, hereafter referred to as teens) with substance use problems who had no treatment or mutual-help organization attendance in the past month to one of three groups: Coping Skills Treatment vs. 12-Step Facilitation vs. Delayed Treatment Control.
- MORE ON STUDY METHODS
-
The Coping Skills Treatment (n = 28) consisted of 12, weekly, 2-hour group sessions, focused on skill development in the context of role plays where participants practiced responding to several difficult situations with the teen (e.g., “Intoxicated adolescent returns home three hours past curfew”). This intervention neither encouraged nor discouraged attendance at 12-step groups, but rather couched it as one type of problem solving option for parents. The 12-Step Facilitation (n = 26) condition also consisted of 12, weekly, 2-hour group sessions, with goals of systematically encouraging parents to attend family-focused 12-step groups, like Al-Anon and Nar-Anon, and helping parents work through the first five of 12 steps, the theoretical, therapeutic plan of action to help parents reduce co-dependence (“preoccupation with, and extreme social and emotional dependence on another person”). The Delayed Treatment Control group (n = 31) had no contact with study staff over the 12-week treatment period, but received the Coping Skills Treatment after this 12-week study period.
A teen substance use problem was defined by: a) using substances 10 or more times in the past year and at least once in the past 3 months, and b) scoring above a cut-off indicating meaningful problems on either one of two questionnaires (e.g., substance “abuse” subscale of the Problem Oriented Screening Instrument for Parents).
Authors compared how individuals fared in the three groups on these four outcomes during the 12-week treatment (i.e., from study entry to post-treatment):
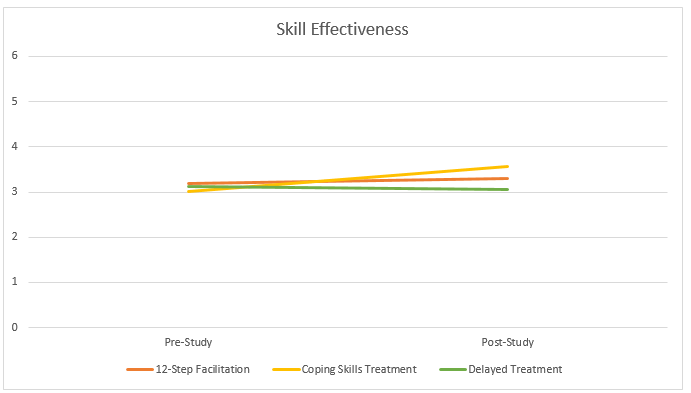
1) Coping skills based on the Parent Situation Inventory, a role play measure where parents are rated on the “effectiveness” of dealing with a situation, from 1 (not effective at all) to 6 (extremely effective)
2) Parent treatment/mutual help meeting attendance (yes or no)
3) Stress level based on the Stress Index for Parents of Adolescents
4) Parent subjective experience of adolescent substance-related problems based on percent of days that adolescent substance use caused a problem for the parent
Study authors re-measured parent stress and percent substance-related problem days at a 12-month follow-up. The parents were mostly female (85%). For 19 of 85 parents, they were part of a couple (i.e., co-parents) but only the parent who spent the most time with the teen counted toward statistical analyses.
WHAT DID THIS STUDY FIND?
As shown in the Figure below, parents receiving Coping Skills Treatment had a significantly larger increase from pre to post-treatment in coping skill effectiveness than those in 12-Step Facilitation, and both had larger increases than those in Delayed Treatment Control. Notably, however, scores in all three groups over time ranged between 3 and 4, on a scale from 1 to 6.
Those receiving 12-Step Facilitation were more likely to attend treatment or mutual-help organizations than both other groups though this difference did not reach statistical significance. All groups experienced similar stress reductions from the “clinically severe” to the lower end of the “clinically significant” range, improvements that were maintained through the 12-month follow-up assessment.
Both the Coping Skills Treatment and 12-step Facilitation groups had greater reductions in percent of parent problem days than the control group. These reductions were similar to each other- there were no treatment group differences-and the reductions were generally maintained 12-months later (see Figure)
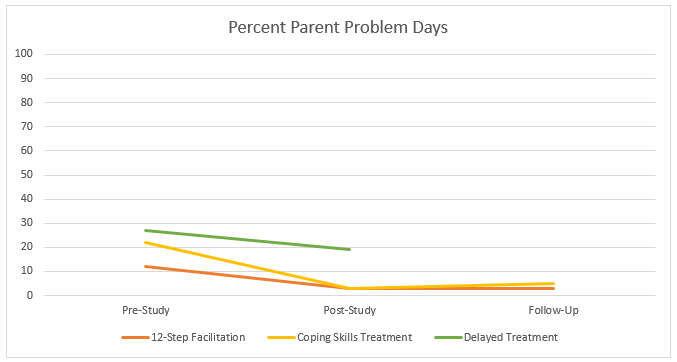
One additional, interesting finding is that when looking at how percent of parent problem days changed over time, in both treatment groups, there was a slight increase in problems initially that decreased steadily over time to well below initial problem levels.
WHY IS THIS STUDY IMPORTANT?
The most important finding from this study is that parents benefit from treatment geared toward their coping and well-being, when compared to no treatment. Regarding improvements in coping skills, however, it is unclear whether improving on a 1 to 6 scale, from an average of 3 to an average of 3.5, as was the case for parents receiving Coping Skills Treatment, is indicative of a meaningful “real-world” difference in addition to a statistically meaningful one. Moreover, this treatment was geared specifically to the assessment – that is, the treatment consisted of skill development specific to the Parent Situation Inventory. Even though authors used different versions of the assessment at post-test and pre-test (i.e., to reduce the likelihood that practice effects on the task were accounting for the improvement), this type of “teaching to the test” may not generalize to challenging situations outside intervention targets.
Overall, the study’s focus on parents of non-treatment seeking adolescents is important to add to the growing scientific literature on interventions for family members of adult (or young adult) individuals with substance-related problems. When the target is working with concerned significant others to engage a non-treatment-seeking loved one in care, Community Reinforcement and Family Training is an evidence-based option for both alcohol and other drugs, with generally 2-3 fold increases in the odds of treatment entry for loved ones, but, like this study, similar improvements in parental well-being, compared to family-focused 12-step facilitation interventions. Finally, for adolescents seeking treatment, it is important to note that adding a skills based component for parents may not provide additional benefit when added to contingency management delivered both at treatment and in the home on either adolescent substance use outcomes or parents’ skills.
- LIMITATIONS
-
- The sample size in this study was modest and replication studies in other settings with larger samples are needed.
NEXT STEPS
- Follow-up research can help determine whether skills improvements observed here translate into real-world improvements in parent skills and whether the Coping Skills Treatment helps parents reach their goals (e.g., improvements in adolescent health-seeking behaviors and day-to-day functioning).
- Because family-focused 12-step facilitation consistently shows similar benefit to behavior/skills focused interventions on parent well-being, more research is needed like this study by Timko and colleagues on the mechanisms by which these free community-based resources help improve family members’ well-being. Non-12-step mutual-help organizations for parents are also important to examine in this context, like Learn2Cope, an organization with meetings in New England and Florida.
BOTTOM LINE
- For individuals & families seeking recovery: For parents and other caregivers of teens with substance use problems, an intervention designed for parents to develop skills for addressing challenging situations may lead to improvements in these skills compared to no treatment. An intervention that systematically links you with family-focused mutual-help organizations, like Al-Anon or Nar-Anon, may help you reduce stress and perceived problems, just as much as the coping skills-based intervention. Both are likely to be better than no treatment at all.
- For scientists: The growing literature on family-focused interventions suggests that behavioral, skills-based interventions like the one tested here as well as Community Reinforcement and Family Training lead to better outcomes for the treatment target (e.g., parent skill or facilitating treatment seeking for a loved one). At the same time, they generally produce similar levels of parental well-being as family-focused 12-step interventions. Future research might examine mechanisms of these behavioral, skills-based interventions to understand why they may be producing similar well-being, but better target outcomes compared to 12-step interventions. In addition, future research might examine alcohol and other drug use among the identified patients (i.e., “loved ones”), particularly given recent data showing similar substance outcomes for Community Reinforcement and Family Training compared to 12-step facilitation, despite higher rates of facilitating treatment engagement.
- For policy makers: The growing literature on family-focused interventions suggests that behavioral, skills-based interventions like the one tested here as well as Community Reinforcement and Family Training lead to better outcomes for the treatment target (e.g., parent skill or facilitating treatment seeking for a loved one). At the same time, they generally produce similar levels of parental well-being as family-focused 12-step interventions. The field would benefit greatly from continued funding to help examine mechanisms of these family-focused interventions to understand why they may be producing similar well-being, but better target outcomes compared to 12-step interventions. Future research also can help determine whether such interventions are cost-effective.
- For treatment professionals and treatment systems: For parents and other caregivers of teens with substance-problems, an intervention designed for parents to develop skills for addressing challenging situations may lead to improvements in these skills compared to no treatment. An intervention that systematically links them with family-focus mutual-help organizations, like Al-Anon or Nar-Anon, may help them reduce stress and perceived problems, just as much as the coping skills-based intervention. Both are likely to be better than no treatment at all. Resources permitting, in adolescent treatment programs, adding groups specifically designed for parents that they can attend whether or not their teen is in treatment may be a valuable service.
CITATIONS
McGillicuddy, N. B., Rychtarik, R. G., & Papandonatos, G. D. (2015). Skill training versus 12-step facilitation for parents of substance-abusing teens. Journal of substance abuse treatment, 50, 11-17.
