WHAT PROBLEM DOES THIS STUDY ADDRESS?
Alcohol use disorder affects millions of Americans and contributes to more than $90 billion in annual healthcare costs, including frequent emergency department visits and hospitalizations. Despite the availability of FDA-approved medications for the condition – such as naltrexone, disulfiram, and acamprosate – fewer than 2% of individuals with alcohol use disorder receive them.
Hospitalization represents a potentially important window to initiate treatment, particularly for individuals who may not otherwise engage in outpatient care. While some studies suggest that starting medications for alcohol use disorder in hospital settings may be helpful, most have focused on short-term outcomes (e.g., within 30 days). It remains unclear how often medications for alcohol use disorder are initiated during hospital stays and whether doing so improves longer-term outcomes. This study examined how frequently these medications are used in hospitalized patients with alcohol use disorder in a large health system and whether receiving them is associated with fewer emergency department visits and hospital readmissions at 3 and 12 months after discharge.
HOW WAS THIS STUDY CONDUCTED?
This retrospective cohort study used electronic health record data from a large US hospital system between 2015 and 2023 and included 7,560 adults with documented medical history of alcohol use disorder. The study compared patients who received medication for alcohol use disorder (naltrexone, acamprosate, or disulfiram) during their hospital stay or at discharge (n = 259) to those who did not (n = 7,301). To make the groups more comparable, the study used a statistical approach called propensity score matching, which helps account for differences in patient characteristics that could influence outcomes (e.g., age, sex, race/ethnicity, co-occurring medical conditions). Using this approach, 131 patients who received medication were compared with a parallel group of 131 patients who did not receive medication. Patients were followed for up to 1 year after discharge, and outcomes included emergency department visits and hospital readmissions at 3 and 12 months.
Because this was an observational (non-randomized) study, the results cannot establish causality. In addition, relatively few patients received medication, which limits the ability to detect meaningful differences between groups. The study also could not determine whether patients were offered medication but declined, or the extent to which they took the medication after receiving it initially in the hospital, which may influence interpretation of the findings.
WHAT DID THIS STUDY FIND?
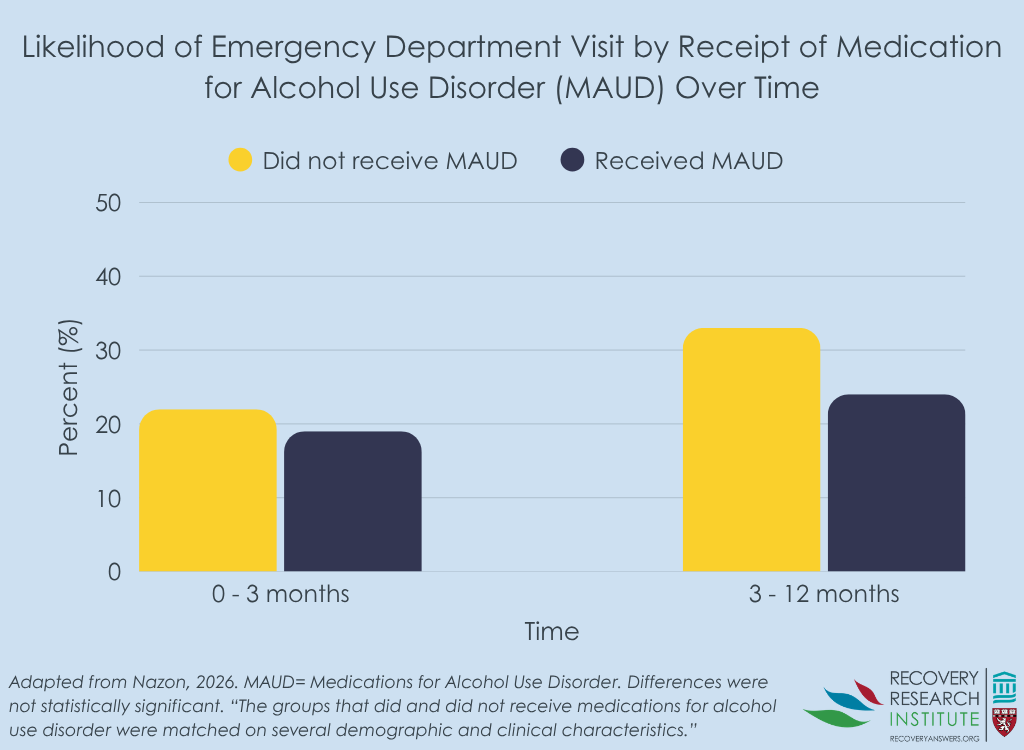
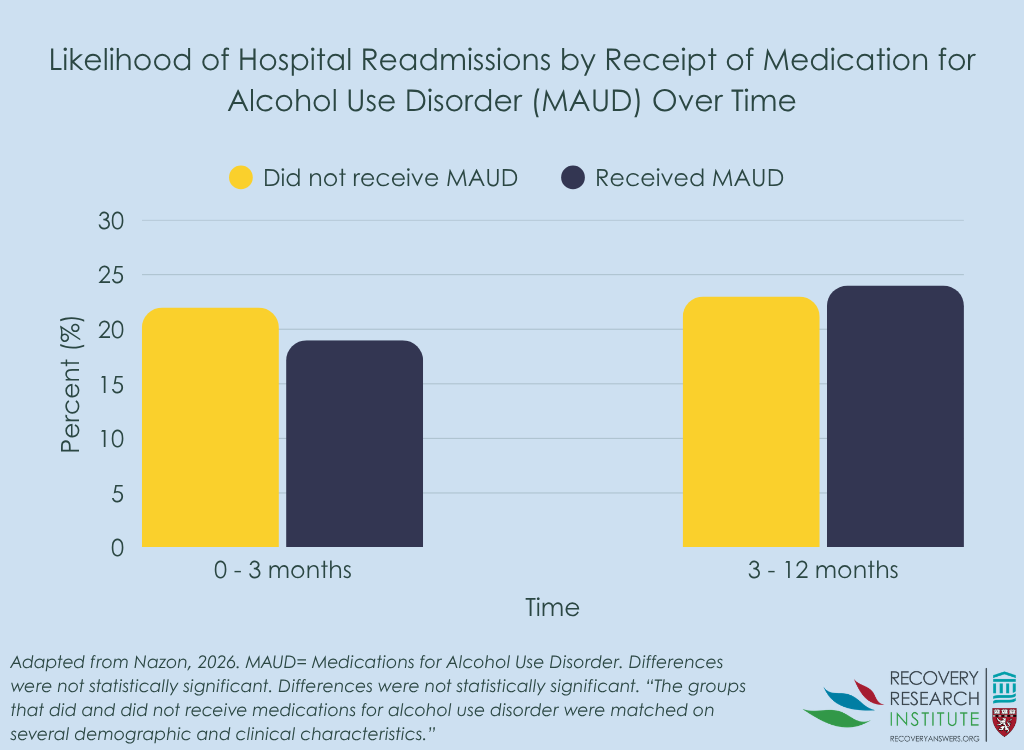
Medications for alcohol use disorder were rarely used during hospitalization, with only about 3% of hospitalized patients with alcohol use disorder receiving medication during their stay or at discharge. After matching 131 patients who received medication with 131 similar patients who did not, there were no significant differences in emergency departments visits or hospital readmissions at either 3 or 12 months after discharge. Although these differences were not statistically significant, outcomes generally trended in a more favorable direction for patients who received medication. These patients were slightly less likely to experience emergency department visits at both time points and hospital readmissions at 3-month follow-up, though patients receiving medication had roughly identical hospitalization rates to those who did not receive medication at 12 month follow-up (see graphs below). However, the small number of patients who received medication and the resulting uncertainty in the estimates make it difficult to draw firm conclusions. Additionally, as a single-site observational study, the findings may not generalize to other settings or and may not fully account for unmeasured differences between groups.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study highlights a substantial gap between evidence-based recommendations and real-world practice for alcohol use disorder. Despite evidence that medications for alcohol use disorder can reduce drinking and improve outcomes, they were rarely used during hospitalizations in this large health system. This finding aligns with broader research showing low use of these medications across healthcare settings, including emergency departments, where clinicians have reported barriers such as limited knowledge, discomfort prescribing these medications, and patient awareness gaps.
At the same time, this study did not find clear evidence that initiating medication during hospitalization reduced emergency department visits or readmissions over the following year. However, these findings should be interpreted cautiously given the small number of patients who received medication and the observational study design.
Prior studies with larger samples and in different settings have found that medications for alcohol use disorder can reduce alcohol use and decrease the risk of hospitalization, suggesting that the lack of strong effects observed here may reflect limited implementation rather than lack of benefit. Furthermore, studies tend to show that alcohol use disorder medications like naltrexone are only modestly helpful. Thus, larger samples would be needed to detect differences between individuals receiving and not receiving alcohol use disorder medication.
That said, hospitalization remains a promising but underutilized opportunity to initiate medication treatment for alcohol use disorder. Improving implementation will likely require system-level approaches, such as clinician training, standardized prescribing protocols, and better integration of addiction services (e.g., recovery coaches or care navigation), to increase access to these medications and better evaluate their impact in real-world settings. These medications also rely on continued use for their benefits so future studies would do well to examine effects of adherence to longer term use.
BOTTOM LINE
Findings indicate that medications for alcohol use disorder were rarely initiated during hospital stays within a large health system, highlighting a missed opportunity to improve care. Patients who received medication, however, did not have fewer post-discharge emergency department visits or hospital readmissions compared to those who did not. Importantly, the small number of patients receiving medications likely limited the ability to detect differences, and prior evidence suggests these medications can help reduce alcohol use and decrease the risk of hospitalization, making expanded access an important goal.
- For individuals and families seeking recovery: If you or a loved one is hospitalized and has concerns about alcohol use, consider asking about medications that can support recovery, as they are not always routinely offered. Trusted resources, such as the National Institute on Alcohol Abuse and Alcoholism, can provide additional information about these options.
- For treatment professionals and treatment systems: Hospitalization may be a key opportunity to initiate medications for alcohol use disorder, yet gaps in implementation persist. Increasing provider knowledge about medications for alcohol use disorder and developing streamlined prescribing processes may help improve access to these treatments.
- For scientists: Further research with larger, multi-site samples is needed to better understand the impact of initiating medications for alcohol use disorder during hospitalization and to identify effective implementation strategies.
- For policy makers: Low use of medications for alcohol use disorder during hospitalization suggests system-level barriers. Policies that support integration of addiction treatment into general medical care may help increase access to evidence-based treatments and reduce the broader healthcare burden of alcohol use.
CITATIONS
Nazon, M., Lavin, P., Pike, C. W., Greenway, K. T., Richard, J., L’Espérance, P., Ostacher, M., Jutras-Aswad, D., Tate, S., Lembke, A., & Garel, N. (2026). A missed opportunity: A retrospective cohort study of alcohol use disorder pharmacotherapy in hospitalized patients. Alcohol and Alcoholism, 61(2). doi: 10.1093/alcalc/agag008.













