Initiating extended-release naltrexone for alcohol use disorder in the emergency room
Emergency Department (ED) visits are prime opportunities to provide alcohol use disorder intervention and initiate pharmacotherapy. This study examined the feasibility of initiating extended-release injectable naltrexone with case management in the ED.
Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. From 2014 to 2018, 3.7 million ED visits were made by individuals with alcohol use disorder, accounting for nearly 4% of all ED visits. Over the last ten years, alcohol-related ED visits have increased by 47%.
At the same time, EDs are currently underutilized as settings to deliver alcohol use disorder interventions. In a national survey, 77% of ED directors reported that patients are “never” or “rarely” screened using a validated screening tool to assess current alcohol use, and only 9% offered brief behavioral interventions, even though EDs are commonly staffed with the skills to do so.
Evidence-supported treatment of alcohol use disorder consists of a combination of pharmacotherapy, behavioral treatments, and community recovery support groups, tailored to the individual. Naltrexone is one of 3 medications approved by the FDA for the treatment of alcohol use disorder. Unlike the other two FDA approved medications that either require abstinence (disulfiram/”Antabuse”) or recommend abstinence (acamprosate/”Campral”) before starting them and are intended to assist with maintaining abstinence, naltrexone can be initiated when patients are actively drinking and seeking to cut down, helping to reduce heavy drinking.
Many patients with alcohol use disorder may prefer a goal of reduced drinking rather than complete abstinence, making naltrexone particularly well-suited for use in the ED to help engage a broader array of individuals with a range of change goals. The extended-release injectable naltrexone may be especially helpful for individuals who don’t have as many resources to incorporate daily pill taking into their routine, such as those who are unstably housed.
Screening, Brief Intervention, and Referral to Treatment (often referred to as SBIRT) is commonly used to initiate substance use treatment for patients that come in contact with the health care system. While SBIRT for alcohol use disorder has had mixed results when delivered in the ED, the benefits of initiating pharmacotherapy for opioid and tobacco use disorder in the ED suggest a similar approach may be beneficial for those with alcohol use disorder too. This study evaluated the feasibility of ED-initiated extended-release naltrexone combined with case management for the treatment of alcohol use disorder and estimated the intervention’s impact on alcohol consumption and quality of life.
HOW WAS THIS STUDY CONDUCTED?
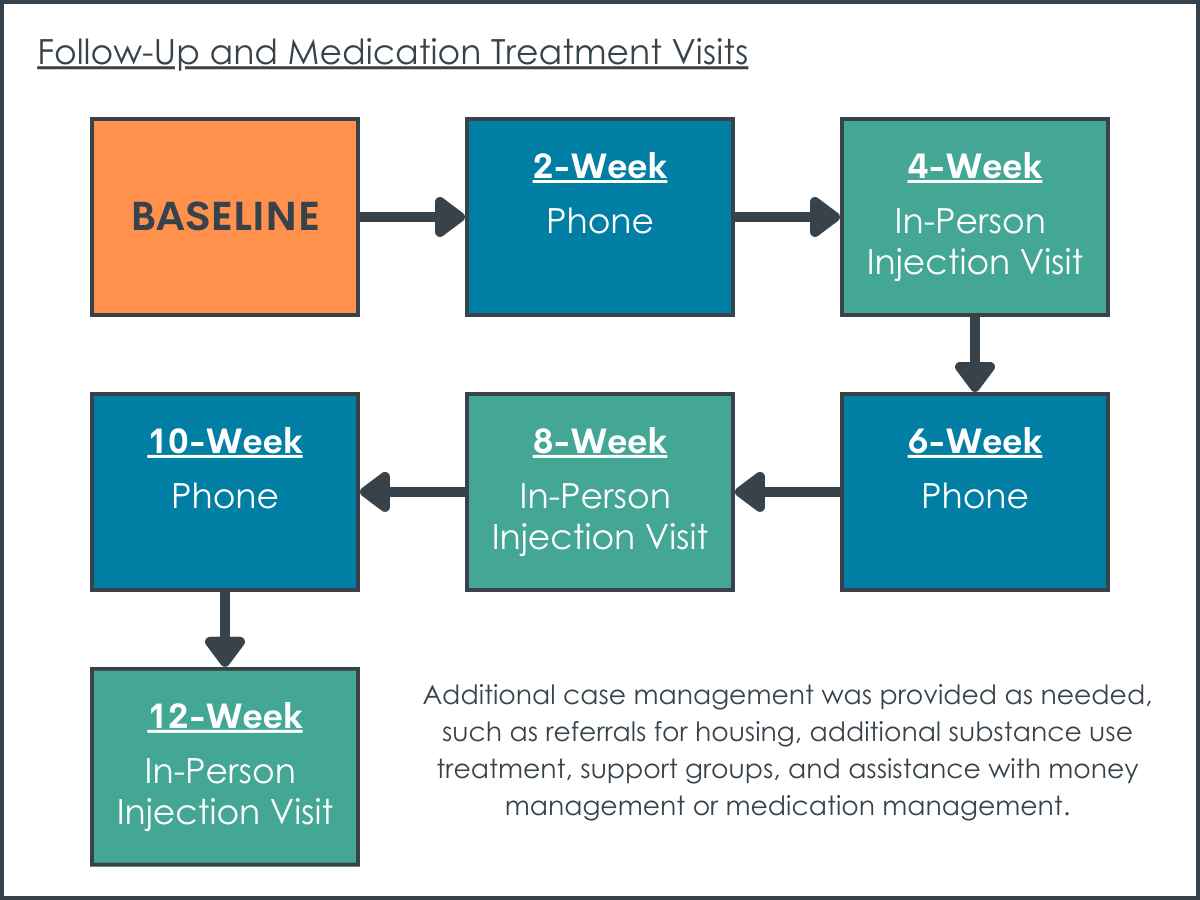
This study was a 12-week prospective open-label single-arm trial of the feasibility of initiating extended-release injectable naltrexone with case management for the treatment of alcohol use disorder in patients (N = 32) presenting to the emergency department (ED). Participants received three extended-release naltrexone injections (one at baseline when they presented to the ED, one at 4 weeks, and one at 8 weeks) combined with case management and were followed up for a total of 12 weeks. Participants were assessed every 2 weeks for current alcohol use, alcohol-related life consequences, quality of life, and World Health Organization (WHO) drinking risk level.
Participants were referred to the research case manager for screening by ED physicians and pharmacists. Patients could be visiting the ED for any reason; however, the researchers asked ED providers to refer patients whom they believed had alcohol use disorder based on their ED presentation. Potential participants could also be referred by ED pharmacists after medications were ordered to treat alcohol withdrawal. A desire to cut back or quit drinking was not an inclusion criterion. Participants were screened for eligibility during their ED visit using the AUDIT-C (a score of > 4), a commonly used brief screening measure of heavy alcohol use and possible alcohol use disorder, and also asked additional inclusion/exclusion criteria questions to ensure safety of administering naltrexone. This included additional laboratory testing (urinary drug screen and testing of liver enzymes and platelet count).
Participants who consented and met inclusion criteria received 15 minutes of motivational interviewing by the research case manager and encouragement to change drinking, were administered the extended-release injectable naltrexone, and scheduled to receive updated injections at 4 weeks and 8 weeks back at the ED. Participants were assessed every two weeks; assessments occurred in person on injection weeks and over the phone in non-injection weeks (baseline, 2 weeks [phone], 4 weeks [in person injection visit]; 6 weeks [phone], 8 weeks [in person injection visit], 10 weeks [phone], 12 weeks [phone]). Additional case management was provided as needed, such as referrals for housing, additional substance use treatment, support groups, and assistance with money management or medication management. Participants were compensated $20 per in person injection visit and provided a pre-paid cell phone if needed for communication with the research case manager.
Alcohol use, alcohol-related life consequences, quality of life, and demographic information and information about other substance use, mental health history, and legal history were obtained using commonly used and psychometrically validated questionnaires and interview procedures. Past medical history, medications, and allergies were obtained from the electronic medical records and verified with the patient at enrollment.
The analysis focused on the feasibility of the intervention, as well as changes to alcohol outcomes. Feasibility was measured by reporting the percentage of patients who enrolled, refused enrollment, completed the trial, and those who continued naltrexone after the trial completed. The analysis also tested changes in alcohol use, alcohol-related life consequences, and WHO drinking risk level from baseline to the 12-week follow-up. Because some participants were hospitalized during the 12-week trial, which would also affect drinking as access to alcohol would be much more difficult while admitted to the hospital, the researchers conducted a “sensitivity analysis” where they excluded the time the participants were hospitalized during the study period from their test of change in alcohol use. They found there were no significant differences in the results of the analysis when including or excluding days hospitalized on alcohol outcomes.
Out of 179 patients approached, 32 enrolled, and 23 completed all study visits. Most participants were White (72%), middle-aged (range 28 to 79 years old), and male (81%). The average alcohol use at baseline was 7.6 drinks per day and participants had also experienced a high number of alcohol-related life consequences. Participants had several clinically complicating factors. About one quarter of participants had a severe mental health diagnosis (e.g., bipolar disorder or schizophrenia), and about a third were unemployed and unstably housed. Half of participants used another substance like amphetamines, cocaine, or cannabis in addition to alcohol. Participants visited the ED for a range of reasons including: alcohol withdrawal (14 participants), alcohol intoxication (8 participants), falls (2 participants), suicidal ideations (2 participants), syncope, seizure not attributed to alcohol withdrawal, shoulder pain, vomiting, dyspnea, and cough (one participant each). Nine participants were admitted to the hospital. Among admitted participants, the median hospital length of stay was 2 days (range, 1 to 5 days). Eight were admitted for alcohol withdrawal and one was admitted for polysubstance drug overdose including alcohol. No participants were hospitalized in the 2 weeks before enrollment or in the final 2 weeks of the treatment period. Because the main analysis compares daily alcohol consumption in the 2 weeks before enrollment to the final 2 weeks of treatment, it is worth noting that the results were unchanged when analyzed according to days hospitalized.
WHAT DID THIS STUDY FIND?
Retention in the study was high, showing high feasibility of initiating extended-release injectable naltrexone with case management in the ED.
Few participants had missing follow-up data (2 patients withdrew, 3 were lost to follow-up), while 78% of participants attended all study visits and provided complete data, 72% of participants received all 3 injections, and 69% continued naltrexone through primary care after the study trial ended. It should be noted, however, that from the 179 patients that met the inclusion criteria of an AUDIT-C score greater than 4, just 55 agreed to the additional requisite screening tests. Patients (19 total) were excluded based on contraindications to initiating naltrexone (lab test results and planned major surgery) and 11% of eligible patients declined to enroll. Consequently, of all those patients who were screened, just 18% enrolled. The implications of this are described below in the, “What are the Implications of the Study Findings” section.
Significant improvements were seen in alcohol use, alcohol-related life consequences, and quality of life.
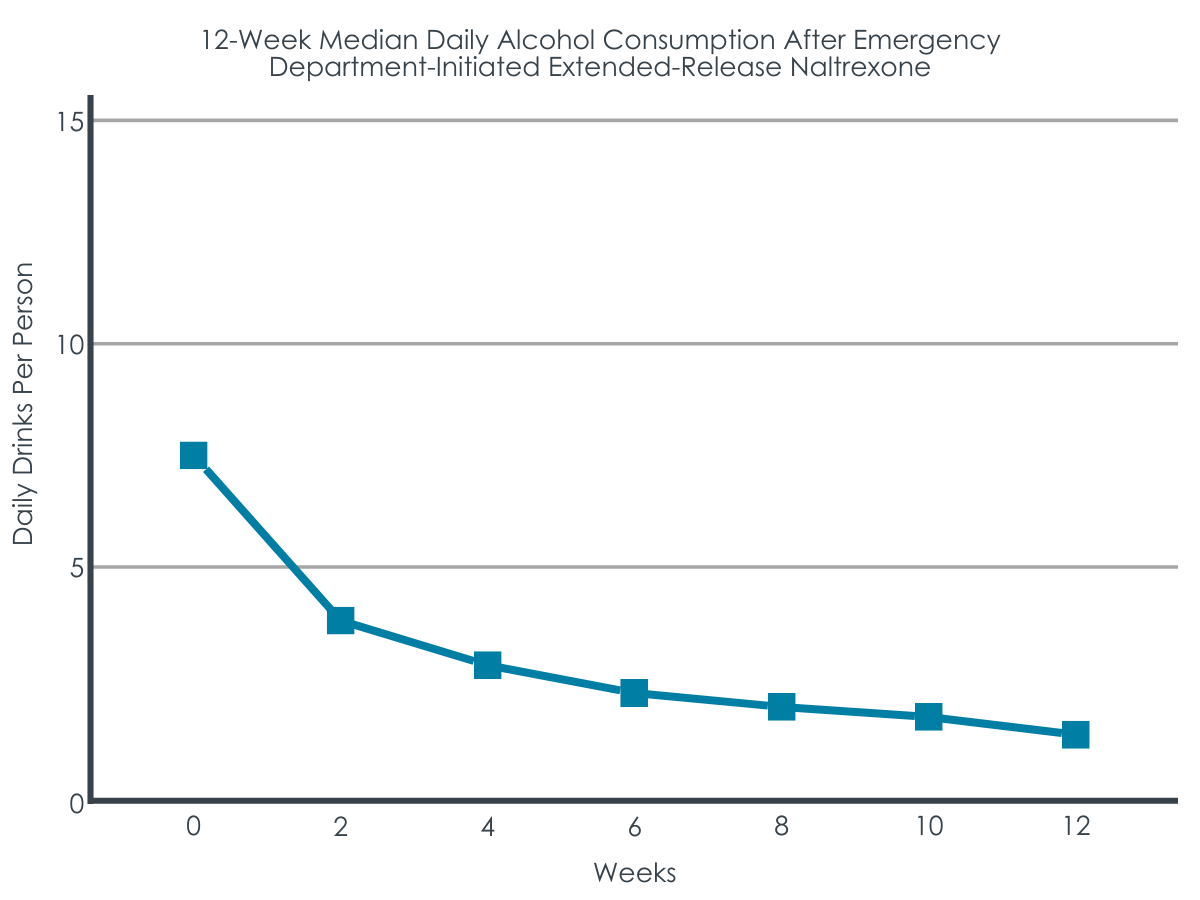
Participants on average went from drinking 7.6 drinks per day to 0 drinks per day, reduced their alcohol-related life consequences on average from 26 to 9 (scores of 30-45 and 23-29 indicate “Very High” and “High” levels of alcohol-related life consequences, respectively), reduced their WHO drinking risk level on average from “very high” to “low,” and improved their quality of life from 3.6 to 4.8 (7-point scale with higher scores indicating better quality of life).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that, among patients admitted to the ED who are willing to take extended-release naltrexone and receive case management for their alcohol use disorder, substantial therapeutic benefits may well be attainable. Specifically, the study found high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants.
While the results of this study are promising, experimental research, for example a randomized controlled trial, is needed to help determine whether the intervention may be causally related to the reductions in drinking. That said, it is worth noting retention in the study was high, with almost 72% of participants receiving all three injections.
This is particularly encouraging considering that a goal to cut down or stop drinking was not required, and many of the patients presented with medical and social complexity, such as unstable housing, co-occurring substance use disorders, and severe mental health disorders, which can introduce barriers to initiation and retention in care and treatment engagement.
Consistent with prior research showing that extended-release naltrexone may be preferred over daily buprenorphine to reduce opioid use among individuals unstably housed, this study shows that initiating extended-release injectable naltrexone in the ED for alcohol use is feasible with clinically complex patients.
Although retention in the trial was high, as alluded to above, it is also worth noting that only 18% of patients prescreened were enrolled in the study. Consistent with the general population of individuals with alcohol use disorder, this finding might also suggest individuals with alcohol use disorder presenting to the ED also have limited perceived need for, or interest in, engaging in treatment. Conversely, it is also possible that some patients would have accepted treatment were it not contingent on participating in a research study.
Of note, the rate of enrollment in this study is the same rate seen in a landmark trial of ED-initiated buprenorphine, which has since been successfully scaled to hundreds of academic, county, and community EDs. Also, the patients in this study were retained at higher levels than others where individuals were initiated on extended-release naltrexone in the ED. For example, in a retrospective analysis of patients visiting the ED from May-October 2020 in an urban, safety-net teaching hospital (i.e., patients were not part of a research study, instead the analysis examined outcomes in regular care), only 28% of patients initiated on naltrexone in the ED attended follow-up 4 weeks later, and 22% had reduced their daily alcohol consumption.
There are several possible reasons for the higher retention rate in the current study. First, patients willing to enroll in an alcohol use disorder research study may be more highly motivated to change their drinking than would be the case for those seeking any type of medical care in the ED. Also, the current study offered case management, which was not offered at the other hospital. It is possible that the case management services provided facilitated higher retention and reduced alcohol use. Most importantly, as part of participation in the research study, patients received $20 per naltrexone injection visit as incentive to remain enrolled. While it is common practice to compensate participants for their time completing assessments, pairing incentives with treatment visits may have had a therapeutic effect in and of itself, as this essentially describes a contingency management type paradigm – an evidence-supported intervention for substance use disorder. In contingency management interventions, patients receive a reward for meeting a treatment goal; for example, receiving cash or another prize in response to having a negative urine toxicology screen. $20 is a meaningful amount of money for most people and may be especially motivating for individuals unstably housed or unemployed.
The lack of a comparison group limits the ability to say whether the intervention actually caused the changes in drinking. Without a comparison, the researchers cannot rule out the possibility that fluctuations in alcohol use may have occurred naturally among the participants, independent of the study intervention. Participants being referred by ED providers also raises the possibility of selection bias, with participants being chosen because they were deemed likely to comply with follow-up visits and decrease their daily alcohol consumption.
The use of a research case manager to deliver the social/behavioral components of the intervention as well as collect outcome data could well have introduced bias into the study. Typically, intervention trials do not have interventionists conduct assessment so as to not unknowingly influence participant responses.
The intervention consisted of multiple components, including pharmacotherapy, motivational interviewing, and case management, financial incentives, and provision of a cell phone if needed. The relative contribution of each component to the study’s results cannot be determined.
Participants drinking was assessed using a brief screening measure; participants were not fully assessed for meeting alcohol use disorder criteria. Although participants self-reported baseline drinking was relatively high on average (7.6 drinks per day) and participants reported experiences a significant number of negative consequences from alcohol use (score of 26, scores of 30-45 and 23-29 indicate “Very High” and “High” levels of alcohol-related life consequences, respectively), because we don’t know if participants met criteria for alcohol use disorder, specifically (although it is very likely they did), the data do not necessarily support whether or not this intervention is feasible for patients presenting to the ED with alcohol use disorder.
BOTTOM LINE
This pilot study suggests that initiating treatment for alcohol use disorder with extended-release naltrexone and case management plus monetary incentives is a feasible and potentially helpful option in an emergency department setting. The study found high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants. While the results of this study are promising, experimental research, for example a randomized controlled trial, is needed along with independent researcher assessment of intervention outcome benefits to help determine whether the intervention actually caused the reductions in drinking.
For individuals and families seeking recovery: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Injectable naltrexone is a long-acting medication for the treatment of alcohol use disorder that could be initiated in the ED to help individuals currently drinking heavily reduce their alcohol use. Learn more about empirically-supported pharmacotherapies here.
For treatment professionals and treatment systems: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Extended-release injectable naltrexone given once every 4 weeks could be initiated in the ED to help reduce drinking, particularly for patients presenting to the ED with alcohol withdrawal or another alcohol-related problem and experience barriers to taking a daily pill. Learn more about empirically-supported pharmacotherapies here.
For scientists: This 12-week prospective open-label single-arm feasibility trial of extended-release injectable naltrexone with case management plus monetary incentives among patients presenting to an urban academic ED with likely alcohol use disorder (N = 32) showed high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants. This provides some promising evidence to test out further this set of interventions in a fully-powered randomized controlled trial with independent researcher assessment of clinical and functional outcomes. The intervention consisted of multiple components, including pharmacotherapy, motivational interviewing, and case management, financial incentives, and provision of a cell phone if needed, thus the relative contribution of each component to the study’s results cannot be determined. Additionally, the use of a research case manager to deliver the social/behavioral components of the intervention as well as collect outcome data could have introduced bias into the study. Finally, although participants drinking and alcohol-related problems were relatively high, participants were not fully assessed for meeting criteria for alcohol use disorder. Future studies testing the efficacy of this intervention should include assessment for alcohol use disorder criteria, have independent research staff separate from the case managers delivering the social/behavioral components of the intervention administer the assessments, and de-couple financial incentives from the injection visit or compare the effect of providing financial incentives at the injection visit to providing financial incentives at a separate assessment visit to determine if the financial incentive during the treatment visit helped account for any part of the therapeutic effect.
For policy makers: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Extended-release injectable naltrexone given once every 4 weeks could be initiated in the ED to help reduce drinking, particularly for patients presenting to the ED with alcohol withdrawal or another alcohol-related problem and experience barriers to taking a daily pill, eradicating the challenging issues of medication compliance. If policies required insurance and Medicaid to cover extended-release injectable naltrexone, this might help hospitals to implement this treatment in EDs for patients experiencing a high degree of social and medical complications. This in turn could well help some of the most complex and severely impacted alcohol use disorder patients and in turn reduce the burden on the health care system and reduce associated health care costs.
Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. From 2014 to 2018, 3.7 million ED visits were made by individuals with alcohol use disorder, accounting for nearly 4% of all ED visits. Over the last ten years, alcohol-related ED visits have increased by 47%.
At the same time, EDs are currently underutilized as settings to deliver alcohol use disorder interventions. In a national survey, 77% of ED directors reported that patients are “never” or “rarely” screened using a validated screening tool to assess current alcohol use, and only 9% offered brief behavioral interventions, even though EDs are commonly staffed with the skills to do so.
Evidence-supported treatment of alcohol use disorder consists of a combination of pharmacotherapy, behavioral treatments, and community recovery support groups, tailored to the individual. Naltrexone is one of 3 medications approved by the FDA for the treatment of alcohol use disorder. Unlike the other two FDA approved medications that either require abstinence (disulfiram/”Antabuse”) or recommend abstinence (acamprosate/”Campral”) before starting them and are intended to assist with maintaining abstinence, naltrexone can be initiated when patients are actively drinking and seeking to cut down, helping to reduce heavy drinking.
Many patients with alcohol use disorder may prefer a goal of reduced drinking rather than complete abstinence, making naltrexone particularly well-suited for use in the ED to help engage a broader array of individuals with a range of change goals. The extended-release injectable naltrexone may be especially helpful for individuals who don’t have as many resources to incorporate daily pill taking into their routine, such as those who are unstably housed.
Screening, Brief Intervention, and Referral to Treatment (often referred to as SBIRT) is commonly used to initiate substance use treatment for patients that come in contact with the health care system. While SBIRT for alcohol use disorder has had mixed results when delivered in the ED, the benefits of initiating pharmacotherapy for opioid and tobacco use disorder in the ED suggest a similar approach may be beneficial for those with alcohol use disorder too. This study evaluated the feasibility of ED-initiated extended-release naltrexone combined with case management for the treatment of alcohol use disorder and estimated the intervention’s impact on alcohol consumption and quality of life.
HOW WAS THIS STUDY CONDUCTED?
This study was a 12-week prospective open-label single-arm trial of the feasibility of initiating extended-release injectable naltrexone with case management for the treatment of alcohol use disorder in patients (N = 32) presenting to the emergency department (ED). Participants received three extended-release naltrexone injections (one at baseline when they presented to the ED, one at 4 weeks, and one at 8 weeks) combined with case management and were followed up for a total of 12 weeks. Participants were assessed every 2 weeks for current alcohol use, alcohol-related life consequences, quality of life, and World Health Organization (WHO) drinking risk level.
Participants were referred to the research case manager for screening by ED physicians and pharmacists. Patients could be visiting the ED for any reason; however, the researchers asked ED providers to refer patients whom they believed had alcohol use disorder based on their ED presentation. Potential participants could also be referred by ED pharmacists after medications were ordered to treat alcohol withdrawal. A desire to cut back or quit drinking was not an inclusion criterion. Participants were screened for eligibility during their ED visit using the AUDIT-C (a score of > 4), a commonly used brief screening measure of heavy alcohol use and possible alcohol use disorder, and also asked additional inclusion/exclusion criteria questions to ensure safety of administering naltrexone. This included additional laboratory testing (urinary drug screen and testing of liver enzymes and platelet count).
Participants who consented and met inclusion criteria received 15 minutes of motivational interviewing by the research case manager and encouragement to change drinking, were administered the extended-release injectable naltrexone, and scheduled to receive updated injections at 4 weeks and 8 weeks back at the ED. Participants were assessed every two weeks; assessments occurred in person on injection weeks and over the phone in non-injection weeks (baseline, 2 weeks [phone], 4 weeks [in person injection visit]; 6 weeks [phone], 8 weeks [in person injection visit], 10 weeks [phone], 12 weeks [phone]). Additional case management was provided as needed, such as referrals for housing, additional substance use treatment, support groups, and assistance with money management or medication management. Participants were compensated $20 per in person injection visit and provided a pre-paid cell phone if needed for communication with the research case manager.
Alcohol use, alcohol-related life consequences, quality of life, and demographic information and information about other substance use, mental health history, and legal history were obtained using commonly used and psychometrically validated questionnaires and interview procedures. Past medical history, medications, and allergies were obtained from the electronic medical records and verified with the patient at enrollment.
The analysis focused on the feasibility of the intervention, as well as changes to alcohol outcomes. Feasibility was measured by reporting the percentage of patients who enrolled, refused enrollment, completed the trial, and those who continued naltrexone after the trial completed. The analysis also tested changes in alcohol use, alcohol-related life consequences, and WHO drinking risk level from baseline to the 12-week follow-up. Because some participants were hospitalized during the 12-week trial, which would also affect drinking as access to alcohol would be much more difficult while admitted to the hospital, the researchers conducted a “sensitivity analysis” where they excluded the time the participants were hospitalized during the study period from their test of change in alcohol use. They found there were no significant differences in the results of the analysis when including or excluding days hospitalized on alcohol outcomes.
Out of 179 patients approached, 32 enrolled, and 23 completed all study visits. Most participants were White (72%), middle-aged (range 28 to 79 years old), and male (81%). The average alcohol use at baseline was 7.6 drinks per day and participants had also experienced a high number of alcohol-related life consequences. Participants had several clinically complicating factors. About one quarter of participants had a severe mental health diagnosis (e.g., bipolar disorder or schizophrenia), and about a third were unemployed and unstably housed. Half of participants used another substance like amphetamines, cocaine, or cannabis in addition to alcohol. Participants visited the ED for a range of reasons including: alcohol withdrawal (14 participants), alcohol intoxication (8 participants), falls (2 participants), suicidal ideations (2 participants), syncope, seizure not attributed to alcohol withdrawal, shoulder pain, vomiting, dyspnea, and cough (one participant each). Nine participants were admitted to the hospital. Among admitted participants, the median hospital length of stay was 2 days (range, 1 to 5 days). Eight were admitted for alcohol withdrawal and one was admitted for polysubstance drug overdose including alcohol. No participants were hospitalized in the 2 weeks before enrollment or in the final 2 weeks of the treatment period. Because the main analysis compares daily alcohol consumption in the 2 weeks before enrollment to the final 2 weeks of treatment, it is worth noting that the results were unchanged when analyzed according to days hospitalized.
WHAT DID THIS STUDY FIND?
Retention in the study was high, showing high feasibility of initiating extended-release injectable naltrexone with case management in the ED.
Few participants had missing follow-up data (2 patients withdrew, 3 were lost to follow-up), while 78% of participants attended all study visits and provided complete data, 72% of participants received all 3 injections, and 69% continued naltrexone through primary care after the study trial ended. It should be noted, however, that from the 179 patients that met the inclusion criteria of an AUDIT-C score greater than 4, just 55 agreed to the additional requisite screening tests. Patients (19 total) were excluded based on contraindications to initiating naltrexone (lab test results and planned major surgery) and 11% of eligible patients declined to enroll. Consequently, of all those patients who were screened, just 18% enrolled. The implications of this are described below in the, “What are the Implications of the Study Findings” section.
Significant improvements were seen in alcohol use, alcohol-related life consequences, and quality of life.
Participants on average went from drinking 7.6 drinks per day to 0 drinks per day, reduced their alcohol-related life consequences on average from 26 to 9 (scores of 30-45 and 23-29 indicate “Very High” and “High” levels of alcohol-related life consequences, respectively), reduced their WHO drinking risk level on average from “very high” to “low,” and improved their quality of life from 3.6 to 4.8 (7-point scale with higher scores indicating better quality of life).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that, among patients admitted to the ED who are willing to take extended-release naltrexone and receive case management for their alcohol use disorder, substantial therapeutic benefits may well be attainable. Specifically, the study found high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants.
While the results of this study are promising, experimental research, for example a randomized controlled trial, is needed to help determine whether the intervention may be causally related to the reductions in drinking. That said, it is worth noting retention in the study was high, with almost 72% of participants receiving all three injections.
This is particularly encouraging considering that a goal to cut down or stop drinking was not required, and many of the patients presented with medical and social complexity, such as unstable housing, co-occurring substance use disorders, and severe mental health disorders, which can introduce barriers to initiation and retention in care and treatment engagement.
Consistent with prior research showing that extended-release naltrexone may be preferred over daily buprenorphine to reduce opioid use among individuals unstably housed, this study shows that initiating extended-release injectable naltrexone in the ED for alcohol use is feasible with clinically complex patients.
Although retention in the trial was high, as alluded to above, it is also worth noting that only 18% of patients prescreened were enrolled in the study. Consistent with the general population of individuals with alcohol use disorder, this finding might also suggest individuals with alcohol use disorder presenting to the ED also have limited perceived need for, or interest in, engaging in treatment. Conversely, it is also possible that some patients would have accepted treatment were it not contingent on participating in a research study.
Of note, the rate of enrollment in this study is the same rate seen in a landmark trial of ED-initiated buprenorphine, which has since been successfully scaled to hundreds of academic, county, and community EDs. Also, the patients in this study were retained at higher levels than others where individuals were initiated on extended-release naltrexone in the ED. For example, in a retrospective analysis of patients visiting the ED from May-October 2020 in an urban, safety-net teaching hospital (i.e., patients were not part of a research study, instead the analysis examined outcomes in regular care), only 28% of patients initiated on naltrexone in the ED attended follow-up 4 weeks later, and 22% had reduced their daily alcohol consumption.
There are several possible reasons for the higher retention rate in the current study. First, patients willing to enroll in an alcohol use disorder research study may be more highly motivated to change their drinking than would be the case for those seeking any type of medical care in the ED. Also, the current study offered case management, which was not offered at the other hospital. It is possible that the case management services provided facilitated higher retention and reduced alcohol use. Most importantly, as part of participation in the research study, patients received $20 per naltrexone injection visit as incentive to remain enrolled. While it is common practice to compensate participants for their time completing assessments, pairing incentives with treatment visits may have had a therapeutic effect in and of itself, as this essentially describes a contingency management type paradigm – an evidence-supported intervention for substance use disorder. In contingency management interventions, patients receive a reward for meeting a treatment goal; for example, receiving cash or another prize in response to having a negative urine toxicology screen. $20 is a meaningful amount of money for most people and may be especially motivating for individuals unstably housed or unemployed.
The lack of a comparison group limits the ability to say whether the intervention actually caused the changes in drinking. Without a comparison, the researchers cannot rule out the possibility that fluctuations in alcohol use may have occurred naturally among the participants, independent of the study intervention. Participants being referred by ED providers also raises the possibility of selection bias, with participants being chosen because they were deemed likely to comply with follow-up visits and decrease their daily alcohol consumption.
The use of a research case manager to deliver the social/behavioral components of the intervention as well as collect outcome data could well have introduced bias into the study. Typically, intervention trials do not have interventionists conduct assessment so as to not unknowingly influence participant responses.
The intervention consisted of multiple components, including pharmacotherapy, motivational interviewing, and case management, financial incentives, and provision of a cell phone if needed. The relative contribution of each component to the study’s results cannot be determined.
Participants drinking was assessed using a brief screening measure; participants were not fully assessed for meeting alcohol use disorder criteria. Although participants self-reported baseline drinking was relatively high on average (7.6 drinks per day) and participants reported experiences a significant number of negative consequences from alcohol use (score of 26, scores of 30-45 and 23-29 indicate “Very High” and “High” levels of alcohol-related life consequences, respectively), because we don’t know if participants met criteria for alcohol use disorder, specifically (although it is very likely they did), the data do not necessarily support whether or not this intervention is feasible for patients presenting to the ED with alcohol use disorder.
BOTTOM LINE
This pilot study suggests that initiating treatment for alcohol use disorder with extended-release naltrexone and case management plus monetary incentives is a feasible and potentially helpful option in an emergency department setting. The study found high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants. While the results of this study are promising, experimental research, for example a randomized controlled trial, is needed along with independent researcher assessment of intervention outcome benefits to help determine whether the intervention actually caused the reductions in drinking.
For individuals and families seeking recovery: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Injectable naltrexone is a long-acting medication for the treatment of alcohol use disorder that could be initiated in the ED to help individuals currently drinking heavily reduce their alcohol use. Learn more about empirically-supported pharmacotherapies here.
For treatment professionals and treatment systems: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Extended-release injectable naltrexone given once every 4 weeks could be initiated in the ED to help reduce drinking, particularly for patients presenting to the ED with alcohol withdrawal or another alcohol-related problem and experience barriers to taking a daily pill. Learn more about empirically-supported pharmacotherapies here.
For scientists: This 12-week prospective open-label single-arm feasibility trial of extended-release injectable naltrexone with case management plus monetary incentives among patients presenting to an urban academic ED with likely alcohol use disorder (N = 32) showed high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants. This provides some promising evidence to test out further this set of interventions in a fully-powered randomized controlled trial with independent researcher assessment of clinical and functional outcomes. The intervention consisted of multiple components, including pharmacotherapy, motivational interviewing, and case management, financial incentives, and provision of a cell phone if needed, thus the relative contribution of each component to the study’s results cannot be determined. Additionally, the use of a research case manager to deliver the social/behavioral components of the intervention as well as collect outcome data could have introduced bias into the study. Finally, although participants drinking and alcohol-related problems were relatively high, participants were not fully assessed for meeting criteria for alcohol use disorder. Future studies testing the efficacy of this intervention should include assessment for alcohol use disorder criteria, have independent research staff separate from the case managers delivering the social/behavioral components of the intervention administer the assessments, and de-couple financial incentives from the injection visit or compare the effect of providing financial incentives at the injection visit to providing financial incentives at a separate assessment visit to determine if the financial incentive during the treatment visit helped account for any part of the therapeutic effect.
For policy makers: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Extended-release injectable naltrexone given once every 4 weeks could be initiated in the ED to help reduce drinking, particularly for patients presenting to the ED with alcohol withdrawal or another alcohol-related problem and experience barriers to taking a daily pill, eradicating the challenging issues of medication compliance. If policies required insurance and Medicaid to cover extended-release injectable naltrexone, this might help hospitals to implement this treatment in EDs for patients experiencing a high degree of social and medical complications. This in turn could well help some of the most complex and severely impacted alcohol use disorder patients and in turn reduce the burden on the health care system and reduce associated health care costs.
Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. From 2014 to 2018, 3.7 million ED visits were made by individuals with alcohol use disorder, accounting for nearly 4% of all ED visits. Over the last ten years, alcohol-related ED visits have increased by 47%.
At the same time, EDs are currently underutilized as settings to deliver alcohol use disorder interventions. In a national survey, 77% of ED directors reported that patients are “never” or “rarely” screened using a validated screening tool to assess current alcohol use, and only 9% offered brief behavioral interventions, even though EDs are commonly staffed with the skills to do so.
Evidence-supported treatment of alcohol use disorder consists of a combination of pharmacotherapy, behavioral treatments, and community recovery support groups, tailored to the individual. Naltrexone is one of 3 medications approved by the FDA for the treatment of alcohol use disorder. Unlike the other two FDA approved medications that either require abstinence (disulfiram/”Antabuse”) or recommend abstinence (acamprosate/”Campral”) before starting them and are intended to assist with maintaining abstinence, naltrexone can be initiated when patients are actively drinking and seeking to cut down, helping to reduce heavy drinking.
Many patients with alcohol use disorder may prefer a goal of reduced drinking rather than complete abstinence, making naltrexone particularly well-suited for use in the ED to help engage a broader array of individuals with a range of change goals. The extended-release injectable naltrexone may be especially helpful for individuals who don’t have as many resources to incorporate daily pill taking into their routine, such as those who are unstably housed.
Screening, Brief Intervention, and Referral to Treatment (often referred to as SBIRT) is commonly used to initiate substance use treatment for patients that come in contact with the health care system. While SBIRT for alcohol use disorder has had mixed results when delivered in the ED, the benefits of initiating pharmacotherapy for opioid and tobacco use disorder in the ED suggest a similar approach may be beneficial for those with alcohol use disorder too. This study evaluated the feasibility of ED-initiated extended-release naltrexone combined with case management for the treatment of alcohol use disorder and estimated the intervention’s impact on alcohol consumption and quality of life.
HOW WAS THIS STUDY CONDUCTED?
This study was a 12-week prospective open-label single-arm trial of the feasibility of initiating extended-release injectable naltrexone with case management for the treatment of alcohol use disorder in patients (N = 32) presenting to the emergency department (ED). Participants received three extended-release naltrexone injections (one at baseline when they presented to the ED, one at 4 weeks, and one at 8 weeks) combined with case management and were followed up for a total of 12 weeks. Participants were assessed every 2 weeks for current alcohol use, alcohol-related life consequences, quality of life, and World Health Organization (WHO) drinking risk level.
Participants were referred to the research case manager for screening by ED physicians and pharmacists. Patients could be visiting the ED for any reason; however, the researchers asked ED providers to refer patients whom they believed had alcohol use disorder based on their ED presentation. Potential participants could also be referred by ED pharmacists after medications were ordered to treat alcohol withdrawal. A desire to cut back or quit drinking was not an inclusion criterion. Participants were screened for eligibility during their ED visit using the AUDIT-C (a score of > 4), a commonly used brief screening measure of heavy alcohol use and possible alcohol use disorder, and also asked additional inclusion/exclusion criteria questions to ensure safety of administering naltrexone. This included additional laboratory testing (urinary drug screen and testing of liver enzymes and platelet count).
Participants who consented and met inclusion criteria received 15 minutes of motivational interviewing by the research case manager and encouragement to change drinking, were administered the extended-release injectable naltrexone, and scheduled to receive updated injections at 4 weeks and 8 weeks back at the ED. Participants were assessed every two weeks; assessments occurred in person on injection weeks and over the phone in non-injection weeks (baseline, 2 weeks [phone], 4 weeks [in person injection visit]; 6 weeks [phone], 8 weeks [in person injection visit], 10 weeks [phone], 12 weeks [phone]). Additional case management was provided as needed, such as referrals for housing, additional substance use treatment, support groups, and assistance with money management or medication management. Participants were compensated $20 per in person injection visit and provided a pre-paid cell phone if needed for communication with the research case manager.
Alcohol use, alcohol-related life consequences, quality of life, and demographic information and information about other substance use, mental health history, and legal history were obtained using commonly used and psychometrically validated questionnaires and interview procedures. Past medical history, medications, and allergies were obtained from the electronic medical records and verified with the patient at enrollment.
The analysis focused on the feasibility of the intervention, as well as changes to alcohol outcomes. Feasibility was measured by reporting the percentage of patients who enrolled, refused enrollment, completed the trial, and those who continued naltrexone after the trial completed. The analysis also tested changes in alcohol use, alcohol-related life consequences, and WHO drinking risk level from baseline to the 12-week follow-up. Because some participants were hospitalized during the 12-week trial, which would also affect drinking as access to alcohol would be much more difficult while admitted to the hospital, the researchers conducted a “sensitivity analysis” where they excluded the time the participants were hospitalized during the study period from their test of change in alcohol use. They found there were no significant differences in the results of the analysis when including or excluding days hospitalized on alcohol outcomes.
Out of 179 patients approached, 32 enrolled, and 23 completed all study visits. Most participants were White (72%), middle-aged (range 28 to 79 years old), and male (81%). The average alcohol use at baseline was 7.6 drinks per day and participants had also experienced a high number of alcohol-related life consequences. Participants had several clinically complicating factors. About one quarter of participants had a severe mental health diagnosis (e.g., bipolar disorder or schizophrenia), and about a third were unemployed and unstably housed. Half of participants used another substance like amphetamines, cocaine, or cannabis in addition to alcohol. Participants visited the ED for a range of reasons including: alcohol withdrawal (14 participants), alcohol intoxication (8 participants), falls (2 participants), suicidal ideations (2 participants), syncope, seizure not attributed to alcohol withdrawal, shoulder pain, vomiting, dyspnea, and cough (one participant each). Nine participants were admitted to the hospital. Among admitted participants, the median hospital length of stay was 2 days (range, 1 to 5 days). Eight were admitted for alcohol withdrawal and one was admitted for polysubstance drug overdose including alcohol. No participants were hospitalized in the 2 weeks before enrollment or in the final 2 weeks of the treatment period. Because the main analysis compares daily alcohol consumption in the 2 weeks before enrollment to the final 2 weeks of treatment, it is worth noting that the results were unchanged when analyzed according to days hospitalized.
WHAT DID THIS STUDY FIND?
Retention in the study was high, showing high feasibility of initiating extended-release injectable naltrexone with case management in the ED.
Few participants had missing follow-up data (2 patients withdrew, 3 were lost to follow-up), while 78% of participants attended all study visits and provided complete data, 72% of participants received all 3 injections, and 69% continued naltrexone through primary care after the study trial ended. It should be noted, however, that from the 179 patients that met the inclusion criteria of an AUDIT-C score greater than 4, just 55 agreed to the additional requisite screening tests. Patients (19 total) were excluded based on contraindications to initiating naltrexone (lab test results and planned major surgery) and 11% of eligible patients declined to enroll. Consequently, of all those patients who were screened, just 18% enrolled. The implications of this are described below in the, “What are the Implications of the Study Findings” section.
Significant improvements were seen in alcohol use, alcohol-related life consequences, and quality of life.
Participants on average went from drinking 7.6 drinks per day to 0 drinks per day, reduced their alcohol-related life consequences on average from 26 to 9 (scores of 30-45 and 23-29 indicate “Very High” and “High” levels of alcohol-related life consequences, respectively), reduced their WHO drinking risk level on average from “very high” to “low,” and improved their quality of life from 3.6 to 4.8 (7-point scale with higher scores indicating better quality of life).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study suggests that, among patients admitted to the ED who are willing to take extended-release naltrexone and receive case management for their alcohol use disorder, substantial therapeutic benefits may well be attainable. Specifically, the study found high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants.
While the results of this study are promising, experimental research, for example a randomized controlled trial, is needed to help determine whether the intervention may be causally related to the reductions in drinking. That said, it is worth noting retention in the study was high, with almost 72% of participants receiving all three injections.
This is particularly encouraging considering that a goal to cut down or stop drinking was not required, and many of the patients presented with medical and social complexity, such as unstable housing, co-occurring substance use disorders, and severe mental health disorders, which can introduce barriers to initiation and retention in care and treatment engagement.
Consistent with prior research showing that extended-release naltrexone may be preferred over daily buprenorphine to reduce opioid use among individuals unstably housed, this study shows that initiating extended-release injectable naltrexone in the ED for alcohol use is feasible with clinically complex patients.
Although retention in the trial was high, as alluded to above, it is also worth noting that only 18% of patients prescreened were enrolled in the study. Consistent with the general population of individuals with alcohol use disorder, this finding might also suggest individuals with alcohol use disorder presenting to the ED also have limited perceived need for, or interest in, engaging in treatment. Conversely, it is also possible that some patients would have accepted treatment were it not contingent on participating in a research study.
Of note, the rate of enrollment in this study is the same rate seen in a landmark trial of ED-initiated buprenorphine, which has since been successfully scaled to hundreds of academic, county, and community EDs. Also, the patients in this study were retained at higher levels than others where individuals were initiated on extended-release naltrexone in the ED. For example, in a retrospective analysis of patients visiting the ED from May-October 2020 in an urban, safety-net teaching hospital (i.e., patients were not part of a research study, instead the analysis examined outcomes in regular care), only 28% of patients initiated on naltrexone in the ED attended follow-up 4 weeks later, and 22% had reduced their daily alcohol consumption.
There are several possible reasons for the higher retention rate in the current study. First, patients willing to enroll in an alcohol use disorder research study may be more highly motivated to change their drinking than would be the case for those seeking any type of medical care in the ED. Also, the current study offered case management, which was not offered at the other hospital. It is possible that the case management services provided facilitated higher retention and reduced alcohol use. Most importantly, as part of participation in the research study, patients received $20 per naltrexone injection visit as incentive to remain enrolled. While it is common practice to compensate participants for their time completing assessments, pairing incentives with treatment visits may have had a therapeutic effect in and of itself, as this essentially describes a contingency management type paradigm – an evidence-supported intervention for substance use disorder. In contingency management interventions, patients receive a reward for meeting a treatment goal; for example, receiving cash or another prize in response to having a negative urine toxicology screen. $20 is a meaningful amount of money for most people and may be especially motivating for individuals unstably housed or unemployed.
The lack of a comparison group limits the ability to say whether the intervention actually caused the changes in drinking. Without a comparison, the researchers cannot rule out the possibility that fluctuations in alcohol use may have occurred naturally among the participants, independent of the study intervention. Participants being referred by ED providers also raises the possibility of selection bias, with participants being chosen because they were deemed likely to comply with follow-up visits and decrease their daily alcohol consumption.
The use of a research case manager to deliver the social/behavioral components of the intervention as well as collect outcome data could well have introduced bias into the study. Typically, intervention trials do not have interventionists conduct assessment so as to not unknowingly influence participant responses.
The intervention consisted of multiple components, including pharmacotherapy, motivational interviewing, and case management, financial incentives, and provision of a cell phone if needed. The relative contribution of each component to the study’s results cannot be determined.
Participants drinking was assessed using a brief screening measure; participants were not fully assessed for meeting alcohol use disorder criteria. Although participants self-reported baseline drinking was relatively high on average (7.6 drinks per day) and participants reported experiences a significant number of negative consequences from alcohol use (score of 26, scores of 30-45 and 23-29 indicate “Very High” and “High” levels of alcohol-related life consequences, respectively), because we don’t know if participants met criteria for alcohol use disorder, specifically (although it is very likely they did), the data do not necessarily support whether or not this intervention is feasible for patients presenting to the ED with alcohol use disorder.
BOTTOM LINE
This pilot study suggests that initiating treatment for alcohol use disorder with extended-release naltrexone and case management plus monetary incentives is a feasible and potentially helpful option in an emergency department setting. The study found high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants. While the results of this study are promising, experimental research, for example a randomized controlled trial, is needed along with independent researcher assessment of intervention outcome benefits to help determine whether the intervention actually caused the reductions in drinking.
For individuals and families seeking recovery: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Injectable naltrexone is a long-acting medication for the treatment of alcohol use disorder that could be initiated in the ED to help individuals currently drinking heavily reduce their alcohol use. Learn more about empirically-supported pharmacotherapies here.
For treatment professionals and treatment systems: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Extended-release injectable naltrexone given once every 4 weeks could be initiated in the ED to help reduce drinking, particularly for patients presenting to the ED with alcohol withdrawal or another alcohol-related problem and experience barriers to taking a daily pill. Learn more about empirically-supported pharmacotherapies here.
For scientists: This 12-week prospective open-label single-arm feasibility trial of extended-release injectable naltrexone with case management plus monetary incentives among patients presenting to an urban academic ED with likely alcohol use disorder (N = 32) showed high levels of treatment retention and significant reductions in self-reported alcohol use, improved quality of life, and fewer alcohol-related consequences for participants. This provides some promising evidence to test out further this set of interventions in a fully-powered randomized controlled trial with independent researcher assessment of clinical and functional outcomes. The intervention consisted of multiple components, including pharmacotherapy, motivational interviewing, and case management, financial incentives, and provision of a cell phone if needed, thus the relative contribution of each component to the study’s results cannot be determined. Additionally, the use of a research case manager to deliver the social/behavioral components of the intervention as well as collect outcome data could have introduced bias into the study. Finally, although participants drinking and alcohol-related problems were relatively high, participants were not fully assessed for meeting criteria for alcohol use disorder. Future studies testing the efficacy of this intervention should include assessment for alcohol use disorder criteria, have independent research staff separate from the case managers delivering the social/behavioral components of the intervention administer the assessments, and de-couple financial incentives from the injection visit or compare the effect of providing financial incentives at the injection visit to providing financial incentives at a separate assessment visit to determine if the financial incentive during the treatment visit helped account for any part of the therapeutic effect.
For policy makers: Emergency department (ED) visits are opportunities to initiate treatment for alcohol use disorder, such as pharmacotherapy, to reduce drinking. EDs treat many patients that present with alcohol-related harms and, for many with alcohol use disorder, serve as the primary point of contact to the health care system. Extended-release injectable naltrexone given once every 4 weeks could be initiated in the ED to help reduce drinking, particularly for patients presenting to the ED with alcohol withdrawal or another alcohol-related problem and experience barriers to taking a daily pill, eradicating the challenging issues of medication compliance. If policies required insurance and Medicaid to cover extended-release injectable naltrexone, this might help hospitals to implement this treatment in EDs for patients experiencing a high degree of social and medical complications. This in turn could well help some of the most complex and severely impacted alcohol use disorder patients and in turn reduce the burden on the health care system and reduce associated health care costs.