Effects of alcohol policy interventions on alcohol consumption
Alcohol use is associated with increased risks for cancer and other diseases, as well as mental health conditions and social harms. Policy interventions can help reduce consumption and thereby address associated public health harms. This article summarized key findings.
Given the associations between alcohol consumption and these numerous harms, interventions are needed to reduce consumption. The International Agency for Research on Cancer created the Handbooks of Cancer Prevention Program, for which the Working Group developed a 2-part volume about the primary prevention of alcohol-related cancers. In the first volume (Volume 20A), the Working Group evaluated studies that examined the association between cessation of alcohol consumption and alcohol-related cancers. Following their evaluation, they concluded that there is sufficient evidence that reducing or quitting alcohol use reduces the risk of alcohol-related cancer.
In the second volume (Volume 20B), the Working Group evaluated studies that examined the effects of policy interventions that aimed to reduce alcohol consumption. Their key findings are summarized in this review article. Such findings can shed light on which alcohol policy interventions are effective at reducing alcohol consumption, thereby informing future policymaking efforts, reducing the risks of alcohol-related harms, and improving public health.
HOW WAS THIS STUDY CONDUCTED?
The International Agency for Research on Cancer Working Group conducted a literature review of studies examining alcohol policy interventions. The strength of the studies’ evidence to reduce alcohol consumption was qualitatively evaluated.
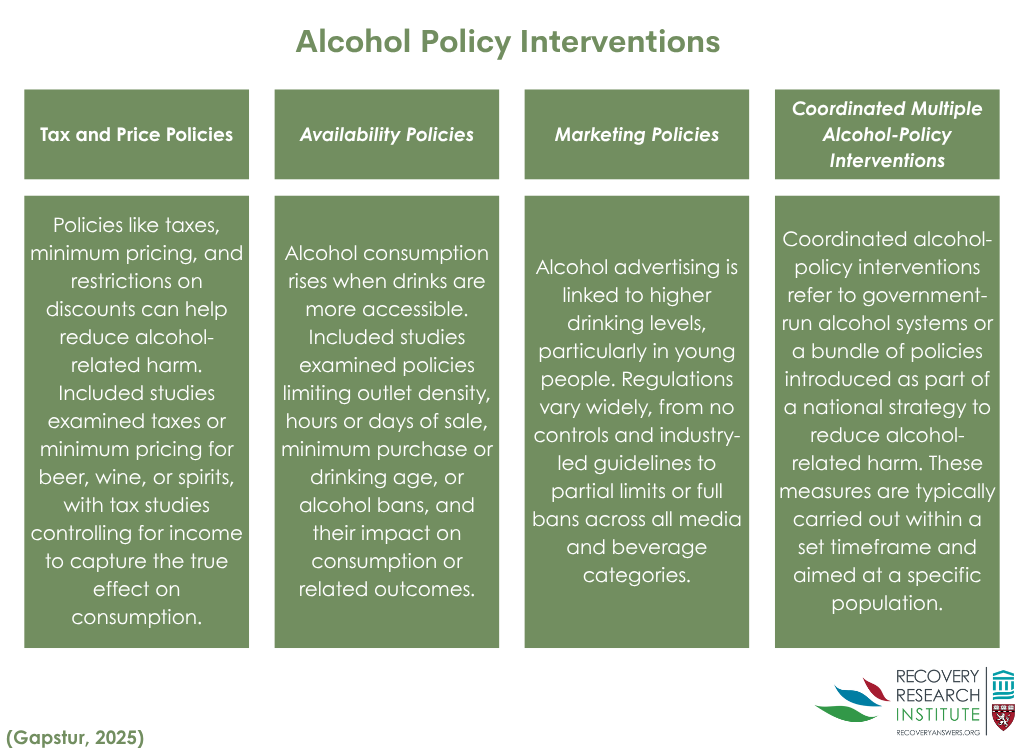
Studies were included if they were published and described empirical data on alcohol policy interventions that examined changes in alcohol consumption (i.e., beer, wine, and spirits). Interventions were chosen that aimed to reduce alcohol consumption at the national or subnational level. These included 20 studies that assessed tax and price policies, 39 studies that assessed alcohol availability policies, 4 studies that assessed marketing policies, and 20 studies that assessed government monopolies or coordinated multiple interventions. See graphic below for descriptions of these different policy types.
The tax and price policy category included policies that were tax-specific, price-specific, or banned alcohol discounts. For tax-specific policies, studies were only included if the analyses controlled for income or a related variable. Such statistical adjustments help to isolate the effects of interest – i.e., whether taxes had an effect on alcohol consumption, since it accounts for the affordability of alcohol. Price-specific policies, referred to as minimum pricing policies, were defined as interventions that established the lowest allowable price for a fixed amount of alcohol.
The availability policy category included policies on outlet densities, time of sale, the minimum legal age for purchasing or drinking alcohol, and total bans on alcohol sales. Outlet density policies included studies that examined the effect of regulating the number of outlets within a certain area, such as per square mile or per inhabitant. Time of sale policies included studies that examined the effect of regulating days of sale or hours of sale.
While marketing policies can range from no restrictions on marketing to a comprehensive ban on all forms of alcohol marketing for all media types across all alcohol types, the Working Group only found studies on strong bans that were informative enough to include. Strong bans were defined as bans on alcohol marketing in at least 1 major media type for all types of alcohol.
Coordinated multiple interventions were defined as government alcohol monopolies or a set of interventions that were part of national plan that aimed to reduce harms that are associated with alcohol consumption. Monopolies are implemented within a national structure and include the policies mentioned above: high taxes on alcohol, restrictions or bans on promotional pricing strategies, limitations on availability, and restrictions or bans on marketing.
Changes in alcohol consumption could be either at the population-level or individual-level. At the population-level, alcohol consumption was defined as the total or recorded average annual per capita consumption or sales. At the individual-level, alcohol consumption was defined as daily consumption as reported by participants. When there were limited studies that used alcohol consumption as an outcome, the Working Group used proxy outcomes for which an association with alcohol consumption had been previously established (e.g., rates of assault, death from cirrhosis). The Working Group either concluded that were was sufficient evidence that a policy was associated with a reduction in alcohol consumption or that there was insufficient evidence.
From the statistical analyses reported in the studies, the Working Group calculated the estimated percentage change in alcohol consumption that was associated with the intervention. When assessing the quality of the studies, the Working Group considered whether other confounding variables were controlled for, such as income, and whether appropriate control groups were used. For individual-level studies, they also considered difference between groups and patterns of non-responses (to ensure missing data was only due to random chance).
WHAT DID THIS STUDY FIND?
Increasing taxes and establishing a minimum price for alcohol reduced alcohol consumption, but banning alcohol discounts had little effect
The Working Group concluded that there is sufficient evidence that increasing taxes on alcohol, which increases overall prices to the consumer, is associated with reduced alcohol consumption. While the magnitude of the effect varied, this conclusion was supported by 7 studies that showed, for example, increasing taxes by 21% for beer and 90% each for wine and spirits in the state of Illinois resulted in a greater decrease in monthly alcohol purchases when compared to 43 other states that did not increase taxes. Specifically, there was a decrease in purchases of 6% among households with residents who reported heavy drinking and a 5% decrease among households with higher incomes. Similar results were seen outside of the US, with a 70% excise-tax increase on ready-to-drink beverages in Australia showing a 9% reduction in the average number of alcoholic drinks consumed daily.
The Working Group concluded that there is sufficient evidence that establishing minimum prices on alcohol is associated with reduced alcohol consumption. This conclusion was supported by the results of 10 studies conducted in Australia, Canada, and the United Kingdom. The majority of them, however, assessed the effects of implementing a minimum price of 50 pence ($0.68 USD) per UK standard unit, which is defined as 8 grams of ethanol, in Scotland during May 2018. The most recent study showed a 3% net reduction in total alcohol sales per adult after 3 years of the policy being in effect. Another study of the same intervention at the individual level showed an 8% decrease in grams of ethanol purchased weekly by each adult in a household after 8 months of implementation of the policy.
The Working Group concluded that there is insufficient evidence that banning alcohol discounts is associated with reduced alcohol consumption. This was due to inconsistent findings reported by the 3 studies included here. These studies all examined the effect of a 2011 partial ban on discounts on the purchase of multiple units of alcohol sold off-premises in Scotland. One study showed a 2% decrease in the volume of alcohol sold off-premises per capita, while another showed a 9% increase in weekly alcohol purchases, and another showed no difference in weekly alcohol purchases.
Reducing the availability of alcohol in communities reduced alcohol consumption
The Working Group concluded that there is sufficient evidence that restricting the density of alcohol outlets is associated with reduced alcohol consumption. This conclusion was supported by the results of 8 studies showing that, for example, the strictest policies that limited alcohol licenses to establishments were associated with a 2% lower alcohol-related hospital admissions rate when compared to locations without licensing policies. Further, the majority of studies examining the effects of increasing alcohol outlet density demonstrated associated increases in alcohol consumption or assault rates.
The Working Group concluded that there is sufficient evidence that restricting the days or hours of alcohol sales is associated with reduced alcohol consumption. This conclusion was supported by the results of 10 studies, all of which were conducted in high-income countries, with the 1 controlled trial showing a 4% increase in average monthly per capita alcohol sales following the implementation of a policy in Sweden that permitted alcohol to be sold on Saturdays and weekdays. In the US, banning off-premises alcohol sales on Sundays was associated with a 4-9% decrease in alcohol consumption.
The Working Group concluded that there is sufficient evidence that increasing the minimum legal age to purchase or drink alcohol is associated with reduced alcohol consumption. This conclusion was supported by the results of 14 studies conducted in the US, Europe, and Canada, showing that, for example, increasing the minimum age to purchase alcohol in Europe by 1 year was associated with a 10% decrease in alcohol consumption.
The Working Group concluded that there is sufficient evidence that banning alcohol sales is associated with reduced alcohol consumption. This conclusion was supported by the results of 9 studies, with 1 examining the effect of the national prohibition of alcohol in the US from 1920-1935. Results of this study demonstrated that alcohol consumption initially decreased by 70% and then leveled off to a 30-40% decrease when compared to pre-prohibition drinking levels. Similarly, a study examining the effect of a 2016 alcohol sales ban in 1 state in India showed a decrease in weekly alcohol consumption from 15% in 2015-2016 to 8% in 2020-2021, a decrease that was not observed in neighboring states allowing alcohol sales.
Strong bans on alcohol marketing reduced alcohol consumption
The Working Group concluded that there is sufficient evidence that strong bans on alcohol marketing (i.e., bans on marketing in at least 1 major media type across all alcohol types) are associated with reduced alcohol consumption. This conclusion was supported by the results of 4 studies showing that, for example, a 1975 ban in Norway on marketing in all media types for alcoholic beverages with an alcohol content greater than 2.5% was associated with 7% decrease in alcohol consumption. Two other studies that used data from the Organization for Economic Cooperation and Development, which included 20 countries from 1970-1995 and 17 countries from 1975-2000, showed that strong bans were associated with 4-9% decrease in alcohol consumption.
Weakening or dissolving government alcohol monopolies and other coordinated multiple alcohol policy interventions increased alcohol consumption
The Working Group concluded that there is sufficient evidence that government monopolies and other coordinated policy interventions are associated with reduced alcohol consumption. This conclusion was supported by the results of 12 studies that examined the effects of weakening or dissolving government alcohol monopolies in relation to alcohol consumption and showed an inverse effect. For example, a study conducted in Poland showed that dissolution of the government alcohol monopoly in 1990 was associated with a 9% increase in alcohol consumption. Similarly, in the US, the 2012 privatization of the retail sales and distribution of liquor in Washington state was associated with a 26% increase in monthly off-premises alcohol purchases per household.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this review article, the International Agency for Research on Cancer Working Group concluded that there was sufficient evidence that the following alcohol policy interventions reduced alcohol consumption: increasing taxes and establishing minimum prices; reducing the overall availability of alcohol by restricting the density of alcohol outlets, restricting the days or hours of sale, setting a minimum legal age for alcohol purchases or consumption, and banning all alcohol sales entirely; having strong bans on alcohol marketing; and having government monopolies or other coordinated multiple alcohol policy interventions. The only policy intervention that the Working Group concluded did not have sufficient evidence was banning discounts on alcohol, given the inconsistent findings produced by the 3 studies that examined this intervention.
These findings add to the availableresearch demonstrating that policy interventions can reduce alcohol consumption and associated health consequences. Additionally, they support the recommendations outlined in the World Health Organization Global Alcohol Action Plan 2022-2030. Some of these recommendations are similar to the policies shown to be effective in the current literature review, such as restricting alcohol availability, enforcing marketing bans, and raising alcohol prices. However, the Action Plan also goes beyond and includes recommendations to advance and enforce efforts to prevent drunk driving and to facilitate access to screening, brief interventions, and treatment.
While the effects reported appear to be relatively modest, at a public health level, they have the potential to have a major impact on individuals’ alcohol use and health across whole populations. Yet, the policy interventions examined here will not fully address the problem of excessive drinking and alcohol use disorder in the US. To have the greatest impact on alcohol use outcomes and counteract the massive influence of the alcohol industry, a multi-pronged approach is needed. This would include policies that support the implementation of evidence-based prevention programs that aim to reduce risk factors and enhance protective factors across the life span, such as the Nurse-Family Partnership for infants and toddlers, the Good Behavior Game for elementary school-aged children, the LifeSkills Training program for adolescents, and the Brief Alcohol Screening and Intervention for College Students (BASICS) program, in addition to programs that support families (e.g., Strengthening Families Program) and communities (e.g., Communities that Care, PROmoting School-Community-University Partnerships to Enhance Resilience (PROSPER)). Such a multi-pronged approach would also include policies that support evidence-based treatment programs (e.g., behavioral health treatment/counseling, medications, and mutual-groups) and promote recovery (e.g., continuation of care, peer-based support, employment services, recovery housing).
The majority of the included studies were conducted before the expansion of digital marketing and online purchasing. Their results may therefore not generalize to the present time where digital marketing and online purchasing are so prevalent.
The majority of the studies were conducted in high income countries. Their results may not generalize to lower income countries.
Implementation and enforcement of the alcohol policy interventions that were examined may have varied across settings, which may have affected their impact on alcohol consumption.
BOTTOM LINE
Taxation and regulatory alcohol policies that target pricing, sales, availability, and marketing are associated with reduced alcohol consumption, thereby decreasing risks for associated health and social consequences. If these policies are combined with prevention, treatment, and recovery approaches, the benefits to public health can be maximized.
For individuals and families seeking recovery: This literature review concluded that taxation and regulatory alcohol policies reduce alcohol consumption. Prior research has shown that reducing alcohol use can decrease the risk of health problems and other social consequences. Accordingly, individuals who reduce the amount of alcohol they drink, or stop drinking entirely, can improve their health and decrease their risk of developing health problems, including the risk of cancer. Further, if given the choice, individuals in, or seeking recovery from, alcohol use disorder may benefit from living in areas with higher taxes on alcohol, bans on advertising/marketing, or reduced availability (e.g., bans on sales during certain times, lower alcohol outlet density) to reduce exposure to alcohol cues and other social triggers.
For treatment professionals and treatment systems: The results from this literature review demonstrated that taxation and regulatory alcohol policies reduce alcohol consumption, which has previously been shown to decrease the risk of cancer and health problems, as well as other social consequences. Accordingly, professionals who provide the necessary treatment to their clients who drink more than the current guidelines suggest (i.e., no more than 2 drinks per day for men and no more than 1 drink per day for women) to reduce their alcohol use may help decrease their risk of health and social consequences. Further, supporting clients in, or seeking recovery from, alcohol use disorder in finding housing in areas with higher taxes on alcohol or reduced alcohol availability may help promote sustained recovery.
For scientists: Because the majority of the included studies were conducted before the expansion of digital marketing and online purchasing, future research that examines similar policy interventions would shed light on the extent to which these findings generalize to the present time where digital marketing and online purchasing are so prevalent. Additionally, because the majority of the included studies were conducted in high-income countries, future studies that replicate them in lower income countries would inform whether the results are similar for such countries. Finally, investigation of the effects of how well these alcohol policies are implemented and enforced on alcohol consumption would help provide information on whether their impact varies across policy settings.
For policy makers: Price and availability are 2 well-known dimensions that affect consumption. This literature review concluded that there is sufficient research evidence that alcohol policies that target pricing, sales, availability, and marketing are associated with reduced alcohol consumption. Previous research has shown that reducing alcohol use can decrease the risk of health problems and other social consequences. Accordingly, policymakers who support the enactment and implementation of such policies can help reduce alcohol use, thereby improving public health. Further, policymakers who consider a multi-pronged approach that includes policies that support evidence-based prevention programs that aim to reduce risk factors and enhance protective factors across the life span, in addition to family- and community-based prevention programs alongside treatment and recovery approaches, may maximize public health benefits.
CITATIONS
Gapstur, S. M., Mariosa, D., Neamtiu, L., Nethan, S. T., Rehm, J., Huckle, T., Jernigan, D. H., O’Connor, E. A., Štelemėkas, M., Allebeck, P., Assanangkornchai, S., Carah, N., Chaiyasong, S., Cukier, S., Dao, T. S., John, R. M., Matzopoulos, R., Meier, P. S., O’Brien P., … & Lauby-Secretan, B. (2025). The IARC Perspective on the Effects of Policies on Reducing Alcohol Consumption.New England Journal of Medicine, 392(17), 1752-1759. doi: 10.1056/NEJMsr2413289.
Given the associations between alcohol consumption and these numerous harms, interventions are needed to reduce consumption. The International Agency for Research on Cancer created the Handbooks of Cancer Prevention Program, for which the Working Group developed a 2-part volume about the primary prevention of alcohol-related cancers. In the first volume (Volume 20A), the Working Group evaluated studies that examined the association between cessation of alcohol consumption and alcohol-related cancers. Following their evaluation, they concluded that there is sufficient evidence that reducing or quitting alcohol use reduces the risk of alcohol-related cancer.
In the second volume (Volume 20B), the Working Group evaluated studies that examined the effects of policy interventions that aimed to reduce alcohol consumption. Their key findings are summarized in this review article. Such findings can shed light on which alcohol policy interventions are effective at reducing alcohol consumption, thereby informing future policymaking efforts, reducing the risks of alcohol-related harms, and improving public health.
HOW WAS THIS STUDY CONDUCTED?
The International Agency for Research on Cancer Working Group conducted a literature review of studies examining alcohol policy interventions. The strength of the studies’ evidence to reduce alcohol consumption was qualitatively evaluated.
Studies were included if they were published and described empirical data on alcohol policy interventions that examined changes in alcohol consumption (i.e., beer, wine, and spirits). Interventions were chosen that aimed to reduce alcohol consumption at the national or subnational level. These included 20 studies that assessed tax and price policies, 39 studies that assessed alcohol availability policies, 4 studies that assessed marketing policies, and 20 studies that assessed government monopolies or coordinated multiple interventions. See graphic below for descriptions of these different policy types.
The tax and price policy category included policies that were tax-specific, price-specific, or banned alcohol discounts. For tax-specific policies, studies were only included if the analyses controlled for income or a related variable. Such statistical adjustments help to isolate the effects of interest – i.e., whether taxes had an effect on alcohol consumption, since it accounts for the affordability of alcohol. Price-specific policies, referred to as minimum pricing policies, were defined as interventions that established the lowest allowable price for a fixed amount of alcohol.
The availability policy category included policies on outlet densities, time of sale, the minimum legal age for purchasing or drinking alcohol, and total bans on alcohol sales. Outlet density policies included studies that examined the effect of regulating the number of outlets within a certain area, such as per square mile or per inhabitant. Time of sale policies included studies that examined the effect of regulating days of sale or hours of sale.
While marketing policies can range from no restrictions on marketing to a comprehensive ban on all forms of alcohol marketing for all media types across all alcohol types, the Working Group only found studies on strong bans that were informative enough to include. Strong bans were defined as bans on alcohol marketing in at least 1 major media type for all types of alcohol.
Coordinated multiple interventions were defined as government alcohol monopolies or a set of interventions that were part of national plan that aimed to reduce harms that are associated with alcohol consumption. Monopolies are implemented within a national structure and include the policies mentioned above: high taxes on alcohol, restrictions or bans on promotional pricing strategies, limitations on availability, and restrictions or bans on marketing.
Changes in alcohol consumption could be either at the population-level or individual-level. At the population-level, alcohol consumption was defined as the total or recorded average annual per capita consumption or sales. At the individual-level, alcohol consumption was defined as daily consumption as reported by participants. When there were limited studies that used alcohol consumption as an outcome, the Working Group used proxy outcomes for which an association with alcohol consumption had been previously established (e.g., rates of assault, death from cirrhosis). The Working Group either concluded that were was sufficient evidence that a policy was associated with a reduction in alcohol consumption or that there was insufficient evidence.
From the statistical analyses reported in the studies, the Working Group calculated the estimated percentage change in alcohol consumption that was associated with the intervention. When assessing the quality of the studies, the Working Group considered whether other confounding variables were controlled for, such as income, and whether appropriate control groups were used. For individual-level studies, they also considered difference between groups and patterns of non-responses (to ensure missing data was only due to random chance).
WHAT DID THIS STUDY FIND?
Increasing taxes and establishing a minimum price for alcohol reduced alcohol consumption, but banning alcohol discounts had little effect
The Working Group concluded that there is sufficient evidence that increasing taxes on alcohol, which increases overall prices to the consumer, is associated with reduced alcohol consumption. While the magnitude of the effect varied, this conclusion was supported by 7 studies that showed, for example, increasing taxes by 21% for beer and 90% each for wine and spirits in the state of Illinois resulted in a greater decrease in monthly alcohol purchases when compared to 43 other states that did not increase taxes. Specifically, there was a decrease in purchases of 6% among households with residents who reported heavy drinking and a 5% decrease among households with higher incomes. Similar results were seen outside of the US, with a 70% excise-tax increase on ready-to-drink beverages in Australia showing a 9% reduction in the average number of alcoholic drinks consumed daily.
The Working Group concluded that there is sufficient evidence that establishing minimum prices on alcohol is associated with reduced alcohol consumption. This conclusion was supported by the results of 10 studies conducted in Australia, Canada, and the United Kingdom. The majority of them, however, assessed the effects of implementing a minimum price of 50 pence ($0.68 USD) per UK standard unit, which is defined as 8 grams of ethanol, in Scotland during May 2018. The most recent study showed a 3% net reduction in total alcohol sales per adult after 3 years of the policy being in effect. Another study of the same intervention at the individual level showed an 8% decrease in grams of ethanol purchased weekly by each adult in a household after 8 months of implementation of the policy.
The Working Group concluded that there is insufficient evidence that banning alcohol discounts is associated with reduced alcohol consumption. This was due to inconsistent findings reported by the 3 studies included here. These studies all examined the effect of a 2011 partial ban on discounts on the purchase of multiple units of alcohol sold off-premises in Scotland. One study showed a 2% decrease in the volume of alcohol sold off-premises per capita, while another showed a 9% increase in weekly alcohol purchases, and another showed no difference in weekly alcohol purchases.
Reducing the availability of alcohol in communities reduced alcohol consumption
The Working Group concluded that there is sufficient evidence that restricting the density of alcohol outlets is associated with reduced alcohol consumption. This conclusion was supported by the results of 8 studies showing that, for example, the strictest policies that limited alcohol licenses to establishments were associated with a 2% lower alcohol-related hospital admissions rate when compared to locations without licensing policies. Further, the majority of studies examining the effects of increasing alcohol outlet density demonstrated associated increases in alcohol consumption or assault rates.
The Working Group concluded that there is sufficient evidence that restricting the days or hours of alcohol sales is associated with reduced alcohol consumption. This conclusion was supported by the results of 10 studies, all of which were conducted in high-income countries, with the 1 controlled trial showing a 4% increase in average monthly per capita alcohol sales following the implementation of a policy in Sweden that permitted alcohol to be sold on Saturdays and weekdays. In the US, banning off-premises alcohol sales on Sundays was associated with a 4-9% decrease in alcohol consumption.
The Working Group concluded that there is sufficient evidence that increasing the minimum legal age to purchase or drink alcohol is associated with reduced alcohol consumption. This conclusion was supported by the results of 14 studies conducted in the US, Europe, and Canada, showing that, for example, increasing the minimum age to purchase alcohol in Europe by 1 year was associated with a 10% decrease in alcohol consumption.
The Working Group concluded that there is sufficient evidence that banning alcohol sales is associated with reduced alcohol consumption. This conclusion was supported by the results of 9 studies, with 1 examining the effect of the national prohibition of alcohol in the US from 1920-1935. Results of this study demonstrated that alcohol consumption initially decreased by 70% and then leveled off to a 30-40% decrease when compared to pre-prohibition drinking levels. Similarly, a study examining the effect of a 2016 alcohol sales ban in 1 state in India showed a decrease in weekly alcohol consumption from 15% in 2015-2016 to 8% in 2020-2021, a decrease that was not observed in neighboring states allowing alcohol sales.
Strong bans on alcohol marketing reduced alcohol consumption
The Working Group concluded that there is sufficient evidence that strong bans on alcohol marketing (i.e., bans on marketing in at least 1 major media type across all alcohol types) are associated with reduced alcohol consumption. This conclusion was supported by the results of 4 studies showing that, for example, a 1975 ban in Norway on marketing in all media types for alcoholic beverages with an alcohol content greater than 2.5% was associated with 7% decrease in alcohol consumption. Two other studies that used data from the Organization for Economic Cooperation and Development, which included 20 countries from 1970-1995 and 17 countries from 1975-2000, showed that strong bans were associated with 4-9% decrease in alcohol consumption.
Weakening or dissolving government alcohol monopolies and other coordinated multiple alcohol policy interventions increased alcohol consumption
The Working Group concluded that there is sufficient evidence that government monopolies and other coordinated policy interventions are associated with reduced alcohol consumption. This conclusion was supported by the results of 12 studies that examined the effects of weakening or dissolving government alcohol monopolies in relation to alcohol consumption and showed an inverse effect. For example, a study conducted in Poland showed that dissolution of the government alcohol monopoly in 1990 was associated with a 9% increase in alcohol consumption. Similarly, in the US, the 2012 privatization of the retail sales and distribution of liquor in Washington state was associated with a 26% increase in monthly off-premises alcohol purchases per household.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this review article, the International Agency for Research on Cancer Working Group concluded that there was sufficient evidence that the following alcohol policy interventions reduced alcohol consumption: increasing taxes and establishing minimum prices; reducing the overall availability of alcohol by restricting the density of alcohol outlets, restricting the days or hours of sale, setting a minimum legal age for alcohol purchases or consumption, and banning all alcohol sales entirely; having strong bans on alcohol marketing; and having government monopolies or other coordinated multiple alcohol policy interventions. The only policy intervention that the Working Group concluded did not have sufficient evidence was banning discounts on alcohol, given the inconsistent findings produced by the 3 studies that examined this intervention.
These findings add to the availableresearch demonstrating that policy interventions can reduce alcohol consumption and associated health consequences. Additionally, they support the recommendations outlined in the World Health Organization Global Alcohol Action Plan 2022-2030. Some of these recommendations are similar to the policies shown to be effective in the current literature review, such as restricting alcohol availability, enforcing marketing bans, and raising alcohol prices. However, the Action Plan also goes beyond and includes recommendations to advance and enforce efforts to prevent drunk driving and to facilitate access to screening, brief interventions, and treatment.
While the effects reported appear to be relatively modest, at a public health level, they have the potential to have a major impact on individuals’ alcohol use and health across whole populations. Yet, the policy interventions examined here will not fully address the problem of excessive drinking and alcohol use disorder in the US. To have the greatest impact on alcohol use outcomes and counteract the massive influence of the alcohol industry, a multi-pronged approach is needed. This would include policies that support the implementation of evidence-based prevention programs that aim to reduce risk factors and enhance protective factors across the life span, such as the Nurse-Family Partnership for infants and toddlers, the Good Behavior Game for elementary school-aged children, the LifeSkills Training program for adolescents, and the Brief Alcohol Screening and Intervention for College Students (BASICS) program, in addition to programs that support families (e.g., Strengthening Families Program) and communities (e.g., Communities that Care, PROmoting School-Community-University Partnerships to Enhance Resilience (PROSPER)). Such a multi-pronged approach would also include policies that support evidence-based treatment programs (e.g., behavioral health treatment/counseling, medications, and mutual-groups) and promote recovery (e.g., continuation of care, peer-based support, employment services, recovery housing).
The majority of the included studies were conducted before the expansion of digital marketing and online purchasing. Their results may therefore not generalize to the present time where digital marketing and online purchasing are so prevalent.
The majority of the studies were conducted in high income countries. Their results may not generalize to lower income countries.
Implementation and enforcement of the alcohol policy interventions that were examined may have varied across settings, which may have affected their impact on alcohol consumption.
BOTTOM LINE
Taxation and regulatory alcohol policies that target pricing, sales, availability, and marketing are associated with reduced alcohol consumption, thereby decreasing risks for associated health and social consequences. If these policies are combined with prevention, treatment, and recovery approaches, the benefits to public health can be maximized.
For individuals and families seeking recovery: This literature review concluded that taxation and regulatory alcohol policies reduce alcohol consumption. Prior research has shown that reducing alcohol use can decrease the risk of health problems and other social consequences. Accordingly, individuals who reduce the amount of alcohol they drink, or stop drinking entirely, can improve their health and decrease their risk of developing health problems, including the risk of cancer. Further, if given the choice, individuals in, or seeking recovery from, alcohol use disorder may benefit from living in areas with higher taxes on alcohol, bans on advertising/marketing, or reduced availability (e.g., bans on sales during certain times, lower alcohol outlet density) to reduce exposure to alcohol cues and other social triggers.
For treatment professionals and treatment systems: The results from this literature review demonstrated that taxation and regulatory alcohol policies reduce alcohol consumption, which has previously been shown to decrease the risk of cancer and health problems, as well as other social consequences. Accordingly, professionals who provide the necessary treatment to their clients who drink more than the current guidelines suggest (i.e., no more than 2 drinks per day for men and no more than 1 drink per day for women) to reduce their alcohol use may help decrease their risk of health and social consequences. Further, supporting clients in, or seeking recovery from, alcohol use disorder in finding housing in areas with higher taxes on alcohol or reduced alcohol availability may help promote sustained recovery.
For scientists: Because the majority of the included studies were conducted before the expansion of digital marketing and online purchasing, future research that examines similar policy interventions would shed light on the extent to which these findings generalize to the present time where digital marketing and online purchasing are so prevalent. Additionally, because the majority of the included studies were conducted in high-income countries, future studies that replicate them in lower income countries would inform whether the results are similar for such countries. Finally, investigation of the effects of how well these alcohol policies are implemented and enforced on alcohol consumption would help provide information on whether their impact varies across policy settings.
For policy makers: Price and availability are 2 well-known dimensions that affect consumption. This literature review concluded that there is sufficient research evidence that alcohol policies that target pricing, sales, availability, and marketing are associated with reduced alcohol consumption. Previous research has shown that reducing alcohol use can decrease the risk of health problems and other social consequences. Accordingly, policymakers who support the enactment and implementation of such policies can help reduce alcohol use, thereby improving public health. Further, policymakers who consider a multi-pronged approach that includes policies that support evidence-based prevention programs that aim to reduce risk factors and enhance protective factors across the life span, in addition to family- and community-based prevention programs alongside treatment and recovery approaches, may maximize public health benefits.
CITATIONS
Gapstur, S. M., Mariosa, D., Neamtiu, L., Nethan, S. T., Rehm, J., Huckle, T., Jernigan, D. H., O’Connor, E. A., Štelemėkas, M., Allebeck, P., Assanangkornchai, S., Carah, N., Chaiyasong, S., Cukier, S., Dao, T. S., John, R. M., Matzopoulos, R., Meier, P. S., O’Brien P., … & Lauby-Secretan, B. (2025). The IARC Perspective on the Effects of Policies on Reducing Alcohol Consumption.New England Journal of Medicine, 392(17), 1752-1759. doi: 10.1056/NEJMsr2413289.
Given the associations between alcohol consumption and these numerous harms, interventions are needed to reduce consumption. The International Agency for Research on Cancer created the Handbooks of Cancer Prevention Program, for which the Working Group developed a 2-part volume about the primary prevention of alcohol-related cancers. In the first volume (Volume 20A), the Working Group evaluated studies that examined the association between cessation of alcohol consumption and alcohol-related cancers. Following their evaluation, they concluded that there is sufficient evidence that reducing or quitting alcohol use reduces the risk of alcohol-related cancer.
In the second volume (Volume 20B), the Working Group evaluated studies that examined the effects of policy interventions that aimed to reduce alcohol consumption. Their key findings are summarized in this review article. Such findings can shed light on which alcohol policy interventions are effective at reducing alcohol consumption, thereby informing future policymaking efforts, reducing the risks of alcohol-related harms, and improving public health.
HOW WAS THIS STUDY CONDUCTED?
The International Agency for Research on Cancer Working Group conducted a literature review of studies examining alcohol policy interventions. The strength of the studies’ evidence to reduce alcohol consumption was qualitatively evaluated.
Studies were included if they were published and described empirical data on alcohol policy interventions that examined changes in alcohol consumption (i.e., beer, wine, and spirits). Interventions were chosen that aimed to reduce alcohol consumption at the national or subnational level. These included 20 studies that assessed tax and price policies, 39 studies that assessed alcohol availability policies, 4 studies that assessed marketing policies, and 20 studies that assessed government monopolies or coordinated multiple interventions. See graphic below for descriptions of these different policy types.
The tax and price policy category included policies that were tax-specific, price-specific, or banned alcohol discounts. For tax-specific policies, studies were only included if the analyses controlled for income or a related variable. Such statistical adjustments help to isolate the effects of interest – i.e., whether taxes had an effect on alcohol consumption, since it accounts for the affordability of alcohol. Price-specific policies, referred to as minimum pricing policies, were defined as interventions that established the lowest allowable price for a fixed amount of alcohol.
The availability policy category included policies on outlet densities, time of sale, the minimum legal age for purchasing or drinking alcohol, and total bans on alcohol sales. Outlet density policies included studies that examined the effect of regulating the number of outlets within a certain area, such as per square mile or per inhabitant. Time of sale policies included studies that examined the effect of regulating days of sale or hours of sale.
While marketing policies can range from no restrictions on marketing to a comprehensive ban on all forms of alcohol marketing for all media types across all alcohol types, the Working Group only found studies on strong bans that were informative enough to include. Strong bans were defined as bans on alcohol marketing in at least 1 major media type for all types of alcohol.
Coordinated multiple interventions were defined as government alcohol monopolies or a set of interventions that were part of national plan that aimed to reduce harms that are associated with alcohol consumption. Monopolies are implemented within a national structure and include the policies mentioned above: high taxes on alcohol, restrictions or bans on promotional pricing strategies, limitations on availability, and restrictions or bans on marketing.
Changes in alcohol consumption could be either at the population-level or individual-level. At the population-level, alcohol consumption was defined as the total or recorded average annual per capita consumption or sales. At the individual-level, alcohol consumption was defined as daily consumption as reported by participants. When there were limited studies that used alcohol consumption as an outcome, the Working Group used proxy outcomes for which an association with alcohol consumption had been previously established (e.g., rates of assault, death from cirrhosis). The Working Group either concluded that were was sufficient evidence that a policy was associated with a reduction in alcohol consumption or that there was insufficient evidence.
From the statistical analyses reported in the studies, the Working Group calculated the estimated percentage change in alcohol consumption that was associated with the intervention. When assessing the quality of the studies, the Working Group considered whether other confounding variables were controlled for, such as income, and whether appropriate control groups were used. For individual-level studies, they also considered difference between groups and patterns of non-responses (to ensure missing data was only due to random chance).
WHAT DID THIS STUDY FIND?
Increasing taxes and establishing a minimum price for alcohol reduced alcohol consumption, but banning alcohol discounts had little effect
The Working Group concluded that there is sufficient evidence that increasing taxes on alcohol, which increases overall prices to the consumer, is associated with reduced alcohol consumption. While the magnitude of the effect varied, this conclusion was supported by 7 studies that showed, for example, increasing taxes by 21% for beer and 90% each for wine and spirits in the state of Illinois resulted in a greater decrease in monthly alcohol purchases when compared to 43 other states that did not increase taxes. Specifically, there was a decrease in purchases of 6% among households with residents who reported heavy drinking and a 5% decrease among households with higher incomes. Similar results were seen outside of the US, with a 70% excise-tax increase on ready-to-drink beverages in Australia showing a 9% reduction in the average number of alcoholic drinks consumed daily.
The Working Group concluded that there is sufficient evidence that establishing minimum prices on alcohol is associated with reduced alcohol consumption. This conclusion was supported by the results of 10 studies conducted in Australia, Canada, and the United Kingdom. The majority of them, however, assessed the effects of implementing a minimum price of 50 pence ($0.68 USD) per UK standard unit, which is defined as 8 grams of ethanol, in Scotland during May 2018. The most recent study showed a 3% net reduction in total alcohol sales per adult after 3 years of the policy being in effect. Another study of the same intervention at the individual level showed an 8% decrease in grams of ethanol purchased weekly by each adult in a household after 8 months of implementation of the policy.
The Working Group concluded that there is insufficient evidence that banning alcohol discounts is associated with reduced alcohol consumption. This was due to inconsistent findings reported by the 3 studies included here. These studies all examined the effect of a 2011 partial ban on discounts on the purchase of multiple units of alcohol sold off-premises in Scotland. One study showed a 2% decrease in the volume of alcohol sold off-premises per capita, while another showed a 9% increase in weekly alcohol purchases, and another showed no difference in weekly alcohol purchases.
Reducing the availability of alcohol in communities reduced alcohol consumption
The Working Group concluded that there is sufficient evidence that restricting the density of alcohol outlets is associated with reduced alcohol consumption. This conclusion was supported by the results of 8 studies showing that, for example, the strictest policies that limited alcohol licenses to establishments were associated with a 2% lower alcohol-related hospital admissions rate when compared to locations without licensing policies. Further, the majority of studies examining the effects of increasing alcohol outlet density demonstrated associated increases in alcohol consumption or assault rates.
The Working Group concluded that there is sufficient evidence that restricting the days or hours of alcohol sales is associated with reduced alcohol consumption. This conclusion was supported by the results of 10 studies, all of which were conducted in high-income countries, with the 1 controlled trial showing a 4% increase in average monthly per capita alcohol sales following the implementation of a policy in Sweden that permitted alcohol to be sold on Saturdays and weekdays. In the US, banning off-premises alcohol sales on Sundays was associated with a 4-9% decrease in alcohol consumption.
The Working Group concluded that there is sufficient evidence that increasing the minimum legal age to purchase or drink alcohol is associated with reduced alcohol consumption. This conclusion was supported by the results of 14 studies conducted in the US, Europe, and Canada, showing that, for example, increasing the minimum age to purchase alcohol in Europe by 1 year was associated with a 10% decrease in alcohol consumption.
The Working Group concluded that there is sufficient evidence that banning alcohol sales is associated with reduced alcohol consumption. This conclusion was supported by the results of 9 studies, with 1 examining the effect of the national prohibition of alcohol in the US from 1920-1935. Results of this study demonstrated that alcohol consumption initially decreased by 70% and then leveled off to a 30-40% decrease when compared to pre-prohibition drinking levels. Similarly, a study examining the effect of a 2016 alcohol sales ban in 1 state in India showed a decrease in weekly alcohol consumption from 15% in 2015-2016 to 8% in 2020-2021, a decrease that was not observed in neighboring states allowing alcohol sales.
Strong bans on alcohol marketing reduced alcohol consumption
The Working Group concluded that there is sufficient evidence that strong bans on alcohol marketing (i.e., bans on marketing in at least 1 major media type across all alcohol types) are associated with reduced alcohol consumption. This conclusion was supported by the results of 4 studies showing that, for example, a 1975 ban in Norway on marketing in all media types for alcoholic beverages with an alcohol content greater than 2.5% was associated with 7% decrease in alcohol consumption. Two other studies that used data from the Organization for Economic Cooperation and Development, which included 20 countries from 1970-1995 and 17 countries from 1975-2000, showed that strong bans were associated with 4-9% decrease in alcohol consumption.
Weakening or dissolving government alcohol monopolies and other coordinated multiple alcohol policy interventions increased alcohol consumption
The Working Group concluded that there is sufficient evidence that government monopolies and other coordinated policy interventions are associated with reduced alcohol consumption. This conclusion was supported by the results of 12 studies that examined the effects of weakening or dissolving government alcohol monopolies in relation to alcohol consumption and showed an inverse effect. For example, a study conducted in Poland showed that dissolution of the government alcohol monopoly in 1990 was associated with a 9% increase in alcohol consumption. Similarly, in the US, the 2012 privatization of the retail sales and distribution of liquor in Washington state was associated with a 26% increase in monthly off-premises alcohol purchases per household.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this review article, the International Agency for Research on Cancer Working Group concluded that there was sufficient evidence that the following alcohol policy interventions reduced alcohol consumption: increasing taxes and establishing minimum prices; reducing the overall availability of alcohol by restricting the density of alcohol outlets, restricting the days or hours of sale, setting a minimum legal age for alcohol purchases or consumption, and banning all alcohol sales entirely; having strong bans on alcohol marketing; and having government monopolies or other coordinated multiple alcohol policy interventions. The only policy intervention that the Working Group concluded did not have sufficient evidence was banning discounts on alcohol, given the inconsistent findings produced by the 3 studies that examined this intervention.
These findings add to the availableresearch demonstrating that policy interventions can reduce alcohol consumption and associated health consequences. Additionally, they support the recommendations outlined in the World Health Organization Global Alcohol Action Plan 2022-2030. Some of these recommendations are similar to the policies shown to be effective in the current literature review, such as restricting alcohol availability, enforcing marketing bans, and raising alcohol prices. However, the Action Plan also goes beyond and includes recommendations to advance and enforce efforts to prevent drunk driving and to facilitate access to screening, brief interventions, and treatment.
While the effects reported appear to be relatively modest, at a public health level, they have the potential to have a major impact on individuals’ alcohol use and health across whole populations. Yet, the policy interventions examined here will not fully address the problem of excessive drinking and alcohol use disorder in the US. To have the greatest impact on alcohol use outcomes and counteract the massive influence of the alcohol industry, a multi-pronged approach is needed. This would include policies that support the implementation of evidence-based prevention programs that aim to reduce risk factors and enhance protective factors across the life span, such as the Nurse-Family Partnership for infants and toddlers, the Good Behavior Game for elementary school-aged children, the LifeSkills Training program for adolescents, and the Brief Alcohol Screening and Intervention for College Students (BASICS) program, in addition to programs that support families (e.g., Strengthening Families Program) and communities (e.g., Communities that Care, PROmoting School-Community-University Partnerships to Enhance Resilience (PROSPER)). Such a multi-pronged approach would also include policies that support evidence-based treatment programs (e.g., behavioral health treatment/counseling, medications, and mutual-groups) and promote recovery (e.g., continuation of care, peer-based support, employment services, recovery housing).
The majority of the included studies were conducted before the expansion of digital marketing and online purchasing. Their results may therefore not generalize to the present time where digital marketing and online purchasing are so prevalent.
The majority of the studies were conducted in high income countries. Their results may not generalize to lower income countries.
Implementation and enforcement of the alcohol policy interventions that were examined may have varied across settings, which may have affected their impact on alcohol consumption.
BOTTOM LINE
Taxation and regulatory alcohol policies that target pricing, sales, availability, and marketing are associated with reduced alcohol consumption, thereby decreasing risks for associated health and social consequences. If these policies are combined with prevention, treatment, and recovery approaches, the benefits to public health can be maximized.
For individuals and families seeking recovery: This literature review concluded that taxation and regulatory alcohol policies reduce alcohol consumption. Prior research has shown that reducing alcohol use can decrease the risk of health problems and other social consequences. Accordingly, individuals who reduce the amount of alcohol they drink, or stop drinking entirely, can improve their health and decrease their risk of developing health problems, including the risk of cancer. Further, if given the choice, individuals in, or seeking recovery from, alcohol use disorder may benefit from living in areas with higher taxes on alcohol, bans on advertising/marketing, or reduced availability (e.g., bans on sales during certain times, lower alcohol outlet density) to reduce exposure to alcohol cues and other social triggers.
For treatment professionals and treatment systems: The results from this literature review demonstrated that taxation and regulatory alcohol policies reduce alcohol consumption, which has previously been shown to decrease the risk of cancer and health problems, as well as other social consequences. Accordingly, professionals who provide the necessary treatment to their clients who drink more than the current guidelines suggest (i.e., no more than 2 drinks per day for men and no more than 1 drink per day for women) to reduce their alcohol use may help decrease their risk of health and social consequences. Further, supporting clients in, or seeking recovery from, alcohol use disorder in finding housing in areas with higher taxes on alcohol or reduced alcohol availability may help promote sustained recovery.
For scientists: Because the majority of the included studies were conducted before the expansion of digital marketing and online purchasing, future research that examines similar policy interventions would shed light on the extent to which these findings generalize to the present time where digital marketing and online purchasing are so prevalent. Additionally, because the majority of the included studies were conducted in high-income countries, future studies that replicate them in lower income countries would inform whether the results are similar for such countries. Finally, investigation of the effects of how well these alcohol policies are implemented and enforced on alcohol consumption would help provide information on whether their impact varies across policy settings.
For policy makers: Price and availability are 2 well-known dimensions that affect consumption. This literature review concluded that there is sufficient research evidence that alcohol policies that target pricing, sales, availability, and marketing are associated with reduced alcohol consumption. Previous research has shown that reducing alcohol use can decrease the risk of health problems and other social consequences. Accordingly, policymakers who support the enactment and implementation of such policies can help reduce alcohol use, thereby improving public health. Further, policymakers who consider a multi-pronged approach that includes policies that support evidence-based prevention programs that aim to reduce risk factors and enhance protective factors across the life span, in addition to family- and community-based prevention programs alongside treatment and recovery approaches, may maximize public health benefits.
CITATIONS
Gapstur, S. M., Mariosa, D., Neamtiu, L., Nethan, S. T., Rehm, J., Huckle, T., Jernigan, D. H., O’Connor, E. A., Štelemėkas, M., Allebeck, P., Assanangkornchai, S., Carah, N., Chaiyasong, S., Cukier, S., Dao, T. S., John, R. M., Matzopoulos, R., Meier, P. S., O’Brien P., … & Lauby-Secretan, B. (2025). The IARC Perspective on the Effects of Policies on Reducing Alcohol Consumption.New England Journal of Medicine, 392(17), 1752-1759. doi: 10.1056/NEJMsr2413289.