
How useful is abstinence alone in understanding the effectiveness of SUD treatment?
Abstinence from alcohol and other drugs is commonly perceived as a defining feature of recovery and has been widely used as a marker by which to evaluate the success of substance use disorder (SUD) treatment. Efforts have been made to define recovery more broadly by incorporating indices of functioning and well-being, but even within such broader definitions, achieving abstinence (as opposed to drinking at low-risk levels) is noted as an important milestone. This paper presents three-year outcomes of persons who participated in outpatient treatment for alcohol use disorder, where treatment outcomes are defined in terms of both alcohol use and functioning.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
A focus on abstinence in defining recovery from an alcohol or other substance use problem has a long history in the field of addiction. More recently, however, efforts have been made to broaden the definition of recovery so as to align more closely with the variety of actions one can take toward health and wellness for those with substance use disorder. This broadening of the definition has largely focused on incorporating indices of functioning and well-being, which, of course, are of great relevance to individuals with SUD, both inside and outside the treatment context. When it comes to substance use, however, most definitions of recovery continue to focus on abstinence rather than also considering drinking patterns that do not result in a re-occurrence of substance use disorder symptoms or other harms. Clinically as well, patients are often advised to choose abstinence as their treatment goal. Increasingly, however, it is being questioned if abstinence is a necessary treatment goal for all persons with substance use disorder. To shed further light on this issue, Witkiewitz and colleagues looked at the outcomes of 806 alcohol use disorder outpatients over the course of three years after they started alcohol use disorder outpatient treatment.
HOW WAS THIS STUDY CONDUCTED?
This study was a secondary data analysis of the well-characterized and frequently analyzed dataset stemming from Project MATCH, a multi-site project conducted in the 1990s in the United States. This analysis used a subsample of these study participants who were followed for up to three years following the initial Project MATCH treatments. In this subsample, 952 individuals with alcohol use disorder were randomized to receive one of three individually-delivered outpatient treatments (i.e., cognitive behavioral therapy, motivational enhancement therapy, or Twelve-Step facilitation). Of these, 806 (85%) provided data on their drinking during the three years following treatment and were included in analyses. Assessments were conducted prior to treatment, during the 12 weeks of treatment, immediately following treatment, and 6, 12, and 36 months after treatment end. In addition to reporting on their drinking and negative consequences they experienced due to their drinking, participants also provided information on their experiences during the past 30 days, using four yes/no items (“employed,” experienced “serious depression,” “trouble understanding, concentrating, or remembering,” “serious anxiety or tension”), and completed several items measuring to what degree they engaged in problematic social behaviors and to what degree they felt satisfaction with their life.
Witkiewitz and colleagues then conducted two types of analyses. First, they simply defined three groups of participants in terms of their drinking based on cut-off values of public health interest and described their outcomes over time. The three groups they defined were abstainers, low-risk drinkers (i.e. non-abstinent individuals with no heavy drinking days) and heavy drinkers. A heavy drinking day was defined using nationally-defined standards as consuming four or more drinks in a day for women, or five or more drinks in a day for men. Then, they used an exploratory technique called “latent profile analysis” to identify groups of patients based on their reports of alcohol consumption and life functioning (i.e., as described above) over the three years following entry into outpatient treatment.
WHAT DID THIS STUDY FIND?
When outcomes were defined by public health relevant cut-off values, low-risk drinkers were not significantly different from abstainers (i.e., differences were not greater than could be explained by chance alone) on almost all non-drinking outcomes, with one exception: abstainers were significantly unhappier with life. This may because these individuals tended to have the heaviest drinking and most severe problems prior to treatment and these individuals’ lives can continue to be detrimentally affected for many years even after remission has been achieved.
In defining groups that emerged by considering participants’ data over time, Witkiewitz and colleagues identified four profiles:
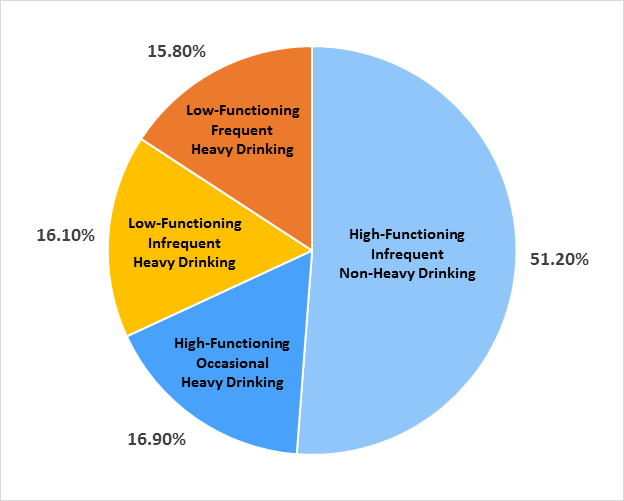
Figure 1. Four drinking categories identified by researchers.
By far the largest group is ‘high-functioning infrequent non-heavy drinking’ (51.2%), which is good news in and of itself. Among these, only 49% were completely abstinent from alcohol, demonstrating that both abstainers and individuals who experienced at least some low-level re-exposure to alcohol were able to achieve high-functioning. Of note, all of these patients were able to refrain from heavy drinking.
For the remaining three groups, whether or not someone remained abstinent was also not a very informative datapoint: a third of these participants were high–functioning despite at least some heavy drinking. Note also that achieving infrequent drinking or abstinence did not guarantee higher functioning: roughly 25% of those achieving infrequent drinking had very poor functioning (i.e., the ‘low-functioning infrequent heavy drinking’ group, which comprises 25% of all participants who were able to refrain from occasional or frequent heavy drinking). Of note, this group also seemed to be worse off at the beginning of the study, as they reported higher levels of depression, tension, and difficulties concentrating at the onset of the study, suggesting that this group was struggling to overcome greater psychosocial challenges than the other groups.
More generally, the study also made observations about how baseline characteristics of patients related to outcomes three years later:
- Higher functioning: Patients who at baseline were found to have better mental health, greater purpose in life, and social support from family and friends were more likely to be high–functioning three years after treatment.
- More frequent heavy drinking: Patients who at baseline had more high-risk social networks that actually supported continuing to consume alcohol were more likely to engage in frequent heavy drinking three years after treatment.
- Achieving high-functioning heavy drinking: Patients who had lower alcohol dependence severity at baseline were more likely to achieve high-functioning despite at least some heavy drinking. Note that high-functioning patients who engaged in occasional heavy drinking were more likely to be White, and at study entry drank fewer drinks per drinking day and experienced fewer consequences due to their drinking than those high-functioning patients who engaged in infrequent non-heavy drinking.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The findings from this secondary data analysis project of a large, multi-site trial delivering outpatient treatment (in the 1990s) to more than 800 alcohol use disorder outpatients lend further weight to recent calls reconsider how the effectiveness of SUD treatments ought best to be measured. It builds on a previous report from the same research group that has highlighted the shortcoming of existing Food and Drug Administration guidance to use heavy drinking as indicative of treatment “failure,” as it fails to acknowledge substantial psychosocial improvements made by individuals who continue to occasionally drink heavily post-treatment. As Witkiewitz and colleagues argue, patient variability (i.e., heterogeneity) has long been acknowledged as an important factor to consider; it may now also be time to acknowledge that there is considerable variability in how some individuals may function following treatment for alcohol use disorder. That said, whereas it is becoming clearer that abstinence is a relatively uninformative indicator of treatment success, engaging in heavy drinking in and of itself confers harm, given that alcohol is a known Group 1 carcinogen – it has the potential to cause cancer. It is also a major cause of liver disease. Thus, while it is possible to engage in heavy drinking occasionally and still function at a high level, such toxicity–related risks need also to be considered. For this reason, perhaps other characterizations of alcohol consumption may be more informative, such as staying within national “low-risk” drinking guidelines. Drinking guidelines, such as those of the American Cancer Society, seek to prevent not only alcohol use disorder, but also the harms posed by both toxicity from alcohol, and recommend that women and men should drink no more than one and two drinks per day respectively, to limit harm due to alcohol’s toxicity-related effects. Beyond broadening our perspective of how alcohol consumption should be considered in terms of defining treatment “success,” the results of this study raise additional intriguing questions surrounding the broad definition of “recovery” that most agree should encompass both indices of functioning and a range of alcohol use indices.
Also of note, roughly half of those who are low-functioning after outpatient treatment show vulnerability to intermittent alcohol exposure, and continue to struggle psychosocially, underscoring the importance of continuing care that can help address these challenges over the longer term.
- LIMITATIONS
-
- Results are based on an older dataset. Alcohol use disorder outpatient treatment, and recovery support services in particular, have changed since 1997. Also note that most treatment is completed in group format and not individually as was done in this trial. Thus, it is not clear how well these findings relate to current outpatients with alcohol use disorder.
- Results are based on the outpatient sample of this dataset, which does not include the inpatients also assessed by Project MATCH. It is not clear if these findings extend to this more severe group of patients.
- Physical health was not tracked in Project MATCH, where drinking in excess of national drinking guidelines would be expected to result in poorer health outcomes long term.
- Functioning status was defined by patient self-report. Family, friends, employers, and providers may have rated it differently.
- “Heavy drinking” was defined in terms of exceeding the national guideline for daily drinking, but this grouping put individuals into the same category who may have had very different drinking patterns (e.g., having 5 drinks versus 20 drinks on a given day).
BOTTOM LINE
This new analysis of a large, multi-site trial with more than 800 alcohol use disorder outpatients showed that some individuals who engage in at least some occasional heavy drinking following treatment may function as well as those who are mostly abstinent with respect to psychosocial functioning, employment, life satisfaction, and mental health. Such individuals tend to have lower addiction severity and fewer alcohol-related consequences prior to treatment, suggesting a more favorable prognosis overall.
- For individuals and families seeking recovery: An incidental finding of this study, but good news that deserves highlighting nevertheless, is the finding that more than half of the alcohol use disorder outpatients examined in this study had a positive outcome for at least 3 years following treatment, both in terms of drinking (i.e., no heavy drinking days) and functioning (i.e., low probability of reporting problematic social behaviors, unemployment, other drug use, or life dissatisfaction). This positive finding is in line with other recent findings highlighting that roughly half of the people seeking to recover from a substance use problem need only two recovery attempts.
- For treatment professionals and treatment systems: This paper provides further empirical support to move beyond a reliance on abstinence as the ultimate indicator of treatment success, and instead to move towards a broader range of drinking as well as psychosocial functioning. See our previous Bulletin article on broader definitions of recovery. Patients with higher addiction severity at treatment entry are less likely to achieve high-functioning with occasional heavy drinking. Moving beyond abstinence as the indicator of treatment success may help decrease barriers to treatment–seeking amongst those who do not wish to abstain from alcohol entirely but may otherwise welcome support in achieving low-risk drinking and higher functioning.
- For scientists: The present study, as well as similar reports, are based on older datasets, and thus replication in more modern-day datasets would help clarify if observed findings generalize to present day alcohol use disorder treatment contexts and recovery supports. Note also that “functioning” may be defined in a number of ways, but in the present study was limited to the indices used in Project MATCH. As Witkiewitz and colleagues highlight, further research should examine the role and impact of heretofore understudied correlates in this context, such as cognitive functioning/executive control, medical health and chronic pain, and misuse of prescription drugs.
- For policy makers: An increasing body of research points to the downfalls of relying on abstinence as a marker of alcohol use disorder treatment success. Far beyond being a simple matter of treatment goal preference of a substantial number of treatment seekers, current evidence, including this paper, suggests that alcohol consumption by itself does not necessarily equate to “treatment failure.” Guidance used to evaluate alcohol use disorder treatment, including FDA regulations, may need to be updated in light of this emerging evidence, with perhaps measures of diagnostic remission status and/or drinking within the national low-risk drinking guidelines being the optimal outcomes.
CITATIONS
Witkiewitz, K., Wilson, A. D., Pearson, M. R., Montes, K. S., Kirouac, M., Roos, C. R., . . . Maisto, S. A. (2018). Profiles of recovery from alcohol use disorder at three years following treatment: Can the definition of recovery be extended to include high functioning heavy drinkers? Addiction, 114(1), 69-80. doi:10.1111/add.14403
