
A Review of Naltrexone Effectiveness for Alcohol Use Disorder Among Women
Few clinical trials have evaluated naltrexone as a treatment for women with alcohol use disorder. This systematic review summarizes the recovery benefit and limitations of what the medicine can and cannot do.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Alcohol use is the third leading cause of preventable death in the US causing 88,000 (62,000 men and 26,000 women) deaths every year. Alcohol use disorder affects almost 30% of US adults at some point in their life (i.e., lifetime prevalence). The disorder is more prevalent among men (36%) yet the disorder also affects almost one in five women (22.7%). Despite this, the effects of different alcohol use disorder treatment interventions addressing women’s alcohol use are only poorly understood.
Oral naltrexone is a medication that is FDA-approved to reduce heavy drinking in individuals with alcohol use disorder, but only about 20% of eligible patients receive any type of FDA approved medicine for alcohol use disorder.
The low rate of medication prescribing for alcohol use disorder perhaps is not surprising considering the efficacy of these interventions varies considerably, yet a previous non-gender specific review found naltrexone was helpful in reducing heavy drinking and cravings. The need to evaluate the impact of treatment options for alcohol use disorders specifically in women is created by notable gender differences such as faster absorption and genetic factors that increase sensitivity to the effects of alcohol. The aim of this new study was to systematically review and summarize the evidence regarding the impact of naltrexone compared to placebo for attenuating alcohol consumption in women with an alcohol use disorder.
HOW WAS THIS STUDY CONDUCTED?
The study was a systematic review, meaning the authors conducted a comprehensive database search with a predefined set of criteria used to include a study in this review. In this case, they searched for peer-reviewed, randomized control trials of naltrexone compared to placebo, published between 1990-2016. The findings had to be presented for women alone or distinct from men plus they had to report a measurable drinking outcome (e.g., percent days abstinent or drinks per day).
WHAT DID THIS STUDY FIND?
Seven studies were identified as meeting criteria and included in the review. These studies included a total of 903 women with alcohol use disorder, with an average age range between 39 to 49, mostly Caucasian, with a treatment duration between 8 to 16 weeks.
Results from each study are detailed in table:
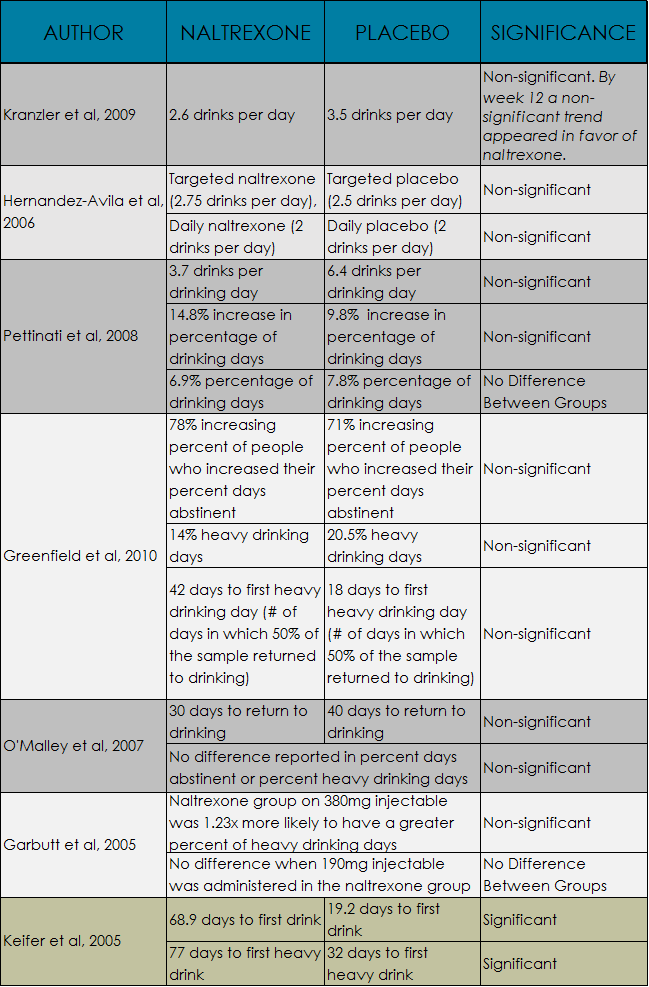
Only 1 of 7 studies reported a statistically significant improvement (i.e., an indicator of the size of the effect relative to the size of the sample) in drinking outcomes among women using naltrexone.
Most studies reported a nonsignificant trend that favored naltrexone and one study reported a nonsignificant trend that favored placebo. Given that four studies had fewer than 100 women they may have been underpowered to detect a significant change in drinking over time. Six studies reported results for both genders and found that three studies observed trends that showed naltrexone reduced drinking more in men than women.
WHY IS THIS STUDY IMPORTANT?
This was an important systematic review given the known sex differences between men and women in alcohol metabolism and its effects and yet no review of naltrexone had focused exclusively on its effects in women.
Overall there was not consistent support that naltrexone can improve drinking outcomes in women. There is a lack of support suggesting that naltrexone can lead to modest reductions in quantity of drinking and time to relapse in women as seen by mostly non-significant trends that favored naltrexone. The number of non-significant trends reported may suggest there was a lack of power to detect a significant change in drinking due to smaller sample sizes. This review has found that naltrexone may not be useful at reducing the frequency of drinking occasions in women.
- LIMITATIONS
-
- The counseling component of the interventions varied widely with some women receiving more counseling than others; therefore, the effect of the medication alone on alcohol use cannot be determined.
- In addition, the treatment duration lasted between 8 and 16 weeks and long-term follow-up data was not reported so the degree to which the results may change over the longer term is unknown.
- Additionally, 4 studies had fewer than 100 women so they may have lacked the statistical power to detect significant changes in drinking.
NEXT STEPS
The field could benefit from study designs that examine gender differences and treatment effects explicitly among persons with alcohol use disorder and present results separately for men and women. This will fuel the development of better treatment options for women.
BOTTOM LINE
- For individuals & families seeking recovery: This was a review of seven rigorous studies on the effectiveness of naltrexone compared to placebo in women. Overall frequency of drinking occasions may not be reduced by naltrexone. Naltrexone may reduce the quantity of drinks in a sitting and increase the time to a relapse in women but that was not consistently or strongly supported. If you or a family member are struggling with drinking, naltrexone is a medicine that has a modest chance at supporting remission from alcohol use disorder. Other kinds of treatments and services may confer greater benefits for women with alcohol use disorder.
- For scientists: While this systematic review of naltrexone for women was informative, studies outlined here generally found that the frequency of drinking occasions was not reduced compared to placebo. Most studies found that the quantity of drinking was reduced in the naltrexone group but the effect was not strong or consistent. Also, women tended not to benefit as much as men from naltrexone. The field would benefit from a meta-analysis to examine gender as a moderator and learn about the different benefit.
- For policy makers: There is a growing body of evidence suggesting a variety of pharmacotherapy (i.e., medicine) and behavioral intervention approaches are helpful in the treatment of alcohol use disorder; however, the effectiveness of one of the more promising treatments (i.e., naltrexone) is understudied in women. This review found that naltrexone reduced the quantity of drinks and increased time to relapse but the effects were not strong or consistent. The frequency of drinking occasions was mostly unaffected by the medication and men tended to receive a greater benefit than women. This highlights the need to support research that seeks to understand women and alcohol use disorder and what treatments might be developed to address their needs more specifically.
- For treatment professionals and treatment systems: Based on the scientific information reviewed, clinicians may wish to advise their patients that naltrexone is an evidenced based FDA approved medicine that can help support remission from alcohol use disorder for both women and men but is less effective for women. Specifically, the medicine may reduce the quantity of drinking and increase time to relapse in women but the effects are modest and inconsistent. Drinking frequency does not appear to respond to the medication in women. Other kinds of treatments and services may confer greater benefits for women with alcohol use disorder and should be used instead of or in addition to naltrexone.
CITATIONS
Canidate, S.S., Carnaby, G.D., Cook, C.L., & Cook, R.L. (2017). A systematic review of naltrexone for attenuating alcohol consumption in women with alcohol use disorders. Alcoholism: Clinical and Experimental Research, Mar; 41(3), 466-472. doi: 10.1111/acer.13313.
