
More Money, More Problems? The Effects of Using Cash as a Reward in Addiction Treatment
Providing a reward for abstinence – contingency management – helps promote better substance use disorder outcomes. There are concerns, however, that using cash as a reward might inadvertently lead to more alcohol and other drug use rather than reduce it. What happens when this understandable concern is investigated using a rigorous scientific approach?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Contingency management (or CM) includes a broad group of behavioral interventions that provide or withhold rewards and negative consequences quickly in response to at least one measurable behavior (e.g., substance use as measured by a toxicology screen). Traditionally programs have used vouchers, tickets without any inherent value which can be exchanged for a range of prizes, because many have concerns that providing actual cash to individuals with substance use disorder will have unintended, triggering consequences.
For example, will patients take that cash and use it to buy alcohol or other drugs? Similarly, given that patients may identify “pay day” as a trigger for thoughts about using and eventual cravings (because they used substances heavily on days they received their paycheck), might they experience similar using-related thoughts and feelings if they received cash as a reward for abstinence?
This study by Festinger and colleagues investigated this concern by comparing abstinence rates for individuals receiving either cash or vouchers as part of a contingency management intervention.
HOW WAS THIS STUDY CONDUCTED?
Patients were 222 individuals with opioid use disorder, newly seeking methadone maintenance treatment who also met criteria for a co-occurring cocaine disorder based on the diagnostic and statistical manual of mental disorders, 4th edition (DSM-IV).
To address the co-occurring cocaine use disorder, they were randomly assigned to one of three conditions:
- Voucher-based contingency management
- Cash-based contingency management
- Control (i.e., no contingency management).
All groups completed three urine toxicology screens (i.e., “drug tests”) per week for 12 weeks, and received methadone maintenance services as usual, including psychosocial treatment for 4-5 hours per week, mostly in group sessions focused on coping skill development and relapse prevention, as well as encouragement to attend mutual-help groups. In the voucher-based contingency management, if a participant screen was cocaine-negative (indicating abstinence), researchers gave the person a voucher that could be exchanged for a range of rewards (e.g., food, toys, gift cards, or to pay outstanding bills). The cash-based contingency management procedure was the same, except researchers gave participants cash (equal to the amount they would have received if in the voucher condition) if their screen was cocaine-negative. Individuals in the control group just completed toxicology screens with no reward for negative screens.
The primary outcome was maximum number of weeks of continuous cocaine abstinence based on the toxicology screen results. Unexcused missed toxicology screens counted as positive – so individuals could not simply no-show to the appointment in order to avoid having to complete the screen. Maximum number of weeks of continuous abstinence is important to distinguish from percentage of days abstinent, which is another typical measure of substance use outcome. Rather than overall number of abstinent days, the measure here prioritizes continuous abstinence without any intermittent use. Secondary outcomes included the number of toxicology screen/psychosocial treatment days attended, cocaine craving (measured by the Cocaine Craving Questionnaire, a 10-item self-report measure), any alcohol use to intoxication (yes or no), and any gambling (yes or no).
The sample was 58% White (authors do not provide specifics on other race/ethnicities, though this value is suggestive of a diverse sample), 69% Male, and 37 years old on average. The three groups (voucher-based contingency management, cash-based contingency management, and control) were similar on demographic characteristics and several clinical characteristics at baseline (e.g., cocaine craving).
WHAT DID THIS STUDY FIND?
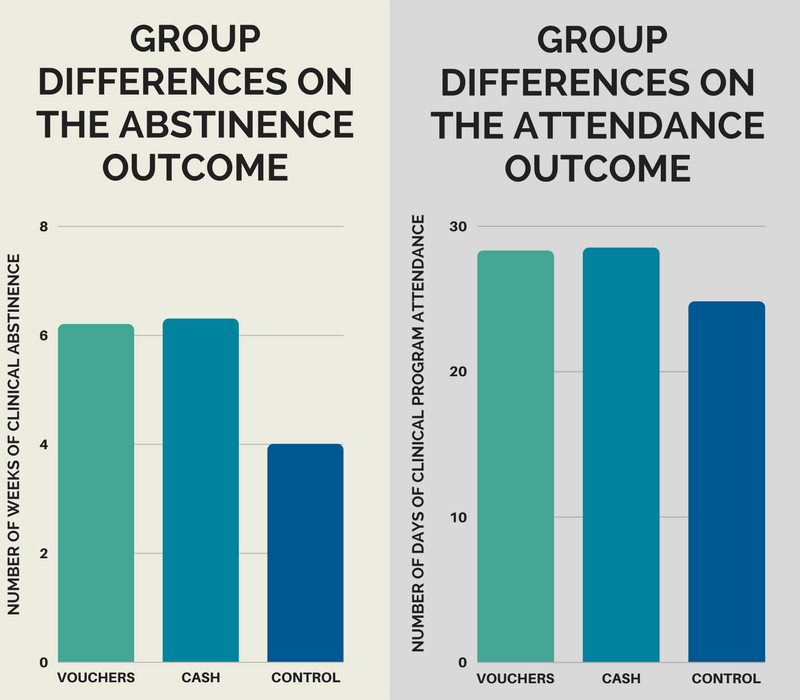
The two contingency management groups both had more weeks of continuous cocaine abstinence than controls, but were not different from each other. This same pattern emerged for number of clinical program attendance days (out of 36), though this difference did not quite reach statistical significance.
See figures below for more detail. The figure on the left depicts groups differences on the abstinence outcome and the figure on the right depicts differences on the attendance outcome.
Overall, the three groups were similar in terms of their cocaine-related craving, as well as instances of alcohol use to intoxication (between 1 and 5% of individuals, across all groups over 12 weeks) and gambling (between 11 and 18% of individuals, across all groups over 12 weeks).
WHY IS THIS STUDY IMPORTANT
This study with a clinical application had similar results to two related earlier studies, also by Festinger and colleagues, which had more of a research application. In those studies, individuals attending an outpatient substance use disorder treatment program were randomized to receive either cash or a gift-card incentive, with a variety of possible amounts (e.g., $10, $40, or $70) for attending a follow-up assessment 6 months later. Then they completed a urine toxicology screen three days after that, for which they received $40, with all participants receiving the same amount.
While participants were more likely to attend the follow-up appointment if they received cash (rather than a gift card), and if they received a higher dollar value, their rates of negative toxicology screens 3 days after the follow-up assessment were similar. In addition, those results showed that individuals receiving cash were more likely to use the reward for essential items (e.g., household/personal need) compared to those receiving a gift card. Taken together with this study outcome, incorporating cash into a contingency management intervention is not likely to lead to poorer substance use outcomes, nor is it likely to result in other undesirable outcomes, such as increased drug craving, drinking to intoxication, or gambling.
Contrary to authors’ hypotheses, however, cash was no better than vouchers at promoting better abstinence rates or clinic attendance. One factor authors point out is that individuals were able to “bank” their cash payments at the clinic – half of the cash participants did this half of the time – and that would essentially negate the more immediate rewarding effects of the cash.
- LIMITATIONS
-
- As with many contingency management studies, authors only examined and rewarded participants for toxicology screen results targeting one substance – cocaine in this study. Whether these results would hold up if the primary substance were different (e.g., marijuana) cannot be determined.
- In addition, the study took place at a single clinical setting. While study authors do not provide details about the sample’s average income, in their related studies, the sample’s average annual income was very low at $6,500. Whether these results – that cash rewards do not lead to more use compared to voucher based rewards – would apply to younger individuals (e.g., students) or older individuals with higher incomes also cannot be determined. Also, methadone programs are unique settings with specific rules, and it is unclear if the results would apply to other types of substance use disorder treatment programs.
- There are several clinical characteristics that could potentially influence results that were not mentioned such as the severity of participants’ opioid use disorder and, correspondingly, their methadone dose. Given that individuals were randomized to condition, however, and the group sizes were adequate, any group differences at treatment entry were likely to be small in magnitude and, thus, not very influential on the group differences in the outcomes described earlier.
NEXT STEPS
This important study has many potential implications for the treatment of individuals with substance use disorder. A system of rewards for abstinence and other positive, healthy, behaviors can be implemented in a wide range of settings, including but not limited to specialty substance use disorder treatment. Given the multitude of factors that could affect how an individual responds to receiving cash in response to positive recovery-related behaviors, however, these results should be replicated in other treatment settings, with samples who have different demographic and clinical characteristics than those investigated in this study.
BOTTOM LINE
- For individuals & families seeking recovery: This study indicates individuals receiving cash as a reward for positive recovery outcomes, like abstinence, are unlikely to do any better or worse than individuals who receive a substitute reward that can also be used to purchase items but with less flexibility making it difficult to use the reward to buy alcohol or other drugs (e.g., a gift card). Both groups are likely to have better outcomes than individuals who receive no reward. This study was conducted in a methadone program, and targeted only cocaine use. Research is needed to confirm (i.e., replicate) these findings in other types of clinical settings and addressing other forms of substance use.
- For scientists: This study provides a good model of how science can be used to test clinical observation and anecdotal evidence. Authors found individuals receiving cash as a reward for positive recovery outcomes, like abstinence, are unlikely to do any better or any worse than individuals who receive a substitute reward that can also be used to purchase items but with less flexibility making it difficult to use the reward to buy alcohol or other drugs (e.g., a gift card). Both groups are likely to have better outcomes than individuals who receive no rewards. While this randomized trial is suggestive of high internal validity, replication studies are needed to examine the study’s external validity.
- For policy makers: This study indicates individuals receiving cash as a reward for positive recovery outcomes, like abstinence, are unlikely to do any better or any worse than individuals who receive a substitute reward that can also be used to purchase items but with less flexibility making it difficult to use the reward to buy alcohol or other drugs making it difficult to use the reward to buy alcohol or other drugs (e.g., a gift card). Both groups are likely to have better outcomes than individuals who receive no reward. This study was conducted in a methadone program, and targeted only cocaine use. Research is needed to confirm (i.e., replicate) these findings in other types of clinical settings and addressing other forms of substance use, before wide-ranging policy decisions are made.
- For treatment professionals and treatment systems: This study indicates individuals in a methadone maintenance program who also had cocaine use disorder receiving cash as a reward for cocaine abstinence are unlikely to do any better or any worse than individuals who receive a substitute reward that can also be used to purchase items but with less flexibility making it difficult to use the reward to buy alcohol or other drugs (e.g., a gift card). They were also similar on other important outcomes including degree of cocaine craving, alcohol use, and gambling behavior. Both groups are likely to have better outcomes than individuals who receive no rewards. Research is needed to replicate these findings in other types of clinical settings and addressing other forms of substance use. Overall, at this point, for programs that implement contingency management and related behavioral principles of reward and consequence, there is no scientific evidence suggesting treatment programs ought to be concerned with recommending use of cash as a reward for abstinence. To date, the evidence is suggestive of no added risk in terms of patient outcomes.
CITATIONS
Festinger, D. S., Dugosh, K. L., Kirby, K. C., & Seymour, B. L. (2014). Contingency management for cocaine treatment: Cash vs. vouchers. Journal of substance abuse treatment, 47(2), 168-174.
