
The Best States for Completing Outpatient Treatment for Substance Use Disorder
Information about which groups of individuals are less likely to complete substance use disorder treatment can help identify areas requiring future attention in treatment and public health policy. This study investigated several types of factors related to failure to complete treatment across US states, including race and ethnicity.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Successful treatment completion for substance use disorder is a known predictor of positive outcomes such as longer term abstinence, fewer relapses, fewer readmissions, higher levels of employment, less criminal involvement, and better overall health. However, racial-ethnic disparities have been documented in the treatment system with White non-Hispanic patients being more likely to complete treatment than non-White patients. Most studies have focused on individual or treatment level factors and few studies have identified completion rates at the state level. States can differ drastically according to regulations, reporting practices, insurance policies, level of integration with mental health services, and other factors. Examining differences between states may provide broader insights to inform public health policy at both state and federal levels, given that most studies rely on samples within a single state.
HOW WAS THIS STUDY CONDUCTED?
This was an exploratory retrospective analysis of state discharge and admission data from the 2006-2008 Treatment Episode Datasets–Discharge (TEDS-D). Data were included from US outpatient substance use disorder treatment centers (such as ambulatory and non-intensive). This study only included participants who had never received treatment for substance use disorder. All first treatment episode clients with admission and discharge records who could be classified as White, Latino, or Black/African American were used (n = 940,058). Alabama, Arizona, New Mexico, Pennsylvania, and Wisconsin were excluded because they were missing critical variables from their state files (e.g., previous treatment admissions in some cases). Clients receiving opioid agonist therapy were also excluded (n = 36,676), although it is unknown why.
In the statistical analysis, the racial-ethnic disparity was expressed as the difference between the percentage of successful discharges among Black clients in a state and the percentage of successful discharges for White clients in the same state. The definition of a successful discharge was not standardized and thus was a clinical judgement of the healthcare worker. Treatment completion rates were adjusted for covariates such as client demographics (e.g., sex, age, employment, housing) and clinical differences (e.g., primary substance) are reported. Controlling for these covariates helps to remove their effects from the estimates of treatment completion that are associated with race-ethnicity. Finally, correlational analyses were used to investigate if state-level disparities increase or decrease with degree of non-White racial composition in the state. For example, do states with relatively few non-White residents have the biggest treatment completion disparities?
WHAT DID THIS STUDY FIND?
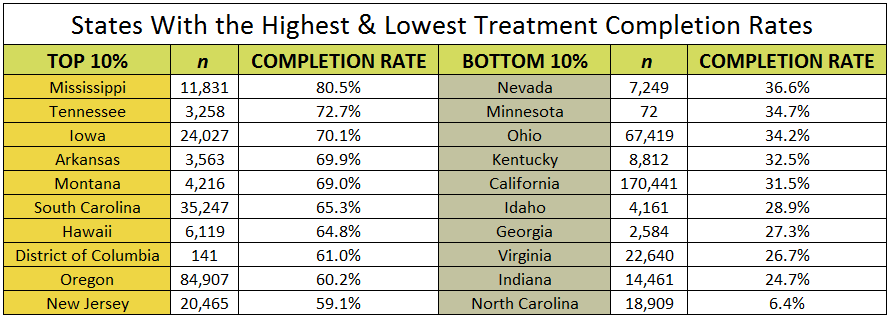
Before accounting for race-ethnicity, initial analyses showed that states varied widely in their treatment completion rates, ranging between 25% and 75%. See Table 1 for the successful treatment completion rates for the top and bottom 10% of states.
Many client level factors were found to be significant predictors of increased likelihood of treatment completion such as being male, older, more educated, being employed full-time, living independently, and having alcohol as a primary substance, and thus were controlled for in the analyses.
Notably, race-ethnicity was a significant predictor of successful treatment completion, even after adjusting for the influence of these variables. Treatment completion rates for White clients was 46.25%; it was 45.55% for Latino clients, and the rate for Black clients was 37.49%. More importantly, there were racial-ethnic differences in treatment completion rates by state.
Figure (Black versus White clients) and Figure (Latino versus White clients) below show state level disparities in treatment completion that are sorted from the largest positive disparity (i.e., the non-White clients completed treatment at a higher rate than White clients) to the smallest.
As illustrated in the figures below, most states have a negative disparity meaning non-White clients are less likely to complete outpatient treatment for substance use disorder. A zero disparity means the completion rates for Black or Latino Clients are similar to White clients. The horizontal line represents a 95% confidence interval centered around the disparity estimate. The confidence interval means we can have high confidence (i.e., 95%) that the true population mean falls somewhere within this range (shorter bars means we can have more confidence in the mean estimate).
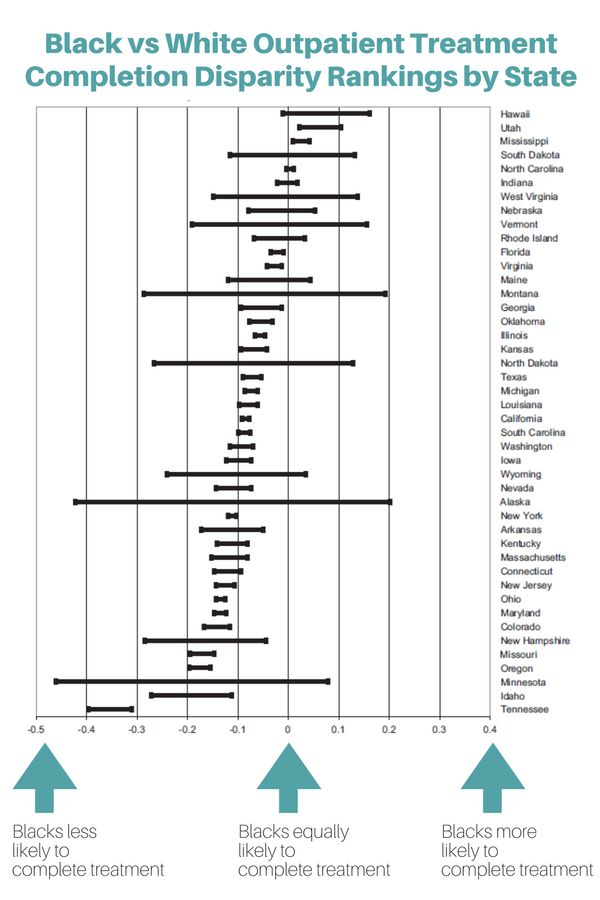
95% Confidence Intervals for the Difference Between Black and White Clients
(i.e, Black treatment completion rate-White completion rate)
(Source: Arndt et al, 2013)
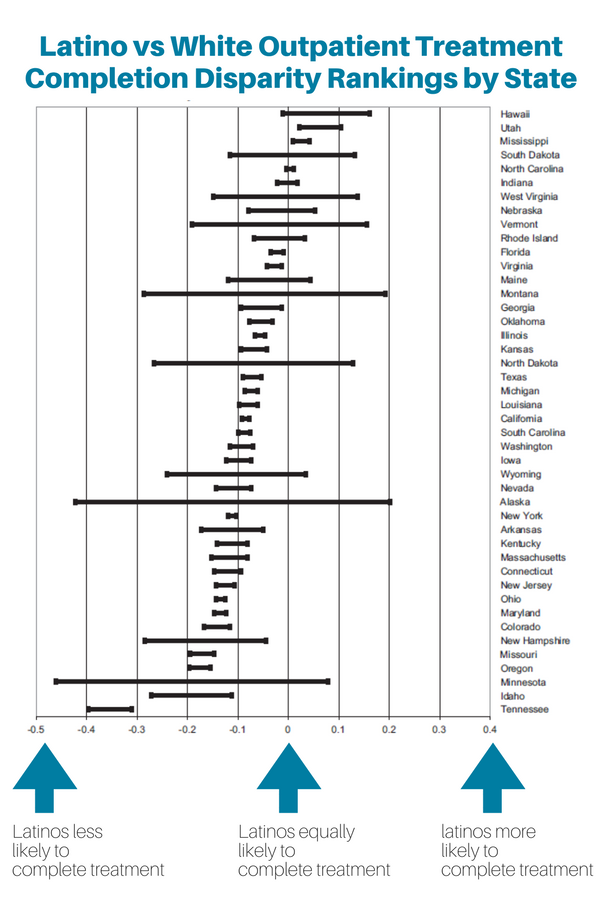
(i.e, Black treatment completion rate-White completion rate)
(Source: Arndt et al, 2013)
The racial-ethnic disparities in treatment completion were not correlated with the proportion of non-White individuals in the state according the US Census, nor was the disparity correlated with the states’ overall success rate for treatment completion.
WHY IS THIS STUDY IMPORTANT
Statewide disparities were generally negative, meaning fewer non-White clients completed outpatient treatment for substance use disorder. Several states showed positive effects for non-White clients as well, especially for Latino clients. There were more statewide disparities that negatively affected Black clients than Latino clients.
Interestingly, racial-ethnic disparities were not correlated with the proportion of non-White residents in the state, the proportion of non-White clients in outpatient treatment, or with the overall completion rate. This suggests that statewide experience with providing treatment to non-White clients did not seem to be related to disparities.
Many factors affect client completion. In this case being male, older, more educated, being employed full-time, living independently, and having alcohol as a primary substance were all associated with treatment completion; however, race-ethnicity predicted treatment completion over and above client level characteristics. A previous study by this author suggested that non-White individuals with a substance use disorder may be less likely to remit because of less social support. A future goal would be to see if social support varies by state and accounts for the state-level disparities observed in this study.
- LIMITATIONS
-
- An important limitation is that the definition of treatment completion was not standardized across treatment systems or states. The definition may be a subjective judgement of the healthcare worker which can vary by client, including client characteristics like race-ethnicity.
NEXT STEPS
More research at the systems and organizational level should be completed to identify macro level factors that influence non-White treatment completion for substance use disorders such as program capacity or staff cultural competence.
BOTTOM LINE
- For individuals & families seeking recovery: This study investigated racial-ethnic disparities in outpatient treatment completion by state. They found that for some states, Black clients were more likely to complete treatment, such as Hawaii, Utah, and Mississippi. Latino clients were more likely to complete treatment in West Virginia and Arkansas, among other states (see Figure 1 & 2). Broadly speaking, non-White clients were less likely to complete treatment across many states; treatment non-completion rates were even larger for Black clients. Ultimately, treatment completion is related to better health and social outcomes and addressing this disparity is an important priority among states, treatment systems, and clients.
- For scientists: Research is needed to determine what factors have created racial-ethnic equivalence in treatment completion rates in the states that demonstrated no disparities. State-level racial-ethnicity disparities were not correlated with the proportion of non-White residents in the state, with the proportion of non-White clients in outpatient treatment, or with the overall completion rate. Statewide experience with providing treatment to non-White clients did not seem to be a factor; therefore, other hypotheses (e.g., insurance coverage) need to be investigated as possible reasons.
- For policy makers: This was an empirically sound study that found statewide disparities were generally negative, meaning fewer non-White clients completed outpatient treatment for substance use disorder. Several states showed positive effects for non-White clients as well, particularly for Latino clients. The researchers suggest that any states showing unjustified racial-ethnic disparities should actively monitor any racial-ethnic effects. In addition, states should investigate system-level causes of any disparities and do a comparison to other states that do not show racial-ethnic disadvantage on elements like service delivery system, services delivered, organizational factors, and counselor criteria.
- For treatment professionals and treatment systems: This national study investigated racial and ethnic disparities in state-level outpatient treatment completion rates, and found that non-White clients are often less likely to complete treatment. Much of the variability in completion rates was independent of client characteristics (e.g., age, primary substance, etc.) which is similar to findings from other studies. If your state was shown to have racial and ethnic disparities in outpatient treatment completion rates, consider comparing your service delivery system, services delivered, organizational factors, and therapist standards to similar states that showed racial and ethnic equivalence.
CITATIONS
Arndt, S., Acion, L., & White, K. (2013). How the states stack up: Disparities in substance abuse outpatient treatment completion rates for minorities. Drug and Alcohol Dependence, 132(3), 547-554.
