Successful follow-up with a peer-based intervention associated with reduced overdose
Peer interventions after an opioid overdose may help reduce subsequent overdose. In this study, patients with higher risk substance use behaviors were more likely to consent to follow-up peer services, but less likely to actually receive them. Results suggest these high-risk patients may face barriers to engaging with peer services after an overdose.
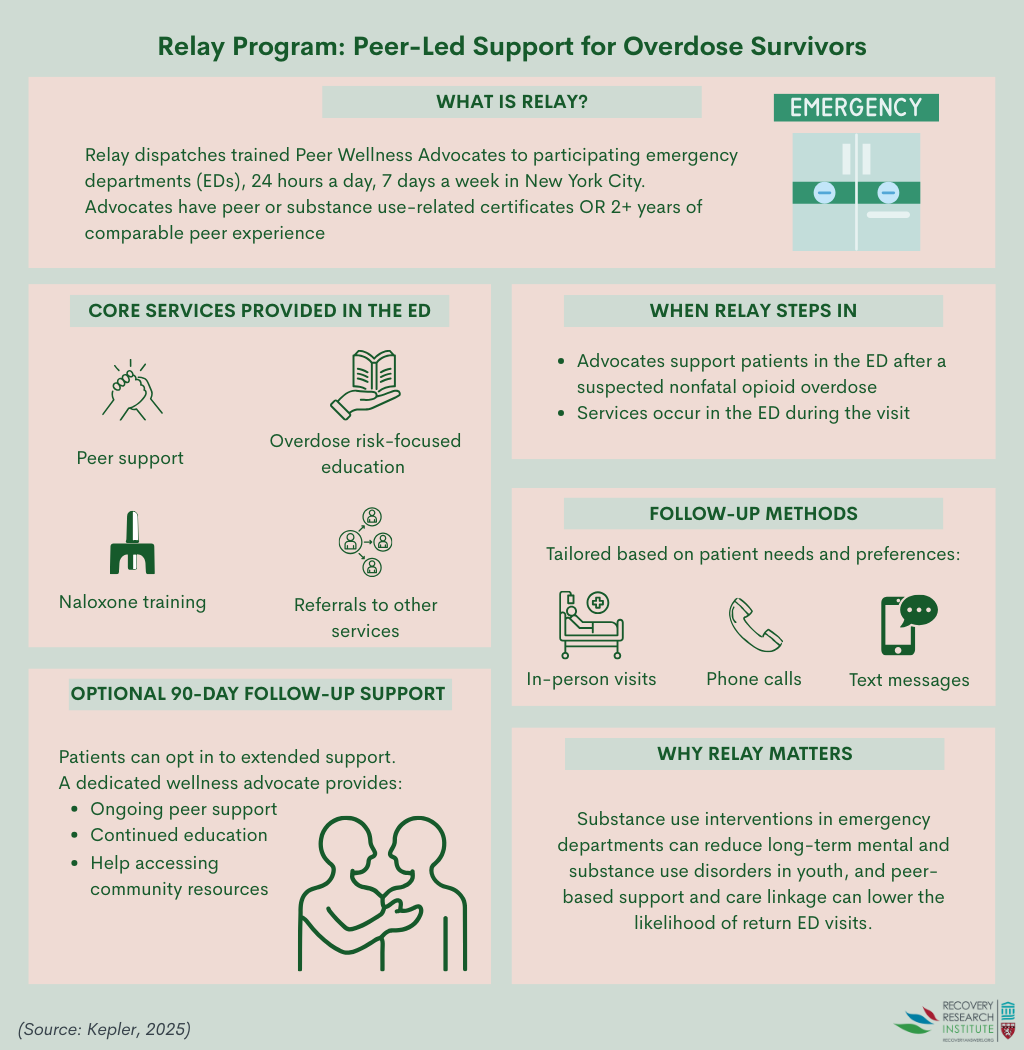
Consistent with this idea, and in response to the opioid overdose epidemic, New York City’s Health Department developed an intervention to be delivered by peers in emergency departments across the city, known as Relay (see graphic below for a summary of the intervention). The Relay intervention was launched in June 2017 and operates 24 hours a day, 7 days a week. It is currently operating in 14 non-public emergency departments. In this intervention, peer wellness advocates engage with patients who present to the emergency department for a suspected nonfatal opioid overdose. Advocates offer them support, education on how to reduce risk of overdoses, training on naloxone (i.e., a drug used to reverse overdoses), and referrals to other services. After patients accept and receive Relay services during their initial emergency department visit, they are also offered follow-up services, where they receive ongoing support and continued education and training for 90 days.
Researchers in this study examined differences between people who consented to receive these follow-up services and whether they were actually reached for them, based on demographics and substance use profiles. They also examined whether level of engagement (i.e., consenting and being reached) reduced the risk of fatal opioid overdose. Such research can help identify who is most likely to consent to follow-up intervention services and be reached for them, which can target intervention efforts towards those hardest to reach. This research can also shed light on whether people who agree to receive follow-up services are reached for them, and the impact this has on risk for experiencing a fatal opioid overdose.
HOW WAS THIS STUDY CONDUCTED?
The researchers in this study examined demographic and substance use behavior differences between people who consented to and were reached for follow-up services from the Relay intervention in New York City emergency departments between 2017 and 2022. The risk of experiencing a fatal opioid overdose following initial Relay intervention services was also examined, based on whether patients consented to and were able to be reached for follow-up services.
The predictor variables of interest included consenting to receive follow-up services and being contacted at least once after the initial emergency department visit, among those who consented. Forms of contact included in-person meeting, telephone call, or text message. The researchers were also interested in demographics, circumstances of the overdose, current engagement with medication treatment for opioid use disorder and syringe service programs, and history of previous overdose. This information was collected by wellness advocates during the emergency department visit. Demographic data included: age, sex, race/ethnicity, and housing status. The primary outcome of interest was death from an unintentional opioid overdose within 1 year after the initial emergency department visit determined by city records.
Patients were included in the study if they were 18 years or older and presented to 1 of the 14 emergency departments in New York City where Relay is currently operating for an unintentional opioid overdose between June 2017 and December 2022. Patients also needed to be eligible for Relay services and accept them in the emergency department. Those who were in police custody, not capable of consenting, or whose overdose was intentional were considered ineligible and excluded from the study. Patients were also excluded if they did not provide their name or did not reside in New York City when they first visited the emergency department.
For the analyses, the researchers first compared the odds of consenting to follow-up services and being reached for follow-up services based on age, sex, race/ethnicity, circumstances of the overdose (i.e., the drug that was intentionally taken and how it was taken), current engagement with medication treatment for opioid use disorder and syringe service programs, and history of previous overdose. Then, the researchers compared the odds of a patient who had consented to follow-up Relay services experiencing a fatal opioid overdose to those who did not consent to follow-up services. Among those who consented, the odds of experiencing a fatal opioid overdose for those who were reached for follow-up were compared to those who were not reached. All analyses were adjusted for age, sex, and race/ethnicity. Such statistical adjustments help to isolate the effect of interest – i.e., whether engagement with Relay services is independently related to the likelihood of experiencing a fatal opioid overdose.
In total, data from 5,006 patients who received Relay services in the emergency department after an unintentional non-fatal opioid overdose were included in the study. Of these, 3,477 (70%) agreed to receive follow-up services and 2,055 (59%) were successfully reached for follow-up services at least once. A total of 269 patients died of an unintentional opioid overdose within 1 year of their initial visit to the emergency department for an overdose and another 121 patients died from other causes.
At the time of their initial visit to the emergency department for an overdose, the majority of the 5,006 patients who were included in the study were men (77%) and were 45 years old or older (53%). Latino/a race was the most commonly reported, with 43% of patients identifying as such. For housing status, 43% reported being stably housed, 32% reported being unstably housed, and 25% reported living with others. Most patients reported that the drug they had intentionally taken that led to their initial overdose was any opioid (83%), with 68% reporting that they took heroin. Another 12% reported taking an opioid painkiller and 4% reported taking fentanyl. The most commonly reported route of administration upon the initial overdose was snorting (63%). The majority of patients reported that they have not experienced an overdose before (59%), were not currently prescribed medications for opioid use disorder (81%), and were not currently engaged with a syringe service program (95%).
WHAT DID THIS STUDY FIND?
Patients who were older and reported higher risk behaviors were more likely to consent to follow-up
There were demographic differences in the odds of consenting to Relay follow-up services. Compared to those who identified as White, people who identified as a different race were 33% less likely to consent to follow-up services. There were no other differences between races.
The odds of consenting to follow-up services were greater among patients who were older. Those who were in the 45-54, 55-64, and 65 years and older age groups were 44%, 61%, and 73% more likely to consent, respectively, than those who were in the 35-44 age group. There were no differences in odds of consenting for those in the 18-24 and 25-34 age groups, as compared to those in the 35-44 age group.
For housing status, those who reported being unstably housed were 31% more likely to consent to follow-up services than those who were stably housed. Those who reported living with others were 22% more likely to consent.
For overdose circumstances, patients who reported taking any opioid upon their initial overdose were 83% more likely to consent. Those who reported taking heroin specifically were twice as likely to consent and those who reported taking fentanyl were 49% more likely to consent. Meanwhile, those who reported taking cocaine or crack with no opioid were 44% less likely to consent, and those who reported an opioid painkiller were 25% less likely. Patients who reported snorting the drug upon overdose were 21% more likely to consent. While it is assumed that these characteristics are being compared to the absence of each characteristic (e.g., any opioid vs. no opioid), the study did not provide this information, making it unclear.
Finally, those who reported experiencing an overdose before were 78% more likely to consent to follow-up services than those who have not and those who were currently prescribed medications for opioid use disorder were 35% more likely than those who were not.
Patients who identified as Black and reported higher risk behaviors were less likely to be reached for follow-up
Among those who consented, there were demographic differences in the odds of being reached for Relay follow-up services. People who identified as Black were 19% less likely to be reached for follow-up services than those who identified as White. There were no other differences between races. There were also no differences between age groups in the odds of being reached for follow-up.
For housing status, those who reported being unstably housed were 52% less likely to be reached for follow-up services than those who were stably housed. Those who reported living with others were 18% less likely to be reached.
For overdose circumstances, patients who reported taking any opioid upon their initial overdose were 19% less likely to be reached for follow-up. Those who reported taking heroin specifically were 28% less likely to be reached. Meanwhile, those who reported taking cocaine or crack with no opioid were 33% more likely to be reached, and those who reported taking an opioid painkiller were 53% more likely to be reached. Patients who reported injecting the drug upon overdose were 28% less likely to be reached and those who reported smoking it were 34% less likely.
Finally, those who reported experiencing an overdose before were 19% less likely to be reached for follow-up services than those who have not and those who were currently engaged with a syringe service program were 33% less likely than those who were not.
Patients reached for follow-up services were less likely to experience a fatal overdose, but there were no differences between those who did and did not consent
In the analyses controlling for age, sex, and race/ethnicity, there were no differences in the risk of experiencing a fatal opioid overdose between patients who consented to receive Relay follow-up services and those who did not consent. However, among patients who consented, those who were reached for follow-up services at least once were 46% less likely to experience a fatal opioid overdose than those who were not reached.
There were no demographic differences in the risk of experiencing a fatal opioid overdose for sex, race/ethnicity, or housing status, but patients who were older had higher risks. Those who were in the age groups of 45-54, 55-64, and 65 years and older were 59%, 63%, and 92% more likely to experience a fatal overdose, respectively, than those in the 35-44 year age group.
For overdose circumstances, patients who reported intentionally taking any opioid upon their initial overdose were 66% more likely to experience a fatal overdose. Those who reported taking heroin specifically were 50% more likely. Meanwhile, those who reported taking cocaine or crack with no opioid were 44% less likely to experience a fatal overdose. As above, it is assumed that these characteristics are being compared to the absence of each characteristic (e.g., any opioid vs. no opioid), though this information was not explicitly provided.
Patients who reported experiencing an overdose before were 53% more likely to experience a fatal overdose than those who have not. Those who were currently prescribed medications for opioid use disorder were 42% less likely to experience a fatal overdose than those who were not, yet those who were currently engaged with a syringe service program were 65% more likely.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined demographic and substance use behavior differences between people who consented to and were reached for follow-up in Relay intervention services in NYC emergency departments between 2017 and 2022, and whether this engagement reduced risk of fatal overdose. Results showed that patients who reported higher risk substance use behaviors (e.g., intentional opioid use, past history of overdose) were more likely to consent to follow-up services, but less likely to actually receive them. This suggests that people who are at higher risk want to receive follow-up services, but face barriers to doing so, such as not having a reliable means of communication or transportation. This may also be due to the possibility of them dying from an overdose within the study period. These findings highlight the need for interventions to better address such barriers and that public health interventions may need to tailor their outreach efforts for people at highest risk.
Results of this study also showed, encouragingly, that patients who were reached for follow-up services were less likely to experience a fatal opioid overdose in the year following initial engagement with the Relay intervention. This demonstrates that providing peer-based follow-up services to people after surviving an opioid overdose can reduce the chances that they will experience a fatal opioid overdose. That said, it cannot be determined whether the Relay intervention was responsible for the reduced overdose risk. People who attended at least one follow-up session in the 90 days after their emergency department stay were likely to be more motivated, and thus, engaged in other types of substance use services. Note that these analyses only controlled for demographic characteristics, not clinical or recovery functioning ones.
That said, these findings may add to the research demonstrating the utility of hospital emergency departments for intervening with people with substance use disorders, particularly when they are delivered by peers. This is likely because emergency department services “meet people where they are”, when they are most in need. Likewise, interventions delivered by peers are likely to reduce the stigma some patients may feel and allow them to feel understood and supported.
The study was conducted in New York City, a large city in the US. Results may not generalize to other cities in the US, especially smaller cities, or other countries.
Because all patients included in the study received the intervention in the emergency department, the study design limits the extent to which the researchers can conclude that the intervention directly caused reductions in overdose risk.
The study design also limits the extent to which the researchers can conclude that the reduced overdose risk was attributable to the follow-up services, since people who are at highest risk are also hardest to reach. In other words, the people who were reached for follow-up services may have been lower risk anyway, regardless of the follow-up services.
The type and intensity of the follow-up services received were not examined. Patients who received only 1 brief follow-up were grouped with patients who may have received more frequent and in-depth follow-up services.
BOTTOM LINE
Patients who reported higher risk substance use behaviors were more likely to consent to receive follow-up services for a peer-based opioid overdose intervention, but less likely to actually receive them. However, patients who were reached for follow-up services were less likely to experience a fatal opioid overdose. These individuals likely had many other factors related to better outcomes, such as motivation and service involvement – thus, these findings should be replicated in an experimental study with a comparison group to determine whether it is useful. That said, these findings may highlight the need for interventions to better reach people who are at highest risk, while also demonstrating the potential public health benefits of follow-up services delivered by peers after an emergency department visit.
For individuals and families seeking recovery: This study shows that staying connected to follow-up services after a visit to the emergency department for a nonfatal opioid overdose can save lives. For people who use opioids at risk of overdose, engaging with peer-based support may reduce the chance of another overdose.
For treatment professionals and treatment systems: Even when patients who are at higher risk of overdose agree to follow-up, many are not ultimately reached, which reveals communication, transportation, and attitudinal barriers they likely face. Treatment professionals and systems who aim to address these barriers and tailor their outreach specifically for people at high risk may be more likely to reach them and reduce their overdose risk. Additionally, treatment systems that incorporate peer-based supports and engage people for follow-up services after surviving an opioid overdose may see reductions in overdose risk and public health benefits.
For scientists: Future research that tests the Relay intervention across diverse geographic settings and care environments can help shed light on the extent to which the results of the current setting generalize. Studies that employ designs capable of establishing causal links can help clarify the extent to which peer-based approaches are directly attributable to reduced risks for overdose deaths. Studies that examine the type and intensity of follow-up can deepen understanding of how frequent and intense follow-up services need to be for beneficial impacts.
For policy makers: Policymakers who support investments in peer recovery programs and infrastructure that helps address barriers to reaching people for follow-up services may help reduce deaths from opioid overdoses. Further, policymakers who support policies that promote hospital-based interventions delivered by peers can help close service gaps and may enhance public health.
Consistent with this idea, and in response to the opioid overdose epidemic, New York City’s Health Department developed an intervention to be delivered by peers in emergency departments across the city, known as Relay (see graphic below for a summary of the intervention). The Relay intervention was launched in June 2017 and operates 24 hours a day, 7 days a week. It is currently operating in 14 non-public emergency departments. In this intervention, peer wellness advocates engage with patients who present to the emergency department for a suspected nonfatal opioid overdose. Advocates offer them support, education on how to reduce risk of overdoses, training on naloxone (i.e., a drug used to reverse overdoses), and referrals to other services. After patients accept and receive Relay services during their initial emergency department visit, they are also offered follow-up services, where they receive ongoing support and continued education and training for 90 days.
Researchers in this study examined differences between people who consented to receive these follow-up services and whether they were actually reached for them, based on demographics and substance use profiles. They also examined whether level of engagement (i.e., consenting and being reached) reduced the risk of fatal opioid overdose. Such research can help identify who is most likely to consent to follow-up intervention services and be reached for them, which can target intervention efforts towards those hardest to reach. This research can also shed light on whether people who agree to receive follow-up services are reached for them, and the impact this has on risk for experiencing a fatal opioid overdose.
HOW WAS THIS STUDY CONDUCTED?
The researchers in this study examined demographic and substance use behavior differences between people who consented to and were reached for follow-up services from the Relay intervention in New York City emergency departments between 2017 and 2022. The risk of experiencing a fatal opioid overdose following initial Relay intervention services was also examined, based on whether patients consented to and were able to be reached for follow-up services.
The predictor variables of interest included consenting to receive follow-up services and being contacted at least once after the initial emergency department visit, among those who consented. Forms of contact included in-person meeting, telephone call, or text message. The researchers were also interested in demographics, circumstances of the overdose, current engagement with medication treatment for opioid use disorder and syringe service programs, and history of previous overdose. This information was collected by wellness advocates during the emergency department visit. Demographic data included: age, sex, race/ethnicity, and housing status. The primary outcome of interest was death from an unintentional opioid overdose within 1 year after the initial emergency department visit determined by city records.
Patients were included in the study if they were 18 years or older and presented to 1 of the 14 emergency departments in New York City where Relay is currently operating for an unintentional opioid overdose between June 2017 and December 2022. Patients also needed to be eligible for Relay services and accept them in the emergency department. Those who were in police custody, not capable of consenting, or whose overdose was intentional were considered ineligible and excluded from the study. Patients were also excluded if they did not provide their name or did not reside in New York City when they first visited the emergency department.
For the analyses, the researchers first compared the odds of consenting to follow-up services and being reached for follow-up services based on age, sex, race/ethnicity, circumstances of the overdose (i.e., the drug that was intentionally taken and how it was taken), current engagement with medication treatment for opioid use disorder and syringe service programs, and history of previous overdose. Then, the researchers compared the odds of a patient who had consented to follow-up Relay services experiencing a fatal opioid overdose to those who did not consent to follow-up services. Among those who consented, the odds of experiencing a fatal opioid overdose for those who were reached for follow-up were compared to those who were not reached. All analyses were adjusted for age, sex, and race/ethnicity. Such statistical adjustments help to isolate the effect of interest – i.e., whether engagement with Relay services is independently related to the likelihood of experiencing a fatal opioid overdose.
In total, data from 5,006 patients who received Relay services in the emergency department after an unintentional non-fatal opioid overdose were included in the study. Of these, 3,477 (70%) agreed to receive follow-up services and 2,055 (59%) were successfully reached for follow-up services at least once. A total of 269 patients died of an unintentional opioid overdose within 1 year of their initial visit to the emergency department for an overdose and another 121 patients died from other causes.
At the time of their initial visit to the emergency department for an overdose, the majority of the 5,006 patients who were included in the study were men (77%) and were 45 years old or older (53%). Latino/a race was the most commonly reported, with 43% of patients identifying as such. For housing status, 43% reported being stably housed, 32% reported being unstably housed, and 25% reported living with others. Most patients reported that the drug they had intentionally taken that led to their initial overdose was any opioid (83%), with 68% reporting that they took heroin. Another 12% reported taking an opioid painkiller and 4% reported taking fentanyl. The most commonly reported route of administration upon the initial overdose was snorting (63%). The majority of patients reported that they have not experienced an overdose before (59%), were not currently prescribed medications for opioid use disorder (81%), and were not currently engaged with a syringe service program (95%).
WHAT DID THIS STUDY FIND?
Patients who were older and reported higher risk behaviors were more likely to consent to follow-up
There were demographic differences in the odds of consenting to Relay follow-up services. Compared to those who identified as White, people who identified as a different race were 33% less likely to consent to follow-up services. There were no other differences between races.
The odds of consenting to follow-up services were greater among patients who were older. Those who were in the 45-54, 55-64, and 65 years and older age groups were 44%, 61%, and 73% more likely to consent, respectively, than those who were in the 35-44 age group. There were no differences in odds of consenting for those in the 18-24 and 25-34 age groups, as compared to those in the 35-44 age group.
For housing status, those who reported being unstably housed were 31% more likely to consent to follow-up services than those who were stably housed. Those who reported living with others were 22% more likely to consent.
For overdose circumstances, patients who reported taking any opioid upon their initial overdose were 83% more likely to consent. Those who reported taking heroin specifically were twice as likely to consent and those who reported taking fentanyl were 49% more likely to consent. Meanwhile, those who reported taking cocaine or crack with no opioid were 44% less likely to consent, and those who reported an opioid painkiller were 25% less likely. Patients who reported snorting the drug upon overdose were 21% more likely to consent. While it is assumed that these characteristics are being compared to the absence of each characteristic (e.g., any opioid vs. no opioid), the study did not provide this information, making it unclear.
Finally, those who reported experiencing an overdose before were 78% more likely to consent to follow-up services than those who have not and those who were currently prescribed medications for opioid use disorder were 35% more likely than those who were not.
Patients who identified as Black and reported higher risk behaviors were less likely to be reached for follow-up
Among those who consented, there were demographic differences in the odds of being reached for Relay follow-up services. People who identified as Black were 19% less likely to be reached for follow-up services than those who identified as White. There were no other differences between races. There were also no differences between age groups in the odds of being reached for follow-up.
For housing status, those who reported being unstably housed were 52% less likely to be reached for follow-up services than those who were stably housed. Those who reported living with others were 18% less likely to be reached.
For overdose circumstances, patients who reported taking any opioid upon their initial overdose were 19% less likely to be reached for follow-up. Those who reported taking heroin specifically were 28% less likely to be reached. Meanwhile, those who reported taking cocaine or crack with no opioid were 33% more likely to be reached, and those who reported taking an opioid painkiller were 53% more likely to be reached. Patients who reported injecting the drug upon overdose were 28% less likely to be reached and those who reported smoking it were 34% less likely.
Finally, those who reported experiencing an overdose before were 19% less likely to be reached for follow-up services than those who have not and those who were currently engaged with a syringe service program were 33% less likely than those who were not.
Patients reached for follow-up services were less likely to experience a fatal overdose, but there were no differences between those who did and did not consent
In the analyses controlling for age, sex, and race/ethnicity, there were no differences in the risk of experiencing a fatal opioid overdose between patients who consented to receive Relay follow-up services and those who did not consent. However, among patients who consented, those who were reached for follow-up services at least once were 46% less likely to experience a fatal opioid overdose than those who were not reached.
There were no demographic differences in the risk of experiencing a fatal opioid overdose for sex, race/ethnicity, or housing status, but patients who were older had higher risks. Those who were in the age groups of 45-54, 55-64, and 65 years and older were 59%, 63%, and 92% more likely to experience a fatal overdose, respectively, than those in the 35-44 year age group.
For overdose circumstances, patients who reported intentionally taking any opioid upon their initial overdose were 66% more likely to experience a fatal overdose. Those who reported taking heroin specifically were 50% more likely. Meanwhile, those who reported taking cocaine or crack with no opioid were 44% less likely to experience a fatal overdose. As above, it is assumed that these characteristics are being compared to the absence of each characteristic (e.g., any opioid vs. no opioid), though this information was not explicitly provided.
Patients who reported experiencing an overdose before were 53% more likely to experience a fatal overdose than those who have not. Those who were currently prescribed medications for opioid use disorder were 42% less likely to experience a fatal overdose than those who were not, yet those who were currently engaged with a syringe service program were 65% more likely.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined demographic and substance use behavior differences between people who consented to and were reached for follow-up in Relay intervention services in NYC emergency departments between 2017 and 2022, and whether this engagement reduced risk of fatal overdose. Results showed that patients who reported higher risk substance use behaviors (e.g., intentional opioid use, past history of overdose) were more likely to consent to follow-up services, but less likely to actually receive them. This suggests that people who are at higher risk want to receive follow-up services, but face barriers to doing so, such as not having a reliable means of communication or transportation. This may also be due to the possibility of them dying from an overdose within the study period. These findings highlight the need for interventions to better address such barriers and that public health interventions may need to tailor their outreach efforts for people at highest risk.
Results of this study also showed, encouragingly, that patients who were reached for follow-up services were less likely to experience a fatal opioid overdose in the year following initial engagement with the Relay intervention. This demonstrates that providing peer-based follow-up services to people after surviving an opioid overdose can reduce the chances that they will experience a fatal opioid overdose. That said, it cannot be determined whether the Relay intervention was responsible for the reduced overdose risk. People who attended at least one follow-up session in the 90 days after their emergency department stay were likely to be more motivated, and thus, engaged in other types of substance use services. Note that these analyses only controlled for demographic characteristics, not clinical or recovery functioning ones.
That said, these findings may add to the research demonstrating the utility of hospital emergency departments for intervening with people with substance use disorders, particularly when they are delivered by peers. This is likely because emergency department services “meet people where they are”, when they are most in need. Likewise, interventions delivered by peers are likely to reduce the stigma some patients may feel and allow them to feel understood and supported.
The study was conducted in New York City, a large city in the US. Results may not generalize to other cities in the US, especially smaller cities, or other countries.
Because all patients included in the study received the intervention in the emergency department, the study design limits the extent to which the researchers can conclude that the intervention directly caused reductions in overdose risk.
The study design also limits the extent to which the researchers can conclude that the reduced overdose risk was attributable to the follow-up services, since people who are at highest risk are also hardest to reach. In other words, the people who were reached for follow-up services may have been lower risk anyway, regardless of the follow-up services.
The type and intensity of the follow-up services received were not examined. Patients who received only 1 brief follow-up were grouped with patients who may have received more frequent and in-depth follow-up services.
BOTTOM LINE
Patients who reported higher risk substance use behaviors were more likely to consent to receive follow-up services for a peer-based opioid overdose intervention, but less likely to actually receive them. However, patients who were reached for follow-up services were less likely to experience a fatal opioid overdose. These individuals likely had many other factors related to better outcomes, such as motivation and service involvement – thus, these findings should be replicated in an experimental study with a comparison group to determine whether it is useful. That said, these findings may highlight the need for interventions to better reach people who are at highest risk, while also demonstrating the potential public health benefits of follow-up services delivered by peers after an emergency department visit.
For individuals and families seeking recovery: This study shows that staying connected to follow-up services after a visit to the emergency department for a nonfatal opioid overdose can save lives. For people who use opioids at risk of overdose, engaging with peer-based support may reduce the chance of another overdose.
For treatment professionals and treatment systems: Even when patients who are at higher risk of overdose agree to follow-up, many are not ultimately reached, which reveals communication, transportation, and attitudinal barriers they likely face. Treatment professionals and systems who aim to address these barriers and tailor their outreach specifically for people at high risk may be more likely to reach them and reduce their overdose risk. Additionally, treatment systems that incorporate peer-based supports and engage people for follow-up services after surviving an opioid overdose may see reductions in overdose risk and public health benefits.
For scientists: Future research that tests the Relay intervention across diverse geographic settings and care environments can help shed light on the extent to which the results of the current setting generalize. Studies that employ designs capable of establishing causal links can help clarify the extent to which peer-based approaches are directly attributable to reduced risks for overdose deaths. Studies that examine the type and intensity of follow-up can deepen understanding of how frequent and intense follow-up services need to be for beneficial impacts.
For policy makers: Policymakers who support investments in peer recovery programs and infrastructure that helps address barriers to reaching people for follow-up services may help reduce deaths from opioid overdoses. Further, policymakers who support policies that promote hospital-based interventions delivered by peers can help close service gaps and may enhance public health.
Consistent with this idea, and in response to the opioid overdose epidemic, New York City’s Health Department developed an intervention to be delivered by peers in emergency departments across the city, known as Relay (see graphic below for a summary of the intervention). The Relay intervention was launched in June 2017 and operates 24 hours a day, 7 days a week. It is currently operating in 14 non-public emergency departments. In this intervention, peer wellness advocates engage with patients who present to the emergency department for a suspected nonfatal opioid overdose. Advocates offer them support, education on how to reduce risk of overdoses, training on naloxone (i.e., a drug used to reverse overdoses), and referrals to other services. After patients accept and receive Relay services during their initial emergency department visit, they are also offered follow-up services, where they receive ongoing support and continued education and training for 90 days.
Researchers in this study examined differences between people who consented to receive these follow-up services and whether they were actually reached for them, based on demographics and substance use profiles. They also examined whether level of engagement (i.e., consenting and being reached) reduced the risk of fatal opioid overdose. Such research can help identify who is most likely to consent to follow-up intervention services and be reached for them, which can target intervention efforts towards those hardest to reach. This research can also shed light on whether people who agree to receive follow-up services are reached for them, and the impact this has on risk for experiencing a fatal opioid overdose.
HOW WAS THIS STUDY CONDUCTED?
The researchers in this study examined demographic and substance use behavior differences between people who consented to and were reached for follow-up services from the Relay intervention in New York City emergency departments between 2017 and 2022. The risk of experiencing a fatal opioid overdose following initial Relay intervention services was also examined, based on whether patients consented to and were able to be reached for follow-up services.
The predictor variables of interest included consenting to receive follow-up services and being contacted at least once after the initial emergency department visit, among those who consented. Forms of contact included in-person meeting, telephone call, or text message. The researchers were also interested in demographics, circumstances of the overdose, current engagement with medication treatment for opioid use disorder and syringe service programs, and history of previous overdose. This information was collected by wellness advocates during the emergency department visit. Demographic data included: age, sex, race/ethnicity, and housing status. The primary outcome of interest was death from an unintentional opioid overdose within 1 year after the initial emergency department visit determined by city records.
Patients were included in the study if they were 18 years or older and presented to 1 of the 14 emergency departments in New York City where Relay is currently operating for an unintentional opioid overdose between June 2017 and December 2022. Patients also needed to be eligible for Relay services and accept them in the emergency department. Those who were in police custody, not capable of consenting, or whose overdose was intentional were considered ineligible and excluded from the study. Patients were also excluded if they did not provide their name or did not reside in New York City when they first visited the emergency department.
For the analyses, the researchers first compared the odds of consenting to follow-up services and being reached for follow-up services based on age, sex, race/ethnicity, circumstances of the overdose (i.e., the drug that was intentionally taken and how it was taken), current engagement with medication treatment for opioid use disorder and syringe service programs, and history of previous overdose. Then, the researchers compared the odds of a patient who had consented to follow-up Relay services experiencing a fatal opioid overdose to those who did not consent to follow-up services. Among those who consented, the odds of experiencing a fatal opioid overdose for those who were reached for follow-up were compared to those who were not reached. All analyses were adjusted for age, sex, and race/ethnicity. Such statistical adjustments help to isolate the effect of interest – i.e., whether engagement with Relay services is independently related to the likelihood of experiencing a fatal opioid overdose.
In total, data from 5,006 patients who received Relay services in the emergency department after an unintentional non-fatal opioid overdose were included in the study. Of these, 3,477 (70%) agreed to receive follow-up services and 2,055 (59%) were successfully reached for follow-up services at least once. A total of 269 patients died of an unintentional opioid overdose within 1 year of their initial visit to the emergency department for an overdose and another 121 patients died from other causes.
At the time of their initial visit to the emergency department for an overdose, the majority of the 5,006 patients who were included in the study were men (77%) and were 45 years old or older (53%). Latino/a race was the most commonly reported, with 43% of patients identifying as such. For housing status, 43% reported being stably housed, 32% reported being unstably housed, and 25% reported living with others. Most patients reported that the drug they had intentionally taken that led to their initial overdose was any opioid (83%), with 68% reporting that they took heroin. Another 12% reported taking an opioid painkiller and 4% reported taking fentanyl. The most commonly reported route of administration upon the initial overdose was snorting (63%). The majority of patients reported that they have not experienced an overdose before (59%), were not currently prescribed medications for opioid use disorder (81%), and were not currently engaged with a syringe service program (95%).
WHAT DID THIS STUDY FIND?
Patients who were older and reported higher risk behaviors were more likely to consent to follow-up
There were demographic differences in the odds of consenting to Relay follow-up services. Compared to those who identified as White, people who identified as a different race were 33% less likely to consent to follow-up services. There were no other differences between races.
The odds of consenting to follow-up services were greater among patients who were older. Those who were in the 45-54, 55-64, and 65 years and older age groups were 44%, 61%, and 73% more likely to consent, respectively, than those who were in the 35-44 age group. There were no differences in odds of consenting for those in the 18-24 and 25-34 age groups, as compared to those in the 35-44 age group.
For housing status, those who reported being unstably housed were 31% more likely to consent to follow-up services than those who were stably housed. Those who reported living with others were 22% more likely to consent.
For overdose circumstances, patients who reported taking any opioid upon their initial overdose were 83% more likely to consent. Those who reported taking heroin specifically were twice as likely to consent and those who reported taking fentanyl were 49% more likely to consent. Meanwhile, those who reported taking cocaine or crack with no opioid were 44% less likely to consent, and those who reported an opioid painkiller were 25% less likely. Patients who reported snorting the drug upon overdose were 21% more likely to consent. While it is assumed that these characteristics are being compared to the absence of each characteristic (e.g., any opioid vs. no opioid), the study did not provide this information, making it unclear.
Finally, those who reported experiencing an overdose before were 78% more likely to consent to follow-up services than those who have not and those who were currently prescribed medications for opioid use disorder were 35% more likely than those who were not.
Patients who identified as Black and reported higher risk behaviors were less likely to be reached for follow-up
Among those who consented, there were demographic differences in the odds of being reached for Relay follow-up services. People who identified as Black were 19% less likely to be reached for follow-up services than those who identified as White. There were no other differences between races. There were also no differences between age groups in the odds of being reached for follow-up.
For housing status, those who reported being unstably housed were 52% less likely to be reached for follow-up services than those who were stably housed. Those who reported living with others were 18% less likely to be reached.
For overdose circumstances, patients who reported taking any opioid upon their initial overdose were 19% less likely to be reached for follow-up. Those who reported taking heroin specifically were 28% less likely to be reached. Meanwhile, those who reported taking cocaine or crack with no opioid were 33% more likely to be reached, and those who reported taking an opioid painkiller were 53% more likely to be reached. Patients who reported injecting the drug upon overdose were 28% less likely to be reached and those who reported smoking it were 34% less likely.
Finally, those who reported experiencing an overdose before were 19% less likely to be reached for follow-up services than those who have not and those who were currently engaged with a syringe service program were 33% less likely than those who were not.
Patients reached for follow-up services were less likely to experience a fatal overdose, but there were no differences between those who did and did not consent
In the analyses controlling for age, sex, and race/ethnicity, there were no differences in the risk of experiencing a fatal opioid overdose between patients who consented to receive Relay follow-up services and those who did not consent. However, among patients who consented, those who were reached for follow-up services at least once were 46% less likely to experience a fatal opioid overdose than those who were not reached.
There were no demographic differences in the risk of experiencing a fatal opioid overdose for sex, race/ethnicity, or housing status, but patients who were older had higher risks. Those who were in the age groups of 45-54, 55-64, and 65 years and older were 59%, 63%, and 92% more likely to experience a fatal overdose, respectively, than those in the 35-44 year age group.
For overdose circumstances, patients who reported intentionally taking any opioid upon their initial overdose were 66% more likely to experience a fatal overdose. Those who reported taking heroin specifically were 50% more likely. Meanwhile, those who reported taking cocaine or crack with no opioid were 44% less likely to experience a fatal overdose. As above, it is assumed that these characteristics are being compared to the absence of each characteristic (e.g., any opioid vs. no opioid), though this information was not explicitly provided.
Patients who reported experiencing an overdose before were 53% more likely to experience a fatal overdose than those who have not. Those who were currently prescribed medications for opioid use disorder were 42% less likely to experience a fatal overdose than those who were not, yet those who were currently engaged with a syringe service program were 65% more likely.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined demographic and substance use behavior differences between people who consented to and were reached for follow-up in Relay intervention services in NYC emergency departments between 2017 and 2022, and whether this engagement reduced risk of fatal overdose. Results showed that patients who reported higher risk substance use behaviors (e.g., intentional opioid use, past history of overdose) were more likely to consent to follow-up services, but less likely to actually receive them. This suggests that people who are at higher risk want to receive follow-up services, but face barriers to doing so, such as not having a reliable means of communication or transportation. This may also be due to the possibility of them dying from an overdose within the study period. These findings highlight the need for interventions to better address such barriers and that public health interventions may need to tailor their outreach efforts for people at highest risk.
Results of this study also showed, encouragingly, that patients who were reached for follow-up services were less likely to experience a fatal opioid overdose in the year following initial engagement with the Relay intervention. This demonstrates that providing peer-based follow-up services to people after surviving an opioid overdose can reduce the chances that they will experience a fatal opioid overdose. That said, it cannot be determined whether the Relay intervention was responsible for the reduced overdose risk. People who attended at least one follow-up session in the 90 days after their emergency department stay were likely to be more motivated, and thus, engaged in other types of substance use services. Note that these analyses only controlled for demographic characteristics, not clinical or recovery functioning ones.
That said, these findings may add to the research demonstrating the utility of hospital emergency departments for intervening with people with substance use disorders, particularly when they are delivered by peers. This is likely because emergency department services “meet people where they are”, when they are most in need. Likewise, interventions delivered by peers are likely to reduce the stigma some patients may feel and allow them to feel understood and supported.
The study was conducted in New York City, a large city in the US. Results may not generalize to other cities in the US, especially smaller cities, or other countries.
Because all patients included in the study received the intervention in the emergency department, the study design limits the extent to which the researchers can conclude that the intervention directly caused reductions in overdose risk.
The study design also limits the extent to which the researchers can conclude that the reduced overdose risk was attributable to the follow-up services, since people who are at highest risk are also hardest to reach. In other words, the people who were reached for follow-up services may have been lower risk anyway, regardless of the follow-up services.
The type and intensity of the follow-up services received were not examined. Patients who received only 1 brief follow-up were grouped with patients who may have received more frequent and in-depth follow-up services.
BOTTOM LINE
Patients who reported higher risk substance use behaviors were more likely to consent to receive follow-up services for a peer-based opioid overdose intervention, but less likely to actually receive them. However, patients who were reached for follow-up services were less likely to experience a fatal opioid overdose. These individuals likely had many other factors related to better outcomes, such as motivation and service involvement – thus, these findings should be replicated in an experimental study with a comparison group to determine whether it is useful. That said, these findings may highlight the need for interventions to better reach people who are at highest risk, while also demonstrating the potential public health benefits of follow-up services delivered by peers after an emergency department visit.
For individuals and families seeking recovery: This study shows that staying connected to follow-up services after a visit to the emergency department for a nonfatal opioid overdose can save lives. For people who use opioids at risk of overdose, engaging with peer-based support may reduce the chance of another overdose.
For treatment professionals and treatment systems: Even when patients who are at higher risk of overdose agree to follow-up, many are not ultimately reached, which reveals communication, transportation, and attitudinal barriers they likely face. Treatment professionals and systems who aim to address these barriers and tailor their outreach specifically for people at high risk may be more likely to reach them and reduce their overdose risk. Additionally, treatment systems that incorporate peer-based supports and engage people for follow-up services after surviving an opioid overdose may see reductions in overdose risk and public health benefits.
For scientists: Future research that tests the Relay intervention across diverse geographic settings and care environments can help shed light on the extent to which the results of the current setting generalize. Studies that employ designs capable of establishing causal links can help clarify the extent to which peer-based approaches are directly attributable to reduced risks for overdose deaths. Studies that examine the type and intensity of follow-up can deepen understanding of how frequent and intense follow-up services need to be for beneficial impacts.
For policy makers: Policymakers who support investments in peer recovery programs and infrastructure that helps address barriers to reaching people for follow-up services may help reduce deaths from opioid overdoses. Further, policymakers who support policies that promote hospital-based interventions delivered by peers can help close service gaps and may enhance public health.