“The long and winding road”: Native Americans have the furthest to travel for opioid use disorder medications
Among all race/ethnic groups in the US, American Indian/Alaska Native and Black populations have the highest rates of opioid overdose death. These disparities may be due to differences in access to treatment generally, and opioid use disorder medications specifically. This study examined differences in geographic proximity to opioid treatment programs and buprenorphine providers by race and ethnicity.
There has been an increase in racial disparities in opioid-involved overdose deaths with American Indian/Alaska Native and Black populations now having the highest rates of opioid overdose deaths of any race/ethnicity in the US. It is unclear why these groups have experienced a surge in opioid overdose deaths. One possible explanation for these findings is differences in opioid treatment program access. Prior to 2023, physicians could not prescribe medications to treat opioid use disorder (e.g., buprenorphine) without first receiving additional training and a waiver from the government. Such restrictions may have further burdened providers serving these communities which experience higher rates of poverty and marginalization than other groups, resulting in Native American/Black populations having to travel further to access treatment. This barrier could result in lower rates of opioid use disorder medication initiation and sustained engagement over time. To date, however, no studies have examined potential differences in geographic location between racial/ethnic groups. The present research offers insights on how the racial/ethnic characteristics of neighborhoods are associated with geographic distance to opioid treatment programs and buprenorphine providers in the US.
HOW WAS THIS STUDY CONDUCTED?
This study used an ecological cross-sectional design- publicly available data from multiple sources were merged to conduct secondary data analysis including 2019 US census tract data used to assess neighborhood characteristics. The study was conducted at the census block level (600-3000 people), resulting in 215,189 block groups. The authors excluded blocks from Alaska and Hawaii because >50 % of land area in Alaska and 10% of land area in Hawaii is not accessible by a road network. Therefore, road distance could not be computed for all block groups in these states. The study also excluded block groups with no population. Regional overdose deaths data were culled from The Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research. The location of opioid treatment programs and buprenorphine providers was derived from the Substance Abuse and Mental Health Services Administration.
The focus of this study was to examine geographic disparities in access to opioid treatment programs and buprenorphine providers by race and ethnicity, neighborhood deprivation, and rurality across the US. Using 2019 Census data the authors categorized block groups based on self-reported predominant racial/ethnic identity of residents. Predominant majority blocks consisted of blocks in which >50% of residents identified with one of racial/ethnic categories adapted from the U.S. Census: American Indian/Alaska Native, Asian, Black, White, Hispanic (regardless of racial identity), or no single racial majority. Block groups where no racial/ethnic identity was endorsed by most of the population were categorized as “no single racial majority”. The authors calculated the percentage of each race/ethnicity residing in census blocks as well. National overdose mortality data from 2019 were used to calculate mortality burden of blocks (e.g., higher, or lower than the national average). The Area Deprivation Index was also used to quantify the economic disadvantage of census blocks, a composite index aggregating factors such as employment, income, and housing. The rurality of census blocks was measured via Rural-Urban Commuting Area codes– a measurement system created by the US Department of Agriculture which measures population density, urbanization, and daily commuting of residents.
The primary outcome of the study was road network distance in miles between a census block group and the nearest opioid treatment program/buprenorphine provider. To measure this the authors geocoded the locations of 1643 opioid treatment providers – which dispense and oversee methadone for opioid use disorder in the US – and 37,692 buprenorphine providers. Next distances between blocks and treatment facilities were calculated using the road network dataset of North America (available on the Environmental Systems Research Institute ArcGIS software).
The researchers utilized statistical modeling to determine the association between racial/ethnic characteristics of census blocks and distance to the nearest source of opioid treatment. These models controlled for overdose cases, economic disadvantage, and rurality of blocks to isolate the effect of race/ethnicity. The authors also identified clusters of block groups with varying patterns of access to opioid treatment. Three patterns emerged from these analyses: clusters of block groups with shorter distances to opioid treatment providers (“hot spots”); block clusters with longer distances to opioid treatment programs (“cold spots”); and clusters which were neither classified as either hot or cold (“neutral zones”).
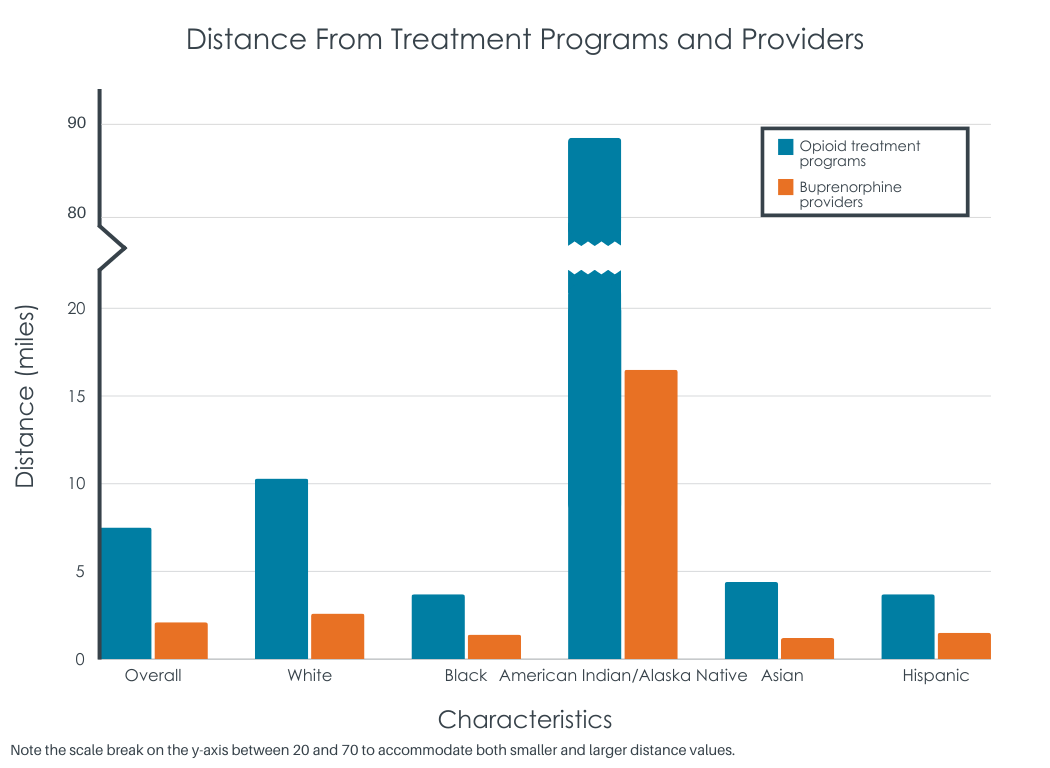
Analyses revealed that the median road distance between blocks and opioid treatment programs and buprenorphine providers was 8 miles (range 3-20) and 2 miles (range 1-5) respectively. Most of the blocks sampled had a majority White population (62.3%) followed by Hispanic (10.2%), no single race majority (11.5%), Black (8.8%), Asian (1.0%) and American Indian/Alaska Native (.2%). Most census blocks were classified as being in metropolitan areas (80.6%) with the remainder being suburban (13.6%) or rural areas (5.8%). Most census blocks were categorized as not being economically disadvantaged (69.4%). Census blocks were evenly split in terms of overdose deaths; 53.5% reported fewer overdose deaths than the national average, while 42.7% reported more (the remaining blocks had unknown rates of overdose deaths [3.8%]).
WHAT DID THIS STUDY FIND?
American Indian/Alaska Native people were the furthest, while other people of color were the closest
The median distance between majority American Indian/Alaska Native census blocks and the nearest opioid treatment program and buprenorphine providers was 88 and 17 miles, respectively. Statistical models showed that relative to White majority blocks, census blocks that were majority American Indian/Alaska Native were about 35.9 and 9.6 miles further from the nearest opioid treatment program and buprenorphine providers than White people respectively. In contrast, census blocks where other people of color lived were closer to such programs than White people. For example, majority Black blocks were about 5.5 miles closer to opioid treatment programs than White majority blocks.
Rural and economically disadvantaged census blocks were further than less disadvantaged areas
Areas designated as more economically disadvantaged were about 11.3 miles and 2.6 miles from the nearest opioid treatment programs and provider respectively. Census blocks that were less disadvantaged were about 6.9 and 1.9 miles from the nearest opioid treatment programs and provider respectively. Those living in areas designated as small town/rural had to travel 35 and 10 miles further to reach opioid treatment programs and opioid treatment providers respectively compared to metropolitan block groups.
Travel distance was greatest for American Indian/Alaska Native residents in rural, economically disadvantaged areas
In more disadvantaged block groups that contained 25% American Indian/Alaska Native residents, the average travel distance was 59 miles, while in block groups with 75% American Indian/Alaska Native residents, the distance was 84 miles. In small town/rural block groups with 25% American Indian/Alaska Native people, the mean distance to the nearest OTPs was 73 miles compared to 99 miles when 75% of block group residents were American Indian/Alaska Native.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that disparities in proximity to opioid treatment exist between race/ethnic, rural, and social class groups in the US. Residents of majority American Indian/Alaska Native census block groups (e.g., those living on reservations) were about 88 and 17 miles from the nearest opioid treatment program and buprenorphine provider, respectively. This is in stark contrast to other majority census block groups which were only about 4 to 10 miles from opioid treatment programs and buprenorphine providers respectively. They also found that the rurality and economic disadvantage of census blocks was associated with travel distance to opioid treatment. Those living in areas rural areas had to travel 35 and 10 miles further to reach opioid treatment programs and opioid treatment providers respectively compared to those living in cities/suburbs. Additionally, the researchers found that the economic disadvantage of a census block was associated with travel distance to opioid use disorder medication providers. Census blocks with more economic disadvantage were about 4 miles and 1.3 miles further from opioid treatment programs and providers respectively than less disadvantaged blocks. The researchers also found that people of color lived closer to sources of opioid medication than White Americans. For instance, Black census block residents lived 5.5 and 2 miles closer to opioid treatment programs and buprenorphine providers respectively than White residents. This finding cannot be explained purely by urban vs. rural location given that models controlled statistically for each block’s rural-urban profile.
It is important to point out, however, that this research also found that other people of color populations lived closer to opioid treatment resources than White Americans. Despite living near opioid treatment, these populations are known to access this care less than White Americans. For instance, research suggests that Black patients are less likely to be prescribed buprenorphine when presenting opioid use disorder symptoms in emergency rooms than White patients. This is especially noteworthy given that people of color continue to be heavily impacted by the opioid overdose epidemic. Taken together, the present research and the existing literature suggests that proximity to care is not the only barrier to treatment. It is possible that other barriers including social stigma of opioid use disorder and/or health insurance likely contribute to successfully receiving opioid use disorder treatment.
The study does not inform us of rates of treatment utilization. The authors used travel distance of opioid use disorder treatment centers as a proxy measure of access to care. However, it is unclear how many residents of sampled blocks used opioid addiction treatment. Therefore, it is unclear if the proximity of these sources of treatment was a factor in treatment usage.
The current study does not indicate how much of a barrier physical distance may be to opioid disorder treatment usage. The authors argue that increasing funding for IHS would improve opioid use treatment usage among American Indian/Alaska Native populations though reducing distance to treatment. However, other studies show that other communities of color living in closer proximity to treatment still do not utilize it. Therefore, it remains unclear how much increasing the availability of care will improve utilization.
The present study was conducted prior to the removal of X-Waiver registration, thereby the results may need to be updated as the opioid use disorder medication landscape shifts in response to this policy change. X-Waiver registration was certification physicians were required to attain before they could prescribe buprenorphine for opioid use disorder. Physicians can now prescribe buprenorphine to any patient for treating opioid use disorder.
BOTTOM LINE
Results suggest that disparities exist in travel distance to sources of opioid use disorder treatment between racial/ethnic composition, socioeconomic status, and rurality of census blocks in the US. Census blocks 1) with American Indian/Alaska Native residents, 2) situated in rural areas, and 3) that were economically disadvantaged were furthest from sources of opioid use disorder treatment. The researchers also found that census blocks in which other people of color resided were closer to opioid treatment programs and buprenorphine providers than those in which White and American Indian/Alaska Natives lived. Taken together, these results suggest that physical distance may serve as a barrier to substance use treatment. However, it is important to acknowledge that due to the recent changes in prescription policies for medications for opioid use disorders, the results should be replicated in this new policy landscape. More research is needed to better understand which barriers to care are most relevant for specific US-based populations, including but not limited to indigenous populations.
For individuals and families seeking recovery: The present research may suggest that access to opioid use disorder treatment is variable across the US. Specifically, those living in rural areas may find accessing such care challenging. Those living in said areas may do well to research all available treatment options, including utilizing telemedicine. Further, it may be important for patients from racial/ethnic minorities to ensure they receive necessary opioid use disorder treatment, those seeking care may need to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: The present study suggests that different groups in the US face barriers to accessing opioid use disorder treatment. Namely that American Indians/Alaska Natives and those in rural/economically disadvantaged areas may have to travel further to get treatment than others. Those providing treatment to and/or work in healthcare system settings serving these populations may want to consider ways to minimize the potential burden of travel among patients. This may include integrating telemedicine more into their practices. In addition, informing patients about potential travel reimbursement options may facilitate healthcare access.
For scientists: Scientists would do well to examine how proximity to opioid treatment options may serve as barrier to utilizing treatment. The extant literature already suggests that numerous barriers exist which reduce patients’ willingness to engage in care. Such barriers include perceived stigma of opioid use disorder and health insurance. To date, it is unclear how distance to sources of treatment may further limit healthcare usage. More research is needed to better understand which barriers to care are most relevant for specific populations.
For policy makers: Although this study suggests that differences exist in distance to sources of opioid use disorder treatment among racial/ethnic and socioeconomic groups in the US, it is unclear how these differences impact opioid use disorder treatment use. It is possible that increasing healthcare access (e.g., increase public clinics serving rural communities) may increase access to care. However, other barriers to care likely also contribute to treatment underutilization. Therefore, it may also be wise for policy makers to also try and minimize the impact of other barriers to care. For example, emulating state policies designed to reduce the social stigma associated with opioid use disorder. Such policies could include expansion of mandatory training for physicians on substance use disorders. Making regulatory flexibility regarding the prescription of medications like buprenorphine during telemedicine visits may also help address barriers to accessing care.
There has been an increase in racial disparities in opioid-involved overdose deaths with American Indian/Alaska Native and Black populations now having the highest rates of opioid overdose deaths of any race/ethnicity in the US. It is unclear why these groups have experienced a surge in opioid overdose deaths. One possible explanation for these findings is differences in opioid treatment program access. Prior to 2023, physicians could not prescribe medications to treat opioid use disorder (e.g., buprenorphine) without first receiving additional training and a waiver from the government. Such restrictions may have further burdened providers serving these communities which experience higher rates of poverty and marginalization than other groups, resulting in Native American/Black populations having to travel further to access treatment. This barrier could result in lower rates of opioid use disorder medication initiation and sustained engagement over time. To date, however, no studies have examined potential differences in geographic location between racial/ethnic groups. The present research offers insights on how the racial/ethnic characteristics of neighborhoods are associated with geographic distance to opioid treatment programs and buprenorphine providers in the US.
HOW WAS THIS STUDY CONDUCTED?
This study used an ecological cross-sectional design- publicly available data from multiple sources were merged to conduct secondary data analysis including 2019 US census tract data used to assess neighborhood characteristics. The study was conducted at the census block level (600-3000 people), resulting in 215,189 block groups. The authors excluded blocks from Alaska and Hawaii because >50 % of land area in Alaska and 10% of land area in Hawaii is not accessible by a road network. Therefore, road distance could not be computed for all block groups in these states. The study also excluded block groups with no population. Regional overdose deaths data were culled from The Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research. The location of opioid treatment programs and buprenorphine providers was derived from the Substance Abuse and Mental Health Services Administration.
The focus of this study was to examine geographic disparities in access to opioid treatment programs and buprenorphine providers by race and ethnicity, neighborhood deprivation, and rurality across the US. Using 2019 Census data the authors categorized block groups based on self-reported predominant racial/ethnic identity of residents. Predominant majority blocks consisted of blocks in which >50% of residents identified with one of racial/ethnic categories adapted from the U.S. Census: American Indian/Alaska Native, Asian, Black, White, Hispanic (regardless of racial identity), or no single racial majority. Block groups where no racial/ethnic identity was endorsed by most of the population were categorized as “no single racial majority”. The authors calculated the percentage of each race/ethnicity residing in census blocks as well. National overdose mortality data from 2019 were used to calculate mortality burden of blocks (e.g., higher, or lower than the national average). The Area Deprivation Index was also used to quantify the economic disadvantage of census blocks, a composite index aggregating factors such as employment, income, and housing. The rurality of census blocks was measured via Rural-Urban Commuting Area codes– a measurement system created by the US Department of Agriculture which measures population density, urbanization, and daily commuting of residents.
The primary outcome of the study was road network distance in miles between a census block group and the nearest opioid treatment program/buprenorphine provider. To measure this the authors geocoded the locations of 1643 opioid treatment providers – which dispense and oversee methadone for opioid use disorder in the US – and 37,692 buprenorphine providers. Next distances between blocks and treatment facilities were calculated using the road network dataset of North America (available on the Environmental Systems Research Institute ArcGIS software).
The researchers utilized statistical modeling to determine the association between racial/ethnic characteristics of census blocks and distance to the nearest source of opioid treatment. These models controlled for overdose cases, economic disadvantage, and rurality of blocks to isolate the effect of race/ethnicity. The authors also identified clusters of block groups with varying patterns of access to opioid treatment. Three patterns emerged from these analyses: clusters of block groups with shorter distances to opioid treatment providers (“hot spots”); block clusters with longer distances to opioid treatment programs (“cold spots”); and clusters which were neither classified as either hot or cold (“neutral zones”).
Analyses revealed that the median road distance between blocks and opioid treatment programs and buprenorphine providers was 8 miles (range 3-20) and 2 miles (range 1-5) respectively. Most of the blocks sampled had a majority White population (62.3%) followed by Hispanic (10.2%), no single race majority (11.5%), Black (8.8%), Asian (1.0%) and American Indian/Alaska Native (.2%). Most census blocks were classified as being in metropolitan areas (80.6%) with the remainder being suburban (13.6%) or rural areas (5.8%). Most census blocks were categorized as not being economically disadvantaged (69.4%). Census blocks were evenly split in terms of overdose deaths; 53.5% reported fewer overdose deaths than the national average, while 42.7% reported more (the remaining blocks had unknown rates of overdose deaths [3.8%]).
WHAT DID THIS STUDY FIND?
American Indian/Alaska Native people were the furthest, while other people of color were the closest
The median distance between majority American Indian/Alaska Native census blocks and the nearest opioid treatment program and buprenorphine providers was 88 and 17 miles, respectively. Statistical models showed that relative to White majority blocks, census blocks that were majority American Indian/Alaska Native were about 35.9 and 9.6 miles further from the nearest opioid treatment program and buprenorphine providers than White people respectively. In contrast, census blocks where other people of color lived were closer to such programs than White people. For example, majority Black blocks were about 5.5 miles closer to opioid treatment programs than White majority blocks.
Rural and economically disadvantaged census blocks were further than less disadvantaged areas
Areas designated as more economically disadvantaged were about 11.3 miles and 2.6 miles from the nearest opioid treatment programs and provider respectively. Census blocks that were less disadvantaged were about 6.9 and 1.9 miles from the nearest opioid treatment programs and provider respectively. Those living in areas designated as small town/rural had to travel 35 and 10 miles further to reach opioid treatment programs and opioid treatment providers respectively compared to metropolitan block groups.
Travel distance was greatest for American Indian/Alaska Native residents in rural, economically disadvantaged areas
In more disadvantaged block groups that contained 25% American Indian/Alaska Native residents, the average travel distance was 59 miles, while in block groups with 75% American Indian/Alaska Native residents, the distance was 84 miles. In small town/rural block groups with 25% American Indian/Alaska Native people, the mean distance to the nearest OTPs was 73 miles compared to 99 miles when 75% of block group residents were American Indian/Alaska Native.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that disparities in proximity to opioid treatment exist between race/ethnic, rural, and social class groups in the US. Residents of majority American Indian/Alaska Native census block groups (e.g., those living on reservations) were about 88 and 17 miles from the nearest opioid treatment program and buprenorphine provider, respectively. This is in stark contrast to other majority census block groups which were only about 4 to 10 miles from opioid treatment programs and buprenorphine providers respectively. They also found that the rurality and economic disadvantage of census blocks was associated with travel distance to opioid treatment. Those living in areas rural areas had to travel 35 and 10 miles further to reach opioid treatment programs and opioid treatment providers respectively compared to those living in cities/suburbs. Additionally, the researchers found that the economic disadvantage of a census block was associated with travel distance to opioid use disorder medication providers. Census blocks with more economic disadvantage were about 4 miles and 1.3 miles further from opioid treatment programs and providers respectively than less disadvantaged blocks. The researchers also found that people of color lived closer to sources of opioid medication than White Americans. For instance, Black census block residents lived 5.5 and 2 miles closer to opioid treatment programs and buprenorphine providers respectively than White residents. This finding cannot be explained purely by urban vs. rural location given that models controlled statistically for each block’s rural-urban profile.
It is important to point out, however, that this research also found that other people of color populations lived closer to opioid treatment resources than White Americans. Despite living near opioid treatment, these populations are known to access this care less than White Americans. For instance, research suggests that Black patients are less likely to be prescribed buprenorphine when presenting opioid use disorder symptoms in emergency rooms than White patients. This is especially noteworthy given that people of color continue to be heavily impacted by the opioid overdose epidemic. Taken together, the present research and the existing literature suggests that proximity to care is not the only barrier to treatment. It is possible that other barriers including social stigma of opioid use disorder and/or health insurance likely contribute to successfully receiving opioid use disorder treatment.
The study does not inform us of rates of treatment utilization. The authors used travel distance of opioid use disorder treatment centers as a proxy measure of access to care. However, it is unclear how many residents of sampled blocks used opioid addiction treatment. Therefore, it is unclear if the proximity of these sources of treatment was a factor in treatment usage.
The current study does not indicate how much of a barrier physical distance may be to opioid disorder treatment usage. The authors argue that increasing funding for IHS would improve opioid use treatment usage among American Indian/Alaska Native populations though reducing distance to treatment. However, other studies show that other communities of color living in closer proximity to treatment still do not utilize it. Therefore, it remains unclear how much increasing the availability of care will improve utilization.
The present study was conducted prior to the removal of X-Waiver registration, thereby the results may need to be updated as the opioid use disorder medication landscape shifts in response to this policy change. X-Waiver registration was certification physicians were required to attain before they could prescribe buprenorphine for opioid use disorder. Physicians can now prescribe buprenorphine to any patient for treating opioid use disorder.
BOTTOM LINE
Results suggest that disparities exist in travel distance to sources of opioid use disorder treatment between racial/ethnic composition, socioeconomic status, and rurality of census blocks in the US. Census blocks 1) with American Indian/Alaska Native residents, 2) situated in rural areas, and 3) that were economically disadvantaged were furthest from sources of opioid use disorder treatment. The researchers also found that census blocks in which other people of color resided were closer to opioid treatment programs and buprenorphine providers than those in which White and American Indian/Alaska Natives lived. Taken together, these results suggest that physical distance may serve as a barrier to substance use treatment. However, it is important to acknowledge that due to the recent changes in prescription policies for medications for opioid use disorders, the results should be replicated in this new policy landscape. More research is needed to better understand which barriers to care are most relevant for specific US-based populations, including but not limited to indigenous populations.
For individuals and families seeking recovery: The present research may suggest that access to opioid use disorder treatment is variable across the US. Specifically, those living in rural areas may find accessing such care challenging. Those living in said areas may do well to research all available treatment options, including utilizing telemedicine. Further, it may be important for patients from racial/ethnic minorities to ensure they receive necessary opioid use disorder treatment, those seeking care may need to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: The present study suggests that different groups in the US face barriers to accessing opioid use disorder treatment. Namely that American Indians/Alaska Natives and those in rural/economically disadvantaged areas may have to travel further to get treatment than others. Those providing treatment to and/or work in healthcare system settings serving these populations may want to consider ways to minimize the potential burden of travel among patients. This may include integrating telemedicine more into their practices. In addition, informing patients about potential travel reimbursement options may facilitate healthcare access.
For scientists: Scientists would do well to examine how proximity to opioid treatment options may serve as barrier to utilizing treatment. The extant literature already suggests that numerous barriers exist which reduce patients’ willingness to engage in care. Such barriers include perceived stigma of opioid use disorder and health insurance. To date, it is unclear how distance to sources of treatment may further limit healthcare usage. More research is needed to better understand which barriers to care are most relevant for specific populations.
For policy makers: Although this study suggests that differences exist in distance to sources of opioid use disorder treatment among racial/ethnic and socioeconomic groups in the US, it is unclear how these differences impact opioid use disorder treatment use. It is possible that increasing healthcare access (e.g., increase public clinics serving rural communities) may increase access to care. However, other barriers to care likely also contribute to treatment underutilization. Therefore, it may also be wise for policy makers to also try and minimize the impact of other barriers to care. For example, emulating state policies designed to reduce the social stigma associated with opioid use disorder. Such policies could include expansion of mandatory training for physicians on substance use disorders. Making regulatory flexibility regarding the prescription of medications like buprenorphine during telemedicine visits may also help address barriers to accessing care.
There has been an increase in racial disparities in opioid-involved overdose deaths with American Indian/Alaska Native and Black populations now having the highest rates of opioid overdose deaths of any race/ethnicity in the US. It is unclear why these groups have experienced a surge in opioid overdose deaths. One possible explanation for these findings is differences in opioid treatment program access. Prior to 2023, physicians could not prescribe medications to treat opioid use disorder (e.g., buprenorphine) without first receiving additional training and a waiver from the government. Such restrictions may have further burdened providers serving these communities which experience higher rates of poverty and marginalization than other groups, resulting in Native American/Black populations having to travel further to access treatment. This barrier could result in lower rates of opioid use disorder medication initiation and sustained engagement over time. To date, however, no studies have examined potential differences in geographic location between racial/ethnic groups. The present research offers insights on how the racial/ethnic characteristics of neighborhoods are associated with geographic distance to opioid treatment programs and buprenorphine providers in the US.
HOW WAS THIS STUDY CONDUCTED?
This study used an ecological cross-sectional design- publicly available data from multiple sources were merged to conduct secondary data analysis including 2019 US census tract data used to assess neighborhood characteristics. The study was conducted at the census block level (600-3000 people), resulting in 215,189 block groups. The authors excluded blocks from Alaska and Hawaii because >50 % of land area in Alaska and 10% of land area in Hawaii is not accessible by a road network. Therefore, road distance could not be computed for all block groups in these states. The study also excluded block groups with no population. Regional overdose deaths data were culled from The Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research. The location of opioid treatment programs and buprenorphine providers was derived from the Substance Abuse and Mental Health Services Administration.
The focus of this study was to examine geographic disparities in access to opioid treatment programs and buprenorphine providers by race and ethnicity, neighborhood deprivation, and rurality across the US. Using 2019 Census data the authors categorized block groups based on self-reported predominant racial/ethnic identity of residents. Predominant majority blocks consisted of blocks in which >50% of residents identified with one of racial/ethnic categories adapted from the U.S. Census: American Indian/Alaska Native, Asian, Black, White, Hispanic (regardless of racial identity), or no single racial majority. Block groups where no racial/ethnic identity was endorsed by most of the population were categorized as “no single racial majority”. The authors calculated the percentage of each race/ethnicity residing in census blocks as well. National overdose mortality data from 2019 were used to calculate mortality burden of blocks (e.g., higher, or lower than the national average). The Area Deprivation Index was also used to quantify the economic disadvantage of census blocks, a composite index aggregating factors such as employment, income, and housing. The rurality of census blocks was measured via Rural-Urban Commuting Area codes– a measurement system created by the US Department of Agriculture which measures population density, urbanization, and daily commuting of residents.
The primary outcome of the study was road network distance in miles between a census block group and the nearest opioid treatment program/buprenorphine provider. To measure this the authors geocoded the locations of 1643 opioid treatment providers – which dispense and oversee methadone for opioid use disorder in the US – and 37,692 buprenorphine providers. Next distances between blocks and treatment facilities were calculated using the road network dataset of North America (available on the Environmental Systems Research Institute ArcGIS software).
The researchers utilized statistical modeling to determine the association between racial/ethnic characteristics of census blocks and distance to the nearest source of opioid treatment. These models controlled for overdose cases, economic disadvantage, and rurality of blocks to isolate the effect of race/ethnicity. The authors also identified clusters of block groups with varying patterns of access to opioid treatment. Three patterns emerged from these analyses: clusters of block groups with shorter distances to opioid treatment providers (“hot spots”); block clusters with longer distances to opioid treatment programs (“cold spots”); and clusters which were neither classified as either hot or cold (“neutral zones”).
Analyses revealed that the median road distance between blocks and opioid treatment programs and buprenorphine providers was 8 miles (range 3-20) and 2 miles (range 1-5) respectively. Most of the blocks sampled had a majority White population (62.3%) followed by Hispanic (10.2%), no single race majority (11.5%), Black (8.8%), Asian (1.0%) and American Indian/Alaska Native (.2%). Most census blocks were classified as being in metropolitan areas (80.6%) with the remainder being suburban (13.6%) or rural areas (5.8%). Most census blocks were categorized as not being economically disadvantaged (69.4%). Census blocks were evenly split in terms of overdose deaths; 53.5% reported fewer overdose deaths than the national average, while 42.7% reported more (the remaining blocks had unknown rates of overdose deaths [3.8%]).
WHAT DID THIS STUDY FIND?
American Indian/Alaska Native people were the furthest, while other people of color were the closest
The median distance between majority American Indian/Alaska Native census blocks and the nearest opioid treatment program and buprenorphine providers was 88 and 17 miles, respectively. Statistical models showed that relative to White majority blocks, census blocks that were majority American Indian/Alaska Native were about 35.9 and 9.6 miles further from the nearest opioid treatment program and buprenorphine providers than White people respectively. In contrast, census blocks where other people of color lived were closer to such programs than White people. For example, majority Black blocks were about 5.5 miles closer to opioid treatment programs than White majority blocks.
Rural and economically disadvantaged census blocks were further than less disadvantaged areas
Areas designated as more economically disadvantaged were about 11.3 miles and 2.6 miles from the nearest opioid treatment programs and provider respectively. Census blocks that were less disadvantaged were about 6.9 and 1.9 miles from the nearest opioid treatment programs and provider respectively. Those living in areas designated as small town/rural had to travel 35 and 10 miles further to reach opioid treatment programs and opioid treatment providers respectively compared to metropolitan block groups.
Travel distance was greatest for American Indian/Alaska Native residents in rural, economically disadvantaged areas
In more disadvantaged block groups that contained 25% American Indian/Alaska Native residents, the average travel distance was 59 miles, while in block groups with 75% American Indian/Alaska Native residents, the distance was 84 miles. In small town/rural block groups with 25% American Indian/Alaska Native people, the mean distance to the nearest OTPs was 73 miles compared to 99 miles when 75% of block group residents were American Indian/Alaska Native.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that disparities in proximity to opioid treatment exist between race/ethnic, rural, and social class groups in the US. Residents of majority American Indian/Alaska Native census block groups (e.g., those living on reservations) were about 88 and 17 miles from the nearest opioid treatment program and buprenorphine provider, respectively. This is in stark contrast to other majority census block groups which were only about 4 to 10 miles from opioid treatment programs and buprenorphine providers respectively. They also found that the rurality and economic disadvantage of census blocks was associated with travel distance to opioid treatment. Those living in areas rural areas had to travel 35 and 10 miles further to reach opioid treatment programs and opioid treatment providers respectively compared to those living in cities/suburbs. Additionally, the researchers found that the economic disadvantage of a census block was associated with travel distance to opioid use disorder medication providers. Census blocks with more economic disadvantage were about 4 miles and 1.3 miles further from opioid treatment programs and providers respectively than less disadvantaged blocks. The researchers also found that people of color lived closer to sources of opioid medication than White Americans. For instance, Black census block residents lived 5.5 and 2 miles closer to opioid treatment programs and buprenorphine providers respectively than White residents. This finding cannot be explained purely by urban vs. rural location given that models controlled statistically for each block’s rural-urban profile.
It is important to point out, however, that this research also found that other people of color populations lived closer to opioid treatment resources than White Americans. Despite living near opioid treatment, these populations are known to access this care less than White Americans. For instance, research suggests that Black patients are less likely to be prescribed buprenorphine when presenting opioid use disorder symptoms in emergency rooms than White patients. This is especially noteworthy given that people of color continue to be heavily impacted by the opioid overdose epidemic. Taken together, the present research and the existing literature suggests that proximity to care is not the only barrier to treatment. It is possible that other barriers including social stigma of opioid use disorder and/or health insurance likely contribute to successfully receiving opioid use disorder treatment.
The study does not inform us of rates of treatment utilization. The authors used travel distance of opioid use disorder treatment centers as a proxy measure of access to care. However, it is unclear how many residents of sampled blocks used opioid addiction treatment. Therefore, it is unclear if the proximity of these sources of treatment was a factor in treatment usage.
The current study does not indicate how much of a barrier physical distance may be to opioid disorder treatment usage. The authors argue that increasing funding for IHS would improve opioid use treatment usage among American Indian/Alaska Native populations though reducing distance to treatment. However, other studies show that other communities of color living in closer proximity to treatment still do not utilize it. Therefore, it remains unclear how much increasing the availability of care will improve utilization.
The present study was conducted prior to the removal of X-Waiver registration, thereby the results may need to be updated as the opioid use disorder medication landscape shifts in response to this policy change. X-Waiver registration was certification physicians were required to attain before they could prescribe buprenorphine for opioid use disorder. Physicians can now prescribe buprenorphine to any patient for treating opioid use disorder.
BOTTOM LINE
Results suggest that disparities exist in travel distance to sources of opioid use disorder treatment between racial/ethnic composition, socioeconomic status, and rurality of census blocks in the US. Census blocks 1) with American Indian/Alaska Native residents, 2) situated in rural areas, and 3) that were economically disadvantaged were furthest from sources of opioid use disorder treatment. The researchers also found that census blocks in which other people of color resided were closer to opioid treatment programs and buprenorphine providers than those in which White and American Indian/Alaska Natives lived. Taken together, these results suggest that physical distance may serve as a barrier to substance use treatment. However, it is important to acknowledge that due to the recent changes in prescription policies for medications for opioid use disorders, the results should be replicated in this new policy landscape. More research is needed to better understand which barriers to care are most relevant for specific US-based populations, including but not limited to indigenous populations.
For individuals and families seeking recovery: The present research may suggest that access to opioid use disorder treatment is variable across the US. Specifically, those living in rural areas may find accessing such care challenging. Those living in said areas may do well to research all available treatment options, including utilizing telemedicine. Further, it may be important for patients from racial/ethnic minorities to ensure they receive necessary opioid use disorder treatment, those seeking care may need to be cognizant of what their needs are and how best to communicate these to their healthcare provider.
For treatment professionals and treatment systems: The present study suggests that different groups in the US face barriers to accessing opioid use disorder treatment. Namely that American Indians/Alaska Natives and those in rural/economically disadvantaged areas may have to travel further to get treatment than others. Those providing treatment to and/or work in healthcare system settings serving these populations may want to consider ways to minimize the potential burden of travel among patients. This may include integrating telemedicine more into their practices. In addition, informing patients about potential travel reimbursement options may facilitate healthcare access.
For scientists: Scientists would do well to examine how proximity to opioid treatment options may serve as barrier to utilizing treatment. The extant literature already suggests that numerous barriers exist which reduce patients’ willingness to engage in care. Such barriers include perceived stigma of opioid use disorder and health insurance. To date, it is unclear how distance to sources of treatment may further limit healthcare usage. More research is needed to better understand which barriers to care are most relevant for specific populations.
For policy makers: Although this study suggests that differences exist in distance to sources of opioid use disorder treatment among racial/ethnic and socioeconomic groups in the US, it is unclear how these differences impact opioid use disorder treatment use. It is possible that increasing healthcare access (e.g., increase public clinics serving rural communities) may increase access to care. However, other barriers to care likely also contribute to treatment underutilization. Therefore, it may also be wise for policy makers to also try and minimize the impact of other barriers to care. For example, emulating state policies designed to reduce the social stigma associated with opioid use disorder. Such policies could include expansion of mandatory training for physicians on substance use disorders. Making regulatory flexibility regarding the prescription of medications like buprenorphine during telemedicine visits may also help address barriers to accessing care.