Opioid use disorder medications more likely received in outpatient than residential treatment patients, but helpful for both
Initiating medications in outpatient treatment settings may result in the best opioid use disorder outcomes, rather than more expensive treatment in residential settings. This study examined whether outcomes for Medicaid beneficiaries receiving treatment for opioid use disorder differed when it was delivered in an outpatient or a residential setting.
Despite medications being the gold standard treatment for opioid use disorder, it is estimated that 87% of individuals who may benefit from medication treatment do not receive it — either because they do not have access or choose not to take it if they do have access. Several approaches may be needed to address this treatment gap. For example, treatment for opioid use disorder may be initiated and delivered in different healthcare settings, including outpatient and residential settings. Although treatment in outpatient settings has been increasing, many individuals, especially those with more severe and often complex profiles, are still treated in residential settings. These settings can offer greater protection against any use while in this more controlled environment, while also providing more structured treatment content (e.g., groups, sessions, etc.) in a shorter period of time. However, less than one third of residential treatment settings offer FDA-approved medication for opioid use disorder. Initiating medication treatment for opioid use disorder in outpatient settings may be superior to other treatment settings, possibly due to a more conducive clinical culture and treatment infrastructure focused on medication use. In this study, researchers examined the association between treatment setting and opioid-related outcomes among Oregon Medicaid beneficiaries with opioid use disorder. Results could potentially provide insight into the most important types of treatment models to scale up to adequately address the large treatment gap among people with opioid use disorder in the United States.
HOW WAS THIS STUDY CONDUCTED?
This was a retrospective cohort study that linked several databases together to examine if opioid-related outcomes differed for Oregon Medicaid beneficiaries who received outpatient or residential treatment. The researchers were also interested in how medications may have influenced the relationship between treatment setting and opioid-related outcomes.
The researchers linked several databases to provide rich data on Oregon Medicaid beneficiaries with opioid use disorder who received treatment from July 2014 to June 2017 as part of the National Drug Abuse Treatment Clinical Trials Network “In and Out Study”, including Medicaid claims data, the Treatment Episode Data Set, and death certificate data from Oregon. The researchers used Medicaid claims data to identify opioid use disorder diagnoses, treatment for this disorder in either an outpatient or residential setting, if a medication prescription was filled during the treatment episode, a range of physical and mental comorbidities that may impact treatment setting and/or outcomes (which were combined to create a composite score known as the Elixhauser Comorbidity Index), and all opioid-related outcomes except for opioid overdose fatalities. The researchers used admission data from the Treatment Episode Data Set to ascertain more detailed information about the patient’s opioid use disorder, such as opioid type, other substances used, frequency and history of opioid use, and injection drug use. The researchers used death certificate data to identify opioid overdose fatalities.
The variable of interest in this study was whether someone received either residential or outpatient treatment for opioid use disorder. The primary outcome of interest was opioid overdose – both fatal and non-fatal. Secondary outcomes of interest included non-overdose opioid-related emergency department visits and hospitalizations as well as any emergency department visits and hospitalization. They also examined treatment retention in a sub-group of patients who received Medicaid for at least 1 year defined as the period of time over which they had insurance claims for any type of substance use disorder treatment, including psychosocial services or medication.
Medicaid beneficiaries were included in the study sample if they had at least 180 days of Medicaid enrollment before their index treatment date (defined as their first treatment encounter if there were more than one treatment episodes during the study period), if they had a diagnosis of opioid use disorder, and if they had a Medicaid claim for a residential treatment stay or an outpatient treatment encounter. Patients were excluded from the sample if they did not have an appropriate admission record in the Treatment Episode Data Set that indicated opioids as a problem substance, and this admission had to occur after 2014 and up to 7 days following the index treatment date.
The study protocol identified 3,293 Medicaid beneficiaries in Oregon who met the study criteria, with 2,336 individuals receiving residential treatment and 957 individuals receiving outpatient treatment for opioid use disorder. Compared to those in outpatient treatment, individuals receiving residential treatment tended to be younger and had clinical characteristics indicative of more complicated cases of opioid use disorder, such as higher rates of depression, higher rates of heroin and stimulant use, and higher rates of injection drug use. Also, rates of prior inpatient medically supervised withdrawal were sixfold higher for individuals receiving treatment in residential settings compared with outpatient settings. For the secondary outcome of treatment retention, only those individuals who were enrolled in Medicaid a full year after the index treatment date were analyzed, limiting the sample to 1,913 individuals.
The research team examined the association between treatment setting and opioid-related outcomes, controlling for baseline demographics (age, race, sex), Elixhauser comorbidity score, opioid use disorder and other substance use characteristics from the Treatment Episode Data Set (e.g., injection drug use), medication use, and medically managed withdrawal immediately preceding the treatment episode. The models also controlled for all-cause and opioid-related emergency department visits and hospitalizations in the 180 days prior to the index treatment date as additional measures to capture potential clinical differences between individuals in each treatment setting.
Since previous research has identified medication as a vital component of opioid use disorder, the researchers stratified their analysis by whether or not medication was used, and also used an interaction term in the models to examine if medication use modified the relationship between treatment setting and each opioid-related outcome. In this study, medication use was measured as an insurance claim for one of the three FDA-approved medications for opioid use disorder including methadone, buprenorphine, and extended-release naltrexone. Therefore, we do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed).
WHAT DID THIS STUDY FIND?
Opioid-related patient outcomes were similar in outpatient and residential treatment.
The outcome of interest, the rate of both fatal and nonfatal opioid overdoses, was not different between individuals receiving opioid use disorder treatment in residential settings and those receiving treatment in outpatient settings. There was also not a difference in opioid-related emergency department visits and hospitalizations between the two treatment settings. However, the interaction with medication use was significant, suggesting that among individuals receiving medications, patients receiving residential treatment had a higher risk of an opioid-related emergency department visit and hospitalization compared to patients receiving outpatient treatment, although severity of opioid use disorder was not directly controlled for. Also, the rate of all-cause emergency department visits and hospitalizations was higher in residential settings compared with outpatient settings.
Treatment retention was higher in residential settings at 6 months, but not 12 months.
However, the results suggest that the benefits of residential treatment on treatment retention, measured as engagement in all treatment across any treatment setting including provision of medications, were limited to individuals who were not receiving medications such that that those who did not receive medication in residential settings had longer periods of treatment retention, on average, than those who did receive medication.
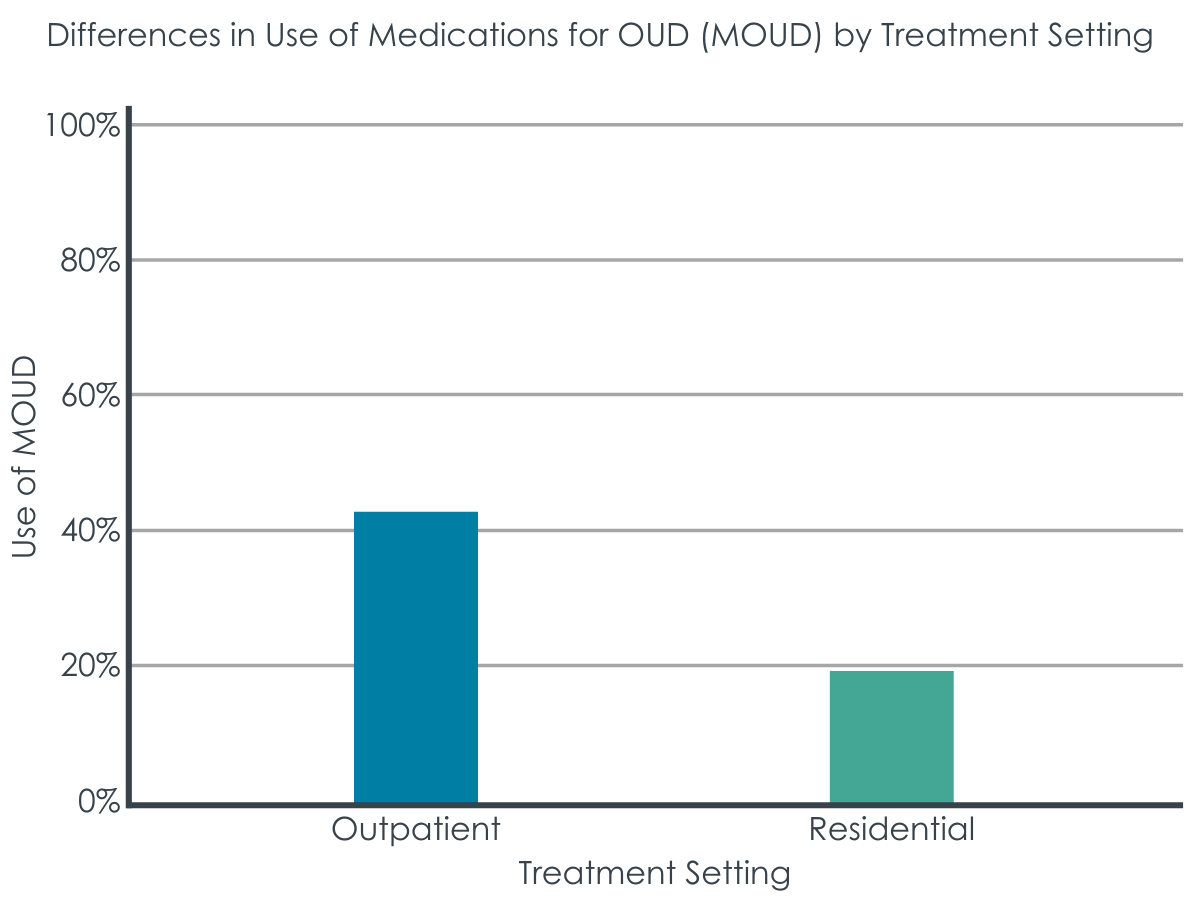
Medication use was low overall, but higher in outpatient settings.
Only 36% of individuals receiving residential or outpatient treatment for opioid use disorder received medications, with this rate higher in outpatient settings (43%) than residential settings (19%). The most commonly used medication was buprenorphine, followed by methadone, with use of extended-release naltrexone very rare. Although the rate of methadone use was similar across treatment settings, the rate of buprenorphine use was 32% in outpatient settings and 9% in residential settings.
Medication use, independent of treatment setting, was associated with a substantial reduction in overdose risk.
Receiving medication (primarily methadone or buprenorphine), regardless of treatment setting, was associated with a significant reduction in the rate of both fatal and nonfatal opioid overdoses, with around half as many of those receiving medications experiencing an opioid overdose compared to those not receiving medications, or stated differently, a 55% reduction in the risk of opioid overdose independent of treatment setting.
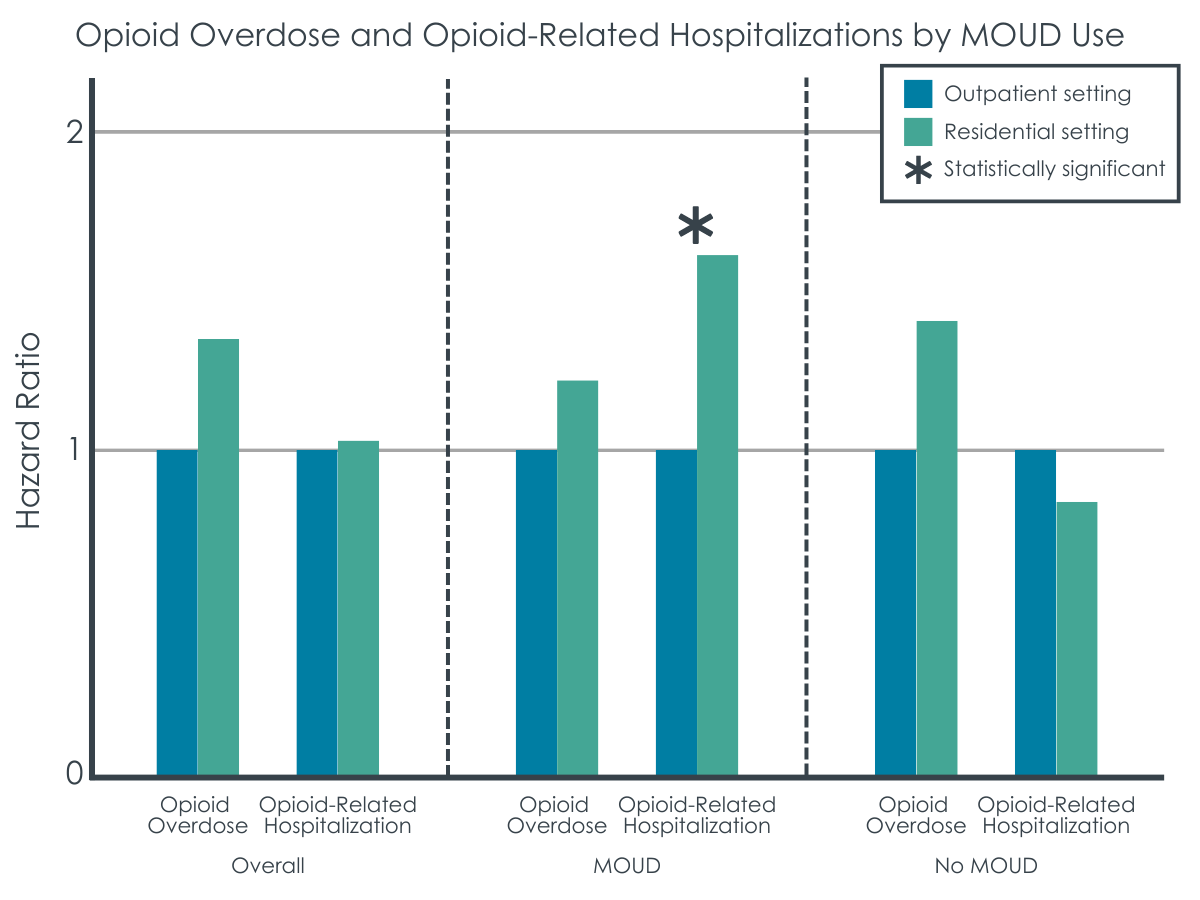
Figure 2. Hazard ratios are essentially used to determine how often something happens in one group compared to another. The way to interpret them is that with 1 as the baseline, anything above 1 indicates more occurrences, while anything below 1 indicates less occurrences. In this instance, only the difference in opioid-related hospitalizations between residential and outpatient treatment in the MOUD condition was statistically significant.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The researchers found that rates of opioid-related outcomes for patients with opioid use disorder receiving residential treatment were no better than patients receiving outpatient treatment. That said, the patients in residential treatments had substantially more severe and complex clinical profiles than those entering outpatient treatment. Thus, having similar outcomes despite greater impairment could be considered a positive. The research team did try to control statistically for a variety of severity indicators in the analyses to try and eradicate this potential confound, but these often cannot capture all of the important nuances that affect outcomes that are associated with such impairment. This is an important limitation in this kind of study design. With this in mind, although medication use was low in both treatment settings, especially residential treatment, use of medications such as buprenorphine or methadone was associated with a 55% reduction in the risk of opioid overdose. As alluded to above, there are obvious self-selection biases operating here that could confound this relationship (i.e., patients most motivated for treatment and overdose prevention might be those using the medication). This large risk reduction is consistent with other large randomized clinical samples, where studies consistently show opioid agonist medications reduce overdose risk by approximately 50%.
The study findings suggest that when targeting crucial outcomes of overdose and emergency department visits, a treatment model that combines outpatient treatment and medication like buprenorphine or methadone may be a better option for most individuals with opioid use disorder rather than more intensive and expensive treatment in a residential setting. This treatment model has been found to be superior to inpatient detox only, residential treatment without medications, or outpatient behavioral health counseling without medications. However, residential treatment facilities should not be ruled out for patients with more severe profiles, such as injection drug use, certain comorbidities (e.g., having other additional severe substance use disorders), and some unique challenges like unstable housing, so long as medications are made available in these settings. In addition, many people with opioid use disorder are not interested in medication treatment, so we need to understand what treatment alternatives are most helpful for these patients.
Most of the outcomes examined were similar in both treatment settings, which has also been shown for individuals with substance use disorder more generally. However, this study did find that among individuals receiving medications, outpatient treatment was associated with less opioid-related hospital use compared to patients treated in a residential setting, and also that, overall, all-cause hospital use was lower in individuals receiving treatment in outpatient settings compared with residential. These findings suggest that there was actually some benefit to outpatient treatment compared to residential treatment for people with opioid use disorder and is similar to findings among commercial beneficiaries nationally. However, as noted earlier, this finding should be interpreted with caution as it may have been due to greater severity in the residential treatment group that was unable to be accounted for adequately in the analysis. More research is needed on identifying subsets of patients that may benefit from residential treatment and how these findings might translate to more recent years in the context of fentanyl inundating the illicit opioid supply.
In this study, treatment in outpatient and residential settings was examined, but this study did not assess the types of services received during these treatment episodes nor did it capture opioid use disorder treatment that may be delivered outside of these settings. Other studies point to ways to improve medication’s benefits, including contingency management and participation in mutual help organizations. Also, recent research has suggested that a “medication first” approach where patients are offered medications with no expectation for them to participate in other treatment services can produce similar outcomes to treatment as usual (e.g., medication plus required counseling). As an example, an individual might receive treatment with buprenorphine at a private doctor’s office with only medication management. However, this approach may not be ideal for more severe and complicated patients.
Only 36% of patients with opioid use disorder who received treatment in residential or outpatient settings received medications, with this rate much higher in outpatient treatment settings compared with residential treatment settings. However, a limitation of this study is that all we know is that the patient was dispensed the medication from a pharmacy, which would appear as an insurance claim, but we do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed). More research is needed into the myriad ways to increase medication uptake beyond availability. Although future studies should identify patients who are most likely to benefit from residential treatment, a more effective strategy that may represent low-hanging fruit for many residential treatment facilities is to ensure that medication is delivered in conjunction with other treatment services. Other research has shown that medications can augment residential treatment. In addition, although higher than residential treatment, medication use in outpatient settings was low and represents a missed opportunity to initiate an evidence-based treatment.
The way that medication use for opioid use disorder was measured in this study, we only know that a patient was dispensed the medication from a pharmacy, which would be captured as an insurance claim, but do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed).
Treatment retention was measured as engagement in all treatment across any treatment setting, including provision of medication. Since many individuals stay on medications long-term, this could have biased the comparison of treatment retention between patients on medications and not on medications.
Although the researchers used several different clinical characteristics to capture the substance use profile of the patients, there was no direct measure for severity of opioid use disorder (e.g., mild, moderate, or severe).
This was a naturalistic observational study and although the research team tried to control for the substantial severity differences between patients treated in residential and outpatient settings findings are still very likely to be affected by selection bias and confounding.
The outcome of interest, both fatal and nonfatal opioid overdoses, is likely undercounted because many people who experience a nonfatal opioid overdose do not seek medical attention. In addition, the outcome of interest was rare (n=56) limiting the statistical power of the study.
This study was not able to capture other services that individuals may have used to improve their well-being, such as recovery community centers or mutual help organizations. Nor did the study examine other settings where medications might be delivered, such as a private doctor’s office.
This study was done on Medicaid beneficiaries in one state (Oregon). Generalizing results to individuals with other types of insurance (e.g., commercial, Medicare), to other states, or nationally should be done with caution.
The study sample was limited to around half of Medicaid beneficiaries who were treated for opioid use disorder in residential or outpatient treatment settings and also had an admissions record in the Treatment Episode Data Set. This would introduce bias if people included in the study sample were very different from people who were not included in the study sample.
BOTTOM LINE
Rates of opioid-related outcomes for patients with opioid use disorder receiving residential treatment were found to be similar to patients receiving outpatient treatment. Given the big differences in clinical severity and complexity indicators among the two types of patient groups, this might be seen as a positive outcome experience for those more severe patients that were treated in residential settings. An alternative explanation is that these similar outcomes may be explained by greater use of opioid use disorder medications in outpatient settings, which helped to compensate, or overcome, the less intensive and structured treatment that is present in residential settings. Although medication use was low in both treatment settings, especially residential treatment, and this study was not randomized or otherwise able to be well controlled from a statistical standpoint, consistent with other large clinical samples, use of medications such as buprenorphine or methadone was associated with a 55% reduction in the risk of opioid overdose in the current study – a figure consistent with more well controlled and randomized investigations.
For individuals and families seeking recovery: Study findings showed that, on average, treatment received for opioid use disorder in a residential setting was similar to treatment received in an outpatient setting. Whereas this might be considered a positive outcome for the much more severe residential patients, another possible explanation is that the equally positive outcomes for those receiving the less expensive and less structured outpatient treatment was due to medication use. Although some people with severe opioid use disorder along with other comorbidities and social determinants of health barriers (e.g., unstable housing, unemployed) may still benefit from residential treatment, outpatient treatment combined with medication use may be the best and most inexpensive treatment model to reduce overdose risk and healthcare costs for many people with opioid use disorder.
For treatment professionals and treatment systems: Healthcare systems might consider focusing on expanding outpatient treatment for opioid use disorder where medications can also be initiated and continued, while also ensuring that medications are available in existing residential treatment facilities. Treatment professionals might consider recommending residential treatment for opioid use disorder along with medication use, especially for patients without severe substance use profiles, such as injection drug use, certain comorbidities (e.g., co-occurring substance use disorders, and/or mental health conditions), and some unique challenges (e.g., unstable housing).
For scientists: This study used a survival analysis to examine the association between opioid-related outcomes and treatment setting, an interaction term to explore how medication use modified this association, and multivariable logistic regression to examine the association between treatment retention and treatment setting. More research is needed to see if this finding would be replicated in states apart from Oregon, given the unique state-level characteristics of Medicaid programs across states as well as the geographic variation of the presence of fentanyl in the illicit opioid supply. Also, there are significant confounds and challenges with the study design in being able to assert with confidence which types of patients would be best served in which type of setting. That said, opioid use disorder medications were associated with reduced overdose and the effect was similar in magnitude with prior experimental and well controlled research designs. More research is needed to identify characteristics of patients who would benefit most from residential treatment, as well as how best to help the many patients who are medication-reluctant.
For policy makers: Policies and interventions that increase medication use in both outpatient and residential treatment settings are likely to be most impactful for people with opioid use disorder. Importantly, this would include expanding availability of medications in these treatment settings but also might include increasing clinical and patient buy-in for medication use. Although more research is needed, some people, especially those with severe clinical characteristics and challenges such as homelessness, are likely to be better fits for residential treatment so long as medications are also made available to prioritize reduce overdose risk. Policymakers may be able to use funding mechanisms, such as making the receipt of federal or state grant money contingent on providing evidence-based treatments, to increase the use of medications for opioid use disorder in all treatment settings.
Despite medications being the gold standard treatment for opioid use disorder, it is estimated that 87% of individuals who may benefit from medication treatment do not receive it — either because they do not have access or choose not to take it if they do have access. Several approaches may be needed to address this treatment gap. For example, treatment for opioid use disorder may be initiated and delivered in different healthcare settings, including outpatient and residential settings. Although treatment in outpatient settings has been increasing, many individuals, especially those with more severe and often complex profiles, are still treated in residential settings. These settings can offer greater protection against any use while in this more controlled environment, while also providing more structured treatment content (e.g., groups, sessions, etc.) in a shorter period of time. However, less than one third of residential treatment settings offer FDA-approved medication for opioid use disorder. Initiating medication treatment for opioid use disorder in outpatient settings may be superior to other treatment settings, possibly due to a more conducive clinical culture and treatment infrastructure focused on medication use. In this study, researchers examined the association between treatment setting and opioid-related outcomes among Oregon Medicaid beneficiaries with opioid use disorder. Results could potentially provide insight into the most important types of treatment models to scale up to adequately address the large treatment gap among people with opioid use disorder in the United States.
HOW WAS THIS STUDY CONDUCTED?
This was a retrospective cohort study that linked several databases together to examine if opioid-related outcomes differed for Oregon Medicaid beneficiaries who received outpatient or residential treatment. The researchers were also interested in how medications may have influenced the relationship between treatment setting and opioid-related outcomes.
The researchers linked several databases to provide rich data on Oregon Medicaid beneficiaries with opioid use disorder who received treatment from July 2014 to June 2017 as part of the National Drug Abuse Treatment Clinical Trials Network “In and Out Study”, including Medicaid claims data, the Treatment Episode Data Set, and death certificate data from Oregon. The researchers used Medicaid claims data to identify opioid use disorder diagnoses, treatment for this disorder in either an outpatient or residential setting, if a medication prescription was filled during the treatment episode, a range of physical and mental comorbidities that may impact treatment setting and/or outcomes (which were combined to create a composite score known as the Elixhauser Comorbidity Index), and all opioid-related outcomes except for opioid overdose fatalities. The researchers used admission data from the Treatment Episode Data Set to ascertain more detailed information about the patient’s opioid use disorder, such as opioid type, other substances used, frequency and history of opioid use, and injection drug use. The researchers used death certificate data to identify opioid overdose fatalities.
The variable of interest in this study was whether someone received either residential or outpatient treatment for opioid use disorder. The primary outcome of interest was opioid overdose – both fatal and non-fatal. Secondary outcomes of interest included non-overdose opioid-related emergency department visits and hospitalizations as well as any emergency department visits and hospitalization. They also examined treatment retention in a sub-group of patients who received Medicaid for at least 1 year defined as the period of time over which they had insurance claims for any type of substance use disorder treatment, including psychosocial services or medication.
Medicaid beneficiaries were included in the study sample if they had at least 180 days of Medicaid enrollment before their index treatment date (defined as their first treatment encounter if there were more than one treatment episodes during the study period), if they had a diagnosis of opioid use disorder, and if they had a Medicaid claim for a residential treatment stay or an outpatient treatment encounter. Patients were excluded from the sample if they did not have an appropriate admission record in the Treatment Episode Data Set that indicated opioids as a problem substance, and this admission had to occur after 2014 and up to 7 days following the index treatment date.
The study protocol identified 3,293 Medicaid beneficiaries in Oregon who met the study criteria, with 2,336 individuals receiving residential treatment and 957 individuals receiving outpatient treatment for opioid use disorder. Compared to those in outpatient treatment, individuals receiving residential treatment tended to be younger and had clinical characteristics indicative of more complicated cases of opioid use disorder, such as higher rates of depression, higher rates of heroin and stimulant use, and higher rates of injection drug use. Also, rates of prior inpatient medically supervised withdrawal were sixfold higher for individuals receiving treatment in residential settings compared with outpatient settings. For the secondary outcome of treatment retention, only those individuals who were enrolled in Medicaid a full year after the index treatment date were analyzed, limiting the sample to 1,913 individuals.
The research team examined the association between treatment setting and opioid-related outcomes, controlling for baseline demographics (age, race, sex), Elixhauser comorbidity score, opioid use disorder and other substance use characteristics from the Treatment Episode Data Set (e.g., injection drug use), medication use, and medically managed withdrawal immediately preceding the treatment episode. The models also controlled for all-cause and opioid-related emergency department visits and hospitalizations in the 180 days prior to the index treatment date as additional measures to capture potential clinical differences between individuals in each treatment setting.
Since previous research has identified medication as a vital component of opioid use disorder, the researchers stratified their analysis by whether or not medication was used, and also used an interaction term in the models to examine if medication use modified the relationship between treatment setting and each opioid-related outcome. In this study, medication use was measured as an insurance claim for one of the three FDA-approved medications for opioid use disorder including methadone, buprenorphine, and extended-release naltrexone. Therefore, we do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed).
WHAT DID THIS STUDY FIND?
Opioid-related patient outcomes were similar in outpatient and residential treatment.
The outcome of interest, the rate of both fatal and nonfatal opioid overdoses, was not different between individuals receiving opioid use disorder treatment in residential settings and those receiving treatment in outpatient settings. There was also not a difference in opioid-related emergency department visits and hospitalizations between the two treatment settings. However, the interaction with medication use was significant, suggesting that among individuals receiving medications, patients receiving residential treatment had a higher risk of an opioid-related emergency department visit and hospitalization compared to patients receiving outpatient treatment, although severity of opioid use disorder was not directly controlled for. Also, the rate of all-cause emergency department visits and hospitalizations was higher in residential settings compared with outpatient settings.
Treatment retention was higher in residential settings at 6 months, but not 12 months.
However, the results suggest that the benefits of residential treatment on treatment retention, measured as engagement in all treatment across any treatment setting including provision of medications, were limited to individuals who were not receiving medications such that that those who did not receive medication in residential settings had longer periods of treatment retention, on average, than those who did receive medication.
Medication use was low overall, but higher in outpatient settings.
Only 36% of individuals receiving residential or outpatient treatment for opioid use disorder received medications, with this rate higher in outpatient settings (43%) than residential settings (19%). The most commonly used medication was buprenorphine, followed by methadone, with use of extended-release naltrexone very rare. Although the rate of methadone use was similar across treatment settings, the rate of buprenorphine use was 32% in outpatient settings and 9% in residential settings.
Medication use, independent of treatment setting, was associated with a substantial reduction in overdose risk.
Receiving medication (primarily methadone or buprenorphine), regardless of treatment setting, was associated with a significant reduction in the rate of both fatal and nonfatal opioid overdoses, with around half as many of those receiving medications experiencing an opioid overdose compared to those not receiving medications, or stated differently, a 55% reduction in the risk of opioid overdose independent of treatment setting.
Figure 2. Hazard ratios are essentially used to determine how often something happens in one group compared to another. The way to interpret them is that with 1 as the baseline, anything above 1 indicates more occurrences, while anything below 1 indicates less occurrences. In this instance, only the difference in opioid-related hospitalizations between residential and outpatient treatment in the MOUD condition was statistically significant.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The researchers found that rates of opioid-related outcomes for patients with opioid use disorder receiving residential treatment were no better than patients receiving outpatient treatment. That said, the patients in residential treatments had substantially more severe and complex clinical profiles than those entering outpatient treatment. Thus, having similar outcomes despite greater impairment could be considered a positive. The research team did try to control statistically for a variety of severity indicators in the analyses to try and eradicate this potential confound, but these often cannot capture all of the important nuances that affect outcomes that are associated with such impairment. This is an important limitation in this kind of study design. With this in mind, although medication use was low in both treatment settings, especially residential treatment, use of medications such as buprenorphine or methadone was associated with a 55% reduction in the risk of opioid overdose. As alluded to above, there are obvious self-selection biases operating here that could confound this relationship (i.e., patients most motivated for treatment and overdose prevention might be those using the medication). This large risk reduction is consistent with other large randomized clinical samples, where studies consistently show opioid agonist medications reduce overdose risk by approximately 50%.
The study findings suggest that when targeting crucial outcomes of overdose and emergency department visits, a treatment model that combines outpatient treatment and medication like buprenorphine or methadone may be a better option for most individuals with opioid use disorder rather than more intensive and expensive treatment in a residential setting. This treatment model has been found to be superior to inpatient detox only, residential treatment without medications, or outpatient behavioral health counseling without medications. However, residential treatment facilities should not be ruled out for patients with more severe profiles, such as injection drug use, certain comorbidities (e.g., having other additional severe substance use disorders), and some unique challenges like unstable housing, so long as medications are made available in these settings. In addition, many people with opioid use disorder are not interested in medication treatment, so we need to understand what treatment alternatives are most helpful for these patients.
Most of the outcomes examined were similar in both treatment settings, which has also been shown for individuals with substance use disorder more generally. However, this study did find that among individuals receiving medications, outpatient treatment was associated with less opioid-related hospital use compared to patients treated in a residential setting, and also that, overall, all-cause hospital use was lower in individuals receiving treatment in outpatient settings compared with residential. These findings suggest that there was actually some benefit to outpatient treatment compared to residential treatment for people with opioid use disorder and is similar to findings among commercial beneficiaries nationally. However, as noted earlier, this finding should be interpreted with caution as it may have been due to greater severity in the residential treatment group that was unable to be accounted for adequately in the analysis. More research is needed on identifying subsets of patients that may benefit from residential treatment and how these findings might translate to more recent years in the context of fentanyl inundating the illicit opioid supply.
In this study, treatment in outpatient and residential settings was examined, but this study did not assess the types of services received during these treatment episodes nor did it capture opioid use disorder treatment that may be delivered outside of these settings. Other studies point to ways to improve medication’s benefits, including contingency management and participation in mutual help organizations. Also, recent research has suggested that a “medication first” approach where patients are offered medications with no expectation for them to participate in other treatment services can produce similar outcomes to treatment as usual (e.g., medication plus required counseling). As an example, an individual might receive treatment with buprenorphine at a private doctor’s office with only medication management. However, this approach may not be ideal for more severe and complicated patients.
Only 36% of patients with opioid use disorder who received treatment in residential or outpatient settings received medications, with this rate much higher in outpatient treatment settings compared with residential treatment settings. However, a limitation of this study is that all we know is that the patient was dispensed the medication from a pharmacy, which would appear as an insurance claim, but we do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed). More research is needed into the myriad ways to increase medication uptake beyond availability. Although future studies should identify patients who are most likely to benefit from residential treatment, a more effective strategy that may represent low-hanging fruit for many residential treatment facilities is to ensure that medication is delivered in conjunction with other treatment services. Other research has shown that medications can augment residential treatment. In addition, although higher than residential treatment, medication use in outpatient settings was low and represents a missed opportunity to initiate an evidence-based treatment.
The way that medication use for opioid use disorder was measured in this study, we only know that a patient was dispensed the medication from a pharmacy, which would be captured as an insurance claim, but do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed).
Treatment retention was measured as engagement in all treatment across any treatment setting, including provision of medication. Since many individuals stay on medications long-term, this could have biased the comparison of treatment retention between patients on medications and not on medications.
Although the researchers used several different clinical characteristics to capture the substance use profile of the patients, there was no direct measure for severity of opioid use disorder (e.g., mild, moderate, or severe).
This was a naturalistic observational study and although the research team tried to control for the substantial severity differences between patients treated in residential and outpatient settings findings are still very likely to be affected by selection bias and confounding.
The outcome of interest, both fatal and nonfatal opioid overdoses, is likely undercounted because many people who experience a nonfatal opioid overdose do not seek medical attention. In addition, the outcome of interest was rare (n=56) limiting the statistical power of the study.
This study was not able to capture other services that individuals may have used to improve their well-being, such as recovery community centers or mutual help organizations. Nor did the study examine other settings where medications might be delivered, such as a private doctor’s office.
This study was done on Medicaid beneficiaries in one state (Oregon). Generalizing results to individuals with other types of insurance (e.g., commercial, Medicare), to other states, or nationally should be done with caution.
The study sample was limited to around half of Medicaid beneficiaries who were treated for opioid use disorder in residential or outpatient treatment settings and also had an admissions record in the Treatment Episode Data Set. This would introduce bias if people included in the study sample were very different from people who were not included in the study sample.
BOTTOM LINE
Rates of opioid-related outcomes for patients with opioid use disorder receiving residential treatment were found to be similar to patients receiving outpatient treatment. Given the big differences in clinical severity and complexity indicators among the two types of patient groups, this might be seen as a positive outcome experience for those more severe patients that were treated in residential settings. An alternative explanation is that these similar outcomes may be explained by greater use of opioid use disorder medications in outpatient settings, which helped to compensate, or overcome, the less intensive and structured treatment that is present in residential settings. Although medication use was low in both treatment settings, especially residential treatment, and this study was not randomized or otherwise able to be well controlled from a statistical standpoint, consistent with other large clinical samples, use of medications such as buprenorphine or methadone was associated with a 55% reduction in the risk of opioid overdose in the current study – a figure consistent with more well controlled and randomized investigations.
For individuals and families seeking recovery: Study findings showed that, on average, treatment received for opioid use disorder in a residential setting was similar to treatment received in an outpatient setting. Whereas this might be considered a positive outcome for the much more severe residential patients, another possible explanation is that the equally positive outcomes for those receiving the less expensive and less structured outpatient treatment was due to medication use. Although some people with severe opioid use disorder along with other comorbidities and social determinants of health barriers (e.g., unstable housing, unemployed) may still benefit from residential treatment, outpatient treatment combined with medication use may be the best and most inexpensive treatment model to reduce overdose risk and healthcare costs for many people with opioid use disorder.
For treatment professionals and treatment systems: Healthcare systems might consider focusing on expanding outpatient treatment for opioid use disorder where medications can also be initiated and continued, while also ensuring that medications are available in existing residential treatment facilities. Treatment professionals might consider recommending residential treatment for opioid use disorder along with medication use, especially for patients without severe substance use profiles, such as injection drug use, certain comorbidities (e.g., co-occurring substance use disorders, and/or mental health conditions), and some unique challenges (e.g., unstable housing).
For scientists: This study used a survival analysis to examine the association between opioid-related outcomes and treatment setting, an interaction term to explore how medication use modified this association, and multivariable logistic regression to examine the association between treatment retention and treatment setting. More research is needed to see if this finding would be replicated in states apart from Oregon, given the unique state-level characteristics of Medicaid programs across states as well as the geographic variation of the presence of fentanyl in the illicit opioid supply. Also, there are significant confounds and challenges with the study design in being able to assert with confidence which types of patients would be best served in which type of setting. That said, opioid use disorder medications were associated with reduced overdose and the effect was similar in magnitude with prior experimental and well controlled research designs. More research is needed to identify characteristics of patients who would benefit most from residential treatment, as well as how best to help the many patients who are medication-reluctant.
For policy makers: Policies and interventions that increase medication use in both outpatient and residential treatment settings are likely to be most impactful for people with opioid use disorder. Importantly, this would include expanding availability of medications in these treatment settings but also might include increasing clinical and patient buy-in for medication use. Although more research is needed, some people, especially those with severe clinical characteristics and challenges such as homelessness, are likely to be better fits for residential treatment so long as medications are also made available to prioritize reduce overdose risk. Policymakers may be able to use funding mechanisms, such as making the receipt of federal or state grant money contingent on providing evidence-based treatments, to increase the use of medications for opioid use disorder in all treatment settings.
Despite medications being the gold standard treatment for opioid use disorder, it is estimated that 87% of individuals who may benefit from medication treatment do not receive it — either because they do not have access or choose not to take it if they do have access. Several approaches may be needed to address this treatment gap. For example, treatment for opioid use disorder may be initiated and delivered in different healthcare settings, including outpatient and residential settings. Although treatment in outpatient settings has been increasing, many individuals, especially those with more severe and often complex profiles, are still treated in residential settings. These settings can offer greater protection against any use while in this more controlled environment, while also providing more structured treatment content (e.g., groups, sessions, etc.) in a shorter period of time. However, less than one third of residential treatment settings offer FDA-approved medication for opioid use disorder. Initiating medication treatment for opioid use disorder in outpatient settings may be superior to other treatment settings, possibly due to a more conducive clinical culture and treatment infrastructure focused on medication use. In this study, researchers examined the association between treatment setting and opioid-related outcomes among Oregon Medicaid beneficiaries with opioid use disorder. Results could potentially provide insight into the most important types of treatment models to scale up to adequately address the large treatment gap among people with opioid use disorder in the United States.
HOW WAS THIS STUDY CONDUCTED?
This was a retrospective cohort study that linked several databases together to examine if opioid-related outcomes differed for Oregon Medicaid beneficiaries who received outpatient or residential treatment. The researchers were also interested in how medications may have influenced the relationship between treatment setting and opioid-related outcomes.
The researchers linked several databases to provide rich data on Oregon Medicaid beneficiaries with opioid use disorder who received treatment from July 2014 to June 2017 as part of the National Drug Abuse Treatment Clinical Trials Network “In and Out Study”, including Medicaid claims data, the Treatment Episode Data Set, and death certificate data from Oregon. The researchers used Medicaid claims data to identify opioid use disorder diagnoses, treatment for this disorder in either an outpatient or residential setting, if a medication prescription was filled during the treatment episode, a range of physical and mental comorbidities that may impact treatment setting and/or outcomes (which were combined to create a composite score known as the Elixhauser Comorbidity Index), and all opioid-related outcomes except for opioid overdose fatalities. The researchers used admission data from the Treatment Episode Data Set to ascertain more detailed information about the patient’s opioid use disorder, such as opioid type, other substances used, frequency and history of opioid use, and injection drug use. The researchers used death certificate data to identify opioid overdose fatalities.
The variable of interest in this study was whether someone received either residential or outpatient treatment for opioid use disorder. The primary outcome of interest was opioid overdose – both fatal and non-fatal. Secondary outcomes of interest included non-overdose opioid-related emergency department visits and hospitalizations as well as any emergency department visits and hospitalization. They also examined treatment retention in a sub-group of patients who received Medicaid for at least 1 year defined as the period of time over which they had insurance claims for any type of substance use disorder treatment, including psychosocial services or medication.
Medicaid beneficiaries were included in the study sample if they had at least 180 days of Medicaid enrollment before their index treatment date (defined as their first treatment encounter if there were more than one treatment episodes during the study period), if they had a diagnosis of opioid use disorder, and if they had a Medicaid claim for a residential treatment stay or an outpatient treatment encounter. Patients were excluded from the sample if they did not have an appropriate admission record in the Treatment Episode Data Set that indicated opioids as a problem substance, and this admission had to occur after 2014 and up to 7 days following the index treatment date.
The study protocol identified 3,293 Medicaid beneficiaries in Oregon who met the study criteria, with 2,336 individuals receiving residential treatment and 957 individuals receiving outpatient treatment for opioid use disorder. Compared to those in outpatient treatment, individuals receiving residential treatment tended to be younger and had clinical characteristics indicative of more complicated cases of opioid use disorder, such as higher rates of depression, higher rates of heroin and stimulant use, and higher rates of injection drug use. Also, rates of prior inpatient medically supervised withdrawal were sixfold higher for individuals receiving treatment in residential settings compared with outpatient settings. For the secondary outcome of treatment retention, only those individuals who were enrolled in Medicaid a full year after the index treatment date were analyzed, limiting the sample to 1,913 individuals.
The research team examined the association between treatment setting and opioid-related outcomes, controlling for baseline demographics (age, race, sex), Elixhauser comorbidity score, opioid use disorder and other substance use characteristics from the Treatment Episode Data Set (e.g., injection drug use), medication use, and medically managed withdrawal immediately preceding the treatment episode. The models also controlled for all-cause and opioid-related emergency department visits and hospitalizations in the 180 days prior to the index treatment date as additional measures to capture potential clinical differences between individuals in each treatment setting.
Since previous research has identified medication as a vital component of opioid use disorder, the researchers stratified their analysis by whether or not medication was used, and also used an interaction term in the models to examine if medication use modified the relationship between treatment setting and each opioid-related outcome. In this study, medication use was measured as an insurance claim for one of the three FDA-approved medications for opioid use disorder including methadone, buprenorphine, and extended-release naltrexone. Therefore, we do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed).
WHAT DID THIS STUDY FIND?
Opioid-related patient outcomes were similar in outpatient and residential treatment.
The outcome of interest, the rate of both fatal and nonfatal opioid overdoses, was not different between individuals receiving opioid use disorder treatment in residential settings and those receiving treatment in outpatient settings. There was also not a difference in opioid-related emergency department visits and hospitalizations between the two treatment settings. However, the interaction with medication use was significant, suggesting that among individuals receiving medications, patients receiving residential treatment had a higher risk of an opioid-related emergency department visit and hospitalization compared to patients receiving outpatient treatment, although severity of opioid use disorder was not directly controlled for. Also, the rate of all-cause emergency department visits and hospitalizations was higher in residential settings compared with outpatient settings.
Treatment retention was higher in residential settings at 6 months, but not 12 months.
However, the results suggest that the benefits of residential treatment on treatment retention, measured as engagement in all treatment across any treatment setting including provision of medications, were limited to individuals who were not receiving medications such that that those who did not receive medication in residential settings had longer periods of treatment retention, on average, than those who did receive medication.
Medication use was low overall, but higher in outpatient settings.
Only 36% of individuals receiving residential or outpatient treatment for opioid use disorder received medications, with this rate higher in outpatient settings (43%) than residential settings (19%). The most commonly used medication was buprenorphine, followed by methadone, with use of extended-release naltrexone very rare. Although the rate of methadone use was similar across treatment settings, the rate of buprenorphine use was 32% in outpatient settings and 9% in residential settings.
Medication use, independent of treatment setting, was associated with a substantial reduction in overdose risk.
Receiving medication (primarily methadone or buprenorphine), regardless of treatment setting, was associated with a significant reduction in the rate of both fatal and nonfatal opioid overdoses, with around half as many of those receiving medications experiencing an opioid overdose compared to those not receiving medications, or stated differently, a 55% reduction in the risk of opioid overdose independent of treatment setting.
Figure 2. Hazard ratios are essentially used to determine how often something happens in one group compared to another. The way to interpret them is that with 1 as the baseline, anything above 1 indicates more occurrences, while anything below 1 indicates less occurrences. In this instance, only the difference in opioid-related hospitalizations between residential and outpatient treatment in the MOUD condition was statistically significant.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The researchers found that rates of opioid-related outcomes for patients with opioid use disorder receiving residential treatment were no better than patients receiving outpatient treatment. That said, the patients in residential treatments had substantially more severe and complex clinical profiles than those entering outpatient treatment. Thus, having similar outcomes despite greater impairment could be considered a positive. The research team did try to control statistically for a variety of severity indicators in the analyses to try and eradicate this potential confound, but these often cannot capture all of the important nuances that affect outcomes that are associated with such impairment. This is an important limitation in this kind of study design. With this in mind, although medication use was low in both treatment settings, especially residential treatment, use of medications such as buprenorphine or methadone was associated with a 55% reduction in the risk of opioid overdose. As alluded to above, there are obvious self-selection biases operating here that could confound this relationship (i.e., patients most motivated for treatment and overdose prevention might be those using the medication). This large risk reduction is consistent with other large randomized clinical samples, where studies consistently show opioid agonist medications reduce overdose risk by approximately 50%.
The study findings suggest that when targeting crucial outcomes of overdose and emergency department visits, a treatment model that combines outpatient treatment and medication like buprenorphine or methadone may be a better option for most individuals with opioid use disorder rather than more intensive and expensive treatment in a residential setting. This treatment model has been found to be superior to inpatient detox only, residential treatment without medications, or outpatient behavioral health counseling without medications. However, residential treatment facilities should not be ruled out for patients with more severe profiles, such as injection drug use, certain comorbidities (e.g., having other additional severe substance use disorders), and some unique challenges like unstable housing, so long as medications are made available in these settings. In addition, many people with opioid use disorder are not interested in medication treatment, so we need to understand what treatment alternatives are most helpful for these patients.
Most of the outcomes examined were similar in both treatment settings, which has also been shown for individuals with substance use disorder more generally. However, this study did find that among individuals receiving medications, outpatient treatment was associated with less opioid-related hospital use compared to patients treated in a residential setting, and also that, overall, all-cause hospital use was lower in individuals receiving treatment in outpatient settings compared with residential. These findings suggest that there was actually some benefit to outpatient treatment compared to residential treatment for people with opioid use disorder and is similar to findings among commercial beneficiaries nationally. However, as noted earlier, this finding should be interpreted with caution as it may have been due to greater severity in the residential treatment group that was unable to be accounted for adequately in the analysis. More research is needed on identifying subsets of patients that may benefit from residential treatment and how these findings might translate to more recent years in the context of fentanyl inundating the illicit opioid supply.
In this study, treatment in outpatient and residential settings was examined, but this study did not assess the types of services received during these treatment episodes nor did it capture opioid use disorder treatment that may be delivered outside of these settings. Other studies point to ways to improve medication’s benefits, including contingency management and participation in mutual help organizations. Also, recent research has suggested that a “medication first” approach where patients are offered medications with no expectation for them to participate in other treatment services can produce similar outcomes to treatment as usual (e.g., medication plus required counseling). As an example, an individual might receive treatment with buprenorphine at a private doctor’s office with only medication management. However, this approach may not be ideal for more severe and complicated patients.
Only 36% of patients with opioid use disorder who received treatment in residential or outpatient settings received medications, with this rate much higher in outpatient treatment settings compared with residential treatment settings. However, a limitation of this study is that all we know is that the patient was dispensed the medication from a pharmacy, which would appear as an insurance claim, but we do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed). More research is needed into the myriad ways to increase medication uptake beyond availability. Although future studies should identify patients who are most likely to benefit from residential treatment, a more effective strategy that may represent low-hanging fruit for many residential treatment facilities is to ensure that medication is delivered in conjunction with other treatment services. Other research has shown that medications can augment residential treatment. In addition, although higher than residential treatment, medication use in outpatient settings was low and represents a missed opportunity to initiate an evidence-based treatment.
The way that medication use for opioid use disorder was measured in this study, we only know that a patient was dispensed the medication from a pharmacy, which would be captured as an insurance claim, but do not know if medication was offered in the treatment setting but the patient was not interested, if the patient was prescribed the medication but did not get it filled at a pharmacy, or if the patient got the medication filled at a pharmacy but was not compliant on the medication (i.e., taking the medication as prescribed).
Treatment retention was measured as engagement in all treatment across any treatment setting, including provision of medication. Since many individuals stay on medications long-term, this could have biased the comparison of treatment retention between patients on medications and not on medications.
Although the researchers used several different clinical characteristics to capture the substance use profile of the patients, there was no direct measure for severity of opioid use disorder (e.g., mild, moderate, or severe).
This was a naturalistic observational study and although the research team tried to control for the substantial severity differences between patients treated in residential and outpatient settings findings are still very likely to be affected by selection bias and confounding.
The outcome of interest, both fatal and nonfatal opioid overdoses, is likely undercounted because many people who experience a nonfatal opioid overdose do not seek medical attention. In addition, the outcome of interest was rare (n=56) limiting the statistical power of the study.
This study was not able to capture other services that individuals may have used to improve their well-being, such as recovery community centers or mutual help organizations. Nor did the study examine other settings where medications might be delivered, such as a private doctor’s office.
This study was done on Medicaid beneficiaries in one state (Oregon). Generalizing results to individuals with other types of insurance (e.g., commercial, Medicare), to other states, or nationally should be done with caution.
The study sample was limited to around half of Medicaid beneficiaries who were treated for opioid use disorder in residential or outpatient treatment settings and also had an admissions record in the Treatment Episode Data Set. This would introduce bias if people included in the study sample were very different from people who were not included in the study sample.
BOTTOM LINE
Rates of opioid-related outcomes for patients with opioid use disorder receiving residential treatment were found to be similar to patients receiving outpatient treatment. Given the big differences in clinical severity and complexity indicators among the two types of patient groups, this might be seen as a positive outcome experience for those more severe patients that were treated in residential settings. An alternative explanation is that these similar outcomes may be explained by greater use of opioid use disorder medications in outpatient settings, which helped to compensate, or overcome, the less intensive and structured treatment that is present in residential settings. Although medication use was low in both treatment settings, especially residential treatment, and this study was not randomized or otherwise able to be well controlled from a statistical standpoint, consistent with other large clinical samples, use of medications such as buprenorphine or methadone was associated with a 55% reduction in the risk of opioid overdose in the current study – a figure consistent with more well controlled and randomized investigations.
For individuals and families seeking recovery: Study findings showed that, on average, treatment received for opioid use disorder in a residential setting was similar to treatment received in an outpatient setting. Whereas this might be considered a positive outcome for the much more severe residential patients, another possible explanation is that the equally positive outcomes for those receiving the less expensive and less structured outpatient treatment was due to medication use. Although some people with severe opioid use disorder along with other comorbidities and social determinants of health barriers (e.g., unstable housing, unemployed) may still benefit from residential treatment, outpatient treatment combined with medication use may be the best and most inexpensive treatment model to reduce overdose risk and healthcare costs for many people with opioid use disorder.
For treatment professionals and treatment systems: Healthcare systems might consider focusing on expanding outpatient treatment for opioid use disorder where medications can also be initiated and continued, while also ensuring that medications are available in existing residential treatment facilities. Treatment professionals might consider recommending residential treatment for opioid use disorder along with medication use, especially for patients without severe substance use profiles, such as injection drug use, certain comorbidities (e.g., co-occurring substance use disorders, and/or mental health conditions), and some unique challenges (e.g., unstable housing).
For scientists: This study used a survival analysis to examine the association between opioid-related outcomes and treatment setting, an interaction term to explore how medication use modified this association, and multivariable logistic regression to examine the association between treatment retention and treatment setting. More research is needed to see if this finding would be replicated in states apart from Oregon, given the unique state-level characteristics of Medicaid programs across states as well as the geographic variation of the presence of fentanyl in the illicit opioid supply. Also, there are significant confounds and challenges with the study design in being able to assert with confidence which types of patients would be best served in which type of setting. That said, opioid use disorder medications were associated with reduced overdose and the effect was similar in magnitude with prior experimental and well controlled research designs. More research is needed to identify characteristics of patients who would benefit most from residential treatment, as well as how best to help the many patients who are medication-reluctant.
For policy makers: Policies and interventions that increase medication use in both outpatient and residential treatment settings are likely to be most impactful for people with opioid use disorder. Importantly, this would include expanding availability of medications in these treatment settings but also might include increasing clinical and patient buy-in for medication use. Although more research is needed, some people, especially those with severe clinical characteristics and challenges such as homelessness, are likely to be better fits for residential treatment so long as medications are also made available to prioritize reduce overdose risk. Policymakers may be able to use funding mechanisms, such as making the receipt of federal or state grant money contingent on providing evidence-based treatments, to increase the use of medications for opioid use disorder in all treatment settings.