
Extended Release Naltrexone Prevents Opioid Relapse in Criminal Justice Offenders
As many evidence-based options as possible are needed in order to address the sharp increase in opioid misuse and opioid overdose deaths seen in the U.S. in the past 10 years. Some groups are at proportionately greater risk to use opioids and to experience their potential negative impact – individuals in the criminal justice system are one such group.
Can a medication administered just once per month reduce risk for opioid use disorder relapse?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
Researchers, clinicians, and policy makers are working hard to find ways to address the increasing rates of opioid use disorder and opioid overdose in the United States. Those in the criminal justice system, and in particular individuals recently released from jail/prison, have been disproportionately affected. Medication-assisted treatments, including the opioid agonists buprenorphine (often packaged in a combined formulation with naloxone, as “Suboxone”) and methadone, have been shown to be effective in helping reduce this relapse risk (Opioid agonists mimic more powerful, reinforcing opioids like heroin by stimulating opioid receptors to a sufficient, but lesser degree, thereby reducing craving and overdose risk)
There are some drawbacks to agonist treatments, including the need to be taken daily, risk for negative cardiovascular outcomes when combined with other substances that slow down the central nervous system (e.g., alcohol or commonly prescribed anxiety medications called benzodiazepenes), and the potential to misuse it.
As such, it is important to conduct research on opioid antagonist treatments (i.e., opioid receptor “blockers”), which may be slightly less effective in reducing craving, but without carrying the risks of opioid agonists.
The most popular opioid antagonist, naltrexone, is available in a once-a-month, extended release injection (administered by a medical professional), under the brand name “Vivitrol”, which was approved by the Food and Drug Administration (FDA) in October 2010.
To help determine whether this naltrexone formulation is effective for individuals involved in the criminal justice system, the authors first conducted a pilot study. This important and timely study built on those results by conducted a randomized controlled trial with over 300 justice system involved individuals who were living in the community and who also preferred an “opioid-free” medication-assisted treatment, as study authors referred to it.
HOW WAS THIS STUDY CONDUCTED?
This randomized controlled trial compared extended release naltrexone to treatment-as-usual for individuals with opioid use disorder who were involved in the criminal justice system. This involvement included but was not limited to being on probation (36% in the naltrexone group and 40% in the treatment-as-usual group) and parole (37% vs. 35%).
All individuals had current or lifetime opioid dependence (based on the diagnostic and statistical manual of mental disorders, 5th edition) and were abstinent from opioids before being randomized. On average, participants were 44 years old, 85% male, and 77% Black or Hispanic. Upon entering the study, 65% had not used opioids in the past 30 days while 41% reported lifetime injection drug use, and 9% required opioid detoxification to achieve abstinence. The randomization process balanced groups on the site at which they received treatment, gender, and whether or not they needed opioid detoxification at the start of the study.
Individuals in the naltrexone group received 380mg injection every 4 weeks, consistent with standard clinical practice. Regarding adherence, 77% of all injections in naltrexone participants were completed as scheduled.
The psychosocial treatment component included support for agonist treatment in both groups upon conclusion of the initial 6-month active study period.
WHAT DID THIS STUDY FIND?
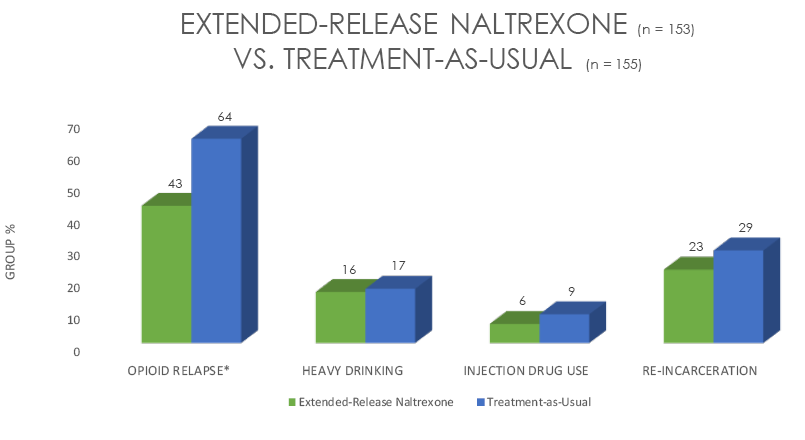
Lee and colleagues found that individuals randomized to receive extended release naltrexone (known by its brand name “Vivitrol”) for 6 months had:
- better opioid outcomes compared to treatment as usual during this time
- lower overall relapse rates while taking the medication (43% to 64%) (Relapse defined as 10 or more days of opioid use in 1 month by self-report, or by a positive opioid toxicology screen)
- greater percentage of opioid-negative urine toxicology screens & of 2-week periods of abstinence
- among the 153 individuals in the naltrexone group, who also received relapse prevention counseling and encouragement to seek treatment in the community, they had longer time to relapse, on average, compared to the 155 who received similar psychosocial treatment but no medication (i.e., treatment-as-usual; 11 vs. 5 weeks)
- similar outcomes to the treatment as usual group for non-opioid outcomes including cocaine use, heavy drinking, injection use, or reincarceration
- had zero overdoses across the entire study – including the time after the medication was discontinued – while there were seven overdoses among treatment-as-usual patients, three of which were fatal
1/3 of those in treatment-as-usual sought agonist treatment during the study (e.g., “suboxone”) compared to just 10% of those in the naltrexone group.
WHY IS THIS STUDY IMPORTANT
For individuals living in the community but involved in the criminal justice system who received a once-per-month injection of extended-release naltrexone, their relapse risk was half as great as those in treatment-as-usual.
However, this advantage disappeared after the medication was discontinued. As authors mention, one reason for this may have been the lack of available extended release naltrexone in the community at the time of the study – it was approved by the FDA while the study was in progress. Zero individuals in the naltrexone group received extended release naltrexone after they stopped receiving it as part of the study. Naltrexone is most effective in reducing risk for relapse when taken continuously.
The results of this study, indicated that naltexone did not decrease heavy drinking in this sample, somewhat surprising as naltrexone was originally developed, and is often prescribed for alcohol use disorder.
- LIMITATIONS
-
- There was no placebo medication given to individuals in the comparison group. Therefore, while they received relapse prevention and encouragement to seek formal treatment in the community, whether naltrexone is helpful over and above the expectation that the medication works (e.g., placebo effect) in this sample is unclear. That said, placebo-controlled studies of extended release naltrexone have shown an advantage for the medication.
NEXT STEPS
As authors point out, long term studies (i.e., beyond 6 months) on the effects of medication-assisted treatment with extended release naltrexone are needed. Recent RRI research reviews have highlighted the benefits of buprenorphine and methadone across multiple years .
Also, while these criminal justice involved individuals were living in the community, researchers have pointed out there are many barriers to implementing medication-assisted treatment for opioid use disorder in jails and prisons. Some of these barriers are related to philosophy and stigma attached to medication assisted treatment (to agonist treatments in particular), some to these systems having medical personnel that are not well trained in addiction treatment, and still others are related to lack of a centralized health care system in the United States that might otherwise carry over to justice system involved individuals.
Future work should focus on the challenges and solutions to medication assisted treatment implementation in this population both before and after their release.
BOTTOM LINE
- For individuals & families seeking recovery: Extended release naltrexone in injection form is likely to help cut your chances of opioid use disorder relapse in half. This study focused on individuals in the criminal justice system (e.g., on probation), though these types of beneficial effects could apply to other individuals with opioid use disorder as well.
- For Scientists: This rigorous study showed extended release naltrexone reduces relapse risk for individuals with opioid use disorder. Few studies have compared the various forms of medication-assisted treatment, including agonists like buprenorphine versus this extended release naltrexone. However, comparisons of the effects and safety profiles of these medications are underway.
- For Policy makers: This rigorous study showed extended release naltrexone reduces relapse risk by two-fold for individuals with opioid use disorder involved in the criminal justice system. In combination with studies showing extended release naltrexone is more effective at reducing relapse risk than placebo, this study suggests this medication is an effective tool against opioid use disorder for this at-risk group. Importantly it may help also reduce the risk of fatal overdose post discontinuation. To prevent fatality and enhance outcomes, greater coverage of this medication by health insurance programs is warranted.
- For Treatment professionals and treatment systems: Extended release naltrexone is likely to help reduce relapse risk in your patients with opioid use disorder. Treatment strategies to help improve adherence or build on this effect with psychosocial approaches are not yet clear given the current research.
CITATIONS
Lee, J. D., Friedmann, P. D., Kinlock, T. W., Nunes, E. V., Boney, T. Y., Hoskinson Jr, R. A., … & Gordon, M. (2016). Extended-release naltrexone to prevent opioid relapse in criminal justice offenders. New England Journal of Medicine, 374(13), 1232-1242.
