Does brain structure predict early substance use initiation?
Adolescence marks a critical window in brain development when neural systems governing reward and self-control are rapidly maturing. Understanding why some youth initiate substance use while others don’t has long been a focus in developmental neuroscience. In this study, researchers explored how subtle variations in brain structure may precede and predict early substance use initiation.
Researchers have long sought brain-based markers that might signal risk for later development of substance use disorder. These markers include factors like the thickness or volume of specific brain regions or broader measures such as total brain volume. Some previous investigations have linked such structural characteristics to later substance involvement. For instance, studies have found that children with thinner dorsolateral prefrontal cortices—a region critical for executive function and emotional regulation—are more likely to develop alcohol-related problems. However, these findings have often failed to replicate, largely because neuroimaging studies are typically costly and small, limiting their ability to detect effects and reproducibility.
The study summarized here drew on this rich ABCD dataset to examine how variations in brain structure may relate to the initiation of substance use during adolescence.
HOW WAS THIS STUDY CONDUCTED?
This was a study of 9,804 children ages 9 to 11 at the start of the study (born 2005-2009) recruited from 22 United States research sites, who were assessed every 6 months for 3 years, on any (yes/no) alcohol, cannabis, nicotine, or substance use more generally, including these and other substances. Participants’ brains were scanned using magnetic resonance imaging (MRI) at baseline, and substance use initiation and other psychosocial individual characteristics were assessed at each subsequent follow-up. Analyses controlled for prenatal exposure to alcohol and other drug, familial relationships (e.g., twins and siblings), and MRI scanner differences across sites, but not demographic factors.
The sample average age was 9.9 years at baseline, of whom 53% were boys. The sample was about three quarters White. By age 15, about 35% reported some form of alcohol or other drug use.
WHAT DID THIS STUDY FIND?
Children who initiated substance use showed subtle but identifiable brain differences
Compared with peers with no substance use, children who reported trying any substance before age 15 had larger overall brain volumes as well as greater cortical surface area (see graphic below). At the same time, they showed a thinner prefrontal cortex, particularly in the right rostral middle frontal gyrus, a region crucial for decision-making, planning, and impulse control.
The direction of associations varied by brain region
The direction of associations between observed brain differences and initiation of substance use varied by structure. In children who’d initiated substance use, the prefrontal regions (e.g., dorsolateral prefrontal cortex, superior frontal gyrus) were thinner. Conversely, the occipital, temporal, and parietal regions were thicker, suggesting imbalanced cortical development that might influence how youth process social and sensory cues. Subcortical areas such as the globus pallidus and hippocampus, which are involved in motivation, reward, and memory, were larger in initiators. Taken together, these patterns may suggest a form of neurobiological vulnerability for early substance experimentation marked by reduced inhibitory/regulatory control but heightened reward sensitivity.
These brain differences existed before substance use began
A critical strength of this study was its ability to separate features that predate (i.e., predispose) substance use from possible neurotoxic effects in the brain from alcohol and other drug use. When the researchers restricted analyses to children who had not yet used any substances at baseline (23% of participants had already initiated substance use before their baseline brain scans), the same associations, like a thinner prefrontal cortex and larger global brain volume, still predicted future initiation. This indicates that many of these brain differences were present prior to first use, making them more likely to be preexisting risk markers versus consequences of early alcohol or other drug use.
Substance-specific patterns were modest but distinct
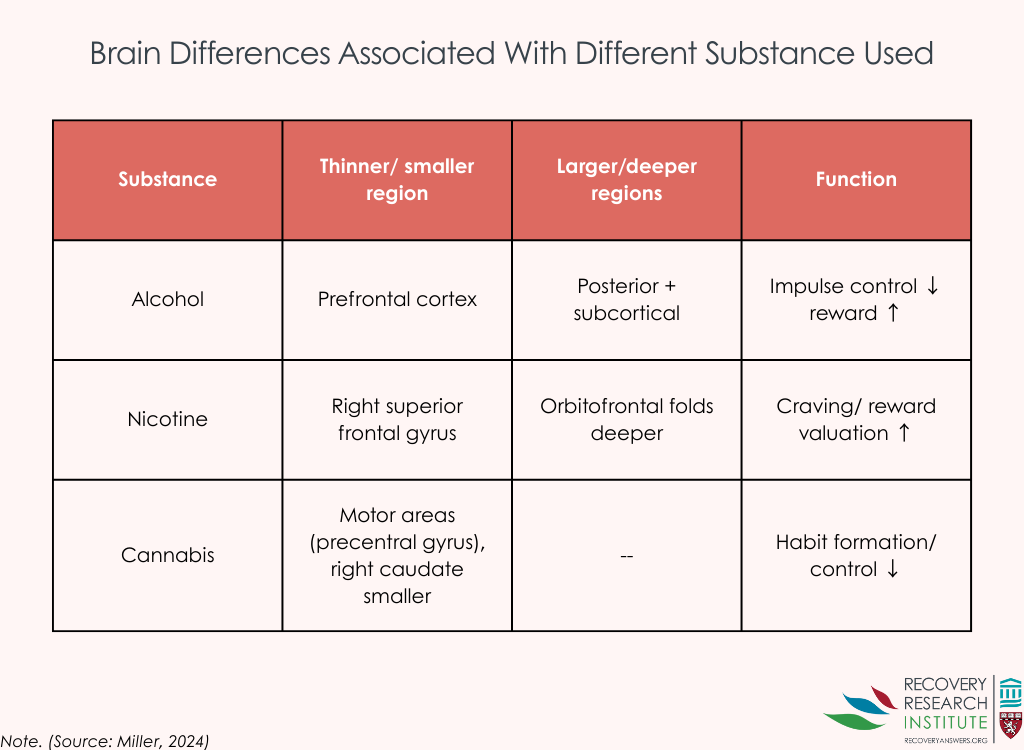
While the overall profile was consistent across substances, some nuanced differences emerged (see graphic below). Alcohol initiation, the most common form of substance use, largely mirrored the general pattern of thinner prefrontal but larger posterior and subcortical regions. Nicotine initiation was associated with smaller right superior frontal gyrus volume and deeper folds in the orbitofrontal cortex, areas involved in craving and valuation of rewards. Cannabis initiation was associated with thinner motor-control areas (precentral gyrus) and smaller right caudate volume, a structure central to habit formation and reward learning. Although these effects were small, they hint at the possibility that differences in brain structure may confer risk for different substances.
Findings held even after accounting for prenatal substance exposure and family factors
Importantly, the associations detected by the researchers remained when analyses controlled for prenatal exposure to alcohol and other drug, familial relationships (e.g., twins and siblings), and MRI scanner differences across sites. This strengthens confidence that the observed brain differences were not artefacts of measurement or family background.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Traditionally, differences in brain structure observed in people who use alcohol or drugs have been interpreted as consequences of substance exposure. However, the results of this large, longitudinal study suggest a more complex picture.
In this research, brain differences linked to early substance use were already present before any use began, implying that certain aspects of brain development may predispose some youth to experiment earlier than others. For instance, thinner prefrontal brain regions—which play a central role in impulse control, planning, and emotion regulation—could make it harder for some children to inhibit impulses or delay gratification in social contexts where substances are available. At the same time, larger subcortical structures and overall brain volumes may reflect developmental patterns associated with greater sensation seeking or reward sensitivity.
It is important to note that these patterns do not mean that brain structure is destiny. The effects for the correlations between these brain characteristics and substance use initiation were quite small, suggesting that some, but not all, youth with these profiles went on to use substances. Also, in terms of the utility, these results cannot yet be applied in clinical settings. For example, we do not yet know the threshold for these neurobiological characteristics (e.g., thinner vs. thicker brain regions) that would accurately classify a child as being at risk for substance use initiation and downstream consequences. Rather, they highlight that differences in neurodevelopment might influence vulnerability, which in turn interacts with other biological, psychological, and social factors. Indeed, this study could not determine why these brain characteristics are present – i.e., developed during childhood as a function of life experience (e.g., trauma, stressors, etc.). That said, the findings held even when controlling for familial risk for substance use – suggesting the risk goes beyond genetic predisposition alone. Supportive family environments, positive peer relationships, and opportunities to develop self-regulatory skills may help buffer against these risks.
For prevention science, these findings may underscore the need for earlier, developmentally informed interventions that target self-regulation, stress management, and healthy risk-taking before adolescence. They also hint that brain-based measures, in combination with behavioral and genetic data, could one day help providers identify individuals most in need of early support.
Finally, the study challenges us to rethink how we interpret neuroimaging findings in addiction research. Not all brain differences seen in youth who use alcohol and other drugs are the result of damage; some may reflect preexisting variations in brain maturation that set the stage for how individuals respond to risk, reward, and social influences during adolescence. Recognizing these developmental nuances can help refine both prevention strategies and public messaging around youth substance use.
Because substance involvement is generally just emerging in early adolescence, the researchers’ analyses focused on initiation rather than escalation, problematic use, or substance use disorder, so findings may not generalize to later presentations.
Brain/behavior associations were modest at the individual level, limiting clinical utility for prediction, even though they are informative for theory and population risk.
Too few substance-naïve youth initiated before the next, post-baseline MRI, preventing the researchers from testing longitudinal change models that would help identify neuroanatomical changes following substance use initiation.
To avoid undercutting identification of potential brain structure differences, the researchers deliberately did not control for socio-demographics factors. This could have influenced or moderated the observed associations in unknown ways.
It can’t be known from this cross-sectional analysis of baseline brain anatomy when observed structural differences may have emerged.
BOTTOM LINE
This uniquely large national study of brain imaging suggests that subtle differences in brain structure—particularly in regions responsible for impulse control and planning—may predispose some children to some degree to try substances earlier in life. While the thresholds at which these subtle differences predict initiation are not yet clear, ultimately, recognizing and supporting these youth could reduce the likelihood of later substance-related problems and improve developmental outcomes.
For individuals and families seeking recovery: While this study focused on youth who had not yet developed substance use problems, its findings reinforce the idea that vulnerability often begins early in life. Subtle brain differences linked to decision-making, impulse control, and emotion regulation can shape how a young person responds to risk and reward. Families can help protect against these vulnerabilities by fostering supportive relationships, open communication, and structured routines.
For treatment professionals and treatment systems: These results highlight the importance of early prevention and resilience-building, not only in high-risk populations but broadly among pre-teens and adolescents. Clinicians and program designers could integrate interventions that strengthen executive function, emotion regulation, and decision-making skills. Recognizing that certain neurodevelopmental factors precede substance use underscores the value of neuroscience-informed prevention and early screening in pediatric and school-based settings.
For scientists: The study demonstrates the power of large, longitudinal, open-science datasets like the ABCD Study for identifying neural markers of risk. Its findings lend support to models emphasizing predispositional neurobiological factors rather than only exposure effects. Future work should examine how these structural brain differences interact with genetics, environment, and psychosocial factors across adolescence to predict trajectories from experimentation to substance use disorder, and whether early interventions can modify these pathways.
For policy makers: These findings provide further justification for investing in early prevention and child development programs. Policies that support family stability, school-based prevention initiatives, and access to mental-health services, may mitigate risk for substance use and later substance-related problems.
Researchers have long sought brain-based markers that might signal risk for later development of substance use disorder. These markers include factors like the thickness or volume of specific brain regions or broader measures such as total brain volume. Some previous investigations have linked such structural characteristics to later substance involvement. For instance, studies have found that children with thinner dorsolateral prefrontal cortices—a region critical for executive function and emotional regulation—are more likely to develop alcohol-related problems. However, these findings have often failed to replicate, largely because neuroimaging studies are typically costly and small, limiting their ability to detect effects and reproducibility.
The study summarized here drew on this rich ABCD dataset to examine how variations in brain structure may relate to the initiation of substance use during adolescence.
HOW WAS THIS STUDY CONDUCTED?
This was a study of 9,804 children ages 9 to 11 at the start of the study (born 2005-2009) recruited from 22 United States research sites, who were assessed every 6 months for 3 years, on any (yes/no) alcohol, cannabis, nicotine, or substance use more generally, including these and other substances. Participants’ brains were scanned using magnetic resonance imaging (MRI) at baseline, and substance use initiation and other psychosocial individual characteristics were assessed at each subsequent follow-up. Analyses controlled for prenatal exposure to alcohol and other drug, familial relationships (e.g., twins and siblings), and MRI scanner differences across sites, but not demographic factors.
The sample average age was 9.9 years at baseline, of whom 53% were boys. The sample was about three quarters White. By age 15, about 35% reported some form of alcohol or other drug use.
WHAT DID THIS STUDY FIND?
Children who initiated substance use showed subtle but identifiable brain differences
Compared with peers with no substance use, children who reported trying any substance before age 15 had larger overall brain volumes as well as greater cortical surface area (see graphic below). At the same time, they showed a thinner prefrontal cortex, particularly in the right rostral middle frontal gyrus, a region crucial for decision-making, planning, and impulse control.
The direction of associations varied by brain region
The direction of associations between observed brain differences and initiation of substance use varied by structure. In children who’d initiated substance use, the prefrontal regions (e.g., dorsolateral prefrontal cortex, superior frontal gyrus) were thinner. Conversely, the occipital, temporal, and parietal regions were thicker, suggesting imbalanced cortical development that might influence how youth process social and sensory cues. Subcortical areas such as the globus pallidus and hippocampus, which are involved in motivation, reward, and memory, were larger in initiators. Taken together, these patterns may suggest a form of neurobiological vulnerability for early substance experimentation marked by reduced inhibitory/regulatory control but heightened reward sensitivity.
These brain differences existed before substance use began
A critical strength of this study was its ability to separate features that predate (i.e., predispose) substance use from possible neurotoxic effects in the brain from alcohol and other drug use. When the researchers restricted analyses to children who had not yet used any substances at baseline (23% of participants had already initiated substance use before their baseline brain scans), the same associations, like a thinner prefrontal cortex and larger global brain volume, still predicted future initiation. This indicates that many of these brain differences were present prior to first use, making them more likely to be preexisting risk markers versus consequences of early alcohol or other drug use.
Substance-specific patterns were modest but distinct
While the overall profile was consistent across substances, some nuanced differences emerged (see graphic below). Alcohol initiation, the most common form of substance use, largely mirrored the general pattern of thinner prefrontal but larger posterior and subcortical regions. Nicotine initiation was associated with smaller right superior frontal gyrus volume and deeper folds in the orbitofrontal cortex, areas involved in craving and valuation of rewards. Cannabis initiation was associated with thinner motor-control areas (precentral gyrus) and smaller right caudate volume, a structure central to habit formation and reward learning. Although these effects were small, they hint at the possibility that differences in brain structure may confer risk for different substances.
Findings held even after accounting for prenatal substance exposure and family factors
Importantly, the associations detected by the researchers remained when analyses controlled for prenatal exposure to alcohol and other drug, familial relationships (e.g., twins and siblings), and MRI scanner differences across sites. This strengthens confidence that the observed brain differences were not artefacts of measurement or family background.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Traditionally, differences in brain structure observed in people who use alcohol or drugs have been interpreted as consequences of substance exposure. However, the results of this large, longitudinal study suggest a more complex picture.
In this research, brain differences linked to early substance use were already present before any use began, implying that certain aspects of brain development may predispose some youth to experiment earlier than others. For instance, thinner prefrontal brain regions—which play a central role in impulse control, planning, and emotion regulation—could make it harder for some children to inhibit impulses or delay gratification in social contexts where substances are available. At the same time, larger subcortical structures and overall brain volumes may reflect developmental patterns associated with greater sensation seeking or reward sensitivity.
It is important to note that these patterns do not mean that brain structure is destiny. The effects for the correlations between these brain characteristics and substance use initiation were quite small, suggesting that some, but not all, youth with these profiles went on to use substances. Also, in terms of the utility, these results cannot yet be applied in clinical settings. For example, we do not yet know the threshold for these neurobiological characteristics (e.g., thinner vs. thicker brain regions) that would accurately classify a child as being at risk for substance use initiation and downstream consequences. Rather, they highlight that differences in neurodevelopment might influence vulnerability, which in turn interacts with other biological, psychological, and social factors. Indeed, this study could not determine why these brain characteristics are present – i.e., developed during childhood as a function of life experience (e.g., trauma, stressors, etc.). That said, the findings held even when controlling for familial risk for substance use – suggesting the risk goes beyond genetic predisposition alone. Supportive family environments, positive peer relationships, and opportunities to develop self-regulatory skills may help buffer against these risks.
For prevention science, these findings may underscore the need for earlier, developmentally informed interventions that target self-regulation, stress management, and healthy risk-taking before adolescence. They also hint that brain-based measures, in combination with behavioral and genetic data, could one day help providers identify individuals most in need of early support.
Finally, the study challenges us to rethink how we interpret neuroimaging findings in addiction research. Not all brain differences seen in youth who use alcohol and other drugs are the result of damage; some may reflect preexisting variations in brain maturation that set the stage for how individuals respond to risk, reward, and social influences during adolescence. Recognizing these developmental nuances can help refine both prevention strategies and public messaging around youth substance use.
Because substance involvement is generally just emerging in early adolescence, the researchers’ analyses focused on initiation rather than escalation, problematic use, or substance use disorder, so findings may not generalize to later presentations.
Brain/behavior associations were modest at the individual level, limiting clinical utility for prediction, even though they are informative for theory and population risk.
Too few substance-naïve youth initiated before the next, post-baseline MRI, preventing the researchers from testing longitudinal change models that would help identify neuroanatomical changes following substance use initiation.
To avoid undercutting identification of potential brain structure differences, the researchers deliberately did not control for socio-demographics factors. This could have influenced or moderated the observed associations in unknown ways.
It can’t be known from this cross-sectional analysis of baseline brain anatomy when observed structural differences may have emerged.
BOTTOM LINE
This uniquely large national study of brain imaging suggests that subtle differences in brain structure—particularly in regions responsible for impulse control and planning—may predispose some children to some degree to try substances earlier in life. While the thresholds at which these subtle differences predict initiation are not yet clear, ultimately, recognizing and supporting these youth could reduce the likelihood of later substance-related problems and improve developmental outcomes.
For individuals and families seeking recovery: While this study focused on youth who had not yet developed substance use problems, its findings reinforce the idea that vulnerability often begins early in life. Subtle brain differences linked to decision-making, impulse control, and emotion regulation can shape how a young person responds to risk and reward. Families can help protect against these vulnerabilities by fostering supportive relationships, open communication, and structured routines.
For treatment professionals and treatment systems: These results highlight the importance of early prevention and resilience-building, not only in high-risk populations but broadly among pre-teens and adolescents. Clinicians and program designers could integrate interventions that strengthen executive function, emotion regulation, and decision-making skills. Recognizing that certain neurodevelopmental factors precede substance use underscores the value of neuroscience-informed prevention and early screening in pediatric and school-based settings.
For scientists: The study demonstrates the power of large, longitudinal, open-science datasets like the ABCD Study for identifying neural markers of risk. Its findings lend support to models emphasizing predispositional neurobiological factors rather than only exposure effects. Future work should examine how these structural brain differences interact with genetics, environment, and psychosocial factors across adolescence to predict trajectories from experimentation to substance use disorder, and whether early interventions can modify these pathways.
For policy makers: These findings provide further justification for investing in early prevention and child development programs. Policies that support family stability, school-based prevention initiatives, and access to mental-health services, may mitigate risk for substance use and later substance-related problems.
Researchers have long sought brain-based markers that might signal risk for later development of substance use disorder. These markers include factors like the thickness or volume of specific brain regions or broader measures such as total brain volume. Some previous investigations have linked such structural characteristics to later substance involvement. For instance, studies have found that children with thinner dorsolateral prefrontal cortices—a region critical for executive function and emotional regulation—are more likely to develop alcohol-related problems. However, these findings have often failed to replicate, largely because neuroimaging studies are typically costly and small, limiting their ability to detect effects and reproducibility.
The study summarized here drew on this rich ABCD dataset to examine how variations in brain structure may relate to the initiation of substance use during adolescence.
HOW WAS THIS STUDY CONDUCTED?
This was a study of 9,804 children ages 9 to 11 at the start of the study (born 2005-2009) recruited from 22 United States research sites, who were assessed every 6 months for 3 years, on any (yes/no) alcohol, cannabis, nicotine, or substance use more generally, including these and other substances. Participants’ brains were scanned using magnetic resonance imaging (MRI) at baseline, and substance use initiation and other psychosocial individual characteristics were assessed at each subsequent follow-up. Analyses controlled for prenatal exposure to alcohol and other drug, familial relationships (e.g., twins and siblings), and MRI scanner differences across sites, but not demographic factors.
The sample average age was 9.9 years at baseline, of whom 53% were boys. The sample was about three quarters White. By age 15, about 35% reported some form of alcohol or other drug use.
WHAT DID THIS STUDY FIND?
Children who initiated substance use showed subtle but identifiable brain differences
Compared with peers with no substance use, children who reported trying any substance before age 15 had larger overall brain volumes as well as greater cortical surface area (see graphic below). At the same time, they showed a thinner prefrontal cortex, particularly in the right rostral middle frontal gyrus, a region crucial for decision-making, planning, and impulse control.
The direction of associations varied by brain region
The direction of associations between observed brain differences and initiation of substance use varied by structure. In children who’d initiated substance use, the prefrontal regions (e.g., dorsolateral prefrontal cortex, superior frontal gyrus) were thinner. Conversely, the occipital, temporal, and parietal regions were thicker, suggesting imbalanced cortical development that might influence how youth process social and sensory cues. Subcortical areas such as the globus pallidus and hippocampus, which are involved in motivation, reward, and memory, were larger in initiators. Taken together, these patterns may suggest a form of neurobiological vulnerability for early substance experimentation marked by reduced inhibitory/regulatory control but heightened reward sensitivity.
These brain differences existed before substance use began
A critical strength of this study was its ability to separate features that predate (i.e., predispose) substance use from possible neurotoxic effects in the brain from alcohol and other drug use. When the researchers restricted analyses to children who had not yet used any substances at baseline (23% of participants had already initiated substance use before their baseline brain scans), the same associations, like a thinner prefrontal cortex and larger global brain volume, still predicted future initiation. This indicates that many of these brain differences were present prior to first use, making them more likely to be preexisting risk markers versus consequences of early alcohol or other drug use.
Substance-specific patterns were modest but distinct
While the overall profile was consistent across substances, some nuanced differences emerged (see graphic below). Alcohol initiation, the most common form of substance use, largely mirrored the general pattern of thinner prefrontal but larger posterior and subcortical regions. Nicotine initiation was associated with smaller right superior frontal gyrus volume and deeper folds in the orbitofrontal cortex, areas involved in craving and valuation of rewards. Cannabis initiation was associated with thinner motor-control areas (precentral gyrus) and smaller right caudate volume, a structure central to habit formation and reward learning. Although these effects were small, they hint at the possibility that differences in brain structure may confer risk for different substances.
Findings held even after accounting for prenatal substance exposure and family factors
Importantly, the associations detected by the researchers remained when analyses controlled for prenatal exposure to alcohol and other drug, familial relationships (e.g., twins and siblings), and MRI scanner differences across sites. This strengthens confidence that the observed brain differences were not artefacts of measurement or family background.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Traditionally, differences in brain structure observed in people who use alcohol or drugs have been interpreted as consequences of substance exposure. However, the results of this large, longitudinal study suggest a more complex picture.
In this research, brain differences linked to early substance use were already present before any use began, implying that certain aspects of brain development may predispose some youth to experiment earlier than others. For instance, thinner prefrontal brain regions—which play a central role in impulse control, planning, and emotion regulation—could make it harder for some children to inhibit impulses or delay gratification in social contexts where substances are available. At the same time, larger subcortical structures and overall brain volumes may reflect developmental patterns associated with greater sensation seeking or reward sensitivity.
It is important to note that these patterns do not mean that brain structure is destiny. The effects for the correlations between these brain characteristics and substance use initiation were quite small, suggesting that some, but not all, youth with these profiles went on to use substances. Also, in terms of the utility, these results cannot yet be applied in clinical settings. For example, we do not yet know the threshold for these neurobiological characteristics (e.g., thinner vs. thicker brain regions) that would accurately classify a child as being at risk for substance use initiation and downstream consequences. Rather, they highlight that differences in neurodevelopment might influence vulnerability, which in turn interacts with other biological, psychological, and social factors. Indeed, this study could not determine why these brain characteristics are present – i.e., developed during childhood as a function of life experience (e.g., trauma, stressors, etc.). That said, the findings held even when controlling for familial risk for substance use – suggesting the risk goes beyond genetic predisposition alone. Supportive family environments, positive peer relationships, and opportunities to develop self-regulatory skills may help buffer against these risks.
For prevention science, these findings may underscore the need for earlier, developmentally informed interventions that target self-regulation, stress management, and healthy risk-taking before adolescence. They also hint that brain-based measures, in combination with behavioral and genetic data, could one day help providers identify individuals most in need of early support.
Finally, the study challenges us to rethink how we interpret neuroimaging findings in addiction research. Not all brain differences seen in youth who use alcohol and other drugs are the result of damage; some may reflect preexisting variations in brain maturation that set the stage for how individuals respond to risk, reward, and social influences during adolescence. Recognizing these developmental nuances can help refine both prevention strategies and public messaging around youth substance use.
Because substance involvement is generally just emerging in early adolescence, the researchers’ analyses focused on initiation rather than escalation, problematic use, or substance use disorder, so findings may not generalize to later presentations.
Brain/behavior associations were modest at the individual level, limiting clinical utility for prediction, even though they are informative for theory and population risk.
Too few substance-naïve youth initiated before the next, post-baseline MRI, preventing the researchers from testing longitudinal change models that would help identify neuroanatomical changes following substance use initiation.
To avoid undercutting identification of potential brain structure differences, the researchers deliberately did not control for socio-demographics factors. This could have influenced or moderated the observed associations in unknown ways.
It can’t be known from this cross-sectional analysis of baseline brain anatomy when observed structural differences may have emerged.
BOTTOM LINE
This uniquely large national study of brain imaging suggests that subtle differences in brain structure—particularly in regions responsible for impulse control and planning—may predispose some children to some degree to try substances earlier in life. While the thresholds at which these subtle differences predict initiation are not yet clear, ultimately, recognizing and supporting these youth could reduce the likelihood of later substance-related problems and improve developmental outcomes.
For individuals and families seeking recovery: While this study focused on youth who had not yet developed substance use problems, its findings reinforce the idea that vulnerability often begins early in life. Subtle brain differences linked to decision-making, impulse control, and emotion regulation can shape how a young person responds to risk and reward. Families can help protect against these vulnerabilities by fostering supportive relationships, open communication, and structured routines.
For treatment professionals and treatment systems: These results highlight the importance of early prevention and resilience-building, not only in high-risk populations but broadly among pre-teens and adolescents. Clinicians and program designers could integrate interventions that strengthen executive function, emotion regulation, and decision-making skills. Recognizing that certain neurodevelopmental factors precede substance use underscores the value of neuroscience-informed prevention and early screening in pediatric and school-based settings.
For scientists: The study demonstrates the power of large, longitudinal, open-science datasets like the ABCD Study for identifying neural markers of risk. Its findings lend support to models emphasizing predispositional neurobiological factors rather than only exposure effects. Future work should examine how these structural brain differences interact with genetics, environment, and psychosocial factors across adolescence to predict trajectories from experimentation to substance use disorder, and whether early interventions can modify these pathways.
For policy makers: These findings provide further justification for investing in early prevention and child development programs. Policies that support family stability, school-based prevention initiatives, and access to mental-health services, may mitigate risk for substance use and later substance-related problems.