Brain differences in recovery: A focus on reward circuits
Connections among brain regions, particularly those related to rewards, may hold clues to understanding the origins and treatment of substance use disorders. This study used brain imaging to investigate potential changes in structural connections among reward-related brain regions during recovery from opioid use disorder.
There is a growing interest in assessing white matter, the brain tissue that contains the myelinated portions of neurons (axons) that connect brain regions to one another. White matter connecting reward structures (e.g., nucleus accumbens, ventral tegmental area) may be different among those with substance use disorder and, therefore, changes in these white matter connections may serve as neurobiological markers of recovery. Determining how the relative strength of these white matter connections changes during substance use recovery may one day lead to better treatments for substance use disorders, such as opioid use disorder, which has serious potential psychological and physical consequences.
This longitudinal study measured white matter brain structure in adults with a history of opioid use disorder, specifically heroin use, in the early period of recovery (approximately 2 months of abstinence) and then 8 months later.
HOW WAS THIS STUDY CONDUCTED?
This study included 42 adults with an opioid use disorder (referred to by the research team as “Persons with Heroin Addiction [PHA]”, recruited from inpatient substance use disorder treatment located at a hospital in China, and 39 adults without a history of opioid use disorder recruited from the community. Opioid use disorder and non-opioid use disorder groups were matched for age and the relative balance of males and females. The opioid use disorder group had an average of 53 days of abstinence at baseline and an average of 307 days of abstinence at the 8-month follow-up. Additional inclusion criteria for the opioid use disorder group included no history of neurological or psychiatric disease, apart from substance use disorders. (Note: assessments used to confirm the presence or absence of neurological or psychiatric disorders were not reported.) Exclusion criteria for all participants included history of a head injury and use of any additional substances other than nicotine and alcohol in the past 5 years.
Opioid use disorder and non-opioid use disorder groups each completed a specialized Magnetic Resonance Imaging (MRI) scan, known as Diffusion Tensor Imaging, that assesses white matter integrity). The opioid use disorder group completed this scan twice, once in the early period of recovery (approximately two months of abstinence from heroin use) and then again 8 months later. In the opioid use disorder group, self-reported craving related for heroin use was measured using a 10-point scale (0 =weakest craving to 10 =strongest craving).
The study examined potential differences between opioid use disorder and non-opioid use disorder groups at baseline and changes between baseline and follow-up in white matter connections among reward-related brain regions.
The research team focused on potential white matter differences generally observed among adults with opioid use disorder and potential changes among these neural circuits during abstinence, respectively. They also tested whether variability in white matter at baseline among adults with opioid use disorder could predict person-specific changes in heroin craving. This approach reveals whether brain imaging can differentiate the relative success of an individuals’ substance use recovery, operationally defined in this study as reduced craving.
WHAT DID THIS STUDY FIND?
Multiple white matter connections differed between opioid use disorder and non-opioid use disorder groups.
Evidence for both increased and decreased white matter integrity (the relative strength of the connection) was seen in adults with opioid use disorder, relative to non-opioid use disorder adults. The largest effects distinguishing opioid use disorder and non-opioid use disorder groups were observed in 1) white matter connections that link a structure in the brain implicated in self-reflective experience called the insula and a structure implicated in reward called the nucleus accumbens as well as 2) those that link another structure implicated in reward called the ventral tegmental area with the nucleus accumbens.
Taken together, these results highlight a complex pattern of differences in structural brain connections between adults with and without opioid use disorder, but appear to converge, at least in part, on the nucleus accumbens, which is widely thought to mediate reward processing. Similar connections among other reward related brain regions (e.g., the ventral tegmental area), although importantly not the same connections, were shown to significantly differ after prolonged abstinence (8 months) from heroin use.
Differences in white matter connections of the nucleus accumbens predicted change in craving for heroin over time.
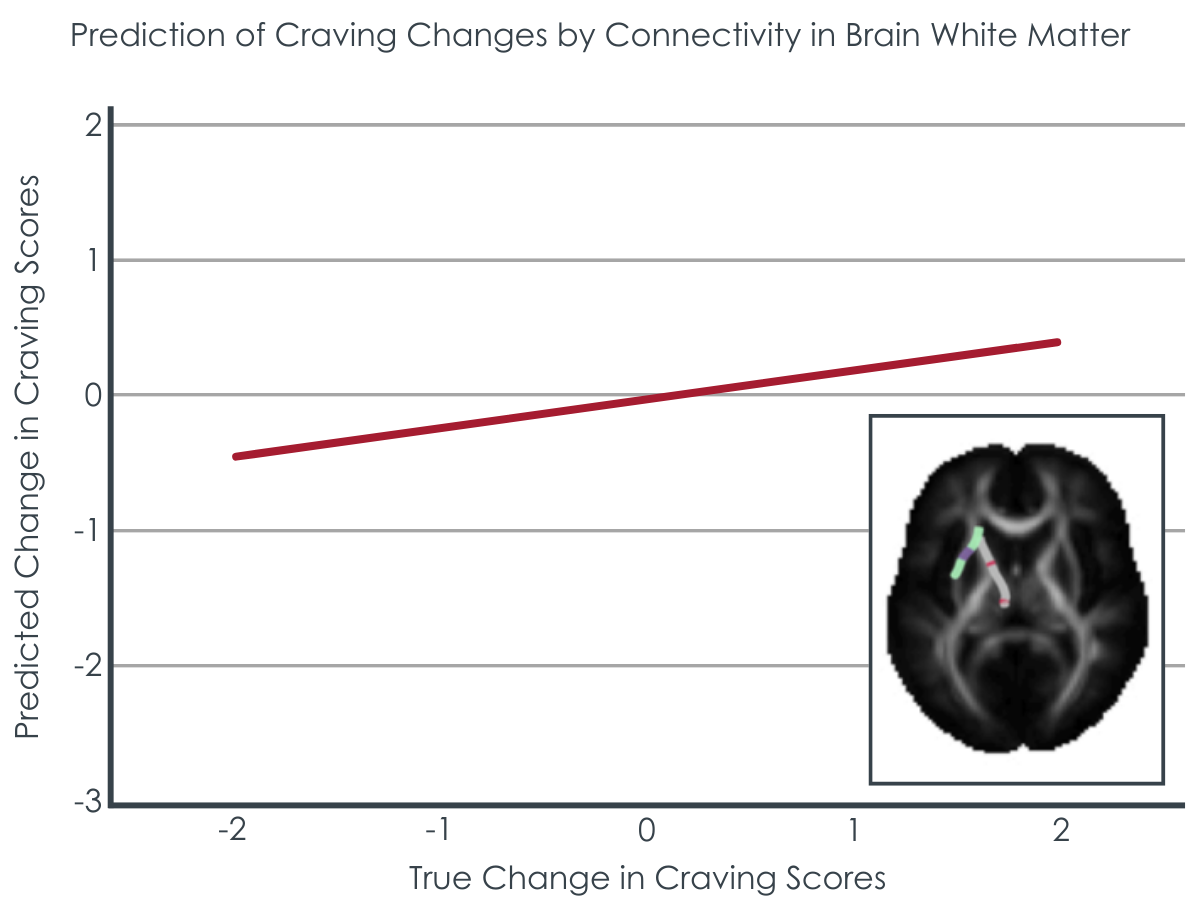
Between the baseline and 8-month assessments (Figure) differences in white matter connections of the nucleus accumbens predicated changes in heroin craving. Craving is a diagnostic feature of opioid use disorder (and other substance use disorders) and is thought to be a reliable marker of substance use disorder recovery.
Figure 1 adapted from Lu et al. 2023. This figure demonstrates the correlation between true changes in heroin craving scores (x-axis) and predicted changes in heroin craving scores (y-axis) generated from a machine learning model developed based on brain white matter differences in adults with opioid use disorder. The relatively large magnitude of the correlation between true and predicted scores and its high statistical significance suggests this may be a relevant neurobiological feature for understanding neural recovery from opioid use.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Adults with opioid use disorder appear to display differences in white matter connections among reward-related brain regions. The observed pattern differentiating adults with and without opioid use disorder in this study are complex.
This study and others using brain imaging techniques like MRI can further our understanding of the origins and treatment of substance use disorders. Longitudinal studies that follow individuals throughout the course of substance use disorder recovery may be especially useful. Towards this goal, the current study demonstrated that structural brain connections among reward-related regions were able to predict person-specific changes in heroin craving. In principle, this provides some indication that these brain regions may one day be useful to develop more personalized treatment and recovery support plans (often called “personalized medicine”). There are, however, limitations of this work worth noting (see below), and brain imaging in substance use recovery remains a relatively new field of scientific research.
The sample size of the study was relatively small. This may limit the generalizability of the results to other individuals and groups.
There were notable imbalances across opioid use disorder and non-opioid use disorder groups in years of education, and nicotine and alcohol use, which raises concern over the specificity of the results to opioid use disorder and raises additional concerns towards generalizability.
It is unclear the extent to which the findings reflect abstinence from opioid use alone or the relative presence/absence of nicotine and alcohol.
The studied periods of abstinence (53 on average at baseline and 307 days at 8-month follow-up) may have been insufficient to capture particularly short- or long-term changes.
The statistical analyses presented here were exploratory. That is, the analyses did not follow a pre-established published plan, which is used to prevent potential bias.
BOTTOM LINE
Opioid use disorder appears to be associated with differences in structural, white matter connections among reward-related brain regions. Similar brain connections also appear to be able to predict an individual’s relative changes in substance use craving during recovery. This work, along with a growing number of previous studies, suggests that brain imaging may one day be able to help tailor treatments for opioid use disorder and other substance use disorders (often called “personalized medicine”) or help measure response to treatment and other recovery-related progress. However, brain imaging in substance use disorders remains a relatively new field of scientific research. This work can therefore contribute to scientific knowledge regarding the neuroscience of recovery but not yet directly influence treatment.
For individuals and families seeking recovery: Brain imaging is providing exciting early insights into the neuroscience of opioid use disorder and other substance use disorders. It may be useful for patients and their families to understand through studies like this one why addiction is classified as disease; it is because chronic exposure to substances like opioids changes the brain structure in these ways and recovery from addiction is associated with reparative changes in the brain. However, this work is still in the early stages of scientific discovery. These and similar results help better clarify the brain basis of recovery, but more research is needed to clarify whether such investigations will prove clinically useful.
For treatment professionals and treatment systems: The results presented here provide potential insight into the mechanisms of opioid use disorder. Neural signatures that predict changes in opioid craving may one day be useful to help measure response to treatment, personalize treatment plans, or better predict outcomes. This area of research is still relatively new, however, and considerably more work is required before such results are equipped to directly impact treatment recommendations or practices.
For scientists:Basic science studies of recovery, including those using brain imaging, can help clarify potential targets for clinical intervention. This brain imaging study of opioid use recovery, however, relied on a relatively small sample size and exploratory analyses. Potential threats to generalizability in the current work further limit the direct translational impact of this work. Future studies, with larger sample sizes, pre-registered analyses and hypotheses, and improved procedures for addressing confounding are required. Additional studies with longer follow-up periods can help disambiguate potentially distinct short-term and long-term mechanisms of recovery.
For policy makers: Brain imaging studies may hold clues to understanding the origins and treatment of opioid use disorder and other substance use disorders. Longitudinal studies, that follow individuals across the course of substance use recovery are particularly valuable in this pursuit. Continued support for neuroscience studies of opioid use disorder, and other substance use disorders, can help test whether the insights generated from neuroimaging studies may be clinically useful.
There is a growing interest in assessing white matter, the brain tissue that contains the myelinated portions of neurons (axons) that connect brain regions to one another. White matter connecting reward structures (e.g., nucleus accumbens, ventral tegmental area) may be different among those with substance use disorder and, therefore, changes in these white matter connections may serve as neurobiological markers of recovery. Determining how the relative strength of these white matter connections changes during substance use recovery may one day lead to better treatments for substance use disorders, such as opioid use disorder, which has serious potential psychological and physical consequences.
This longitudinal study measured white matter brain structure in adults with a history of opioid use disorder, specifically heroin use, in the early period of recovery (approximately 2 months of abstinence) and then 8 months later.
HOW WAS THIS STUDY CONDUCTED?
This study included 42 adults with an opioid use disorder (referred to by the research team as “Persons with Heroin Addiction [PHA]”, recruited from inpatient substance use disorder treatment located at a hospital in China, and 39 adults without a history of opioid use disorder recruited from the community. Opioid use disorder and non-opioid use disorder groups were matched for age and the relative balance of males and females. The opioid use disorder group had an average of 53 days of abstinence at baseline and an average of 307 days of abstinence at the 8-month follow-up. Additional inclusion criteria for the opioid use disorder group included no history of neurological or psychiatric disease, apart from substance use disorders. (Note: assessments used to confirm the presence or absence of neurological or psychiatric disorders were not reported.) Exclusion criteria for all participants included history of a head injury and use of any additional substances other than nicotine and alcohol in the past 5 years.
Opioid use disorder and non-opioid use disorder groups each completed a specialized Magnetic Resonance Imaging (MRI) scan, known as Diffusion Tensor Imaging, that assesses white matter integrity). The opioid use disorder group completed this scan twice, once in the early period of recovery (approximately two months of abstinence from heroin use) and then again 8 months later. In the opioid use disorder group, self-reported craving related for heroin use was measured using a 10-point scale (0 =weakest craving to 10 =strongest craving).
The study examined potential differences between opioid use disorder and non-opioid use disorder groups at baseline and changes between baseline and follow-up in white matter connections among reward-related brain regions.
The research team focused on potential white matter differences generally observed among adults with opioid use disorder and potential changes among these neural circuits during abstinence, respectively. They also tested whether variability in white matter at baseline among adults with opioid use disorder could predict person-specific changes in heroin craving. This approach reveals whether brain imaging can differentiate the relative success of an individuals’ substance use recovery, operationally defined in this study as reduced craving.
WHAT DID THIS STUDY FIND?
Multiple white matter connections differed between opioid use disorder and non-opioid use disorder groups.
Evidence for both increased and decreased white matter integrity (the relative strength of the connection) was seen in adults with opioid use disorder, relative to non-opioid use disorder adults. The largest effects distinguishing opioid use disorder and non-opioid use disorder groups were observed in 1) white matter connections that link a structure in the brain implicated in self-reflective experience called the insula and a structure implicated in reward called the nucleus accumbens as well as 2) those that link another structure implicated in reward called the ventral tegmental area with the nucleus accumbens.
Taken together, these results highlight a complex pattern of differences in structural brain connections between adults with and without opioid use disorder, but appear to converge, at least in part, on the nucleus accumbens, which is widely thought to mediate reward processing. Similar connections among other reward related brain regions (e.g., the ventral tegmental area), although importantly not the same connections, were shown to significantly differ after prolonged abstinence (8 months) from heroin use.
Differences in white matter connections of the nucleus accumbens predicted change in craving for heroin over time.
Between the baseline and 8-month assessments (Figure) differences in white matter connections of the nucleus accumbens predicated changes in heroin craving. Craving is a diagnostic feature of opioid use disorder (and other substance use disorders) and is thought to be a reliable marker of substance use disorder recovery.
Figure 1 adapted from Lu et al. 2023. This figure demonstrates the correlation between true changes in heroin craving scores (x-axis) and predicted changes in heroin craving scores (y-axis) generated from a machine learning model developed based on brain white matter differences in adults with opioid use disorder. The relatively large magnitude of the correlation between true and predicted scores and its high statistical significance suggests this may be a relevant neurobiological feature for understanding neural recovery from opioid use.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Adults with opioid use disorder appear to display differences in white matter connections among reward-related brain regions. The observed pattern differentiating adults with and without opioid use disorder in this study are complex.
This study and others using brain imaging techniques like MRI can further our understanding of the origins and treatment of substance use disorders. Longitudinal studies that follow individuals throughout the course of substance use disorder recovery may be especially useful. Towards this goal, the current study demonstrated that structural brain connections among reward-related regions were able to predict person-specific changes in heroin craving. In principle, this provides some indication that these brain regions may one day be useful to develop more personalized treatment and recovery support plans (often called “personalized medicine”). There are, however, limitations of this work worth noting (see below), and brain imaging in substance use recovery remains a relatively new field of scientific research.
The sample size of the study was relatively small. This may limit the generalizability of the results to other individuals and groups.
There were notable imbalances across opioid use disorder and non-opioid use disorder groups in years of education, and nicotine and alcohol use, which raises concern over the specificity of the results to opioid use disorder and raises additional concerns towards generalizability.
It is unclear the extent to which the findings reflect abstinence from opioid use alone or the relative presence/absence of nicotine and alcohol.
The studied periods of abstinence (53 on average at baseline and 307 days at 8-month follow-up) may have been insufficient to capture particularly short- or long-term changes.
The statistical analyses presented here were exploratory. That is, the analyses did not follow a pre-established published plan, which is used to prevent potential bias.
BOTTOM LINE
Opioid use disorder appears to be associated with differences in structural, white matter connections among reward-related brain regions. Similar brain connections also appear to be able to predict an individual’s relative changes in substance use craving during recovery. This work, along with a growing number of previous studies, suggests that brain imaging may one day be able to help tailor treatments for opioid use disorder and other substance use disorders (often called “personalized medicine”) or help measure response to treatment and other recovery-related progress. However, brain imaging in substance use disorders remains a relatively new field of scientific research. This work can therefore contribute to scientific knowledge regarding the neuroscience of recovery but not yet directly influence treatment.
For individuals and families seeking recovery: Brain imaging is providing exciting early insights into the neuroscience of opioid use disorder and other substance use disorders. It may be useful for patients and their families to understand through studies like this one why addiction is classified as disease; it is because chronic exposure to substances like opioids changes the brain structure in these ways and recovery from addiction is associated with reparative changes in the brain. However, this work is still in the early stages of scientific discovery. These and similar results help better clarify the brain basis of recovery, but more research is needed to clarify whether such investigations will prove clinically useful.
For treatment professionals and treatment systems: The results presented here provide potential insight into the mechanisms of opioid use disorder. Neural signatures that predict changes in opioid craving may one day be useful to help measure response to treatment, personalize treatment plans, or better predict outcomes. This area of research is still relatively new, however, and considerably more work is required before such results are equipped to directly impact treatment recommendations or practices.
For scientists:Basic science studies of recovery, including those using brain imaging, can help clarify potential targets for clinical intervention. This brain imaging study of opioid use recovery, however, relied on a relatively small sample size and exploratory analyses. Potential threats to generalizability in the current work further limit the direct translational impact of this work. Future studies, with larger sample sizes, pre-registered analyses and hypotheses, and improved procedures for addressing confounding are required. Additional studies with longer follow-up periods can help disambiguate potentially distinct short-term and long-term mechanisms of recovery.
For policy makers: Brain imaging studies may hold clues to understanding the origins and treatment of opioid use disorder and other substance use disorders. Longitudinal studies, that follow individuals across the course of substance use recovery are particularly valuable in this pursuit. Continued support for neuroscience studies of opioid use disorder, and other substance use disorders, can help test whether the insights generated from neuroimaging studies may be clinically useful.
There is a growing interest in assessing white matter, the brain tissue that contains the myelinated portions of neurons (axons) that connect brain regions to one another. White matter connecting reward structures (e.g., nucleus accumbens, ventral tegmental area) may be different among those with substance use disorder and, therefore, changes in these white matter connections may serve as neurobiological markers of recovery. Determining how the relative strength of these white matter connections changes during substance use recovery may one day lead to better treatments for substance use disorders, such as opioid use disorder, which has serious potential psychological and physical consequences.
This longitudinal study measured white matter brain structure in adults with a history of opioid use disorder, specifically heroin use, in the early period of recovery (approximately 2 months of abstinence) and then 8 months later.
HOW WAS THIS STUDY CONDUCTED?
This study included 42 adults with an opioid use disorder (referred to by the research team as “Persons with Heroin Addiction [PHA]”, recruited from inpatient substance use disorder treatment located at a hospital in China, and 39 adults without a history of opioid use disorder recruited from the community. Opioid use disorder and non-opioid use disorder groups were matched for age and the relative balance of males and females. The opioid use disorder group had an average of 53 days of abstinence at baseline and an average of 307 days of abstinence at the 8-month follow-up. Additional inclusion criteria for the opioid use disorder group included no history of neurological or psychiatric disease, apart from substance use disorders. (Note: assessments used to confirm the presence or absence of neurological or psychiatric disorders were not reported.) Exclusion criteria for all participants included history of a head injury and use of any additional substances other than nicotine and alcohol in the past 5 years.
Opioid use disorder and non-opioid use disorder groups each completed a specialized Magnetic Resonance Imaging (MRI) scan, known as Diffusion Tensor Imaging, that assesses white matter integrity). The opioid use disorder group completed this scan twice, once in the early period of recovery (approximately two months of abstinence from heroin use) and then again 8 months later. In the opioid use disorder group, self-reported craving related for heroin use was measured using a 10-point scale (0 =weakest craving to 10 =strongest craving).
The study examined potential differences between opioid use disorder and non-opioid use disorder groups at baseline and changes between baseline and follow-up in white matter connections among reward-related brain regions.
The research team focused on potential white matter differences generally observed among adults with opioid use disorder and potential changes among these neural circuits during abstinence, respectively. They also tested whether variability in white matter at baseline among adults with opioid use disorder could predict person-specific changes in heroin craving. This approach reveals whether brain imaging can differentiate the relative success of an individuals’ substance use recovery, operationally defined in this study as reduced craving.
WHAT DID THIS STUDY FIND?
Multiple white matter connections differed between opioid use disorder and non-opioid use disorder groups.
Evidence for both increased and decreased white matter integrity (the relative strength of the connection) was seen in adults with opioid use disorder, relative to non-opioid use disorder adults. The largest effects distinguishing opioid use disorder and non-opioid use disorder groups were observed in 1) white matter connections that link a structure in the brain implicated in self-reflective experience called the insula and a structure implicated in reward called the nucleus accumbens as well as 2) those that link another structure implicated in reward called the ventral tegmental area with the nucleus accumbens.
Taken together, these results highlight a complex pattern of differences in structural brain connections between adults with and without opioid use disorder, but appear to converge, at least in part, on the nucleus accumbens, which is widely thought to mediate reward processing. Similar connections among other reward related brain regions (e.g., the ventral tegmental area), although importantly not the same connections, were shown to significantly differ after prolonged abstinence (8 months) from heroin use.
Differences in white matter connections of the nucleus accumbens predicted change in craving for heroin over time.
Between the baseline and 8-month assessments (Figure) differences in white matter connections of the nucleus accumbens predicated changes in heroin craving. Craving is a diagnostic feature of opioid use disorder (and other substance use disorders) and is thought to be a reliable marker of substance use disorder recovery.
Figure 1 adapted from Lu et al. 2023. This figure demonstrates the correlation between true changes in heroin craving scores (x-axis) and predicted changes in heroin craving scores (y-axis) generated from a machine learning model developed based on brain white matter differences in adults with opioid use disorder. The relatively large magnitude of the correlation between true and predicted scores and its high statistical significance suggests this may be a relevant neurobiological feature for understanding neural recovery from opioid use.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Adults with opioid use disorder appear to display differences in white matter connections among reward-related brain regions. The observed pattern differentiating adults with and without opioid use disorder in this study are complex.
This study and others using brain imaging techniques like MRI can further our understanding of the origins and treatment of substance use disorders. Longitudinal studies that follow individuals throughout the course of substance use disorder recovery may be especially useful. Towards this goal, the current study demonstrated that structural brain connections among reward-related regions were able to predict person-specific changes in heroin craving. In principle, this provides some indication that these brain regions may one day be useful to develop more personalized treatment and recovery support plans (often called “personalized medicine”). There are, however, limitations of this work worth noting (see below), and brain imaging in substance use recovery remains a relatively new field of scientific research.
The sample size of the study was relatively small. This may limit the generalizability of the results to other individuals and groups.
There were notable imbalances across opioid use disorder and non-opioid use disorder groups in years of education, and nicotine and alcohol use, which raises concern over the specificity of the results to opioid use disorder and raises additional concerns towards generalizability.
It is unclear the extent to which the findings reflect abstinence from opioid use alone or the relative presence/absence of nicotine and alcohol.
The studied periods of abstinence (53 on average at baseline and 307 days at 8-month follow-up) may have been insufficient to capture particularly short- or long-term changes.
The statistical analyses presented here were exploratory. That is, the analyses did not follow a pre-established published plan, which is used to prevent potential bias.
BOTTOM LINE
Opioid use disorder appears to be associated with differences in structural, white matter connections among reward-related brain regions. Similar brain connections also appear to be able to predict an individual’s relative changes in substance use craving during recovery. This work, along with a growing number of previous studies, suggests that brain imaging may one day be able to help tailor treatments for opioid use disorder and other substance use disorders (often called “personalized medicine”) or help measure response to treatment and other recovery-related progress. However, brain imaging in substance use disorders remains a relatively new field of scientific research. This work can therefore contribute to scientific knowledge regarding the neuroscience of recovery but not yet directly influence treatment.
For individuals and families seeking recovery: Brain imaging is providing exciting early insights into the neuroscience of opioid use disorder and other substance use disorders. It may be useful for patients and their families to understand through studies like this one why addiction is classified as disease; it is because chronic exposure to substances like opioids changes the brain structure in these ways and recovery from addiction is associated with reparative changes in the brain. However, this work is still in the early stages of scientific discovery. These and similar results help better clarify the brain basis of recovery, but more research is needed to clarify whether such investigations will prove clinically useful.
For treatment professionals and treatment systems: The results presented here provide potential insight into the mechanisms of opioid use disorder. Neural signatures that predict changes in opioid craving may one day be useful to help measure response to treatment, personalize treatment plans, or better predict outcomes. This area of research is still relatively new, however, and considerably more work is required before such results are equipped to directly impact treatment recommendations or practices.
For scientists:Basic science studies of recovery, including those using brain imaging, can help clarify potential targets for clinical intervention. This brain imaging study of opioid use recovery, however, relied on a relatively small sample size and exploratory analyses. Potential threats to generalizability in the current work further limit the direct translational impact of this work. Future studies, with larger sample sizes, pre-registered analyses and hypotheses, and improved procedures for addressing confounding are required. Additional studies with longer follow-up periods can help disambiguate potentially distinct short-term and long-term mechanisms of recovery.
For policy makers: Brain imaging studies may hold clues to understanding the origins and treatment of opioid use disorder and other substance use disorders. Longitudinal studies, that follow individuals across the course of substance use recovery are particularly valuable in this pursuit. Continued support for neuroscience studies of opioid use disorder, and other substance use disorders, can help test whether the insights generated from neuroimaging studies may be clinically useful.