“Who You Gonna Call?” Not Medicaid patients: Telehealth substance use disorder treatment disparities
Telehealth services may help reduce treatment disparities by addressing some of the known healthcare barriers like distance to treatment. Yet it is unclear how recent telehealth expansion has impacted utilization. This study looked at this with a particular focus on insurance coverage and rural vs. urban location.
Telehealth services (e.g., consulting with healthcare providers directly via video conferencing software) has become increasingly common over the past few years – telehealth visits increased by 75% from 2020 to 2021. This shift to telehealth was initially related to public gathering restrictions to curb the COVID-19 pandemic. These restrictions lead to healthcare professionals pivoting from providing traditional in-person visits to relying more on telehealth services. This transition allowed patients that had access to the internet to continue receiving needed care while also following COVID-19 physical distancing guidelines. In addition to reducing potential infection, telehealth services have the added benefit of alleviating transportation and local workforce shortage barriers to care – important barriers to treatment for those on Medicaid and/or living in rural areas.
Medicaid is public health insurance for low-income people. Currently 72 million people in the US are on Medicaid. Despite being a common form of insurance coverage, evidence suggests that those on Medicaid experience many barriers to engaging in, and benefitting from, substance use disorder care. This may be partially due to Medicaid disproportionately serving racially/ethnically minoritized people (e.g., Hispanic Americans), an issue where providers lack the capacity to speak languages other than English. In addition, individuals living in rural areas face multiple challenges to effective treatment including a lack of local providers. That is, evidence shows that rural areas are less likely to attract specialty-trained clinicians making it challenging to access quality care in such areas. There is also evidence that transportation can make care harder to access among those on Medicaid and/or those in rural settings. Telehealth has the potential to remove such barriers by allowing those on Medicaid and/or in rural areas to virtually connect with providers who meet their needs while remaining in their homes. However, it is unclear how much Medicaid recipients and those living in rural areas utilize telehealth substance use disorder treatment services. To this end, the current study sought to determine how rates of telehealth services for substance use disorder treatment have changed since 2019 and how such changes differ across insurance coverage and rurality of patients.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the MedInsight Emerging Experience database. Data were enrollees’ health care visits for services billed to the health plan for payment purposes (e.g., visit or procedure codes) across the US. This dataset included those receiving Medicaid managed care, Medicare Advantage, and commercial insurance. This data also included patient rurality as defined by Rural-Urban Commuting Area Codes. Aside from rurality, data were completely de-identified (anonymous) – no other demographic information on patients (e.g., age, assigned birth sex, etc.) were included.
The study included a cohort of US adults (18+ years of age), who were insured for at least 12 months during the study period (January 1, 2019, to June 30, 2023). This resulted in a sample of 16.2 million people. The authors calculated utilization for in-person, telehealth, and overall (telehealth and in-person) substance use disorder treatment using the Milliman Health Cost Guidelines grouper. Telehealth services were identified through procedure and modifier codes and place of service.
The main outcome of this study was proportional use of each substance use disorder treatment service modality (telehealth vs. in-person) compared with overall substance use disorder treatment. The authors calculated average monthly substance use disorder treatment utilization per 100,000 adults to adjust for enrollment volume. All analyses were stratified by patients’ insurance type and rurality.
WHAT DID THIS STUDY FIND?
Overall substance use disorder treatment service rates increased from 2019-2023
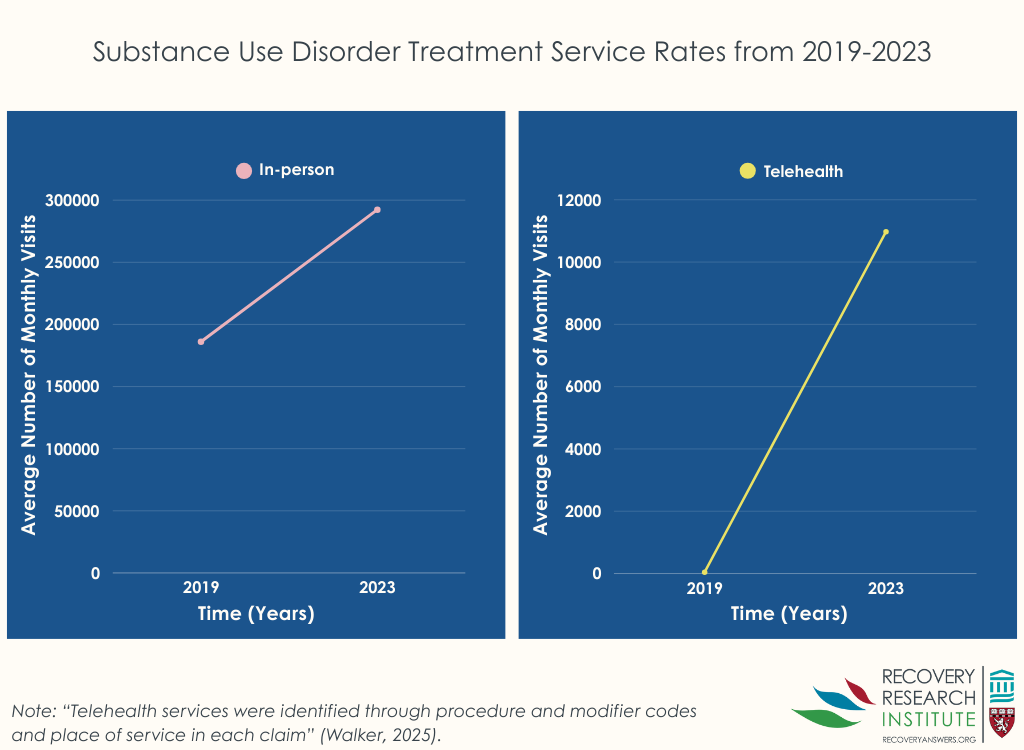
Between 2019 and 2023, the average number of monthly telehealth visits for substance use disorder treatment increased dramatically from just 44.6 to 10,974.3. In addition, the average number of in-person substance use disorder visits increased from 186,064 to 292,364 (Figure below).
Medicaid-covered individuals were underrepresented in telehealth services
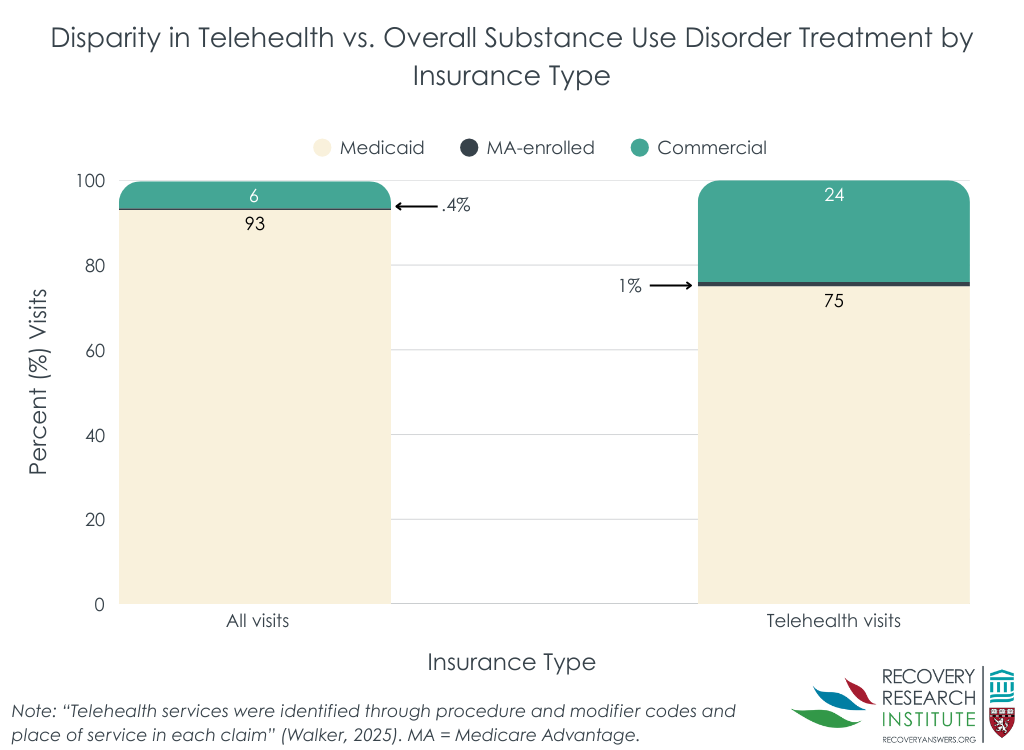
Despite making up 93.0% of all substance use disorder treatment visits, Medicaid-covered individuals only accounted for 75.0% of telehealth substance use disorder treatment services used (Figure below). In contrast, Medicare-Advantage-enrolled and commercially insured individuals accounted for 1.0% and 24.0% respectively of telehealth substance use disorder treatment services used, despite only accounting for 0.4% and 6.4% respectively of overall substance use disorder treatment visits.
Rural and urban individuals used telehealth services at proportional rates
Rural individuals increased their overall treatment rates more than those in urban areas, but this increase was mostly accounted for by in-person visits. Indeed, rural individuals accounted for 6.4% of all substance use disorder treatment services used and 8.1% of telehealth substance use disorder treatment services used. In comparison, urban individuals accounted for 93.2% of all substance use disorder treatment service used and for 91.0% of telehealth substance use disorder treatment service usage. Therefore, counter to expectations, no differences between telehealth services were found for individuals in rural areas.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study show individuals with Medicaid coverage are underrepresented in telehealth substance use disorder treatment services based on their overall treatment utilization. However, somewhat surprisingly, those in rural settings used telehealth services for substance use disorder treatment at rates proportional to their overall treatment utilization.
Results of the present study suggest that despite telehealth services alleviating potential barriers to treatment for some, those on Medicaid may have difficulty leveraging the increased access offered by telehealth. That is, telehealth removes the need to travel for treatment and rely on local providers, so other factors specific to Medicaid recipients – such as lower socioeconomic conditions – may be limiting its use. In addition, there is evidence that due to differing state policies, telehealth can be more difficult to access for Medicaid recipients than those with private insurance. Furthermore, telehealth often requires stable internet access, which low-income patients (i.e. those on Medicaid) are less likely to have. Recovery community centers – centrally-located community services that provide recovery supports and resources including internet access – may be helpful ways to address these barriers, though their utility specifically in Medicaid patients has not yet been examined. Relatedly, it is also possible that broadband internet infrastructure is not sufficient in rural areas – many of whom may also covered by Medicare – across the US to improve their access to telehealth.
Ultimately, the results of this study suggest that telehealth can be a viable treatment option for substance use disorder treatment. Although telehealth was disproportionately used by those with Medicare Advantage or commercially available insurance, increases in telehealth use were seen across all patients. To be clear, this study did not examine how effective the telehealth services were at treating substance use disorder (although other research suggests that telehealth for individual substance use disorder therapy in general is effective). Nevertheless, eliminating barriers to telehealth in the US could be a way to reduce the impact of substance use disorder on the population. Efforts to ensure access to telehealth services (e.g., access to affordable high-speed internet) should be expanded.
The present study offers very little information on the dataset and analysis procedures, making the results difficult to interpret. The authors state that they used the MedInsight Emerging Experience database which appears to be proprietary. The authors also declined to make their data publicly available as “The MedInsight Emerging Experience database used for this study is considered proprietary to Milliman MedInsight® and therefore cannot be shared”. It is unclear how these data were collected and how representative they are of the general US population.
Relatedly, the analytical tools/techniques used are not clear. The authors describe using the Milliman Health Cost Guidelines grouper which appears to be proprietary statistical software. No guidelines or examples were cited which could shed light on how exactly this software works or how it handles data. This lack of clarity calls into question the conclusions drawn from this research.
The present study does not differentiate treatment utilization by specific types of treatment. This is relevant as there is some evidence that different substance use disorder treatments are harder to deliver via telehealth services (e.g., group therapy).
Telehealth services increased substantially from 2019-2023, though Medicaid-covered individuals were underrepresented compared to their overall treatment utilization. The study also found that, unexpectedly, rural and urban individuals used telehealth services at proportional rates. It is possible that other barriers associated with lower socioeconomic status may be preventing full telehealth service utilization among Medicaid recipients. Relatedly, broadband internet infrastructure may not be sufficient in rural areas to improve their access to telehealth. Understanding what these barriers may be and how they can be overcome will be vital in expanding uptake of telehealth substance use disorder treatments.
For individuals and families seeking recovery: The present study suggests that individuals and families seeking recovery may find that telehealth is a viable treatment option for substance use disorder. Telehealth services can be useful in overcoming barriers to in-person care, like transportation challenges and limited local provider availability. Families should encourage their loved ones to explore telehealth options, especially if access to local in-person treatment programs is limited. However, those seeking recovery would do well to check insurance coverage. Although Medicaid covers some telehealth services, there may be barriers to utilizing telehealth for substance use disorder treatment. As telehealth continues to expand, being proactive about understanding available resources and advocating for access to high-quality, remote treatment services can help individuals and families navigate recovery more effectively.
For treatment professionals and treatment systems: The present study highlights the need for treatment professionals and those working in treatment systems to address disparities in telehealth utilization. While telehealth has expanded access to care, particularly during the COVID-19 pandemic, Medicaid recipients continue to use these services at disproportionately lower rates. Providers should work to ensure that telehealth options are accessible and effectively integrated into treatment plans, particularly for underserved populations. This may include assisting patients with navigating insurance coverage, providing technical support for telehealth access, and advocating for policy changes that expand Medicaid reimbursement for remote services. Additionally, treatment systems would do well to incorporate multilingual providers. By addressing these barriers, treatment professionals and systems can help maximize the potential of telehealth to improve substance use disorder treatment access and outcomes.
For scientists: The present study underscores the need for scientists to further research the effectiveness, accessibility, and equity of telehealth for substance use disorder treatment. Although, telehealth utilization has increased overall, this study suggests that Medicaid recipients face barriers to access. Future research should explore the specific factors limiting telehealth use among Medicaid beneficiaries, including policy restrictions, provider availability, and technological challenges (e.g., stable internet access). By addressing these gaps, researchers can inform policies and interventions that enhance telehealth’s role in expanding equitable access to substance use disorder treatment.
For policy makers: The present study suggests that policymakers may consider policies that improve equitable access to telehealth substance use disorder treatment for Medicaid recipients. Expanding Medicaid reimbursement for telehealth-based substance use disorder care could help address disparities. Policymakers could also invest in infrastructure to ensure individuals in rural and low-income areas have stable broadband internet so they can reliably access telehealth services. Additionally, policies should encourage provider participation in Medicaid telehealth programs by streamlining reimbursement processes and reducing administrative burdens. Finally, addressing regulatory barriers that limit telehealth access across state lines could enhance provider availability and improve care access and ultimately treatment success. By prioritizing these policy changes, lawmakers can strengthen the role of telehealth in expanding access to effective, evidence-based substance use disorder treatment.
Telehealth services (e.g., consulting with healthcare providers directly via video conferencing software) has become increasingly common over the past few years – telehealth visits increased by 75% from 2020 to 2021. This shift to telehealth was initially related to public gathering restrictions to curb the COVID-19 pandemic. These restrictions lead to healthcare professionals pivoting from providing traditional in-person visits to relying more on telehealth services. This transition allowed patients that had access to the internet to continue receiving needed care while also following COVID-19 physical distancing guidelines. In addition to reducing potential infection, telehealth services have the added benefit of alleviating transportation and local workforce shortage barriers to care – important barriers to treatment for those on Medicaid and/or living in rural areas.
Medicaid is public health insurance for low-income people. Currently 72 million people in the US are on Medicaid. Despite being a common form of insurance coverage, evidence suggests that those on Medicaid experience many barriers to engaging in, and benefitting from, substance use disorder care. This may be partially due to Medicaid disproportionately serving racially/ethnically minoritized people (e.g., Hispanic Americans), an issue where providers lack the capacity to speak languages other than English. In addition, individuals living in rural areas face multiple challenges to effective treatment including a lack of local providers. That is, evidence shows that rural areas are less likely to attract specialty-trained clinicians making it challenging to access quality care in such areas. There is also evidence that transportation can make care harder to access among those on Medicaid and/or those in rural settings. Telehealth has the potential to remove such barriers by allowing those on Medicaid and/or in rural areas to virtually connect with providers who meet their needs while remaining in their homes. However, it is unclear how much Medicaid recipients and those living in rural areas utilize telehealth substance use disorder treatment services. To this end, the current study sought to determine how rates of telehealth services for substance use disorder treatment have changed since 2019 and how such changes differ across insurance coverage and rurality of patients.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the MedInsight Emerging Experience database. Data were enrollees’ health care visits for services billed to the health plan for payment purposes (e.g., visit or procedure codes) across the US. This dataset included those receiving Medicaid managed care, Medicare Advantage, and commercial insurance. This data also included patient rurality as defined by Rural-Urban Commuting Area Codes. Aside from rurality, data were completely de-identified (anonymous) – no other demographic information on patients (e.g., age, assigned birth sex, etc.) were included.
The study included a cohort of US adults (18+ years of age), who were insured for at least 12 months during the study period (January 1, 2019, to June 30, 2023). This resulted in a sample of 16.2 million people. The authors calculated utilization for in-person, telehealth, and overall (telehealth and in-person) substance use disorder treatment using the Milliman Health Cost Guidelines grouper. Telehealth services were identified through procedure and modifier codes and place of service.
The main outcome of this study was proportional use of each substance use disorder treatment service modality (telehealth vs. in-person) compared with overall substance use disorder treatment. The authors calculated average monthly substance use disorder treatment utilization per 100,000 adults to adjust for enrollment volume. All analyses were stratified by patients’ insurance type and rurality.
WHAT DID THIS STUDY FIND?
Overall substance use disorder treatment service rates increased from 2019-2023
Between 2019 and 2023, the average number of monthly telehealth visits for substance use disorder treatment increased dramatically from just 44.6 to 10,974.3. In addition, the average number of in-person substance use disorder visits increased from 186,064 to 292,364 (Figure below).
Medicaid-covered individuals were underrepresented in telehealth services
Despite making up 93.0% of all substance use disorder treatment visits, Medicaid-covered individuals only accounted for 75.0% of telehealth substance use disorder treatment services used (Figure below). In contrast, Medicare-Advantage-enrolled and commercially insured individuals accounted for 1.0% and 24.0% respectively of telehealth substance use disorder treatment services used, despite only accounting for 0.4% and 6.4% respectively of overall substance use disorder treatment visits.
Rural and urban individuals used telehealth services at proportional rates
Rural individuals increased their overall treatment rates more than those in urban areas, but this increase was mostly accounted for by in-person visits. Indeed, rural individuals accounted for 6.4% of all substance use disorder treatment services used and 8.1% of telehealth substance use disorder treatment services used. In comparison, urban individuals accounted for 93.2% of all substance use disorder treatment service used and for 91.0% of telehealth substance use disorder treatment service usage. Therefore, counter to expectations, no differences between telehealth services were found for individuals in rural areas.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study show individuals with Medicaid coverage are underrepresented in telehealth substance use disorder treatment services based on their overall treatment utilization. However, somewhat surprisingly, those in rural settings used telehealth services for substance use disorder treatment at rates proportional to their overall treatment utilization.
Results of the present study suggest that despite telehealth services alleviating potential barriers to treatment for some, those on Medicaid may have difficulty leveraging the increased access offered by telehealth. That is, telehealth removes the need to travel for treatment and rely on local providers, so other factors specific to Medicaid recipients – such as lower socioeconomic conditions – may be limiting its use. In addition, there is evidence that due to differing state policies, telehealth can be more difficult to access for Medicaid recipients than those with private insurance. Furthermore, telehealth often requires stable internet access, which low-income patients (i.e. those on Medicaid) are less likely to have. Recovery community centers – centrally-located community services that provide recovery supports and resources including internet access – may be helpful ways to address these barriers, though their utility specifically in Medicaid patients has not yet been examined. Relatedly, it is also possible that broadband internet infrastructure is not sufficient in rural areas – many of whom may also covered by Medicare – across the US to improve their access to telehealth.
Ultimately, the results of this study suggest that telehealth can be a viable treatment option for substance use disorder treatment. Although telehealth was disproportionately used by those with Medicare Advantage or commercially available insurance, increases in telehealth use were seen across all patients. To be clear, this study did not examine how effective the telehealth services were at treating substance use disorder (although other research suggests that telehealth for individual substance use disorder therapy in general is effective). Nevertheless, eliminating barriers to telehealth in the US could be a way to reduce the impact of substance use disorder on the population. Efforts to ensure access to telehealth services (e.g., access to affordable high-speed internet) should be expanded.
The present study offers very little information on the dataset and analysis procedures, making the results difficult to interpret. The authors state that they used the MedInsight Emerging Experience database which appears to be proprietary. The authors also declined to make their data publicly available as “The MedInsight Emerging Experience database used for this study is considered proprietary to Milliman MedInsight® and therefore cannot be shared”. It is unclear how these data were collected and how representative they are of the general US population.
Relatedly, the analytical tools/techniques used are not clear. The authors describe using the Milliman Health Cost Guidelines grouper which appears to be proprietary statistical software. No guidelines or examples were cited which could shed light on how exactly this software works or how it handles data. This lack of clarity calls into question the conclusions drawn from this research.
The present study does not differentiate treatment utilization by specific types of treatment. This is relevant as there is some evidence that different substance use disorder treatments are harder to deliver via telehealth services (e.g., group therapy).
Telehealth services increased substantially from 2019-2023, though Medicaid-covered individuals were underrepresented compared to their overall treatment utilization. The study also found that, unexpectedly, rural and urban individuals used telehealth services at proportional rates. It is possible that other barriers associated with lower socioeconomic status may be preventing full telehealth service utilization among Medicaid recipients. Relatedly, broadband internet infrastructure may not be sufficient in rural areas to improve their access to telehealth. Understanding what these barriers may be and how they can be overcome will be vital in expanding uptake of telehealth substance use disorder treatments.
For individuals and families seeking recovery: The present study suggests that individuals and families seeking recovery may find that telehealth is a viable treatment option for substance use disorder. Telehealth services can be useful in overcoming barriers to in-person care, like transportation challenges and limited local provider availability. Families should encourage their loved ones to explore telehealth options, especially if access to local in-person treatment programs is limited. However, those seeking recovery would do well to check insurance coverage. Although Medicaid covers some telehealth services, there may be barriers to utilizing telehealth for substance use disorder treatment. As telehealth continues to expand, being proactive about understanding available resources and advocating for access to high-quality, remote treatment services can help individuals and families navigate recovery more effectively.
For treatment professionals and treatment systems: The present study highlights the need for treatment professionals and those working in treatment systems to address disparities in telehealth utilization. While telehealth has expanded access to care, particularly during the COVID-19 pandemic, Medicaid recipients continue to use these services at disproportionately lower rates. Providers should work to ensure that telehealth options are accessible and effectively integrated into treatment plans, particularly for underserved populations. This may include assisting patients with navigating insurance coverage, providing technical support for telehealth access, and advocating for policy changes that expand Medicaid reimbursement for remote services. Additionally, treatment systems would do well to incorporate multilingual providers. By addressing these barriers, treatment professionals and systems can help maximize the potential of telehealth to improve substance use disorder treatment access and outcomes.
For scientists: The present study underscores the need for scientists to further research the effectiveness, accessibility, and equity of telehealth for substance use disorder treatment. Although, telehealth utilization has increased overall, this study suggests that Medicaid recipients face barriers to access. Future research should explore the specific factors limiting telehealth use among Medicaid beneficiaries, including policy restrictions, provider availability, and technological challenges (e.g., stable internet access). By addressing these gaps, researchers can inform policies and interventions that enhance telehealth’s role in expanding equitable access to substance use disorder treatment.
For policy makers: The present study suggests that policymakers may consider policies that improve equitable access to telehealth substance use disorder treatment for Medicaid recipients. Expanding Medicaid reimbursement for telehealth-based substance use disorder care could help address disparities. Policymakers could also invest in infrastructure to ensure individuals in rural and low-income areas have stable broadband internet so they can reliably access telehealth services. Additionally, policies should encourage provider participation in Medicaid telehealth programs by streamlining reimbursement processes and reducing administrative burdens. Finally, addressing regulatory barriers that limit telehealth access across state lines could enhance provider availability and improve care access and ultimately treatment success. By prioritizing these policy changes, lawmakers can strengthen the role of telehealth in expanding access to effective, evidence-based substance use disorder treatment.
Telehealth services (e.g., consulting with healthcare providers directly via video conferencing software) has become increasingly common over the past few years – telehealth visits increased by 75% from 2020 to 2021. This shift to telehealth was initially related to public gathering restrictions to curb the COVID-19 pandemic. These restrictions lead to healthcare professionals pivoting from providing traditional in-person visits to relying more on telehealth services. This transition allowed patients that had access to the internet to continue receiving needed care while also following COVID-19 physical distancing guidelines. In addition to reducing potential infection, telehealth services have the added benefit of alleviating transportation and local workforce shortage barriers to care – important barriers to treatment for those on Medicaid and/or living in rural areas.
Medicaid is public health insurance for low-income people. Currently 72 million people in the US are on Medicaid. Despite being a common form of insurance coverage, evidence suggests that those on Medicaid experience many barriers to engaging in, and benefitting from, substance use disorder care. This may be partially due to Medicaid disproportionately serving racially/ethnically minoritized people (e.g., Hispanic Americans), an issue where providers lack the capacity to speak languages other than English. In addition, individuals living in rural areas face multiple challenges to effective treatment including a lack of local providers. That is, evidence shows that rural areas are less likely to attract specialty-trained clinicians making it challenging to access quality care in such areas. There is also evidence that transportation can make care harder to access among those on Medicaid and/or those in rural settings. Telehealth has the potential to remove such barriers by allowing those on Medicaid and/or in rural areas to virtually connect with providers who meet their needs while remaining in their homes. However, it is unclear how much Medicaid recipients and those living in rural areas utilize telehealth substance use disorder treatment services. To this end, the current study sought to determine how rates of telehealth services for substance use disorder treatment have changed since 2019 and how such changes differ across insurance coverage and rurality of patients.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the MedInsight Emerging Experience database. Data were enrollees’ health care visits for services billed to the health plan for payment purposes (e.g., visit or procedure codes) across the US. This dataset included those receiving Medicaid managed care, Medicare Advantage, and commercial insurance. This data also included patient rurality as defined by Rural-Urban Commuting Area Codes. Aside from rurality, data were completely de-identified (anonymous) – no other demographic information on patients (e.g., age, assigned birth sex, etc.) were included.
The study included a cohort of US adults (18+ years of age), who were insured for at least 12 months during the study period (January 1, 2019, to June 30, 2023). This resulted in a sample of 16.2 million people. The authors calculated utilization for in-person, telehealth, and overall (telehealth and in-person) substance use disorder treatment using the Milliman Health Cost Guidelines grouper. Telehealth services were identified through procedure and modifier codes and place of service.
The main outcome of this study was proportional use of each substance use disorder treatment service modality (telehealth vs. in-person) compared with overall substance use disorder treatment. The authors calculated average monthly substance use disorder treatment utilization per 100,000 adults to adjust for enrollment volume. All analyses were stratified by patients’ insurance type and rurality.
WHAT DID THIS STUDY FIND?
Overall substance use disorder treatment service rates increased from 2019-2023
Between 2019 and 2023, the average number of monthly telehealth visits for substance use disorder treatment increased dramatically from just 44.6 to 10,974.3. In addition, the average number of in-person substance use disorder visits increased from 186,064 to 292,364 (Figure below).
Medicaid-covered individuals were underrepresented in telehealth services
Despite making up 93.0% of all substance use disorder treatment visits, Medicaid-covered individuals only accounted for 75.0% of telehealth substance use disorder treatment services used (Figure below). In contrast, Medicare-Advantage-enrolled and commercially insured individuals accounted for 1.0% and 24.0% respectively of telehealth substance use disorder treatment services used, despite only accounting for 0.4% and 6.4% respectively of overall substance use disorder treatment visits.
Rural and urban individuals used telehealth services at proportional rates
Rural individuals increased their overall treatment rates more than those in urban areas, but this increase was mostly accounted for by in-person visits. Indeed, rural individuals accounted for 6.4% of all substance use disorder treatment services used and 8.1% of telehealth substance use disorder treatment services used. In comparison, urban individuals accounted for 93.2% of all substance use disorder treatment service used and for 91.0% of telehealth substance use disorder treatment service usage. Therefore, counter to expectations, no differences between telehealth services were found for individuals in rural areas.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study show individuals with Medicaid coverage are underrepresented in telehealth substance use disorder treatment services based on their overall treatment utilization. However, somewhat surprisingly, those in rural settings used telehealth services for substance use disorder treatment at rates proportional to their overall treatment utilization.
Results of the present study suggest that despite telehealth services alleviating potential barriers to treatment for some, those on Medicaid may have difficulty leveraging the increased access offered by telehealth. That is, telehealth removes the need to travel for treatment and rely on local providers, so other factors specific to Medicaid recipients – such as lower socioeconomic conditions – may be limiting its use. In addition, there is evidence that due to differing state policies, telehealth can be more difficult to access for Medicaid recipients than those with private insurance. Furthermore, telehealth often requires stable internet access, which low-income patients (i.e. those on Medicaid) are less likely to have. Recovery community centers – centrally-located community services that provide recovery supports and resources including internet access – may be helpful ways to address these barriers, though their utility specifically in Medicaid patients has not yet been examined. Relatedly, it is also possible that broadband internet infrastructure is not sufficient in rural areas – many of whom may also covered by Medicare – across the US to improve their access to telehealth.
Ultimately, the results of this study suggest that telehealth can be a viable treatment option for substance use disorder treatment. Although telehealth was disproportionately used by those with Medicare Advantage or commercially available insurance, increases in telehealth use were seen across all patients. To be clear, this study did not examine how effective the telehealth services were at treating substance use disorder (although other research suggests that telehealth for individual substance use disorder therapy in general is effective). Nevertheless, eliminating barriers to telehealth in the US could be a way to reduce the impact of substance use disorder on the population. Efforts to ensure access to telehealth services (e.g., access to affordable high-speed internet) should be expanded.
The present study offers very little information on the dataset and analysis procedures, making the results difficult to interpret. The authors state that they used the MedInsight Emerging Experience database which appears to be proprietary. The authors also declined to make their data publicly available as “The MedInsight Emerging Experience database used for this study is considered proprietary to Milliman MedInsight® and therefore cannot be shared”. It is unclear how these data were collected and how representative they are of the general US population.
Relatedly, the analytical tools/techniques used are not clear. The authors describe using the Milliman Health Cost Guidelines grouper which appears to be proprietary statistical software. No guidelines or examples were cited which could shed light on how exactly this software works or how it handles data. This lack of clarity calls into question the conclusions drawn from this research.
The present study does not differentiate treatment utilization by specific types of treatment. This is relevant as there is some evidence that different substance use disorder treatments are harder to deliver via telehealth services (e.g., group therapy).
Telehealth services increased substantially from 2019-2023, though Medicaid-covered individuals were underrepresented compared to their overall treatment utilization. The study also found that, unexpectedly, rural and urban individuals used telehealth services at proportional rates. It is possible that other barriers associated with lower socioeconomic status may be preventing full telehealth service utilization among Medicaid recipients. Relatedly, broadband internet infrastructure may not be sufficient in rural areas to improve their access to telehealth. Understanding what these barriers may be and how they can be overcome will be vital in expanding uptake of telehealth substance use disorder treatments.
For individuals and families seeking recovery: The present study suggests that individuals and families seeking recovery may find that telehealth is a viable treatment option for substance use disorder. Telehealth services can be useful in overcoming barriers to in-person care, like transportation challenges and limited local provider availability. Families should encourage their loved ones to explore telehealth options, especially if access to local in-person treatment programs is limited. However, those seeking recovery would do well to check insurance coverage. Although Medicaid covers some telehealth services, there may be barriers to utilizing telehealth for substance use disorder treatment. As telehealth continues to expand, being proactive about understanding available resources and advocating for access to high-quality, remote treatment services can help individuals and families navigate recovery more effectively.
For treatment professionals and treatment systems: The present study highlights the need for treatment professionals and those working in treatment systems to address disparities in telehealth utilization. While telehealth has expanded access to care, particularly during the COVID-19 pandemic, Medicaid recipients continue to use these services at disproportionately lower rates. Providers should work to ensure that telehealth options are accessible and effectively integrated into treatment plans, particularly for underserved populations. This may include assisting patients with navigating insurance coverage, providing technical support for telehealth access, and advocating for policy changes that expand Medicaid reimbursement for remote services. Additionally, treatment systems would do well to incorporate multilingual providers. By addressing these barriers, treatment professionals and systems can help maximize the potential of telehealth to improve substance use disorder treatment access and outcomes.
For scientists: The present study underscores the need for scientists to further research the effectiveness, accessibility, and equity of telehealth for substance use disorder treatment. Although, telehealth utilization has increased overall, this study suggests that Medicaid recipients face barriers to access. Future research should explore the specific factors limiting telehealth use among Medicaid beneficiaries, including policy restrictions, provider availability, and technological challenges (e.g., stable internet access). By addressing these gaps, researchers can inform policies and interventions that enhance telehealth’s role in expanding equitable access to substance use disorder treatment.
For policy makers: The present study suggests that policymakers may consider policies that improve equitable access to telehealth substance use disorder treatment for Medicaid recipients. Expanding Medicaid reimbursement for telehealth-based substance use disorder care could help address disparities. Policymakers could also invest in infrastructure to ensure individuals in rural and low-income areas have stable broadband internet so they can reliably access telehealth services. Additionally, policies should encourage provider participation in Medicaid telehealth programs by streamlining reimbursement processes and reducing administrative burdens. Finally, addressing regulatory barriers that limit telehealth access across state lines could enhance provider availability and improve care access and ultimately treatment success. By prioritizing these policy changes, lawmakers can strengthen the role of telehealth in expanding access to effective, evidence-based substance use disorder treatment.