Patients with alcohol use disorders embraced telemedicine during the COVID-19 pandemic
Physical distancing guidelines during the COVID-19 pandemic disrupted treatment for patients globally. However, it is unknown how the pandemic impacted outpatient treatment for alcohol use disorder. This study examined outpatient alcohol use disorder treatment during the first year of the COVID-19 pandemic with a particular focus on telemedicine visits.
The COVID-19 pandemic resulted in widespread restrictions in public activities. As a result, healthcare visits among patients dropped precipitously. These restrictions lead to healthcare professionals pivoting from providing traditional in-person visits to relying primarily on telemedicine. This transition allowed patients that had access to broadband internet to continue receiving needed care while also following COVID-19 physical distancing guidelines.
It is unclear how alcohol use disorder treatment may have been impacted by this transition to remote visits. Given that the pandemic was associated with a rise in alcohol use in the US, and many health care institutions scaled up telemedicine access, there may have been an increase in alcohol use disorder treatment engagement. Conversely, because there were reductions to in-person service access, and some do not have access to broadband internet or smartphones with a data plan needed to engage with telemedicine, there may have been a decrease in alcohol use disorder treatment engagement Additionally, specific groups within the alcohol use disorder patient population have experienced more barriers to care than others (e.g., women, and those living in rural areas), so the pandemic may have hit them especially hard. To empirically test these questions, this study examined outpatient alcohol use disorder treatment during the first year of COVID-19 with a particular focus on telemedicine visits.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed health insurance claims data from the OptumLabs Data Warehouse. Data were enrollees’ health care visits for services billed to the health plan for payment purposes (e.g., visit or procedure codes) across the US. These data included some demographic information on patients (e.g., age, assigned sex, and rurality). All data were de-identified (anonymous).
Participants in the current analysis (N=92,621) came from two cohorts of patients identified as having an alcohol use disorder (see below). The first cohort consisted of individuals from 2018-2020 (n=23,204) and the second was made up of patients from 2019-2021(n=23,445). The latter cohort was used to compare treatment utilization during the pandemic to treatment utilization pre-pandemic. Patients included in the analyses had to meet these criteria: 1) 18-64 years of age; 2) have continuous enrollment in medical, behavioral health, and pharmacy benefits for 2 years (i.e., 2018 and 2019 or 2019 and 2020); and 3) have a diagnosis of alcohol use disorder. Individuals were identified as having an alcohol use disorder if at least one of the following were present in their healthcare claims data within the first year of their cohort: a) 1+ hospitalizations where alcohol use disorder was the primary diagnosis, 2) 1+ emergency department visit where alcohol use disorder was in the first or second diagnostic field, or 3) at least 2 face-to-face visits (e.g., non-laboratory or imaging) on separate days in either outpatient, intensive outpatient, partial hospital, or residential care with a diagnosis of alcohol use disorder in the primary or secondary diagnosis field. As such, each of the 2018 and 2019 cohorts was made up of an established group of alcohol use disorder patients that sought care in that calendar year.
The main outcome of this study was use of any alcohol use disorder related outpatient treatment in the year following the index year. For the 2018 cohort, the study examined treatment in 2019 and for the 2019 cohort, the study examined treatment in 2020 (overlapping with onset of the COVID-19 pandemic). Such treatment was defined as any outpatient visit where an alcohol use disorder diagnosis was in the primary or secondary diagnostic field of the claim defined by using Current Procedural Terminology and Healthcare Common Procedure Coding System codes. Outpatient visit types were categorized as initial assessments, evaluation and management visits, or therapy (individual, group, or family) visits. In addition, this study examined usage of medications for alcohol use disorder. This included prescription fills, or facility administered administration for any of the following medications: acamprosate, naltrexone (also prescribed as a monthly injection known and marketed by the brand name “Vivitrol”), disulfiram (also known and marketed by the brand name “Antabuse”), or topiramate.
Participants in both cohorts were predominately identified as male (64.2% and 64.3% for the 2018 and 2019 cohorts respectively). The majority of patients lived in non-rural regions of the US (97.9% and 97.3% for the 2018 and 2019 cohorts respectively). Most participants were between the ages of 35-64 (71.8% and 68.1% for the 2018 and 2019 cohorts respectively). Roughly 25% of participants from each cohort were diagnosed with a cooccurring substance use disorder during the first year of their cohort.
WHAT DID THIS STUDY FIND?
Outpatient alcohol use disorder treatment during the pandemic initially declined, later rebounded.
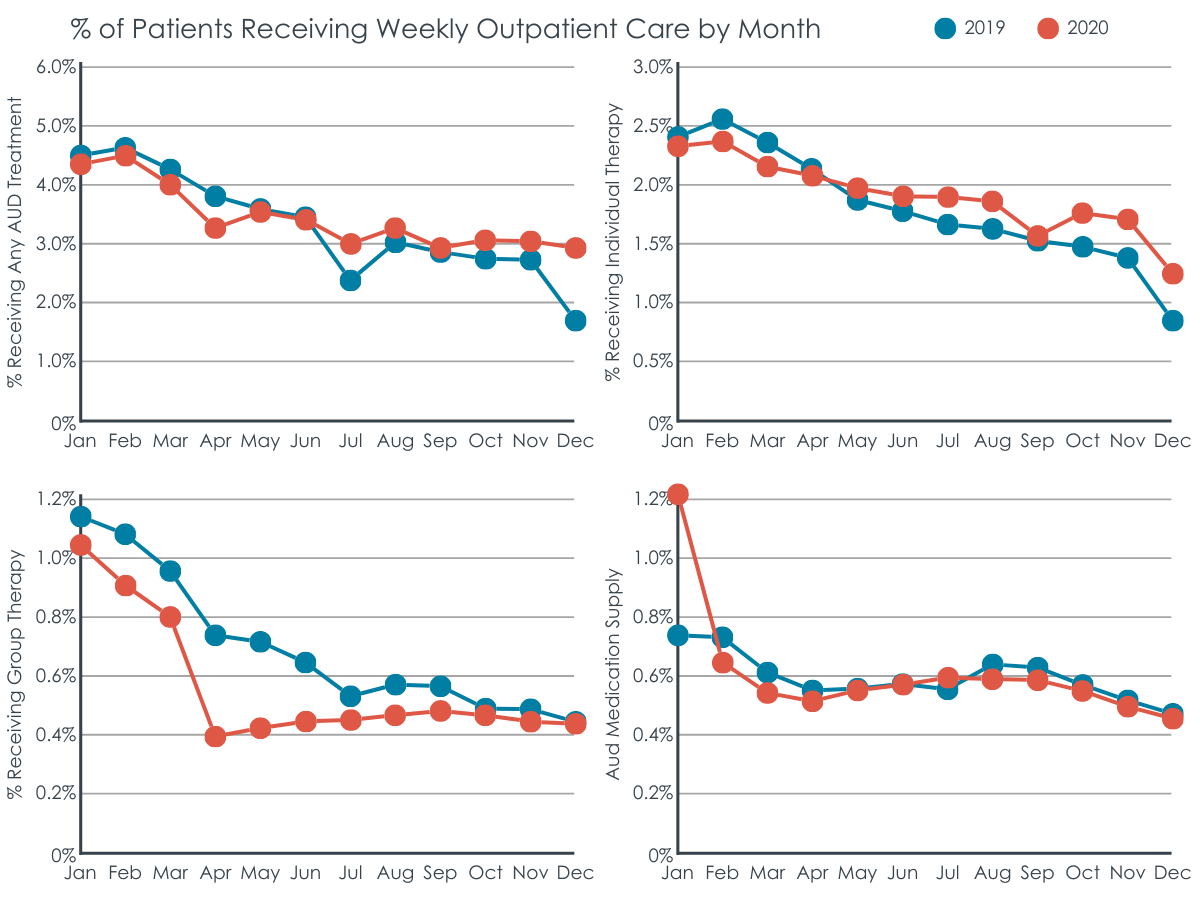
During the first weeks of the pandemic (mid-March through mid-April) there were 23% fewer outpatient visits for alcohol use disorder across all types of treatment relative to the same weeks in 2019. This began to change by early August 2020, however, when the number of people receiving outpatient treatment was nearly identical to the same period in 2019. The similar rates of treatment attendance remained when controlling for participant characteristics (e.g., age and gender assigned in the patient record). Use of medications for alcohol use disorder was the same before and during the pandemic.
After an initial dip in visits, the total number of outpatient visits for alcohol use disorder during the pandemic was roughly the same as before the pandemic.
Telemedicine use helped treatment rates overall keep up or increase during the pandemic, but not for group therapy.
Telemedicine use increased from 2% of alcohol use disorder outpatient visits before the COVID-19 pandemic, to 30% in the first week after the public health emergency declaration in March 2020, to a peak of 60% in May 2020. Following early July 2020, the percentage of individual therapy visits conducted via telemedicine ranged from 48.4% to 59.9% and for group therapy ranged from 39.4% to 51.6%.
Alcohol use disorder treatment attendance was stable, overall, between 2019 and 2020, a pattern generally similar across gender, rural vs. urban location, alcohol use disorder severity, and co-occurring mental health disorders. Of note, this stability was carried primarily by individual therapy attendance. For those with alcohol use disorder, 8.21% attended individual therapy in 2019 compared to 8.60% in 2020, a nonsignificant 5% increase. For group therapy, however, 2.19% attended treatment in 2019 and 1.67% in 2020, a significant 24% decline.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study demonstrate that despite an initial drop in visits, patients continued receiving outpatient treatment for alcohol use disorder during the COVID-19 pandemic, and for individual therapy even increased engagement, descriptively, compared to pre-pandemic rates. It is important to mention that these findings only tell us about rates of telemedicine engagement, not about treatment outcomes.
Results of the present study suggest that telemedicine may be better suited to individual therapy compared to group therapy for alcohol use disorder. The researchers found that although the number of outpatient visits for alcohol use disorder rivaled or outpaced pre-pandemic levels, the lion’s share of these visits consisted of individual therapy sessions. The number of group therapy sessions was lower during the pandemic relative to pre-pandemic. These trends were concurrent with a dramatic rise in the use of telemedicine technologies- suggesting conducting group therapy for alcohol use disorder via telemedicine technology may be more challenging than individual therapy.
Of note, this study also found that participant characteristics did not significantly impact receiving alcohol use disorder treatment during the pandemic. This is surprising as past research has shown that subpopulations within the larger group of alcohol use disorder patients face unique barriers to care. For instance, women with alcohol use disorders are less likely to access treatment than men and are more likely to report stigma as a barrier to accessing care. Similarly, those living in rural areas are less likely to access alcohol use disorder care relative to those in urban areas. It is not clear why the current study’s findings differ. One possible explanation for this divergence from past research may be that the sample was derived exclusively from those with consistent commercial health insurance for two years pre- or during the pandemic. The exclusion of those without such coverage (e.g., those on Medicaid) may have excluded populations who face barriers to alcohol use disorder treatment.
Ultimately, these results imply that telemedicine may be a viable alternative treatment modality for alcohol use disorder therapy if in-person options are not available. To be clear, this study did not examine outcomes during the pandemic and how they compared to pre-pandemic levels. Therefore, it is unknown how effective the telemedicine used by enrollees was (although other research suggests that telemedicine in general is effective). Nevertheless, eliminating barriers to telemedicine in the US could be an invaluable way to reduce the impact of alcohol use disorder in the population at large. Efforts to ensure access to telemedicine (e.g., access to affordable high-speed internet) should be expanded.
The present study does not tell us anything about the effectiveness of the treatment received. Although alcohol use disorder patients received outpatient treatment at similar rates to before the COVID-19 pandemic, the presented data do not tell us if patients fared as well during the pandemic as before. It is possible that despite receiving individual therapy via telemedicine, patients suffered relapses. This is plausible given other research demonstrating increases in drinking among US populations during the COVID-19 pandemic. It is beyond the scope of these data to elucidate how patients responded to treatment during the pandemic. Although some evidence suggests that telemedicine can be useful in treating addiction, it is important for researchers to investigate this further.
The sample used in this study was disproportionately from non-rural areas. This limits the study’s generalizability. For example, evidence suggests that those living in rural areas are less likely to access substance use disorder treatment (e.g., due to a lack of treatment providers). Given telemedicine was used more during the pandemic, it is possible that telemedicine could be a valuable tool in treating alcohol use disorder in rural parts of the US, though findings here did not examine that question.
Exclusive sampling of those who had continuous commercial healthcare coverage for 2 years is also a limitation of this research. People on Medicaid or who had a lapse in insurance coverage (e.g., due to unemployment) were not included in the sample. Furthermore, the study also did not include incarcerated people as far as can be determined. Given that alcohol use disorder is correlated with both socio-economic and carceral status these are noteworthy issues with the generalizability. It is possible that had the sample included such people, different results may have been obtained.
BOTTOM LINE
This study found that patients continued to receive treatment for alcohol use disorder despite challenges posed by the COVID-19 pandemic. Treatment was provided via the use of telemedicine, where rates of treatment seeking outpaced pre-pandemic levels by September 2020. This pattern, however, was accounted for by greater rates of individual therapy which was likely easier to deliver to individuals than across multiple patients in group therapy. Understanding how this shift in treatment modality may have impacted the trajectory of alcohol use disorder (e.g., relapse rates) for these patients is important. Given that barriers to treatment access predated COVID-19 and will persist well beyond the pandemic, understanding telemedicine and other innovative ways to engage individuals with alcohol use disorder in care will allow for more effective treatment beyond the COVID-19 pandemic.
For individuals and families seeking recovery: The present research suggests that telemedicine may be a viable pathway to alcohol use disorder treatment. Therefore, it is important for those seeking treatment for alcohol use disorders for themselves or others to be aware that remote therapy visits may be a helpful and, for many, accessible treatment option. This is especially important if distance to providers is a barrier to receiving care. Those seeking services should also be aware of what telemedicine services are covered by their insurance as this coverage varies across plans. For example, Medicare covers some telemedicine services.
For treatment professionals and treatment systems: Results suggest that telemedicine expansion could be a valuable tool for engaging individuals with alcohol use disorder. Although the study did not examine the effectiveness of telemedicine therapy sessions in treating alcohol use disorder, other research does suggest telemedicine can be useful in treating addiction. Those providing treatment to, and/or who work in healthcare system settings serving, people with alcohol use disorders, may consider expanding implementation of telemedicine services. However, reductions in group therapy with concurrent increases in individual therapy shown in this study may require more resources needed to provide care.
For scientists: Researchers may want to examine what factors impact the effectiveness of telemedicine therapy in treating alcohol use disorder. The scope of the present study does not allow us to infer how well patients fared after switching from in-person to virtual therapy sessions. In addition, it is unclear how a potential switch from group to individual-focused therapy may have impacted alcohol use disorder treatment outcomes. It is imperative that scientists further investigate these factors to inform recommendations on developing interventions and policies.
For policy makers: The present data suggests that telemedicine may be a useful approach to increase access and availability of alcohol use disorder treatment. In combination with data suggesting telemedicine-delivered substance use disorder treatment may be as effective as in-person treatment, policymakers may want to consider how they can help maintain or scale up adoption of telemedicine. The present data do not compare telemedicine treatment utilization across populations, so it is difficult to say what specific populations need help accessing care. Regardless policymakers may want to consider expanding access to high-speed internet across locales.
The COVID-19 pandemic resulted in widespread restrictions in public activities. As a result, healthcare visits among patients dropped precipitously. These restrictions lead to healthcare professionals pivoting from providing traditional in-person visits to relying primarily on telemedicine. This transition allowed patients that had access to broadband internet to continue receiving needed care while also following COVID-19 physical distancing guidelines.
It is unclear how alcohol use disorder treatment may have been impacted by this transition to remote visits. Given that the pandemic was associated with a rise in alcohol use in the US, and many health care institutions scaled up telemedicine access, there may have been an increase in alcohol use disorder treatment engagement. Conversely, because there were reductions to in-person service access, and some do not have access to broadband internet or smartphones with a data plan needed to engage with telemedicine, there may have been a decrease in alcohol use disorder treatment engagement Additionally, specific groups within the alcohol use disorder patient population have experienced more barriers to care than others (e.g., women, and those living in rural areas), so the pandemic may have hit them especially hard. To empirically test these questions, this study examined outpatient alcohol use disorder treatment during the first year of COVID-19 with a particular focus on telemedicine visits.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed health insurance claims data from the OptumLabs Data Warehouse. Data were enrollees’ health care visits for services billed to the health plan for payment purposes (e.g., visit or procedure codes) across the US. These data included some demographic information on patients (e.g., age, assigned sex, and rurality). All data were de-identified (anonymous).
Participants in the current analysis (N=92,621) came from two cohorts of patients identified as having an alcohol use disorder (see below). The first cohort consisted of individuals from 2018-2020 (n=23,204) and the second was made up of patients from 2019-2021(n=23,445). The latter cohort was used to compare treatment utilization during the pandemic to treatment utilization pre-pandemic. Patients included in the analyses had to meet these criteria: 1) 18-64 years of age; 2) have continuous enrollment in medical, behavioral health, and pharmacy benefits for 2 years (i.e., 2018 and 2019 or 2019 and 2020); and 3) have a diagnosis of alcohol use disorder. Individuals were identified as having an alcohol use disorder if at least one of the following were present in their healthcare claims data within the first year of their cohort: a) 1+ hospitalizations where alcohol use disorder was the primary diagnosis, 2) 1+ emergency department visit where alcohol use disorder was in the first or second diagnostic field, or 3) at least 2 face-to-face visits (e.g., non-laboratory or imaging) on separate days in either outpatient, intensive outpatient, partial hospital, or residential care with a diagnosis of alcohol use disorder in the primary or secondary diagnosis field. As such, each of the 2018 and 2019 cohorts was made up of an established group of alcohol use disorder patients that sought care in that calendar year.
The main outcome of this study was use of any alcohol use disorder related outpatient treatment in the year following the index year. For the 2018 cohort, the study examined treatment in 2019 and for the 2019 cohort, the study examined treatment in 2020 (overlapping with onset of the COVID-19 pandemic). Such treatment was defined as any outpatient visit where an alcohol use disorder diagnosis was in the primary or secondary diagnostic field of the claim defined by using Current Procedural Terminology and Healthcare Common Procedure Coding System codes. Outpatient visit types were categorized as initial assessments, evaluation and management visits, or therapy (individual, group, or family) visits. In addition, this study examined usage of medications for alcohol use disorder. This included prescription fills, or facility administered administration for any of the following medications: acamprosate, naltrexone (also prescribed as a monthly injection known and marketed by the brand name “Vivitrol”), disulfiram (also known and marketed by the brand name “Antabuse”), or topiramate.
Participants in both cohorts were predominately identified as male (64.2% and 64.3% for the 2018 and 2019 cohorts respectively). The majority of patients lived in non-rural regions of the US (97.9% and 97.3% for the 2018 and 2019 cohorts respectively). Most participants were between the ages of 35-64 (71.8% and 68.1% for the 2018 and 2019 cohorts respectively). Roughly 25% of participants from each cohort were diagnosed with a cooccurring substance use disorder during the first year of their cohort.
WHAT DID THIS STUDY FIND?
Outpatient alcohol use disorder treatment during the pandemic initially declined, later rebounded.
During the first weeks of the pandemic (mid-March through mid-April) there were 23% fewer outpatient visits for alcohol use disorder across all types of treatment relative to the same weeks in 2019. This began to change by early August 2020, however, when the number of people receiving outpatient treatment was nearly identical to the same period in 2019. The similar rates of treatment attendance remained when controlling for participant characteristics (e.g., age and gender assigned in the patient record). Use of medications for alcohol use disorder was the same before and during the pandemic.
After an initial dip in visits, the total number of outpatient visits for alcohol use disorder during the pandemic was roughly the same as before the pandemic.
Telemedicine use helped treatment rates overall keep up or increase during the pandemic, but not for group therapy.
Telemedicine use increased from 2% of alcohol use disorder outpatient visits before the COVID-19 pandemic, to 30% in the first week after the public health emergency declaration in March 2020, to a peak of 60% in May 2020. Following early July 2020, the percentage of individual therapy visits conducted via telemedicine ranged from 48.4% to 59.9% and for group therapy ranged from 39.4% to 51.6%.
Alcohol use disorder treatment attendance was stable, overall, between 2019 and 2020, a pattern generally similar across gender, rural vs. urban location, alcohol use disorder severity, and co-occurring mental health disorders. Of note, this stability was carried primarily by individual therapy attendance. For those with alcohol use disorder, 8.21% attended individual therapy in 2019 compared to 8.60% in 2020, a nonsignificant 5% increase. For group therapy, however, 2.19% attended treatment in 2019 and 1.67% in 2020, a significant 24% decline.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study demonstrate that despite an initial drop in visits, patients continued receiving outpatient treatment for alcohol use disorder during the COVID-19 pandemic, and for individual therapy even increased engagement, descriptively, compared to pre-pandemic rates. It is important to mention that these findings only tell us about rates of telemedicine engagement, not about treatment outcomes.
Results of the present study suggest that telemedicine may be better suited to individual therapy compared to group therapy for alcohol use disorder. The researchers found that although the number of outpatient visits for alcohol use disorder rivaled or outpaced pre-pandemic levels, the lion’s share of these visits consisted of individual therapy sessions. The number of group therapy sessions was lower during the pandemic relative to pre-pandemic. These trends were concurrent with a dramatic rise in the use of telemedicine technologies- suggesting conducting group therapy for alcohol use disorder via telemedicine technology may be more challenging than individual therapy.
Of note, this study also found that participant characteristics did not significantly impact receiving alcohol use disorder treatment during the pandemic. This is surprising as past research has shown that subpopulations within the larger group of alcohol use disorder patients face unique barriers to care. For instance, women with alcohol use disorders are less likely to access treatment than men and are more likely to report stigma as a barrier to accessing care. Similarly, those living in rural areas are less likely to access alcohol use disorder care relative to those in urban areas. It is not clear why the current study’s findings differ. One possible explanation for this divergence from past research may be that the sample was derived exclusively from those with consistent commercial health insurance for two years pre- or during the pandemic. The exclusion of those without such coverage (e.g., those on Medicaid) may have excluded populations who face barriers to alcohol use disorder treatment.
Ultimately, these results imply that telemedicine may be a viable alternative treatment modality for alcohol use disorder therapy if in-person options are not available. To be clear, this study did not examine outcomes during the pandemic and how they compared to pre-pandemic levels. Therefore, it is unknown how effective the telemedicine used by enrollees was (although other research suggests that telemedicine in general is effective). Nevertheless, eliminating barriers to telemedicine in the US could be an invaluable way to reduce the impact of alcohol use disorder in the population at large. Efforts to ensure access to telemedicine (e.g., access to affordable high-speed internet) should be expanded.
The present study does not tell us anything about the effectiveness of the treatment received. Although alcohol use disorder patients received outpatient treatment at similar rates to before the COVID-19 pandemic, the presented data do not tell us if patients fared as well during the pandemic as before. It is possible that despite receiving individual therapy via telemedicine, patients suffered relapses. This is plausible given other research demonstrating increases in drinking among US populations during the COVID-19 pandemic. It is beyond the scope of these data to elucidate how patients responded to treatment during the pandemic. Although some evidence suggests that telemedicine can be useful in treating addiction, it is important for researchers to investigate this further.
The sample used in this study was disproportionately from non-rural areas. This limits the study’s generalizability. For example, evidence suggests that those living in rural areas are less likely to access substance use disorder treatment (e.g., due to a lack of treatment providers). Given telemedicine was used more during the pandemic, it is possible that telemedicine could be a valuable tool in treating alcohol use disorder in rural parts of the US, though findings here did not examine that question.
Exclusive sampling of those who had continuous commercial healthcare coverage for 2 years is also a limitation of this research. People on Medicaid or who had a lapse in insurance coverage (e.g., due to unemployment) were not included in the sample. Furthermore, the study also did not include incarcerated people as far as can be determined. Given that alcohol use disorder is correlated with both socio-economic and carceral status these are noteworthy issues with the generalizability. It is possible that had the sample included such people, different results may have been obtained.
BOTTOM LINE
This study found that patients continued to receive treatment for alcohol use disorder despite challenges posed by the COVID-19 pandemic. Treatment was provided via the use of telemedicine, where rates of treatment seeking outpaced pre-pandemic levels by September 2020. This pattern, however, was accounted for by greater rates of individual therapy which was likely easier to deliver to individuals than across multiple patients in group therapy. Understanding how this shift in treatment modality may have impacted the trajectory of alcohol use disorder (e.g., relapse rates) for these patients is important. Given that barriers to treatment access predated COVID-19 and will persist well beyond the pandemic, understanding telemedicine and other innovative ways to engage individuals with alcohol use disorder in care will allow for more effective treatment beyond the COVID-19 pandemic.
For individuals and families seeking recovery: The present research suggests that telemedicine may be a viable pathway to alcohol use disorder treatment. Therefore, it is important for those seeking treatment for alcohol use disorders for themselves or others to be aware that remote therapy visits may be a helpful and, for many, accessible treatment option. This is especially important if distance to providers is a barrier to receiving care. Those seeking services should also be aware of what telemedicine services are covered by their insurance as this coverage varies across plans. For example, Medicare covers some telemedicine services.
For treatment professionals and treatment systems: Results suggest that telemedicine expansion could be a valuable tool for engaging individuals with alcohol use disorder. Although the study did not examine the effectiveness of telemedicine therapy sessions in treating alcohol use disorder, other research does suggest telemedicine can be useful in treating addiction. Those providing treatment to, and/or who work in healthcare system settings serving, people with alcohol use disorders, may consider expanding implementation of telemedicine services. However, reductions in group therapy with concurrent increases in individual therapy shown in this study may require more resources needed to provide care.
For scientists: Researchers may want to examine what factors impact the effectiveness of telemedicine therapy in treating alcohol use disorder. The scope of the present study does not allow us to infer how well patients fared after switching from in-person to virtual therapy sessions. In addition, it is unclear how a potential switch from group to individual-focused therapy may have impacted alcohol use disorder treatment outcomes. It is imperative that scientists further investigate these factors to inform recommendations on developing interventions and policies.
For policy makers: The present data suggests that telemedicine may be a useful approach to increase access and availability of alcohol use disorder treatment. In combination with data suggesting telemedicine-delivered substance use disorder treatment may be as effective as in-person treatment, policymakers may want to consider how they can help maintain or scale up adoption of telemedicine. The present data do not compare telemedicine treatment utilization across populations, so it is difficult to say what specific populations need help accessing care. Regardless policymakers may want to consider expanding access to high-speed internet across locales.
The COVID-19 pandemic resulted in widespread restrictions in public activities. As a result, healthcare visits among patients dropped precipitously. These restrictions lead to healthcare professionals pivoting from providing traditional in-person visits to relying primarily on telemedicine. This transition allowed patients that had access to broadband internet to continue receiving needed care while also following COVID-19 physical distancing guidelines.
It is unclear how alcohol use disorder treatment may have been impacted by this transition to remote visits. Given that the pandemic was associated with a rise in alcohol use in the US, and many health care institutions scaled up telemedicine access, there may have been an increase in alcohol use disorder treatment engagement. Conversely, because there were reductions to in-person service access, and some do not have access to broadband internet or smartphones with a data plan needed to engage with telemedicine, there may have been a decrease in alcohol use disorder treatment engagement Additionally, specific groups within the alcohol use disorder patient population have experienced more barriers to care than others (e.g., women, and those living in rural areas), so the pandemic may have hit them especially hard. To empirically test these questions, this study examined outpatient alcohol use disorder treatment during the first year of COVID-19 with a particular focus on telemedicine visits.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed health insurance claims data from the OptumLabs Data Warehouse. Data were enrollees’ health care visits for services billed to the health plan for payment purposes (e.g., visit or procedure codes) across the US. These data included some demographic information on patients (e.g., age, assigned sex, and rurality). All data were de-identified (anonymous).
Participants in the current analysis (N=92,621) came from two cohorts of patients identified as having an alcohol use disorder (see below). The first cohort consisted of individuals from 2018-2020 (n=23,204) and the second was made up of patients from 2019-2021(n=23,445). The latter cohort was used to compare treatment utilization during the pandemic to treatment utilization pre-pandemic. Patients included in the analyses had to meet these criteria: 1) 18-64 years of age; 2) have continuous enrollment in medical, behavioral health, and pharmacy benefits for 2 years (i.e., 2018 and 2019 or 2019 and 2020); and 3) have a diagnosis of alcohol use disorder. Individuals were identified as having an alcohol use disorder if at least one of the following were present in their healthcare claims data within the first year of their cohort: a) 1+ hospitalizations where alcohol use disorder was the primary diagnosis, 2) 1+ emergency department visit where alcohol use disorder was in the first or second diagnostic field, or 3) at least 2 face-to-face visits (e.g., non-laboratory or imaging) on separate days in either outpatient, intensive outpatient, partial hospital, or residential care with a diagnosis of alcohol use disorder in the primary or secondary diagnosis field. As such, each of the 2018 and 2019 cohorts was made up of an established group of alcohol use disorder patients that sought care in that calendar year.
The main outcome of this study was use of any alcohol use disorder related outpatient treatment in the year following the index year. For the 2018 cohort, the study examined treatment in 2019 and for the 2019 cohort, the study examined treatment in 2020 (overlapping with onset of the COVID-19 pandemic). Such treatment was defined as any outpatient visit where an alcohol use disorder diagnosis was in the primary or secondary diagnostic field of the claim defined by using Current Procedural Terminology and Healthcare Common Procedure Coding System codes. Outpatient visit types were categorized as initial assessments, evaluation and management visits, or therapy (individual, group, or family) visits. In addition, this study examined usage of medications for alcohol use disorder. This included prescription fills, or facility administered administration for any of the following medications: acamprosate, naltrexone (also prescribed as a monthly injection known and marketed by the brand name “Vivitrol”), disulfiram (also known and marketed by the brand name “Antabuse”), or topiramate.
Participants in both cohorts were predominately identified as male (64.2% and 64.3% for the 2018 and 2019 cohorts respectively). The majority of patients lived in non-rural regions of the US (97.9% and 97.3% for the 2018 and 2019 cohorts respectively). Most participants were between the ages of 35-64 (71.8% and 68.1% for the 2018 and 2019 cohorts respectively). Roughly 25% of participants from each cohort were diagnosed with a cooccurring substance use disorder during the first year of their cohort.
WHAT DID THIS STUDY FIND?
Outpatient alcohol use disorder treatment during the pandemic initially declined, later rebounded.
During the first weeks of the pandemic (mid-March through mid-April) there were 23% fewer outpatient visits for alcohol use disorder across all types of treatment relative to the same weeks in 2019. This began to change by early August 2020, however, when the number of people receiving outpatient treatment was nearly identical to the same period in 2019. The similar rates of treatment attendance remained when controlling for participant characteristics (e.g., age and gender assigned in the patient record). Use of medications for alcohol use disorder was the same before and during the pandemic.
After an initial dip in visits, the total number of outpatient visits for alcohol use disorder during the pandemic was roughly the same as before the pandemic.
Telemedicine use helped treatment rates overall keep up or increase during the pandemic, but not for group therapy.
Telemedicine use increased from 2% of alcohol use disorder outpatient visits before the COVID-19 pandemic, to 30% in the first week after the public health emergency declaration in March 2020, to a peak of 60% in May 2020. Following early July 2020, the percentage of individual therapy visits conducted via telemedicine ranged from 48.4% to 59.9% and for group therapy ranged from 39.4% to 51.6%.
Alcohol use disorder treatment attendance was stable, overall, between 2019 and 2020, a pattern generally similar across gender, rural vs. urban location, alcohol use disorder severity, and co-occurring mental health disorders. Of note, this stability was carried primarily by individual therapy attendance. For those with alcohol use disorder, 8.21% attended individual therapy in 2019 compared to 8.60% in 2020, a nonsignificant 5% increase. For group therapy, however, 2.19% attended treatment in 2019 and 1.67% in 2020, a significant 24% decline.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study demonstrate that despite an initial drop in visits, patients continued receiving outpatient treatment for alcohol use disorder during the COVID-19 pandemic, and for individual therapy even increased engagement, descriptively, compared to pre-pandemic rates. It is important to mention that these findings only tell us about rates of telemedicine engagement, not about treatment outcomes.
Results of the present study suggest that telemedicine may be better suited to individual therapy compared to group therapy for alcohol use disorder. The researchers found that although the number of outpatient visits for alcohol use disorder rivaled or outpaced pre-pandemic levels, the lion’s share of these visits consisted of individual therapy sessions. The number of group therapy sessions was lower during the pandemic relative to pre-pandemic. These trends were concurrent with a dramatic rise in the use of telemedicine technologies- suggesting conducting group therapy for alcohol use disorder via telemedicine technology may be more challenging than individual therapy.
Of note, this study also found that participant characteristics did not significantly impact receiving alcohol use disorder treatment during the pandemic. This is surprising as past research has shown that subpopulations within the larger group of alcohol use disorder patients face unique barriers to care. For instance, women with alcohol use disorders are less likely to access treatment than men and are more likely to report stigma as a barrier to accessing care. Similarly, those living in rural areas are less likely to access alcohol use disorder care relative to those in urban areas. It is not clear why the current study’s findings differ. One possible explanation for this divergence from past research may be that the sample was derived exclusively from those with consistent commercial health insurance for two years pre- or during the pandemic. The exclusion of those without such coverage (e.g., those on Medicaid) may have excluded populations who face barriers to alcohol use disorder treatment.
Ultimately, these results imply that telemedicine may be a viable alternative treatment modality for alcohol use disorder therapy if in-person options are not available. To be clear, this study did not examine outcomes during the pandemic and how they compared to pre-pandemic levels. Therefore, it is unknown how effective the telemedicine used by enrollees was (although other research suggests that telemedicine in general is effective). Nevertheless, eliminating barriers to telemedicine in the US could be an invaluable way to reduce the impact of alcohol use disorder in the population at large. Efforts to ensure access to telemedicine (e.g., access to affordable high-speed internet) should be expanded.
The present study does not tell us anything about the effectiveness of the treatment received. Although alcohol use disorder patients received outpatient treatment at similar rates to before the COVID-19 pandemic, the presented data do not tell us if patients fared as well during the pandemic as before. It is possible that despite receiving individual therapy via telemedicine, patients suffered relapses. This is plausible given other research demonstrating increases in drinking among US populations during the COVID-19 pandemic. It is beyond the scope of these data to elucidate how patients responded to treatment during the pandemic. Although some evidence suggests that telemedicine can be useful in treating addiction, it is important for researchers to investigate this further.
The sample used in this study was disproportionately from non-rural areas. This limits the study’s generalizability. For example, evidence suggests that those living in rural areas are less likely to access substance use disorder treatment (e.g., due to a lack of treatment providers). Given telemedicine was used more during the pandemic, it is possible that telemedicine could be a valuable tool in treating alcohol use disorder in rural parts of the US, though findings here did not examine that question.
Exclusive sampling of those who had continuous commercial healthcare coverage for 2 years is also a limitation of this research. People on Medicaid or who had a lapse in insurance coverage (e.g., due to unemployment) were not included in the sample. Furthermore, the study also did not include incarcerated people as far as can be determined. Given that alcohol use disorder is correlated with both socio-economic and carceral status these are noteworthy issues with the generalizability. It is possible that had the sample included such people, different results may have been obtained.
BOTTOM LINE
This study found that patients continued to receive treatment for alcohol use disorder despite challenges posed by the COVID-19 pandemic. Treatment was provided via the use of telemedicine, where rates of treatment seeking outpaced pre-pandemic levels by September 2020. This pattern, however, was accounted for by greater rates of individual therapy which was likely easier to deliver to individuals than across multiple patients in group therapy. Understanding how this shift in treatment modality may have impacted the trajectory of alcohol use disorder (e.g., relapse rates) for these patients is important. Given that barriers to treatment access predated COVID-19 and will persist well beyond the pandemic, understanding telemedicine and other innovative ways to engage individuals with alcohol use disorder in care will allow for more effective treatment beyond the COVID-19 pandemic.
For individuals and families seeking recovery: The present research suggests that telemedicine may be a viable pathway to alcohol use disorder treatment. Therefore, it is important for those seeking treatment for alcohol use disorders for themselves or others to be aware that remote therapy visits may be a helpful and, for many, accessible treatment option. This is especially important if distance to providers is a barrier to receiving care. Those seeking services should also be aware of what telemedicine services are covered by their insurance as this coverage varies across plans. For example, Medicare covers some telemedicine services.
For treatment professionals and treatment systems: Results suggest that telemedicine expansion could be a valuable tool for engaging individuals with alcohol use disorder. Although the study did not examine the effectiveness of telemedicine therapy sessions in treating alcohol use disorder, other research does suggest telemedicine can be useful in treating addiction. Those providing treatment to, and/or who work in healthcare system settings serving, people with alcohol use disorders, may consider expanding implementation of telemedicine services. However, reductions in group therapy with concurrent increases in individual therapy shown in this study may require more resources needed to provide care.
For scientists: Researchers may want to examine what factors impact the effectiveness of telemedicine therapy in treating alcohol use disorder. The scope of the present study does not allow us to infer how well patients fared after switching from in-person to virtual therapy sessions. In addition, it is unclear how a potential switch from group to individual-focused therapy may have impacted alcohol use disorder treatment outcomes. It is imperative that scientists further investigate these factors to inform recommendations on developing interventions and policies.
For policy makers: The present data suggests that telemedicine may be a useful approach to increase access and availability of alcohol use disorder treatment. In combination with data suggesting telemedicine-delivered substance use disorder treatment may be as effective as in-person treatment, policymakers may want to consider how they can help maintain or scale up adoption of telemedicine. The present data do not compare telemedicine treatment utilization across populations, so it is difficult to say what specific populations need help accessing care. Regardless policymakers may want to consider expanding access to high-speed internet across locales.