Weekly clinical support and guidance improves adherence to web-based alcohol treatment, but not outcomes
Web-based cognitive behavioral therapy for alcohol use disorder is a cost-efficient approach to improving outcomes. Effects, however, remain modest. What if there were simple ways to further boost outcomes? This study examined whether adding a pre-treatment assessment interview or ongoing clinical guidance to an existing web-based cognitive behavior therapy improved drinking outcomes.
Given the modest effects of these interventions, clinical researchers are always looking for ways to enhance impact. There could be some simple ways to build on these outcomes and boost results using brief add-ons. There are several potential add-ons that research suggests might enhance web-based CBT.
One idea is that a pre-treatment assessment interview could improve outcomes by putting participants in a self-reflective mode that has the potential to increase their motivation for engagement in the intervention. For example, pre-treatment assessments that ask a participant to report on their current drinking behaviors, could encourage participants to begin to consider their drinking and whether it is something they might want to change. This is a well-known concept, called Assessment Reactivity, and it has been studied in a variety of disciplines including alcohol research. Research has shown that more frequent and comprehensive assessments tend to show the greatest boost in positive outcomes among patients treated for alcohol use disorders.
One other potentially helpful add-on, that might require more resources than a pre-treatment assessment, would be to include a clinical guidance component. In this component, the participant would meet with a clinician in addition to completing the online intervention components. Adding this aspect to an online intervention could help personalize the experience for the patient, increase their motivation, and increase their accountability or further engagement with clinical care. Yet, previous research has demonstrated mixed results on whether adding clinical guidance makes a big difference in participant outcomes.
In this study, the researchers tested whether adding a pre-treatment assessment interview and/or guidance to an existing web-based cognitive behavior therapy (CBT) improved participant outcomes and reduced alcohol use.
HOW WAS THIS STUDY CONDUCTED?
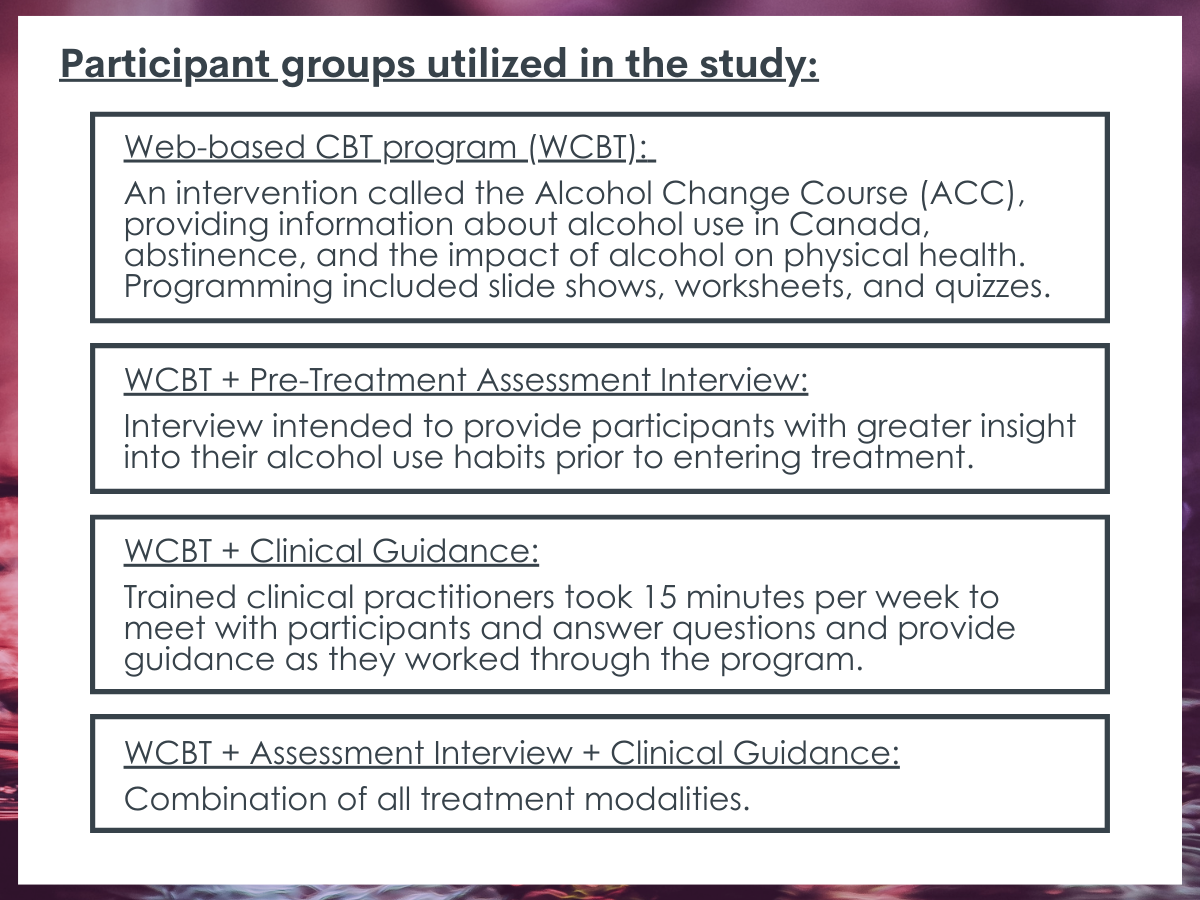
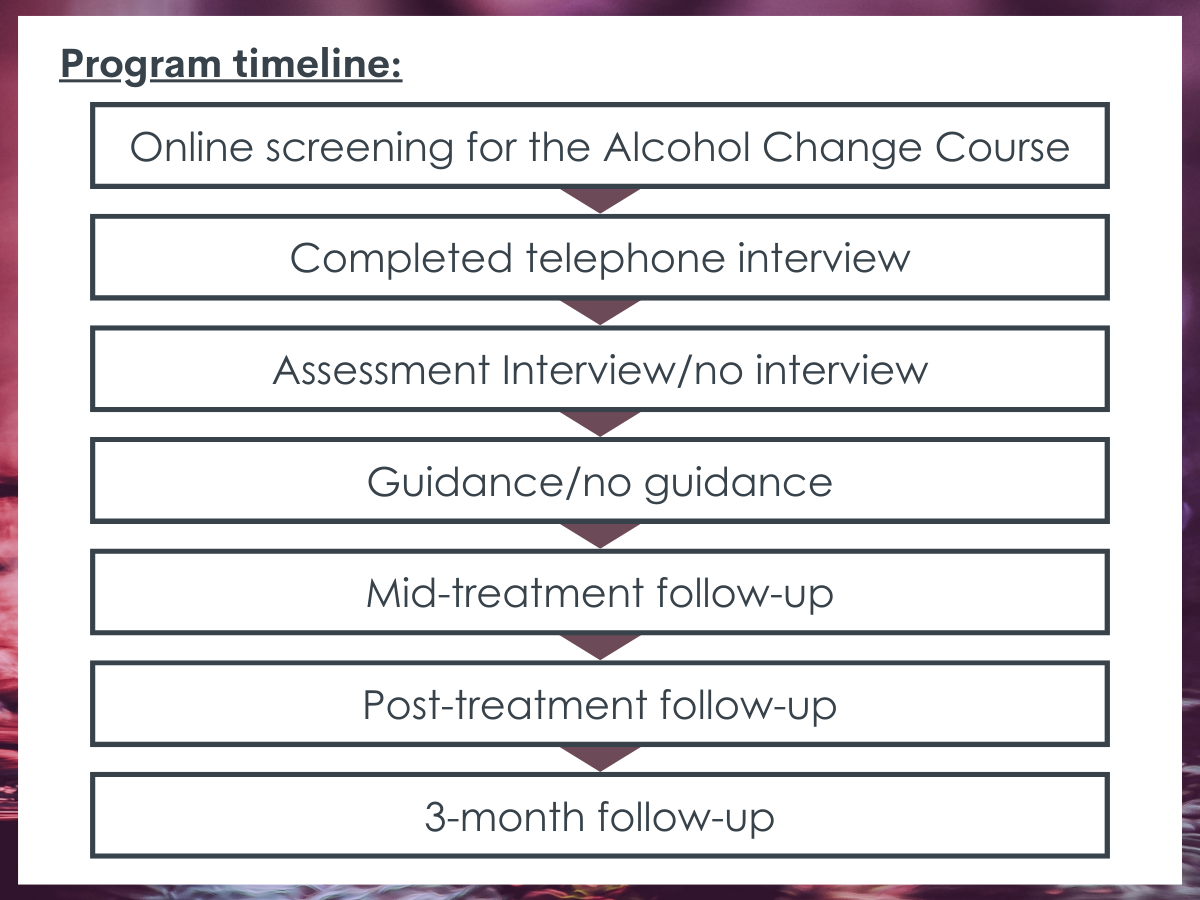
This was a 2X2 factorial randomized controlled trial, where participants were randomized to one of 4 groups: (1) 8-week web-based CBT program, which the researchers called “internet-delivered CBT, or IBCT”; (2) 8-week web-based CBT program + pre-treatment assessment interview; (3) 8-week web-based CBT program + clinical guidance; or (4) 8-week web-based CBT program + pre-treatment assessment interview and clinical guidance. A “2X2” design means there were two independent variables each with two different groups – assessment (yes or no) and guidance (yes or no). To be eligible for the study, participants had to be adults who scored 8 or higher on the Alcohol Use Disorders Identification Test (AUDIT) and who consumed 14 or more drinks in the previous week (a standard drink in Canada is 13.45 grams of pure alcohol or about 12 oz. of beer with 5% ABV).
Participants who were assigned to the pre-treatment assessment interview condition were asked to complete the alcohol use disorder module of the Structured Clinical Interview Diagnostic Statistical Manual 5 – Research Version with a member of the research team. On average the screening calls that included this aspect of the study lasted 36 minutes while those without lasted 18.4 minutes, suggesting the assessment interview was about 15-20 minutes long.
Participants who were assigned to the clinical guidance condition received messages and interaction primarily from clinicians over time through the treatment platform. These interactions lasted about 15 minutes/week and messages included answering participants’ questions, trying to reinforce module completion, and boosting participant’s motivation.
In addition to the different components of each treatment condition, as part of the study, all participants received weekly emails about the next week’s content and were asked to complete reflection questions on challenges they might have had with the activities and lessons learned, and to complete a brief questionnaire assessing depression, anxiety, and suicidal ideation (Patient Health Questionnaire-4 and PHQ-9). They were also asked the following two questions about past week alcohol use: (1) How many drinks have you had in the past week; and (2) Over how many days did you consume these drinks?
The primary outcomes, measured at 3 months were the number of drinks consumed and the number of heavy drinking days during the previous week (defined as ≥ 4 drinks per day for women and ≥ 5 drinks per day for men). The secondary outcomes included scores from the Alcohol Use Disorder Identification Test, alcohol craving (Penn Alcohol scale), Confidence in the ability to not drink/drink less (Brief situational confidence questionnaire), Daily functioning (Sheehan disability scale), Depression (PHQ), Anxiety (GAD-7), motivation to change (Readiness to change questionnaire, treatment version), and treatment credibility (Credibility/Expectancy questionnaire). Adherence to treatment was also captured through recording module completion. They also captured the number of logins to the website, number of modules accessed, and time in days between first and last using the website.
Of the sample of 270 adult participants, most were White (93%), had further formal education after completing high school (85.6%), employed (69%), female (67%), and married (63%), and they were 46.5 years old on average. Participants, on average, reported consuming 41.7 (SD = 24.8) drinks and had 4.5 (SD = 2.1) heavy drinking days in the preceding week. The average score on the AUDIT was 24.0 (SD = 5.8), indicating high average likelihood of alcohol use disorder across the sample.
WHAT DID THIS STUDY FIND?
Participants completed most of the intervention with an advantage for those getting the clinical guidance.
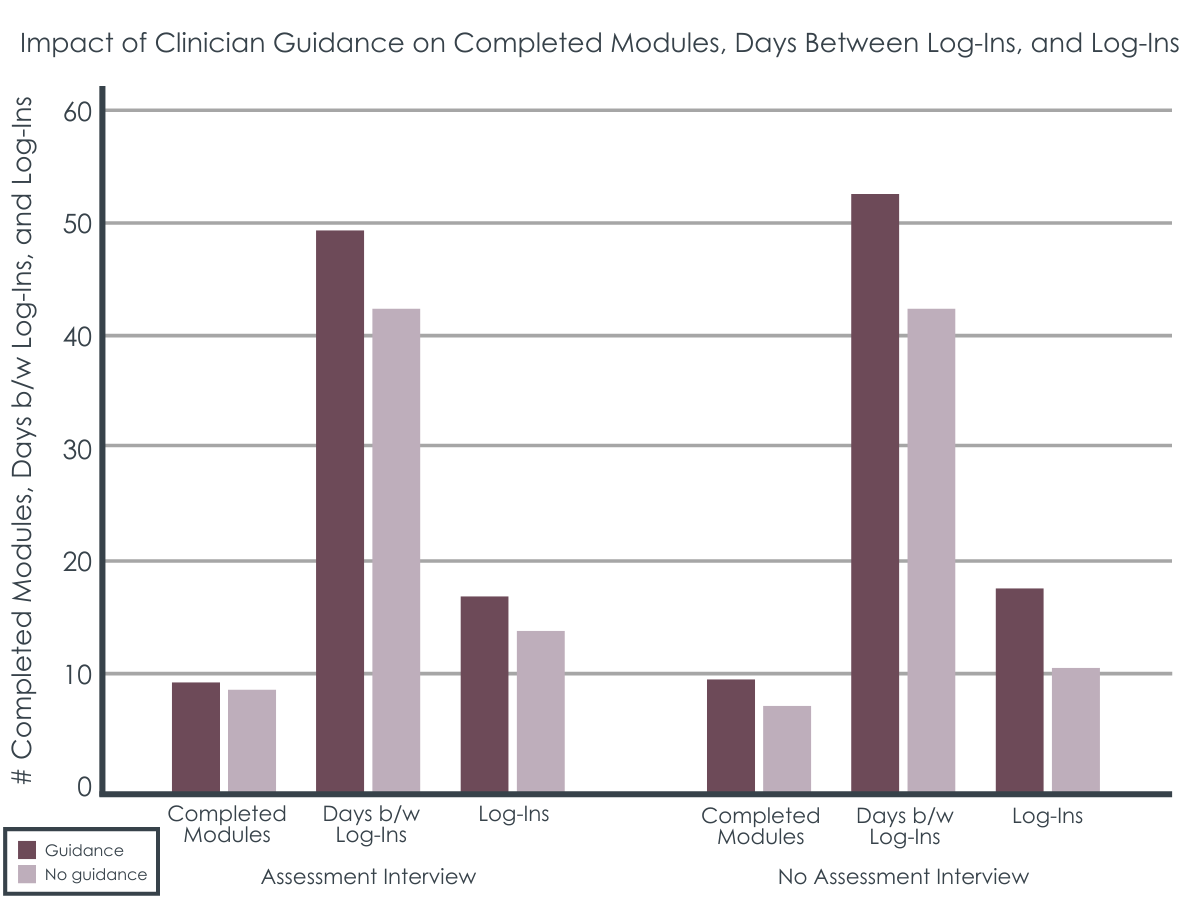
On average, participants across all four conditions completed 8 out of the 12 modules of the online treatment (67%). But participants who received the clinician guidance completed more modules, used the program for a longer time, and had more logins than the other groups.
There were no group differences on drinking outcomes.
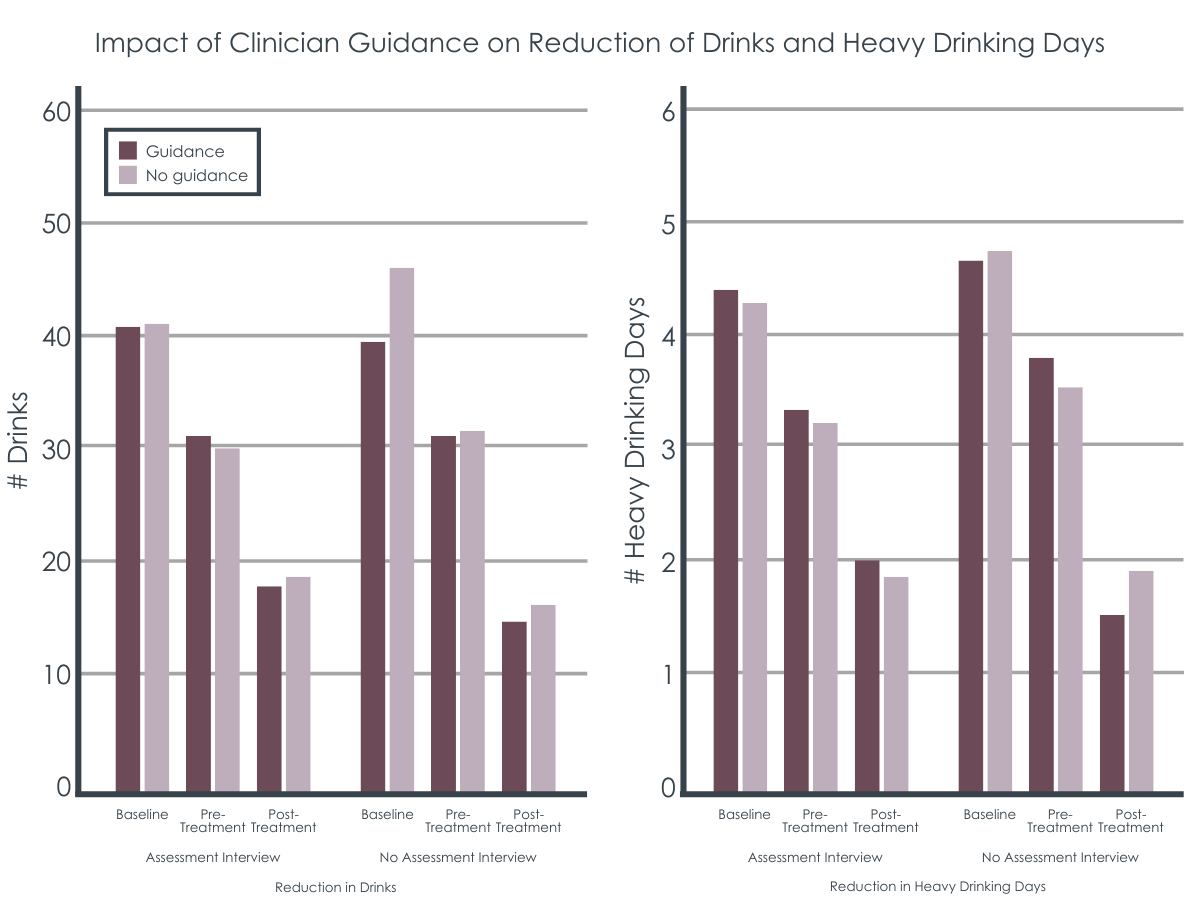
Participants in each of the four intervention groups improved by about the same amount reducing their number of drinks and number of heavy drinking days. That is, participants halved both their number of drinks and number of heavy drinking days from screening to post-treatment and these findings were maintained at 3 months. Importantly, although all groups demonstrated improvement, this also means that the add-ons of assessment or guidance did not improve drinking outcomes beyond the web-based CBT by itself, as researchers hypothesized.
Similarly, all participants improved to roughly the same degree from pre-treatment to 3 months on the secondary outcomes of alcohol use disorder identification scores, alcohol craving, situational confidence, daily functioning, depression, and anxiety. Additionally, secondary outcomes related to the treatment experience including treatment credibility, satisfaction, or negative effects did not differ between the groups.
Pre-treatment shifts in motivation may be responsible for lack of group differences.
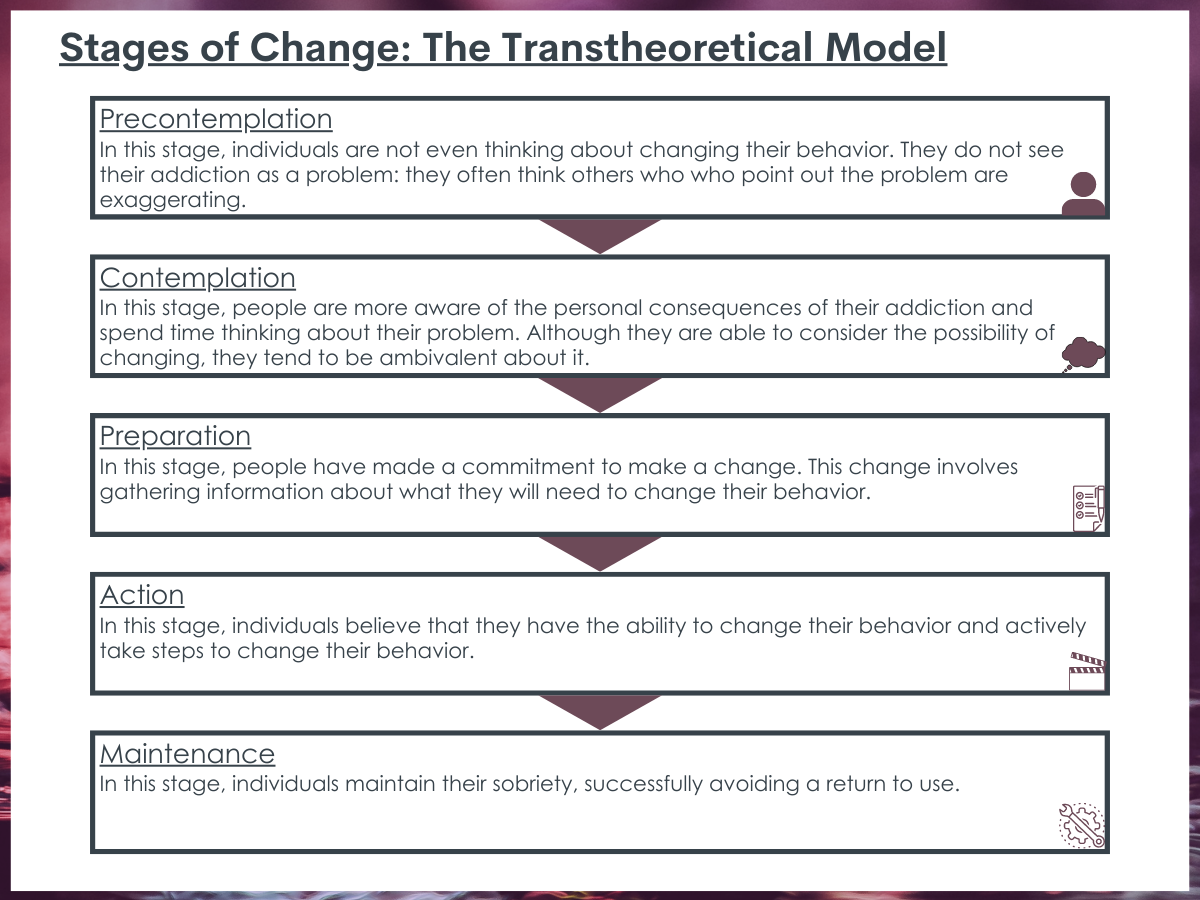
Participants demonstrated motivational change from the time of pre-screening to beginning treatment. Using the readiness to change scale – which goes from thinking about change (pre-contemplation) to actually making change – nearly all participants moved from a pre-contemplation stage of change to the action stage of readiness to change at pre-treatment. In addition, the initial reductions in drinking alcohol during the pre-treatment phase were strongly correlated with changes during treatment: the correlations indicated a relationship of 0.52 for drinking amount and 0.46 for heavy drinking days.
Yet, in this study, the add-on components of pre-treatment assessment and clinical guidance did not bolster these outcomes – even among participants who received both the pre-treatment interview assessment as well as the ongoing weekly clinical guidance over time. Given that the web-based CBT was helpful in reducing drinking and that the clinical guidance did improve participant engagement in the modules (but did not further boost outcomes), it seems that another approach to boosting engagement and to improving subsequent outcomes might be necessary. That is, there may be a need to create other add-ons (aside from assessments and clinical guidance) that target different mechanisms of behavior change to boost outcomes. Or perhaps, by altering the intensity, nature, and/or timing of the clinical guidance making it more flexibly available and “on demand” at times perhaps when some participants might actually need it more (e.g., evenings and weekends). This could be examined in future research.
Assessment reactivity, the response to having questions asked about a behavior, could have been initiated even prior to the pre-treatment assessment interview and been a factor in each of the four groups. That is, all potential participants were screened prior to enrollment in the study using the Alcohol Use Disorder Identification Tool (AUDIT), a tool which asks questions about alcohol use behaviors. As a result, all participants could have already been primed to reflect on their alcohol consumption behaviors prior to their assignment to the study treatment condition. Thus, the pre-treatment assessment interview condition may not be distinct enough to produce additional lasting effects.
Furthermore, although the clinical guidance condition was not more effective than the other conditions, it could be that engagement in this condition leads to improved outcomes later, such as by helping to make a participant more comfortable talking with their physician or engaging in the healthcare system for treatment. This could be a beneficial effect of the study that may go unrecognized but have longer lasting implications beyond the study time frame. One indication of these potential benefits is that participants in this condition did engage in more of the online treatment modules and for longer which may have resulted in deeper and more elaborative processing of the information and consequently be more likely to have a more lasting positive effect down the road.
The degree of participant motivation across all groups could be a driving factor in the overall reduction in drinking. Nearly all participants moved from a pre-contemplation stage of change to the action stage of readiness to change before they engaged with the web-based intervention or either of the additional components – assessment and guidance. Thus, this effect on increasing motivation to a high level that can drive behavior change, may mean that once a certain motivational threshold is reached any additional therapeutic components may have little additional benefit in most cases as the individual is able to make changes themselves without any need for those additional elements.
There was also likely a relatively high degree of psychosocial stability and financial recovery capital present in this sample and so these findings may not generalize to other samples. That is, the majority of participants had education beyond high school and were employed, suggesting they had a set of resources supporting their overall well-being and potential for seeking treatment and engaging in recovery. And, the 30% of participants who were not retained in the study, might have needed different types or more supports than provided here and actually fared worse than those who remained in the study. In other words, people with alcohol problems who do not have these resources to depend on and draw from, might still benefit from some of these additional elements and clinician support over time. Further research is needed to confirm this.
There were several additional components that participants engaged in through the study design (e.g., reflection questions, contacts with the study team), which could have made it difficult to show any effect over and above these components that both groups got. Thus, while this study did not demonstrate increased impacts due to the add-on of a pre-treatment assessment or clinical guidance, these components could still be important to consider incorporating in other study designs.
The outcomes represent short-term findings, but as longer-term findings are still in process (6-month and 1-year), there may be some differences across the intervention groups that could represent durability of the different approaches.
There was a large amount of missing data due to participant non-response or attrition. That is, 27% of participants were not retained at post-treatment and a further 10% of participants (for a total of 37%) were not retained at 3-months. The attrition differed by groups: those in the clinical guidance group were significantly more likely to complete posttreatment and 3-month follow-ups. The authors used multiple imputation analysis to address this potential selection bias, but the outcomes present in this sample could only represent findings from a select group of participants who were able to stay engaged.
BOTTOM LINE
Adults with heavy drinking patterns but relatively high psychosocial stability and available resources reduced their drinking levels and number of heavy drinking days through their engagement in a web-based cognitive behavioral therapy intervention. According to their survey measures, the intervention was viewed as credible and acceptable to participants. Additionally, these participants also improved in several other areas of life, including in craving, daily functioning, depression, and anxiety. Despite the overall success of the intervention, the study did not find that the add-on components of pre-treatment interview assessment and/or ongoing weekly clinical guidance served to bolster these outcomes; yet pre-treatment motivation changes were also predictive of participant drinking reductions. Thus, it is possible that the design of the web-based CBT produced a strong treatment effect and to improve upon that, perhaps either the timing, frequency, or duration, of these elements, or new or additional strategies, need to be added and tested.
For individuals and families seeking recovery: Reducing alcohol use can result in improved health and well-being and save lives. Engaging in a brief online intervention that helps to address thoughts and behaviors related to drinking may help initiate change in harmful drinking habits. Locating and accessing one of these types of well-established online interventions could have a positive effect on reducing harms without the need to engage with a formal treatment facility.
For treatment professionals and treatment systems: Reducing alcohol use can result in improved health and well-being and save lives. As a clinician, given the prevalence of harmful/hazardous alcohol use and alcohol use disorder, routine alcohol screening is recommended. This initial conversation can be a starting point for building a relationship to addressing any unknown issues, and there are many evidence-based resources to direct patients to, including online approaches like the one used in this study. Furthermore, simply asking them about their behavior may initiate reflection which could be later motivation for change.
For scientists:This article provides further evidence of the acceptability and potential helpfulness of online brief intervention approaches that utilize CBT. Strikingly, the outcomes benefits observed here using standard online CBT are of a potentially meaningful public health magnitude (i.e., reductions in heavy drinking days of 50%). Yet, there is always room for improvement and there is still a lack of knowledge around how best to improve on web-based intervention outcomes for individuals who don’t engage with formal in-person treatment (which is nearly all cases of alcohol use disorder – 90% or more do not engage with professional alcohol treatment services in any given year). As well, this study consisted largely of individuals with higher levels of education and income. Further research needs to examine whether these approaches are acceptable with other populations and whether they also demonstrate reductions in drinking.
For policy makers: The reduction of alcohol use can result in improved health and well-being and save lives. Funding for healthcare system linkages (e.g., from primary care) to support early screening and intervention may help to prevent future alcohol problems. Brief online evidence-based interventions can work for some individuals to initiate and sustain a process of change. Online programs such as the one used in this study have the potential increase the reach to the vast population of untreated heavy drinkers of alcohol and have a beneficial public health impact.
Given the modest effects of these interventions, clinical researchers are always looking for ways to enhance impact. There could be some simple ways to build on these outcomes and boost results using brief add-ons. There are several potential add-ons that research suggests might enhance web-based CBT.
One idea is that a pre-treatment assessment interview could improve outcomes by putting participants in a self-reflective mode that has the potential to increase their motivation for engagement in the intervention. For example, pre-treatment assessments that ask a participant to report on their current drinking behaviors, could encourage participants to begin to consider their drinking and whether it is something they might want to change. This is a well-known concept, called Assessment Reactivity, and it has been studied in a variety of disciplines including alcohol research. Research has shown that more frequent and comprehensive assessments tend to show the greatest boost in positive outcomes among patients treated for alcohol use disorders.
One other potentially helpful add-on, that might require more resources than a pre-treatment assessment, would be to include a clinical guidance component. In this component, the participant would meet with a clinician in addition to completing the online intervention components. Adding this aspect to an online intervention could help personalize the experience for the patient, increase their motivation, and increase their accountability or further engagement with clinical care. Yet, previous research has demonstrated mixed results on whether adding clinical guidance makes a big difference in participant outcomes.
In this study, the researchers tested whether adding a pre-treatment assessment interview and/or guidance to an existing web-based cognitive behavior therapy (CBT) improved participant outcomes and reduced alcohol use.
HOW WAS THIS STUDY CONDUCTED?
This was a 2X2 factorial randomized controlled trial, where participants were randomized to one of 4 groups: (1) 8-week web-based CBT program, which the researchers called “internet-delivered CBT, or IBCT”; (2) 8-week web-based CBT program + pre-treatment assessment interview; (3) 8-week web-based CBT program + clinical guidance; or (4) 8-week web-based CBT program + pre-treatment assessment interview and clinical guidance. A “2X2” design means there were two independent variables each with two different groups – assessment (yes or no) and guidance (yes or no). To be eligible for the study, participants had to be adults who scored 8 or higher on the Alcohol Use Disorders Identification Test (AUDIT) and who consumed 14 or more drinks in the previous week (a standard drink in Canada is 13.45 grams of pure alcohol or about 12 oz. of beer with 5% ABV).
Participants who were assigned to the pre-treatment assessment interview condition were asked to complete the alcohol use disorder module of the Structured Clinical Interview Diagnostic Statistical Manual 5 – Research Version with a member of the research team. On average the screening calls that included this aspect of the study lasted 36 minutes while those without lasted 18.4 minutes, suggesting the assessment interview was about 15-20 minutes long.
Participants who were assigned to the clinical guidance condition received messages and interaction primarily from clinicians over time through the treatment platform. These interactions lasted about 15 minutes/week and messages included answering participants’ questions, trying to reinforce module completion, and boosting participant’s motivation.
In addition to the different components of each treatment condition, as part of the study, all participants received weekly emails about the next week’s content and were asked to complete reflection questions on challenges they might have had with the activities and lessons learned, and to complete a brief questionnaire assessing depression, anxiety, and suicidal ideation (Patient Health Questionnaire-4 and PHQ-9). They were also asked the following two questions about past week alcohol use: (1) How many drinks have you had in the past week; and (2) Over how many days did you consume these drinks?
The primary outcomes, measured at 3 months were the number of drinks consumed and the number of heavy drinking days during the previous week (defined as ≥ 4 drinks per day for women and ≥ 5 drinks per day for men). The secondary outcomes included scores from the Alcohol Use Disorder Identification Test, alcohol craving (Penn Alcohol scale), Confidence in the ability to not drink/drink less (Brief situational confidence questionnaire), Daily functioning (Sheehan disability scale), Depression (PHQ), Anxiety (GAD-7), motivation to change (Readiness to change questionnaire, treatment version), and treatment credibility (Credibility/Expectancy questionnaire). Adherence to treatment was also captured through recording module completion. They also captured the number of logins to the website, number of modules accessed, and time in days between first and last using the website.
Of the sample of 270 adult participants, most were White (93%), had further formal education after completing high school (85.6%), employed (69%), female (67%), and married (63%), and they were 46.5 years old on average. Participants, on average, reported consuming 41.7 (SD = 24.8) drinks and had 4.5 (SD = 2.1) heavy drinking days in the preceding week. The average score on the AUDIT was 24.0 (SD = 5.8), indicating high average likelihood of alcohol use disorder across the sample.
WHAT DID THIS STUDY FIND?
Participants completed most of the intervention with an advantage for those getting the clinical guidance.
On average, participants across all four conditions completed 8 out of the 12 modules of the online treatment (67%). But participants who received the clinician guidance completed more modules, used the program for a longer time, and had more logins than the other groups.
There were no group differences on drinking outcomes.
Participants in each of the four intervention groups improved by about the same amount reducing their number of drinks and number of heavy drinking days. That is, participants halved both their number of drinks and number of heavy drinking days from screening to post-treatment and these findings were maintained at 3 months. Importantly, although all groups demonstrated improvement, this also means that the add-ons of assessment or guidance did not improve drinking outcomes beyond the web-based CBT by itself, as researchers hypothesized.
Similarly, all participants improved to roughly the same degree from pre-treatment to 3 months on the secondary outcomes of alcohol use disorder identification scores, alcohol craving, situational confidence, daily functioning, depression, and anxiety. Additionally, secondary outcomes related to the treatment experience including treatment credibility, satisfaction, or negative effects did not differ between the groups.
Pre-treatment shifts in motivation may be responsible for lack of group differences.
Participants demonstrated motivational change from the time of pre-screening to beginning treatment. Using the readiness to change scale – which goes from thinking about change (pre-contemplation) to actually making change – nearly all participants moved from a pre-contemplation stage of change to the action stage of readiness to change at pre-treatment. In addition, the initial reductions in drinking alcohol during the pre-treatment phase were strongly correlated with changes during treatment: the correlations indicated a relationship of 0.52 for drinking amount and 0.46 for heavy drinking days.
Yet, in this study, the add-on components of pre-treatment assessment and clinical guidance did not bolster these outcomes – even among participants who received both the pre-treatment interview assessment as well as the ongoing weekly clinical guidance over time. Given that the web-based CBT was helpful in reducing drinking and that the clinical guidance did improve participant engagement in the modules (but did not further boost outcomes), it seems that another approach to boosting engagement and to improving subsequent outcomes might be necessary. That is, there may be a need to create other add-ons (aside from assessments and clinical guidance) that target different mechanisms of behavior change to boost outcomes. Or perhaps, by altering the intensity, nature, and/or timing of the clinical guidance making it more flexibly available and “on demand” at times perhaps when some participants might actually need it more (e.g., evenings and weekends). This could be examined in future research.
Assessment reactivity, the response to having questions asked about a behavior, could have been initiated even prior to the pre-treatment assessment interview and been a factor in each of the four groups. That is, all potential participants were screened prior to enrollment in the study using the Alcohol Use Disorder Identification Tool (AUDIT), a tool which asks questions about alcohol use behaviors. As a result, all participants could have already been primed to reflect on their alcohol consumption behaviors prior to their assignment to the study treatment condition. Thus, the pre-treatment assessment interview condition may not be distinct enough to produce additional lasting effects.
Furthermore, although the clinical guidance condition was not more effective than the other conditions, it could be that engagement in this condition leads to improved outcomes later, such as by helping to make a participant more comfortable talking with their physician or engaging in the healthcare system for treatment. This could be a beneficial effect of the study that may go unrecognized but have longer lasting implications beyond the study time frame. One indication of these potential benefits is that participants in this condition did engage in more of the online treatment modules and for longer which may have resulted in deeper and more elaborative processing of the information and consequently be more likely to have a more lasting positive effect down the road.
The degree of participant motivation across all groups could be a driving factor in the overall reduction in drinking. Nearly all participants moved from a pre-contemplation stage of change to the action stage of readiness to change before they engaged with the web-based intervention or either of the additional components – assessment and guidance. Thus, this effect on increasing motivation to a high level that can drive behavior change, may mean that once a certain motivational threshold is reached any additional therapeutic components may have little additional benefit in most cases as the individual is able to make changes themselves without any need for those additional elements.
There was also likely a relatively high degree of psychosocial stability and financial recovery capital present in this sample and so these findings may not generalize to other samples. That is, the majority of participants had education beyond high school and were employed, suggesting they had a set of resources supporting their overall well-being and potential for seeking treatment and engaging in recovery. And, the 30% of participants who were not retained in the study, might have needed different types or more supports than provided here and actually fared worse than those who remained in the study. In other words, people with alcohol problems who do not have these resources to depend on and draw from, might still benefit from some of these additional elements and clinician support over time. Further research is needed to confirm this.
There were several additional components that participants engaged in through the study design (e.g., reflection questions, contacts with the study team), which could have made it difficult to show any effect over and above these components that both groups got. Thus, while this study did not demonstrate increased impacts due to the add-on of a pre-treatment assessment or clinical guidance, these components could still be important to consider incorporating in other study designs.
The outcomes represent short-term findings, but as longer-term findings are still in process (6-month and 1-year), there may be some differences across the intervention groups that could represent durability of the different approaches.
There was a large amount of missing data due to participant non-response or attrition. That is, 27% of participants were not retained at post-treatment and a further 10% of participants (for a total of 37%) were not retained at 3-months. The attrition differed by groups: those in the clinical guidance group were significantly more likely to complete posttreatment and 3-month follow-ups. The authors used multiple imputation analysis to address this potential selection bias, but the outcomes present in this sample could only represent findings from a select group of participants who were able to stay engaged.
BOTTOM LINE
Adults with heavy drinking patterns but relatively high psychosocial stability and available resources reduced their drinking levels and number of heavy drinking days through their engagement in a web-based cognitive behavioral therapy intervention. According to their survey measures, the intervention was viewed as credible and acceptable to participants. Additionally, these participants also improved in several other areas of life, including in craving, daily functioning, depression, and anxiety. Despite the overall success of the intervention, the study did not find that the add-on components of pre-treatment interview assessment and/or ongoing weekly clinical guidance served to bolster these outcomes; yet pre-treatment motivation changes were also predictive of participant drinking reductions. Thus, it is possible that the design of the web-based CBT produced a strong treatment effect and to improve upon that, perhaps either the timing, frequency, or duration, of these elements, or new or additional strategies, need to be added and tested.
For individuals and families seeking recovery: Reducing alcohol use can result in improved health and well-being and save lives. Engaging in a brief online intervention that helps to address thoughts and behaviors related to drinking may help initiate change in harmful drinking habits. Locating and accessing one of these types of well-established online interventions could have a positive effect on reducing harms without the need to engage with a formal treatment facility.
For treatment professionals and treatment systems: Reducing alcohol use can result in improved health and well-being and save lives. As a clinician, given the prevalence of harmful/hazardous alcohol use and alcohol use disorder, routine alcohol screening is recommended. This initial conversation can be a starting point for building a relationship to addressing any unknown issues, and there are many evidence-based resources to direct patients to, including online approaches like the one used in this study. Furthermore, simply asking them about their behavior may initiate reflection which could be later motivation for change.
For scientists:This article provides further evidence of the acceptability and potential helpfulness of online brief intervention approaches that utilize CBT. Strikingly, the outcomes benefits observed here using standard online CBT are of a potentially meaningful public health magnitude (i.e., reductions in heavy drinking days of 50%). Yet, there is always room for improvement and there is still a lack of knowledge around how best to improve on web-based intervention outcomes for individuals who don’t engage with formal in-person treatment (which is nearly all cases of alcohol use disorder – 90% or more do not engage with professional alcohol treatment services in any given year). As well, this study consisted largely of individuals with higher levels of education and income. Further research needs to examine whether these approaches are acceptable with other populations and whether they also demonstrate reductions in drinking.
For policy makers: The reduction of alcohol use can result in improved health and well-being and save lives. Funding for healthcare system linkages (e.g., from primary care) to support early screening and intervention may help to prevent future alcohol problems. Brief online evidence-based interventions can work for some individuals to initiate and sustain a process of change. Online programs such as the one used in this study have the potential increase the reach to the vast population of untreated heavy drinkers of alcohol and have a beneficial public health impact.
Given the modest effects of these interventions, clinical researchers are always looking for ways to enhance impact. There could be some simple ways to build on these outcomes and boost results using brief add-ons. There are several potential add-ons that research suggests might enhance web-based CBT.
One idea is that a pre-treatment assessment interview could improve outcomes by putting participants in a self-reflective mode that has the potential to increase their motivation for engagement in the intervention. For example, pre-treatment assessments that ask a participant to report on their current drinking behaviors, could encourage participants to begin to consider their drinking and whether it is something they might want to change. This is a well-known concept, called Assessment Reactivity, and it has been studied in a variety of disciplines including alcohol research. Research has shown that more frequent and comprehensive assessments tend to show the greatest boost in positive outcomes among patients treated for alcohol use disorders.
One other potentially helpful add-on, that might require more resources than a pre-treatment assessment, would be to include a clinical guidance component. In this component, the participant would meet with a clinician in addition to completing the online intervention components. Adding this aspect to an online intervention could help personalize the experience for the patient, increase their motivation, and increase their accountability or further engagement with clinical care. Yet, previous research has demonstrated mixed results on whether adding clinical guidance makes a big difference in participant outcomes.
In this study, the researchers tested whether adding a pre-treatment assessment interview and/or guidance to an existing web-based cognitive behavior therapy (CBT) improved participant outcomes and reduced alcohol use.
HOW WAS THIS STUDY CONDUCTED?
This was a 2X2 factorial randomized controlled trial, where participants were randomized to one of 4 groups: (1) 8-week web-based CBT program, which the researchers called “internet-delivered CBT, or IBCT”; (2) 8-week web-based CBT program + pre-treatment assessment interview; (3) 8-week web-based CBT program + clinical guidance; or (4) 8-week web-based CBT program + pre-treatment assessment interview and clinical guidance. A “2X2” design means there were two independent variables each with two different groups – assessment (yes or no) and guidance (yes or no). To be eligible for the study, participants had to be adults who scored 8 or higher on the Alcohol Use Disorders Identification Test (AUDIT) and who consumed 14 or more drinks in the previous week (a standard drink in Canada is 13.45 grams of pure alcohol or about 12 oz. of beer with 5% ABV).
Participants who were assigned to the pre-treatment assessment interview condition were asked to complete the alcohol use disorder module of the Structured Clinical Interview Diagnostic Statistical Manual 5 – Research Version with a member of the research team. On average the screening calls that included this aspect of the study lasted 36 minutes while those without lasted 18.4 minutes, suggesting the assessment interview was about 15-20 minutes long.
Participants who were assigned to the clinical guidance condition received messages and interaction primarily from clinicians over time through the treatment platform. These interactions lasted about 15 minutes/week and messages included answering participants’ questions, trying to reinforce module completion, and boosting participant’s motivation.
In addition to the different components of each treatment condition, as part of the study, all participants received weekly emails about the next week’s content and were asked to complete reflection questions on challenges they might have had with the activities and lessons learned, and to complete a brief questionnaire assessing depression, anxiety, and suicidal ideation (Patient Health Questionnaire-4 and PHQ-9). They were also asked the following two questions about past week alcohol use: (1) How many drinks have you had in the past week; and (2) Over how many days did you consume these drinks?
The primary outcomes, measured at 3 months were the number of drinks consumed and the number of heavy drinking days during the previous week (defined as ≥ 4 drinks per day for women and ≥ 5 drinks per day for men). The secondary outcomes included scores from the Alcohol Use Disorder Identification Test, alcohol craving (Penn Alcohol scale), Confidence in the ability to not drink/drink less (Brief situational confidence questionnaire), Daily functioning (Sheehan disability scale), Depression (PHQ), Anxiety (GAD-7), motivation to change (Readiness to change questionnaire, treatment version), and treatment credibility (Credibility/Expectancy questionnaire). Adherence to treatment was also captured through recording module completion. They also captured the number of logins to the website, number of modules accessed, and time in days between first and last using the website.
Of the sample of 270 adult participants, most were White (93%), had further formal education after completing high school (85.6%), employed (69%), female (67%), and married (63%), and they were 46.5 years old on average. Participants, on average, reported consuming 41.7 (SD = 24.8) drinks and had 4.5 (SD = 2.1) heavy drinking days in the preceding week. The average score on the AUDIT was 24.0 (SD = 5.8), indicating high average likelihood of alcohol use disorder across the sample.
WHAT DID THIS STUDY FIND?
Participants completed most of the intervention with an advantage for those getting the clinical guidance.
On average, participants across all four conditions completed 8 out of the 12 modules of the online treatment (67%). But participants who received the clinician guidance completed more modules, used the program for a longer time, and had more logins than the other groups.
There were no group differences on drinking outcomes.
Participants in each of the four intervention groups improved by about the same amount reducing their number of drinks and number of heavy drinking days. That is, participants halved both their number of drinks and number of heavy drinking days from screening to post-treatment and these findings were maintained at 3 months. Importantly, although all groups demonstrated improvement, this also means that the add-ons of assessment or guidance did not improve drinking outcomes beyond the web-based CBT by itself, as researchers hypothesized.
Similarly, all participants improved to roughly the same degree from pre-treatment to 3 months on the secondary outcomes of alcohol use disorder identification scores, alcohol craving, situational confidence, daily functioning, depression, and anxiety. Additionally, secondary outcomes related to the treatment experience including treatment credibility, satisfaction, or negative effects did not differ between the groups.
Pre-treatment shifts in motivation may be responsible for lack of group differences.
Participants demonstrated motivational change from the time of pre-screening to beginning treatment. Using the readiness to change scale – which goes from thinking about change (pre-contemplation) to actually making change – nearly all participants moved from a pre-contemplation stage of change to the action stage of readiness to change at pre-treatment. In addition, the initial reductions in drinking alcohol during the pre-treatment phase were strongly correlated with changes during treatment: the correlations indicated a relationship of 0.52 for drinking amount and 0.46 for heavy drinking days.
Yet, in this study, the add-on components of pre-treatment assessment and clinical guidance did not bolster these outcomes – even among participants who received both the pre-treatment interview assessment as well as the ongoing weekly clinical guidance over time. Given that the web-based CBT was helpful in reducing drinking and that the clinical guidance did improve participant engagement in the modules (but did not further boost outcomes), it seems that another approach to boosting engagement and to improving subsequent outcomes might be necessary. That is, there may be a need to create other add-ons (aside from assessments and clinical guidance) that target different mechanisms of behavior change to boost outcomes. Or perhaps, by altering the intensity, nature, and/or timing of the clinical guidance making it more flexibly available and “on demand” at times perhaps when some participants might actually need it more (e.g., evenings and weekends). This could be examined in future research.
Assessment reactivity, the response to having questions asked about a behavior, could have been initiated even prior to the pre-treatment assessment interview and been a factor in each of the four groups. That is, all potential participants were screened prior to enrollment in the study using the Alcohol Use Disorder Identification Tool (AUDIT), a tool which asks questions about alcohol use behaviors. As a result, all participants could have already been primed to reflect on their alcohol consumption behaviors prior to their assignment to the study treatment condition. Thus, the pre-treatment assessment interview condition may not be distinct enough to produce additional lasting effects.
Furthermore, although the clinical guidance condition was not more effective than the other conditions, it could be that engagement in this condition leads to improved outcomes later, such as by helping to make a participant more comfortable talking with their physician or engaging in the healthcare system for treatment. This could be a beneficial effect of the study that may go unrecognized but have longer lasting implications beyond the study time frame. One indication of these potential benefits is that participants in this condition did engage in more of the online treatment modules and for longer which may have resulted in deeper and more elaborative processing of the information and consequently be more likely to have a more lasting positive effect down the road.
The degree of participant motivation across all groups could be a driving factor in the overall reduction in drinking. Nearly all participants moved from a pre-contemplation stage of change to the action stage of readiness to change before they engaged with the web-based intervention or either of the additional components – assessment and guidance. Thus, this effect on increasing motivation to a high level that can drive behavior change, may mean that once a certain motivational threshold is reached any additional therapeutic components may have little additional benefit in most cases as the individual is able to make changes themselves without any need for those additional elements.
There was also likely a relatively high degree of psychosocial stability and financial recovery capital present in this sample and so these findings may not generalize to other samples. That is, the majority of participants had education beyond high school and were employed, suggesting they had a set of resources supporting their overall well-being and potential for seeking treatment and engaging in recovery. And, the 30% of participants who were not retained in the study, might have needed different types or more supports than provided here and actually fared worse than those who remained in the study. In other words, people with alcohol problems who do not have these resources to depend on and draw from, might still benefit from some of these additional elements and clinician support over time. Further research is needed to confirm this.
There were several additional components that participants engaged in through the study design (e.g., reflection questions, contacts with the study team), which could have made it difficult to show any effect over and above these components that both groups got. Thus, while this study did not demonstrate increased impacts due to the add-on of a pre-treatment assessment or clinical guidance, these components could still be important to consider incorporating in other study designs.
The outcomes represent short-term findings, but as longer-term findings are still in process (6-month and 1-year), there may be some differences across the intervention groups that could represent durability of the different approaches.
There was a large amount of missing data due to participant non-response or attrition. That is, 27% of participants were not retained at post-treatment and a further 10% of participants (for a total of 37%) were not retained at 3-months. The attrition differed by groups: those in the clinical guidance group were significantly more likely to complete posttreatment and 3-month follow-ups. The authors used multiple imputation analysis to address this potential selection bias, but the outcomes present in this sample could only represent findings from a select group of participants who were able to stay engaged.
BOTTOM LINE
Adults with heavy drinking patterns but relatively high psychosocial stability and available resources reduced their drinking levels and number of heavy drinking days through their engagement in a web-based cognitive behavioral therapy intervention. According to their survey measures, the intervention was viewed as credible and acceptable to participants. Additionally, these participants also improved in several other areas of life, including in craving, daily functioning, depression, and anxiety. Despite the overall success of the intervention, the study did not find that the add-on components of pre-treatment interview assessment and/or ongoing weekly clinical guidance served to bolster these outcomes; yet pre-treatment motivation changes were also predictive of participant drinking reductions. Thus, it is possible that the design of the web-based CBT produced a strong treatment effect and to improve upon that, perhaps either the timing, frequency, or duration, of these elements, or new or additional strategies, need to be added and tested.
For individuals and families seeking recovery: Reducing alcohol use can result in improved health and well-being and save lives. Engaging in a brief online intervention that helps to address thoughts and behaviors related to drinking may help initiate change in harmful drinking habits. Locating and accessing one of these types of well-established online interventions could have a positive effect on reducing harms without the need to engage with a formal treatment facility.
For treatment professionals and treatment systems: Reducing alcohol use can result in improved health and well-being and save lives. As a clinician, given the prevalence of harmful/hazardous alcohol use and alcohol use disorder, routine alcohol screening is recommended. This initial conversation can be a starting point for building a relationship to addressing any unknown issues, and there are many evidence-based resources to direct patients to, including online approaches like the one used in this study. Furthermore, simply asking them about their behavior may initiate reflection which could be later motivation for change.
For scientists:This article provides further evidence of the acceptability and potential helpfulness of online brief intervention approaches that utilize CBT. Strikingly, the outcomes benefits observed here using standard online CBT are of a potentially meaningful public health magnitude (i.e., reductions in heavy drinking days of 50%). Yet, there is always room for improvement and there is still a lack of knowledge around how best to improve on web-based intervention outcomes for individuals who don’t engage with formal in-person treatment (which is nearly all cases of alcohol use disorder – 90% or more do not engage with professional alcohol treatment services in any given year). As well, this study consisted largely of individuals with higher levels of education and income. Further research needs to examine whether these approaches are acceptable with other populations and whether they also demonstrate reductions in drinking.
For policy makers: The reduction of alcohol use can result in improved health and well-being and save lives. Funding for healthcare system linkages (e.g., from primary care) to support early screening and intervention may help to prevent future alcohol problems. Brief online evidence-based interventions can work for some individuals to initiate and sustain a process of change. Online programs such as the one used in this study have the potential increase the reach to the vast population of untreated heavy drinkers of alcohol and have a beneficial public health impact.