Preventing burnout and improving resilience in hospital-based addiction medicine professionals
Despite the high occurrence of substance-related accidents and illness among hospital patients, most hospital staff receive little substance use disorder training. Addiction consultation services are designed to help fill this need by providing acute care and connecting patients with community resources. Given the high prevalence and complexity of such clinical cases, however, consultation staff are often at heightened risk of burnout. This study asked 26 clinicians working on multidisciplinary addiction consultation teams to identify factors connected with burnout and resilience.
Substance use disorder patients make up 1 in 11 emergency department visits and 1 in 9 hospitalizations. Some of these visits may result from substance use disorder-related events (e.g., alcohol-related liver damage, endocarditis), while others may result from accidents not related to an individual’s substance use disorder (e.g., appendicitis, COVID-19). Identifying and capitalizing on opportunities to address substance use disorders in acute care settings in tandem with other medical concerns may be an important way to reduce time to treatment and reduce harms from substance use.
Despite the potential to address substance use during hospital stays, most medical staff do not have addiction medicine training or experience. Addiction consultation services are one intervention that has been shown to reduce addiction severity and increase abstinence as well as reduce 30-day readmission rates among patients with current or suspected substance use disorder being treated in a medical unit that does not directly address substance use disorder (e.g., for liver, cardiac, or pulmonary conditions, as examples). Addiction consultations services vary across hospitals, but they often initiate or link patients with pharmacotherapy services (e.g., buprenorphine, methadone), provide brief counseling, support aftercare planning, and connect patients directly to treatment following discharge. Members of these teams may include physicians, psychiatrists, psychologists, advanced practice nurses, social workers, recovery coaches, and peer workers.
Providers of addiction services may be more prone to burnout due to the complex social and behavioral needs of individuals with substance use disorder (SUD), as well as the high prevalence of trauma among this population. Burnout is a state of chronic physical and emotional exhaustion, accompanied by a lack of motivation and feelings of cynicism or detachment. Symptoms of burnout may include fatigue, difficulty concentrating, irritability, and a decreased ability to find enjoyment in work or other activities. In severe cases, burnout can lead to physical illness and may require time off work or other interventions to recover. Yet, addiction consultations teams may also exhibit resilience. Resilience is the ability to bounce back from adversity or difficult experiences, and to adapt and cope with challenges in a healthy and effective way. Resilience involves a range of skills and strategies, including the ability to manage stress, to maintain a positive outlook, to seek support when needed, and to learn from difficult experiences. Identifying factors associated with resilience and burnout among addiction service providers may provide possible targets for future interventions to best support providers in these unique and increasingly valuable roles.
HOW WAS THIS STUDY CONDUCTED?
This was a qualitative study that analyzed individual interviews with members of addiction consultations teams to identify factors associated with burnout and resilience among hospital-based addiction medicine providers. A total of 26 interviews with clinicians working on these teams were conducted representing 3 different provider types and 12 institutions. Interviews were conducted between October 2020 and March 2021.
For this study, the participants were healthcare providers who worked in hospitals and provided consultation services for addiction treatment. The researchers recruited these participants by contacting the directors of addiction consultation teams and through recommendations from the early participants (i.e., snowball sampling). The interviews with the participants focused on various aspects of their work, including the meaning they found in their work, how they balanced their work and personal lives, the demands and workload of their job, the efficiency and resources available to them, their level of control and flexibility, the support they received from colleagues and the organization, and the culture and values of the organization.
Twenty-six providers completed interviews representing 12 different academic hospitals across the country. Participants included 15 physicians, 8 social workers, and 3 advanced practice providers. Sixteen of the participants (64%) identified as female and 18 (72%) had at least 3 years of experience practicing in addiction medicine. Among the physicians, 11 (79%) were boarded in addiction medicine, and 10 (71%) were trained in internal medicine. Two physicians were trained in family medicine, and 2 others were trained in psychiatry. Most of the providers (75%) worked on other services (e.g., outpatient primary care, outpatient addiction medicine, etc.) in addition to the inpatient addiction consultation team. The others (25%) worked exclusively on the consultation team.
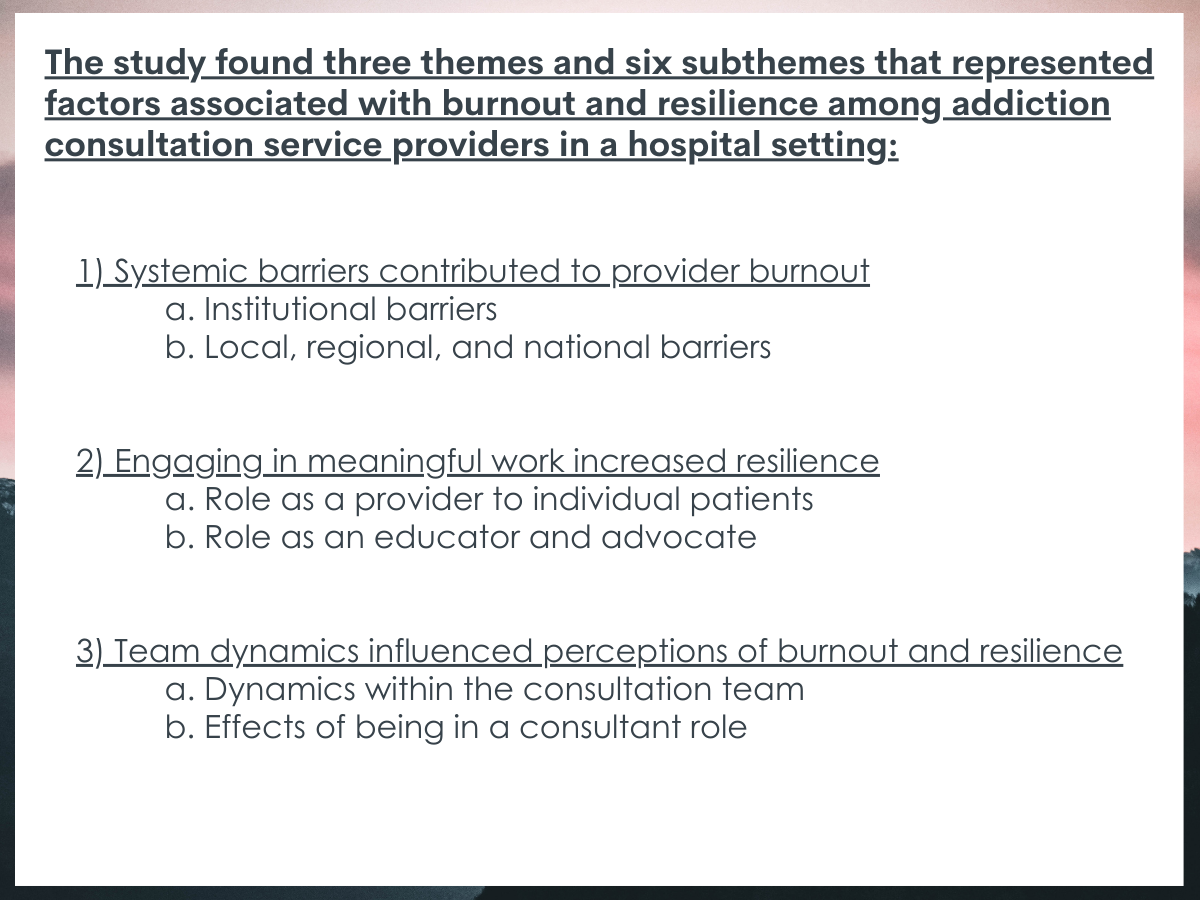
WHAT DID THIS STUDY FIND?
Persistent barriers contribute to burnout.
Providers identified barriers within the hospital and in the community. Within the hospital, providers felt pressured to discharge patients even if they did not have a solid plan to address the patient’s substance use disorder. High patient turnover in the inpatient setting also conflicted with the much slower pace of community programs. Additionally, hospital policies, such as those that limited prescribing medications for opioid use disorder (e.g., buprenorphine, methadone) frustrated staff and was viewed as problematic. The pressure to discharge patients alongside potentially limiting hospital policies contributed to feelings of burnout, especially when providers sought to change internal practices and policies. More generally, barriers such as limited community resources or long waitlists for addiction treatment left providers feeling frustrated at the lack of available resources for patients upon discharge.
Meaningful work confers resilience.
Hospital-based providers in the field of addiction medicine often found their work deeply rewarding through their non-judgmental care of patients and advocacy/education work within the hospital and in the community. Participants cited that providing such care to patients who may face discrimination or negative attitudes within the healthcare system due to their substance use can increase optimism in the field and be intrinsically motivating. Moreover, providers derived a sense of meaning through advocacy work and education within their institutions as well as within their broader communities. The sense of meaning and satisfaction found within addiction medicine were factors of resilience among these providers.
Team dynamics can influence burnout and resilience.
Members of addiction consultation teams expressed feelings of support from other members of their team. They valued working on interdisciplinary teams and felt doing so benefited patients and themselves. However, some providers were discouraged by negative dealings with other hospital staff. Negative interactions included other teams not acting on the addiction consultative team’s recommendations, perceived stigma, and when patients were discharged without an adequate care plan to address their substance use.
Stigma impacts burnout and sparks resilience.
Stigma appeared as a key component of burnout and resilience, and it was seen a mechanism that influenced team dynamics. Hospital-based and systemic barriers were believed to arise from stigma. Policies restricting effective medications, such as medications for opioid use disorder, were viewed as rooted in stigma and negatively impacted the care of patients with substance use disorders. Addiction service providers also felt intrinsic rewards when they were able to deliver patient-centered care to patients that experience intense stigma within the healthcare system. Advocacy and education were often done to address stigma within the hospital and in the community. For example, training future addiction medicine providers to reduce the stigmatization of patients with substance use disorders was perceived as an effective way to reduce stigma long-term. However, on-going exposure to stigma within the hospital and elsewhere was noted as contributing to burnout.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Hospital-based addiction consultation services have been shown to improve outcomes for patients with substance use disorder (e.g., fewer inpatient days, fewer emergency department visits). However, providers of these services may face heightened risk of burnout due to the complex social and behavioral needs of patients with substance use disorders. The findings from this study highlight how administrative and societal barriers may also increase burnout among these providers. However, the findings also highlight how practicing addiction medicine can support a sense of meaning and satisfaction. Team dynamics, within addiction consultation teams and between other hospital teams, can be supportive or discouraging. Maintaining a sustainable workforce will require reducing factors of burnout, increasing factors of resilience, and improving team dynamics.
Providers felt they were not always able to provide the effective, evidence-based care (e.g., medications for opioid use disorder) due to hospital and federal policies they viewed as rooted in stigma. Moreover, participants in the study witnessed the stigmatization of patients by other medical professionals, which further contribute to perceptions of burnout. Although providers derived meaning and value from providing patient-centered care in a non-judgmental way and educating their peers against stigmatizing beliefs and actions, providers also felt burdened by the sensed responsibility of reducing stigma within healthcare and the larger society. The findings from this study suggest that reducing stigma towards substance use disorders among all hospital providers may reduce burnout among providers of addiction services. Moreover, the findings showed that the meaning derived from addiction medicine work can promote resilience. Thus, uncovering ways to enhance the sense of meaning providers feel for the work (e.g., public recognition, patient feedback) may reduce burnout.
For example, one review of interventions with healthcare providers showed educational interventions can have positive effects and that interventions featuring contact with individuals with lived experience can enhance and sustain those positive changes. Additionally, changing the language used to describe people who use drugs and addiction may also effectively reduce stigma. For example, experimental research has shown that using the term “substance abuser” increases stigma compared with the person-first term “person with a substance use disorder.” The words and phrases that we use can influence the way that people perceive and understand these issues and can either reinforce or challenge stigma and negative stereotypes. It is important to use language that is respectful, accurate, and non-judgmental when discussing substance use and recovery. The Addictionary® is a resource developed by the Recovery Research Institute that provides guidance on using language that is inclusive and non-stigmatizing when discussing substance use and recovery. If you would like to learn more about destigmatizing language, you may find it helpful to consult the Addictionary®.
The study did not include non-clinical or peer workers with lived experiences, which may have minimized perceptions and experiences of burnout and/or resilience.
Participants were recruited via email and recommendations from early participants. Thus, the providers that self-selected to participate may have felt especially burned out or motivated by their experiences on addiction consultation services potentially skewing findings toward more exhausted clinicians.
As with all qualitative research studies, the findings of this study are influenced by the specific lines of inquiry that were pursued by the research team. The questions that the researchers asked during the interviews may have shaped the themes and insights that were expressed by the providers and may have influenced the implications of the study. This is important to consider when interpreting and applying the findings of the study.
Because the researchers did not continue to investigate the effects of psilocybin beyond the 32-week follow-up period, it is unknown whether the beneficial effects observed in the psilocybin group persist.
BOTTOM LINE
This qualitative study found that providers on hospital addiction consultation services find addiction medicine highly rewarding but also face numerous challenges that may contribute to burnout. Reducing factors that contribute to burnout (i.e., stigma) and promoting factors of resilience (i.e., education and advocacy) would likely improve the well-being of providers and thus facilitate improved care for patients with substance use disorders.
For individuals and families seeking recovery: Given that clinician burnout is linked to poorer service delivery and quality care, Individuals and families seeking treatment may benefit from selecting agencies that provide ongoing clinical training and advocacy and that adhere to the current best clinical practice standards as these may help reduce stigma and clinician burnout toward people with substance use disorders and thereby result in better quality care.
For treatment professionals and treatment systems: The findings from this study identified factors of burnout and resilience among addiction consultation services. Key aspects, such as stigma, likely impact addiction professionals across medical services and fields. Working to reduce stigma may be an effective way to reduce burnout. Facilitating advocacy campaigns targeting specific barriers (e.g., regulations of medications for opioid use disorder) may also increase resilience among participants of those campaigns. Interventions surrounding education, empathy, and contact with people with lived experience may also be needed to reduce factors of burnout. The language that is used also plays a central role in framing how society views substance use and recovery. RRI’s Addictionary® provides additional information on destigmatizing language. Moreover, team dynamics may contribute to burnout or resilience. Promoting team-based care may help reduce burnout and increase resilience.
For scientists:Burnout and resilience are complex, multifaceted constructs. So, exploring them and facilitating their reduction or amplification is not simple. Qualitative studies, such as this one, identify factors that warrant additional investigation. Findings from this study confer with others that hospital- and society-based barriers increase feelings of burnout. Key among them may be stigma. The limited community resources available to link patients to also emerged as an important barrier. Future studies might explore if more community resources (e.g., treatment centers, mutual-aid groups, recovery community centers) are empirically linked with lower burnout among addiction medicine providers. Additionally, education and advocacy work were seen to promote resilience. Future investigation might examine if providing education or participating in advocacy work quantitively improves resilience. Lastly, the magnitude of effect of team dynamics and the specific mechanisms that contribute to burnout or resilience may reveal if targeting team dynamics is effective and/or feasible to reduce burnout and improve resilience.
For policy makers: Findings from this study highlight multilevel barriers that contribute to burnout among hospital-based addiction consultation services such as over-regulation of medications for opioid use disorder and high levels of pressure from hospitals to discharge patients as quickly as possible. Hospital-based addiction consultation services have been found to improve patient outcomes. However, providers on these services may be more at risk of experiencing burnout. To maintain an effective work force and continue supporting patients with substance use disorders, policies that are informed by the most recent empirical evidence and those with lived experience may facilitate better patient outcomes and maintain addiction medicine providers in the workforce.
Substance use disorder patients make up 1 in 11 emergency department visits and 1 in 9 hospitalizations. Some of these visits may result from substance use disorder-related events (e.g., alcohol-related liver damage, endocarditis), while others may result from accidents not related to an individual’s substance use disorder (e.g., appendicitis, COVID-19). Identifying and capitalizing on opportunities to address substance use disorders in acute care settings in tandem with other medical concerns may be an important way to reduce time to treatment and reduce harms from substance use.
Despite the potential to address substance use during hospital stays, most medical staff do not have addiction medicine training or experience. Addiction consultation services are one intervention that has been shown to reduce addiction severity and increase abstinence as well as reduce 30-day readmission rates among patients with current or suspected substance use disorder being treated in a medical unit that does not directly address substance use disorder (e.g., for liver, cardiac, or pulmonary conditions, as examples). Addiction consultations services vary across hospitals, but they often initiate or link patients with pharmacotherapy services (e.g., buprenorphine, methadone), provide brief counseling, support aftercare planning, and connect patients directly to treatment following discharge. Members of these teams may include physicians, psychiatrists, psychologists, advanced practice nurses, social workers, recovery coaches, and peer workers.
Providers of addiction services may be more prone to burnout due to the complex social and behavioral needs of individuals with substance use disorder (SUD), as well as the high prevalence of trauma among this population. Burnout is a state of chronic physical and emotional exhaustion, accompanied by a lack of motivation and feelings of cynicism or detachment. Symptoms of burnout may include fatigue, difficulty concentrating, irritability, and a decreased ability to find enjoyment in work or other activities. In severe cases, burnout can lead to physical illness and may require time off work or other interventions to recover. Yet, addiction consultations teams may also exhibit resilience. Resilience is the ability to bounce back from adversity or difficult experiences, and to adapt and cope with challenges in a healthy and effective way. Resilience involves a range of skills and strategies, including the ability to manage stress, to maintain a positive outlook, to seek support when needed, and to learn from difficult experiences. Identifying factors associated with resilience and burnout among addiction service providers may provide possible targets for future interventions to best support providers in these unique and increasingly valuable roles.
HOW WAS THIS STUDY CONDUCTED?
This was a qualitative study that analyzed individual interviews with members of addiction consultations teams to identify factors associated with burnout and resilience among hospital-based addiction medicine providers. A total of 26 interviews with clinicians working on these teams were conducted representing 3 different provider types and 12 institutions. Interviews were conducted between October 2020 and March 2021.
For this study, the participants were healthcare providers who worked in hospitals and provided consultation services for addiction treatment. The researchers recruited these participants by contacting the directors of addiction consultation teams and through recommendations from the early participants (i.e., snowball sampling). The interviews with the participants focused on various aspects of their work, including the meaning they found in their work, how they balanced their work and personal lives, the demands and workload of their job, the efficiency and resources available to them, their level of control and flexibility, the support they received from colleagues and the organization, and the culture and values of the organization.
Twenty-six providers completed interviews representing 12 different academic hospitals across the country. Participants included 15 physicians, 8 social workers, and 3 advanced practice providers. Sixteen of the participants (64%) identified as female and 18 (72%) had at least 3 years of experience practicing in addiction medicine. Among the physicians, 11 (79%) were boarded in addiction medicine, and 10 (71%) were trained in internal medicine. Two physicians were trained in family medicine, and 2 others were trained in psychiatry. Most of the providers (75%) worked on other services (e.g., outpatient primary care, outpatient addiction medicine, etc.) in addition to the inpatient addiction consultation team. The others (25%) worked exclusively on the consultation team.
WHAT DID THIS STUDY FIND?
Persistent barriers contribute to burnout.
Providers identified barriers within the hospital and in the community. Within the hospital, providers felt pressured to discharge patients even if they did not have a solid plan to address the patient’s substance use disorder. High patient turnover in the inpatient setting also conflicted with the much slower pace of community programs. Additionally, hospital policies, such as those that limited prescribing medications for opioid use disorder (e.g., buprenorphine, methadone) frustrated staff and was viewed as problematic. The pressure to discharge patients alongside potentially limiting hospital policies contributed to feelings of burnout, especially when providers sought to change internal practices and policies. More generally, barriers such as limited community resources or long waitlists for addiction treatment left providers feeling frustrated at the lack of available resources for patients upon discharge.
Meaningful work confers resilience.
Hospital-based providers in the field of addiction medicine often found their work deeply rewarding through their non-judgmental care of patients and advocacy/education work within the hospital and in the community. Participants cited that providing such care to patients who may face discrimination or negative attitudes within the healthcare system due to their substance use can increase optimism in the field and be intrinsically motivating. Moreover, providers derived a sense of meaning through advocacy work and education within their institutions as well as within their broader communities. The sense of meaning and satisfaction found within addiction medicine were factors of resilience among these providers.
Team dynamics can influence burnout and resilience.
Members of addiction consultation teams expressed feelings of support from other members of their team. They valued working on interdisciplinary teams and felt doing so benefited patients and themselves. However, some providers were discouraged by negative dealings with other hospital staff. Negative interactions included other teams not acting on the addiction consultative team’s recommendations, perceived stigma, and when patients were discharged without an adequate care plan to address their substance use.
Stigma impacts burnout and sparks resilience.
Stigma appeared as a key component of burnout and resilience, and it was seen a mechanism that influenced team dynamics. Hospital-based and systemic barriers were believed to arise from stigma. Policies restricting effective medications, such as medications for opioid use disorder, were viewed as rooted in stigma and negatively impacted the care of patients with substance use disorders. Addiction service providers also felt intrinsic rewards when they were able to deliver patient-centered care to patients that experience intense stigma within the healthcare system. Advocacy and education were often done to address stigma within the hospital and in the community. For example, training future addiction medicine providers to reduce the stigmatization of patients with substance use disorders was perceived as an effective way to reduce stigma long-term. However, on-going exposure to stigma within the hospital and elsewhere was noted as contributing to burnout.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Hospital-based addiction consultation services have been shown to improve outcomes for patients with substance use disorder (e.g., fewer inpatient days, fewer emergency department visits). However, providers of these services may face heightened risk of burnout due to the complex social and behavioral needs of patients with substance use disorders. The findings from this study highlight how administrative and societal barriers may also increase burnout among these providers. However, the findings also highlight how practicing addiction medicine can support a sense of meaning and satisfaction. Team dynamics, within addiction consultation teams and between other hospital teams, can be supportive or discouraging. Maintaining a sustainable workforce will require reducing factors of burnout, increasing factors of resilience, and improving team dynamics.
Providers felt they were not always able to provide the effective, evidence-based care (e.g., medications for opioid use disorder) due to hospital and federal policies they viewed as rooted in stigma. Moreover, participants in the study witnessed the stigmatization of patients by other medical professionals, which further contribute to perceptions of burnout. Although providers derived meaning and value from providing patient-centered care in a non-judgmental way and educating their peers against stigmatizing beliefs and actions, providers also felt burdened by the sensed responsibility of reducing stigma within healthcare and the larger society. The findings from this study suggest that reducing stigma towards substance use disorders among all hospital providers may reduce burnout among providers of addiction services. Moreover, the findings showed that the meaning derived from addiction medicine work can promote resilience. Thus, uncovering ways to enhance the sense of meaning providers feel for the work (e.g., public recognition, patient feedback) may reduce burnout.
For example, one review of interventions with healthcare providers showed educational interventions can have positive effects and that interventions featuring contact with individuals with lived experience can enhance and sustain those positive changes. Additionally, changing the language used to describe people who use drugs and addiction may also effectively reduce stigma. For example, experimental research has shown that using the term “substance abuser” increases stigma compared with the person-first term “person with a substance use disorder.” The words and phrases that we use can influence the way that people perceive and understand these issues and can either reinforce or challenge stigma and negative stereotypes. It is important to use language that is respectful, accurate, and non-judgmental when discussing substance use and recovery. The Addictionary® is a resource developed by the Recovery Research Institute that provides guidance on using language that is inclusive and non-stigmatizing when discussing substance use and recovery. If you would like to learn more about destigmatizing language, you may find it helpful to consult the Addictionary®.
The study did not include non-clinical or peer workers with lived experiences, which may have minimized perceptions and experiences of burnout and/or resilience.
Participants were recruited via email and recommendations from early participants. Thus, the providers that self-selected to participate may have felt especially burned out or motivated by their experiences on addiction consultation services potentially skewing findings toward more exhausted clinicians.
As with all qualitative research studies, the findings of this study are influenced by the specific lines of inquiry that were pursued by the research team. The questions that the researchers asked during the interviews may have shaped the themes and insights that were expressed by the providers and may have influenced the implications of the study. This is important to consider when interpreting and applying the findings of the study.
Because the researchers did not continue to investigate the effects of psilocybin beyond the 32-week follow-up period, it is unknown whether the beneficial effects observed in the psilocybin group persist.
BOTTOM LINE
This qualitative study found that providers on hospital addiction consultation services find addiction medicine highly rewarding but also face numerous challenges that may contribute to burnout. Reducing factors that contribute to burnout (i.e., stigma) and promoting factors of resilience (i.e., education and advocacy) would likely improve the well-being of providers and thus facilitate improved care for patients with substance use disorders.
For individuals and families seeking recovery: Given that clinician burnout is linked to poorer service delivery and quality care, Individuals and families seeking treatment may benefit from selecting agencies that provide ongoing clinical training and advocacy and that adhere to the current best clinical practice standards as these may help reduce stigma and clinician burnout toward people with substance use disorders and thereby result in better quality care.
For treatment professionals and treatment systems: The findings from this study identified factors of burnout and resilience among addiction consultation services. Key aspects, such as stigma, likely impact addiction professionals across medical services and fields. Working to reduce stigma may be an effective way to reduce burnout. Facilitating advocacy campaigns targeting specific barriers (e.g., regulations of medications for opioid use disorder) may also increase resilience among participants of those campaigns. Interventions surrounding education, empathy, and contact with people with lived experience may also be needed to reduce factors of burnout. The language that is used also plays a central role in framing how society views substance use and recovery. RRI’s Addictionary® provides additional information on destigmatizing language. Moreover, team dynamics may contribute to burnout or resilience. Promoting team-based care may help reduce burnout and increase resilience.
For scientists:Burnout and resilience are complex, multifaceted constructs. So, exploring them and facilitating their reduction or amplification is not simple. Qualitative studies, such as this one, identify factors that warrant additional investigation. Findings from this study confer with others that hospital- and society-based barriers increase feelings of burnout. Key among them may be stigma. The limited community resources available to link patients to also emerged as an important barrier. Future studies might explore if more community resources (e.g., treatment centers, mutual-aid groups, recovery community centers) are empirically linked with lower burnout among addiction medicine providers. Additionally, education and advocacy work were seen to promote resilience. Future investigation might examine if providing education or participating in advocacy work quantitively improves resilience. Lastly, the magnitude of effect of team dynamics and the specific mechanisms that contribute to burnout or resilience may reveal if targeting team dynamics is effective and/or feasible to reduce burnout and improve resilience.
For policy makers: Findings from this study highlight multilevel barriers that contribute to burnout among hospital-based addiction consultation services such as over-regulation of medications for opioid use disorder and high levels of pressure from hospitals to discharge patients as quickly as possible. Hospital-based addiction consultation services have been found to improve patient outcomes. However, providers on these services may be more at risk of experiencing burnout. To maintain an effective work force and continue supporting patients with substance use disorders, policies that are informed by the most recent empirical evidence and those with lived experience may facilitate better patient outcomes and maintain addiction medicine providers in the workforce.
Substance use disorder patients make up 1 in 11 emergency department visits and 1 in 9 hospitalizations. Some of these visits may result from substance use disorder-related events (e.g., alcohol-related liver damage, endocarditis), while others may result from accidents not related to an individual’s substance use disorder (e.g., appendicitis, COVID-19). Identifying and capitalizing on opportunities to address substance use disorders in acute care settings in tandem with other medical concerns may be an important way to reduce time to treatment and reduce harms from substance use.
Despite the potential to address substance use during hospital stays, most medical staff do not have addiction medicine training or experience. Addiction consultation services are one intervention that has been shown to reduce addiction severity and increase abstinence as well as reduce 30-day readmission rates among patients with current or suspected substance use disorder being treated in a medical unit that does not directly address substance use disorder (e.g., for liver, cardiac, or pulmonary conditions, as examples). Addiction consultations services vary across hospitals, but they often initiate or link patients with pharmacotherapy services (e.g., buprenorphine, methadone), provide brief counseling, support aftercare planning, and connect patients directly to treatment following discharge. Members of these teams may include physicians, psychiatrists, psychologists, advanced practice nurses, social workers, recovery coaches, and peer workers.
Providers of addiction services may be more prone to burnout due to the complex social and behavioral needs of individuals with substance use disorder (SUD), as well as the high prevalence of trauma among this population. Burnout is a state of chronic physical and emotional exhaustion, accompanied by a lack of motivation and feelings of cynicism or detachment. Symptoms of burnout may include fatigue, difficulty concentrating, irritability, and a decreased ability to find enjoyment in work or other activities. In severe cases, burnout can lead to physical illness and may require time off work or other interventions to recover. Yet, addiction consultations teams may also exhibit resilience. Resilience is the ability to bounce back from adversity or difficult experiences, and to adapt and cope with challenges in a healthy and effective way. Resilience involves a range of skills and strategies, including the ability to manage stress, to maintain a positive outlook, to seek support when needed, and to learn from difficult experiences. Identifying factors associated with resilience and burnout among addiction service providers may provide possible targets for future interventions to best support providers in these unique and increasingly valuable roles.
HOW WAS THIS STUDY CONDUCTED?
This was a qualitative study that analyzed individual interviews with members of addiction consultations teams to identify factors associated with burnout and resilience among hospital-based addiction medicine providers. A total of 26 interviews with clinicians working on these teams were conducted representing 3 different provider types and 12 institutions. Interviews were conducted between October 2020 and March 2021.
For this study, the participants were healthcare providers who worked in hospitals and provided consultation services for addiction treatment. The researchers recruited these participants by contacting the directors of addiction consultation teams and through recommendations from the early participants (i.e., snowball sampling). The interviews with the participants focused on various aspects of their work, including the meaning they found in their work, how they balanced their work and personal lives, the demands and workload of their job, the efficiency and resources available to them, their level of control and flexibility, the support they received from colleagues and the organization, and the culture and values of the organization.
Twenty-six providers completed interviews representing 12 different academic hospitals across the country. Participants included 15 physicians, 8 social workers, and 3 advanced practice providers. Sixteen of the participants (64%) identified as female and 18 (72%) had at least 3 years of experience practicing in addiction medicine. Among the physicians, 11 (79%) were boarded in addiction medicine, and 10 (71%) were trained in internal medicine. Two physicians were trained in family medicine, and 2 others were trained in psychiatry. Most of the providers (75%) worked on other services (e.g., outpatient primary care, outpatient addiction medicine, etc.) in addition to the inpatient addiction consultation team. The others (25%) worked exclusively on the consultation team.
WHAT DID THIS STUDY FIND?
Persistent barriers contribute to burnout.
Providers identified barriers within the hospital and in the community. Within the hospital, providers felt pressured to discharge patients even if they did not have a solid plan to address the patient’s substance use disorder. High patient turnover in the inpatient setting also conflicted with the much slower pace of community programs. Additionally, hospital policies, such as those that limited prescribing medications for opioid use disorder (e.g., buprenorphine, methadone) frustrated staff and was viewed as problematic. The pressure to discharge patients alongside potentially limiting hospital policies contributed to feelings of burnout, especially when providers sought to change internal practices and policies. More generally, barriers such as limited community resources or long waitlists for addiction treatment left providers feeling frustrated at the lack of available resources for patients upon discharge.
Meaningful work confers resilience.
Hospital-based providers in the field of addiction medicine often found their work deeply rewarding through their non-judgmental care of patients and advocacy/education work within the hospital and in the community. Participants cited that providing such care to patients who may face discrimination or negative attitudes within the healthcare system due to their substance use can increase optimism in the field and be intrinsically motivating. Moreover, providers derived a sense of meaning through advocacy work and education within their institutions as well as within their broader communities. The sense of meaning and satisfaction found within addiction medicine were factors of resilience among these providers.
Team dynamics can influence burnout and resilience.
Members of addiction consultation teams expressed feelings of support from other members of their team. They valued working on interdisciplinary teams and felt doing so benefited patients and themselves. However, some providers were discouraged by negative dealings with other hospital staff. Negative interactions included other teams not acting on the addiction consultative team’s recommendations, perceived stigma, and when patients were discharged without an adequate care plan to address their substance use.
Stigma impacts burnout and sparks resilience.
Stigma appeared as a key component of burnout and resilience, and it was seen a mechanism that influenced team dynamics. Hospital-based and systemic barriers were believed to arise from stigma. Policies restricting effective medications, such as medications for opioid use disorder, were viewed as rooted in stigma and negatively impacted the care of patients with substance use disorders. Addiction service providers also felt intrinsic rewards when they were able to deliver patient-centered care to patients that experience intense stigma within the healthcare system. Advocacy and education were often done to address stigma within the hospital and in the community. For example, training future addiction medicine providers to reduce the stigmatization of patients with substance use disorders was perceived as an effective way to reduce stigma long-term. However, on-going exposure to stigma within the hospital and elsewhere was noted as contributing to burnout.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Hospital-based addiction consultation services have been shown to improve outcomes for patients with substance use disorder (e.g., fewer inpatient days, fewer emergency department visits). However, providers of these services may face heightened risk of burnout due to the complex social and behavioral needs of patients with substance use disorders. The findings from this study highlight how administrative and societal barriers may also increase burnout among these providers. However, the findings also highlight how practicing addiction medicine can support a sense of meaning and satisfaction. Team dynamics, within addiction consultation teams and between other hospital teams, can be supportive or discouraging. Maintaining a sustainable workforce will require reducing factors of burnout, increasing factors of resilience, and improving team dynamics.
Providers felt they were not always able to provide the effective, evidence-based care (e.g., medications for opioid use disorder) due to hospital and federal policies they viewed as rooted in stigma. Moreover, participants in the study witnessed the stigmatization of patients by other medical professionals, which further contribute to perceptions of burnout. Although providers derived meaning and value from providing patient-centered care in a non-judgmental way and educating their peers against stigmatizing beliefs and actions, providers also felt burdened by the sensed responsibility of reducing stigma within healthcare and the larger society. The findings from this study suggest that reducing stigma towards substance use disorders among all hospital providers may reduce burnout among providers of addiction services. Moreover, the findings showed that the meaning derived from addiction medicine work can promote resilience. Thus, uncovering ways to enhance the sense of meaning providers feel for the work (e.g., public recognition, patient feedback) may reduce burnout.
For example, one review of interventions with healthcare providers showed educational interventions can have positive effects and that interventions featuring contact with individuals with lived experience can enhance and sustain those positive changes. Additionally, changing the language used to describe people who use drugs and addiction may also effectively reduce stigma. For example, experimental research has shown that using the term “substance abuser” increases stigma compared with the person-first term “person with a substance use disorder.” The words and phrases that we use can influence the way that people perceive and understand these issues and can either reinforce or challenge stigma and negative stereotypes. It is important to use language that is respectful, accurate, and non-judgmental when discussing substance use and recovery. The Addictionary® is a resource developed by the Recovery Research Institute that provides guidance on using language that is inclusive and non-stigmatizing when discussing substance use and recovery. If you would like to learn more about destigmatizing language, you may find it helpful to consult the Addictionary®.
The study did not include non-clinical or peer workers with lived experiences, which may have minimized perceptions and experiences of burnout and/or resilience.
Participants were recruited via email and recommendations from early participants. Thus, the providers that self-selected to participate may have felt especially burned out or motivated by their experiences on addiction consultation services potentially skewing findings toward more exhausted clinicians.
As with all qualitative research studies, the findings of this study are influenced by the specific lines of inquiry that were pursued by the research team. The questions that the researchers asked during the interviews may have shaped the themes and insights that were expressed by the providers and may have influenced the implications of the study. This is important to consider when interpreting and applying the findings of the study.
Because the researchers did not continue to investigate the effects of psilocybin beyond the 32-week follow-up period, it is unknown whether the beneficial effects observed in the psilocybin group persist.
BOTTOM LINE
This qualitative study found that providers on hospital addiction consultation services find addiction medicine highly rewarding but also face numerous challenges that may contribute to burnout. Reducing factors that contribute to burnout (i.e., stigma) and promoting factors of resilience (i.e., education and advocacy) would likely improve the well-being of providers and thus facilitate improved care for patients with substance use disorders.
For individuals and families seeking recovery: Given that clinician burnout is linked to poorer service delivery and quality care, Individuals and families seeking treatment may benefit from selecting agencies that provide ongoing clinical training and advocacy and that adhere to the current best clinical practice standards as these may help reduce stigma and clinician burnout toward people with substance use disorders and thereby result in better quality care.
For treatment professionals and treatment systems: The findings from this study identified factors of burnout and resilience among addiction consultation services. Key aspects, such as stigma, likely impact addiction professionals across medical services and fields. Working to reduce stigma may be an effective way to reduce burnout. Facilitating advocacy campaigns targeting specific barriers (e.g., regulations of medications for opioid use disorder) may also increase resilience among participants of those campaigns. Interventions surrounding education, empathy, and contact with people with lived experience may also be needed to reduce factors of burnout. The language that is used also plays a central role in framing how society views substance use and recovery. RRI’s Addictionary® provides additional information on destigmatizing language. Moreover, team dynamics may contribute to burnout or resilience. Promoting team-based care may help reduce burnout and increase resilience.
For scientists:Burnout and resilience are complex, multifaceted constructs. So, exploring them and facilitating their reduction or amplification is not simple. Qualitative studies, such as this one, identify factors that warrant additional investigation. Findings from this study confer with others that hospital- and society-based barriers increase feelings of burnout. Key among them may be stigma. The limited community resources available to link patients to also emerged as an important barrier. Future studies might explore if more community resources (e.g., treatment centers, mutual-aid groups, recovery community centers) are empirically linked with lower burnout among addiction medicine providers. Additionally, education and advocacy work were seen to promote resilience. Future investigation might examine if providing education or participating in advocacy work quantitively improves resilience. Lastly, the magnitude of effect of team dynamics and the specific mechanisms that contribute to burnout or resilience may reveal if targeting team dynamics is effective and/or feasible to reduce burnout and improve resilience.
For policy makers: Findings from this study highlight multilevel barriers that contribute to burnout among hospital-based addiction consultation services such as over-regulation of medications for opioid use disorder and high levels of pressure from hospitals to discharge patients as quickly as possible. Hospital-based addiction consultation services have been found to improve patient outcomes. However, providers on these services may be more at risk of experiencing burnout. To maintain an effective work force and continue supporting patients with substance use disorders, policies that are informed by the most recent empirical evidence and those with lived experience may facilitate better patient outcomes and maintain addiction medicine providers in the workforce.