Peer recovery specialists – agents of stigma reduction?
Stigma toward methadone and buprenorphine may lead individuals to discontinue these life-saving medications. This study examined the multiple sources of stigma towards methadone, including racism, and explores the possible role of peer recovery specialists in reducing stigma’s impact.
Agonist medications for opioid use disorder- methadone, and buprenorphine – are effective treatments that reduce overdose mortality and harmful opioid use. Recommendations vary as to how long individuals should continue to take opioid disorder medications and research is currently limited. The consensus amongmanyexperts is that patients should continue treatment long-term, if not indefinitely.
Multiple studies show that the majority of people return to opioid use after stopping medication and retention on medication is associated with decreased risk of overdose and all-cause mortality. It is therefore noteworthy that retention on opioid use disorder medications is generally low, with discontinuation rates ranging from 20 to 80 percent of individuals depending on the study. There are several factors that likely contribute to low retention on these medications, including side-effects, recurrences of substance use (“relapses”), methadone treatment system restrictions, as well as housing and transport challenges.
Another addressable barrier may be the stigma people face who are taking these medications. Despite wide-spread acceptance that medication is a valid path of recovery by professionals, the perception still exists in some 12-step spaces, and among certain treatment providers as well as the general public that utilizing methadone or buprenorphine is “replacing one drug with another” and therefore not a genuine path of recovery.
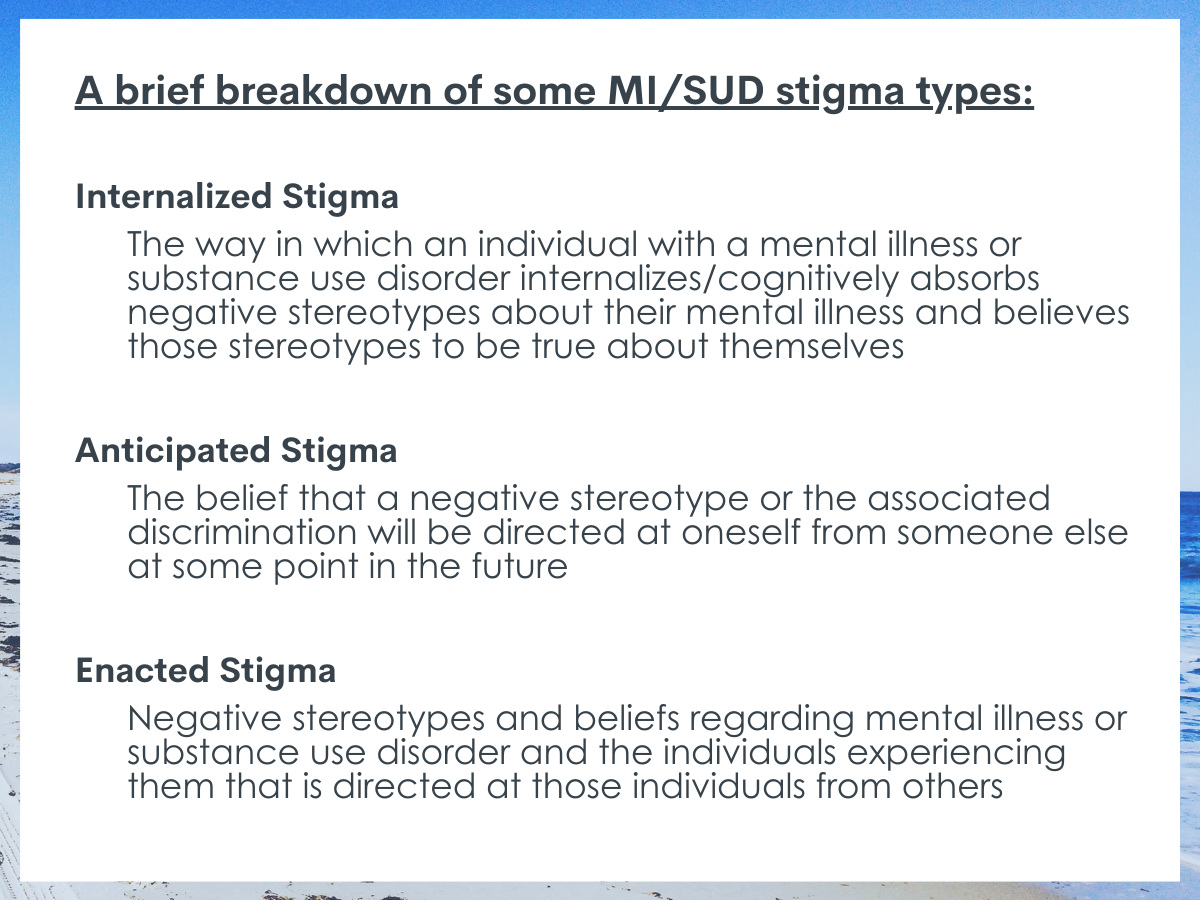
There is little research on how to reduce stigma against opioid use disorder medications. Particularly challenging is how to address internalized stigma: the process where individuals accept stereotypes and negative perceptions and apply them to themselves. One recent study suggests that self-stigma among methadone users may impact people’s quality of life and social functioning largely through their experience of psychological distress. This finding aligns with a recent literature review that concluded that, with the exception of one study that showed a direct impact of stigma on treatment outcomes, most studies found an indirect effect of stigma on treatment outcomes via negative emotions and cognitive mechanisms such as reducing self-efficacy, that is, confidence in one’s ability to overcome challenges.
Peer recovery support specialists may be able to help reduce stigma toward opioid use disorder medication, both within treatment organizations and internalized stigma, by leveraging their lived experiences of medication-supported recovery. Peer recovery specialists are individuals in long-term recovery who are professionally trained to offer non-clinical support to people in or seeking recovery from substance use disorders. They can act as role models, link individuals to services and recovery supports, provide education and emotional support, and advocate for patients within treatments systems.
This qualitative study of providers and largely African American clients at one Maryland treatment program explores sources of stigma towards methadone and solicited ideas from both providers and patients about how peer recovery specialist might help address stigma directed towards methadone treatment.
HOW WAS THIS STUDY CONDUCTED?
This qualitative study distilled findings from interviews with 20 patients enrolled in methadone treatment as the University of Maryland Drug Treatment Center, 8 staff members in the same program (including case managers, physicians, nurses, and counselors), and 4 peer recovery specialists from other Baltimore programs. Interviews were conducted between September 2019 and March 2020. Participants were given the option of either participating in focus groups or being interviewed individually (but not both).
The majority of patient participants identified as African American and male. The interview guide was developed in collaboration with peer recovery specialists and was adapted iteratively throughout the research process based on feedback from participants. Thematic analysis (a method used to code interview transcripts) was used to extract themes from interviews. It is important to note that qualitative research does not generally seek to make generalizations from the particular study group to larger populations or establish causal connections. Qualitative methods allow researchers to explore specific contexts or communities to generate theories, develop new research questions, refine concepts, or document complex social processes that are difficult to research through other methods.
WHAT DID THIS STUDY FIND?
Patients reported internalized stigma about both methadone treatment and opioid use disorder.
Participants expressed that they had somehow been permanently changed or ruined by substance use. They also described feeling abnormal as a result of their substance use and they hoped that treatment would restore them to normality. Some patients also expressed negative views of themselves because they were on methadone treatment, perceiving methadone as replacing “one drug by another.” Providers described patients, even as they are “bounding back” into society still feeling “less than” because of their methadone use or worrying that they are still getting “high” on methadone and therefore are not really “clean” (that is, in recovery). Other staff members reported that patients worried that they would not be seen as “clean” in abstinence based mutual-help groups (such as Narcotics Anonymous and other 12-step groups).
Patients described experiencing enacted stigma at multiple levels.
Patients experiencing enacted stigma from multiple sources, including from other patients, providers/staff, family members, and the larger community. These experiences of stigma separated into three levels: patient-level (internalized stigma/other patients, organizational-level (the treatment center), and societal level (government, family, community). Some patients in abstinence-based recovery described other patients who still used substances as not having “strong enough” willpower; others criticized patients who only used methadone to stave off withdrawals but continued using other drugs as misusing methadone. Multiple patients discussed experiences with one staff member that regularly referred to them as “junkies.” Some patients also described stigmatizing views from their families towards methadone treatment as a barrier to reaching their goals, including encouragement to discontinue treatment. Finally, patients and staff both described stigma regarding low socio-economic status, racial/ethnic minority status, methadone, and substance use disorder. Participants described powerful negative attitudes toward each of these four statuses as existing at a general societal level as well as negative comments regarding methadone by government officials.
Patients and staff identified several ways that peer recovery specialists might shift stigma.
Staff and patient participants suggested that the shared experience between peer recovery specialists and patients could help normalize the patient’s experience, undercutting stigma, while providing patients someone to talk with who understand their experience in ways that a counselor without lived experience may not. Participants also suggested that peer recovery specialists might provide patients with a person that they can disclose information to safely without judgement—that type of safe and healthy relationship might promote engagement in treatment. Staff participants stated that many patients come into treatment with limited information around methadone treatment specifically. Staff members postulated peer recovery specialists might orient new patients to treatment and reduce misunderstandings, stigma, and confusion. Finally, staff and peer recovery specialist participants suggested that peer recovery specialists, by providing a model of someone in recovery contributing to the treatment center, might help reduce stigma within the organization.
Some peer specialists might reinforce stigma.
One patient respondent expressed the concern that peer recovery specialists with “differences in recovery paths” could cause the patient to feel like the peer recovery specialist is “looking down on them”. This concern may be connected with earlier expressions of judgement by patients practicing abstinence-based recovery towards patients that are still using or concerns by patients that they may not be seen as “clean” (i.e., genuinely in recovery) within 12-step mutual-help contexts.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study investigated the experiences of stigma among low-income, predominantly African American men in methadone treatment at one Maryland treatment center. In keeping with other studies, this study found that stigma regarding both substance use disorders and methadone operates on multiple levels, ranging from remarks by other patients and staff to broader social stereotypes voiced by family members and city officials. Staff members described a broader web of negative social attitudes towards individuals who are economically disadvantaged, African American or Latino, and on methadone. Future research should build on this work to better understand how these multiple levels interact in different contexts and influence treatment retention and outcomes. Given that stigma operates at multiple levels, it follows that strategies to combat stigma must intervene on each of these levels.
Participants and staff also underlined the ability of peer recovery specialists to create healthy relationships with clients, which they may not have in other aspects of their life and provide a safe space for clients to disclose where they will not encounter negative judgement. Staff participants, especially, stressed the potential role of peer recovery specialists in educating clients, emphasizing that patients often enter their program with little knowledge and much misinformation about methadone treatment. Peer recovery specialists from other programs spoke to the potential for the employment of people in recovery within treatment programs to challenge organizational stigma. By demonstrating the value of people in recovery to the organization, peer recovery specialists—according to some participants—may help challenge misconceptions among staff and demonstrate the value of lived experience, encouraging staff to perceive potential contributions of clients as well.
That being said, stigma may be one of the more difficult obstacles to ameliorate. Working closely with a person in recovery would be considered a “contact intervention,” that is, firsthand exposure to members of a stigmatized group. While one recent systematic review found that contact interventions did have some impact on stigma among providers, this was based on a relatively small number of studies, the majority of which were low-quality. It is important to emphasize that contact interventions seem to be successful only under certain conditions: members of the stigmatized group must have equal status, share goals with the contact group, and support from those with power or authority. Substantial institutional support for the goal of reducing stigma would likely be required for the presence of a peer specialist to result in a meaningful impact. Also of note is that short-term stigma interventions appear to produce short-term results. In this respect, the continual presence of peer-recovery specialists in organizations might lead to better results than standard interventions, although research would need to test this hypothesis.
One limitation of this study is that the authors did not develop a clear set of criteria that differentiated between negative judgements reflecting stigma and negative judgements reflecting personal experience or other sociocultural influences. The level of stigma encountered by people in methadone treatment, especially economically disadvantaged people who experience racism, is well documented. At the same time, stigma is not the only possible explanation for negative judgements about substance use disorder or methadone treatment. In some cases, study participants appeared to be making observations about negative impacts of substance use or methadone on their own lives, for example about the long-term cognitive effects of substance use. Future qualitative work in the area could inform interventions to enhance methadone engagement and retention by separating judgments linked to stigma from other reasons underlying negative perceptions of medication. For example, there is a history of suspicion about methadone in some African American communities that reflects racism and racial disparities in addiction treatment and medical care more broadly. These views might better be understood as medical mistrust; classifying them as stigma risks mischaracterizing responses that are more likely due to historical and contemporary racism.
The peer recovery specialists interviewed were not employed at the main study site but were recruited from other Maryland treatment programs. Given that that the main study site does not appear to employ peer recovery specialists, it is not clear what participant statements about the potential impact of peer recovery specialists on stigma are based on.
Influential critiques of the “attitudinal fallacy” in qualitative methodology have warned about the limits of utilizing semistructured interviews for making inferences about behaviors and social contexts without either additional observations or analytic justification. One potential shortfall is that basing analysis solely on semistructured interviews or focus groups might classify negative attitudes as stigma that, when their expression is analyzed within a broader social or institutional context, may be better understood as medical mistrust, or reflecting cultural beliefs, such as spirituality.
BOTTOM LINE
Agonist medications for opioid use disorder, such as methadone and buprenorphine, are effective treatments and reduce overdose mortality and opioid use. Individuals in methadone treatment, however, often face stigma from other people in recovery, family members, providers, and the broader public. This qualitative study of largely African American patients and providers at a Maryland treatment clinic found that people on methadone experience stigma from multiple sources, including family, other patients, providers, and in the media. It also underlined that methadone related stigma is compounded byotherforms of prejudice, including racism, perceptions that associate methadone with lower socio-economic status, and stigma against the medication itself. While further research is required, this study also suggests that employing peer recovery specialists with lived experience of medication-supported recovery may help reduce stigma by providing positive, non-judgmental role models and challenging prejudice against agonist medications within treatment organizations.
For individuals and families seeking recovery: While there are many reasons people may discontinue opioid use disorder medications, stigma (especially the idea that treatment with methadone or buprenorphine is “replacing one drug with another”) is a prominent concern. Addiction is a biopsychosocial illness and the use of medications to treat addiction is similar to using medications to treat other chronic illnesses. Medication assisted recovery is widely recognized as a valid pathway of recovery by addiction professionals and embraced in many parts of the recovery community. This study suggests that working with peer recovery specialists may help reduce stigma by providing positive, non-judgmental role models and a safe relationship for people taking opioid use disorder medications to talk about their experiences.
For treatment professionals and treatment systems: Patients facing multiple forms of stigma may require additional support. While the potential role of peer recovery specialists in counteracting stigma requires further research, the patients and staff interviewed in this article identify several areas where they may help with retaining patients on opioid use disorder medication, including by providing positive examples of people who have achieved long-term recovery using medications, building supportive and non-judgmental relationships based on common experience, and challenging stereotypes about methadone-supported recovery among both patients and staff.
For scientists:This qualitative study of providers and largely African American men in a Maryland methadone treatment program highlights several important directions for future research. First, it raises questions about the potential role of stigma from family, providers, other patients, and mutual-help groups in producing high levels of discontinuation from medications for opioid use disorder despite their established effectiveness. Second, it points to a potential role for peer recovery specialists working in methadone treatment programs in reducing stigma and promoting increased retention in treatment. Third, it underlines a general trend in research on stigma towards viewing stigma against substance use disorders as intersecting and interacting with other forms of social marginalization, such a racism, which can increase the overall burden associated with stigma. Thus, it raises useful questions about how such intersections can be modelled and accounted for in intervention design. Given the established effectiveness of medications for OUD and the high rates of discontinuation, all three areas are urgent directions for future research.
For policy makers: In the context of regulatory changes to methadone treatment introduced during COVID-19, advocates have argued for decreasing barriers to methadone treatment through expanding pharmacy or primary practice-based distribution, as well as increasing the amount of “take home” doses, as a way to increase retention. This qualitative study points to the possible strategy of employing peer recovery specialists (people with lived experience and training to provide non-clinical support) in order to reduce stigma and increase treatment retention.
CITATIONS
Anvari, M. S., Kleinman, M. B., Massey, E. C., Bradley, V. D., Felton, J. W., Belcher, A. M., & Magidson, J. F. (2022). “In their mind, they always felt less than”: The role of peers in shifting stigma as a barrier to opioid use disorder treatment retention. Journal of Substance Abuse Treatment, 138. doi: 10.1016/j.jsat.2022.108721
Agonist medications for opioid use disorder- methadone, and buprenorphine – are effective treatments that reduce overdose mortality and harmful opioid use. Recommendations vary as to how long individuals should continue to take opioid disorder medications and research is currently limited. The consensus amongmanyexperts is that patients should continue treatment long-term, if not indefinitely.
Multiple studies show that the majority of people return to opioid use after stopping medication and retention on medication is associated with decreased risk of overdose and all-cause mortality. It is therefore noteworthy that retention on opioid use disorder medications is generally low, with discontinuation rates ranging from 20 to 80 percent of individuals depending on the study. There are several factors that likely contribute to low retention on these medications, including side-effects, recurrences of substance use (“relapses”), methadone treatment system restrictions, as well as housing and transport challenges.
Another addressable barrier may be the stigma people face who are taking these medications. Despite wide-spread acceptance that medication is a valid path of recovery by professionals, the perception still exists in some 12-step spaces, and among certain treatment providers as well as the general public that utilizing methadone or buprenorphine is “replacing one drug with another” and therefore not a genuine path of recovery.
There is little research on how to reduce stigma against opioid use disorder medications. Particularly challenging is how to address internalized stigma: the process where individuals accept stereotypes and negative perceptions and apply them to themselves. One recent study suggests that self-stigma among methadone users may impact people’s quality of life and social functioning largely through their experience of psychological distress. This finding aligns with a recent literature review that concluded that, with the exception of one study that showed a direct impact of stigma on treatment outcomes, most studies found an indirect effect of stigma on treatment outcomes via negative emotions and cognitive mechanisms such as reducing self-efficacy, that is, confidence in one’s ability to overcome challenges.
Peer recovery support specialists may be able to help reduce stigma toward opioid use disorder medication, both within treatment organizations and internalized stigma, by leveraging their lived experiences of medication-supported recovery. Peer recovery specialists are individuals in long-term recovery who are professionally trained to offer non-clinical support to people in or seeking recovery from substance use disorders. They can act as role models, link individuals to services and recovery supports, provide education and emotional support, and advocate for patients within treatments systems.
This qualitative study of providers and largely African American clients at one Maryland treatment program explores sources of stigma towards methadone and solicited ideas from both providers and patients about how peer recovery specialist might help address stigma directed towards methadone treatment.
HOW WAS THIS STUDY CONDUCTED?
This qualitative study distilled findings from interviews with 20 patients enrolled in methadone treatment as the University of Maryland Drug Treatment Center, 8 staff members in the same program (including case managers, physicians, nurses, and counselors), and 4 peer recovery specialists from other Baltimore programs. Interviews were conducted between September 2019 and March 2020. Participants were given the option of either participating in focus groups or being interviewed individually (but not both).
The majority of patient participants identified as African American and male. The interview guide was developed in collaboration with peer recovery specialists and was adapted iteratively throughout the research process based on feedback from participants. Thematic analysis (a method used to code interview transcripts) was used to extract themes from interviews. It is important to note that qualitative research does not generally seek to make generalizations from the particular study group to larger populations or establish causal connections. Qualitative methods allow researchers to explore specific contexts or communities to generate theories, develop new research questions, refine concepts, or document complex social processes that are difficult to research through other methods.
WHAT DID THIS STUDY FIND?
Patients reported internalized stigma about both methadone treatment and opioid use disorder.
Participants expressed that they had somehow been permanently changed or ruined by substance use. They also described feeling abnormal as a result of their substance use and they hoped that treatment would restore them to normality. Some patients also expressed negative views of themselves because they were on methadone treatment, perceiving methadone as replacing “one drug by another.” Providers described patients, even as they are “bounding back” into society still feeling “less than” because of their methadone use or worrying that they are still getting “high” on methadone and therefore are not really “clean” (that is, in recovery). Other staff members reported that patients worried that they would not be seen as “clean” in abstinence based mutual-help groups (such as Narcotics Anonymous and other 12-step groups).
Patients described experiencing enacted stigma at multiple levels.
Patients experiencing enacted stigma from multiple sources, including from other patients, providers/staff, family members, and the larger community. These experiences of stigma separated into three levels: patient-level (internalized stigma/other patients, organizational-level (the treatment center), and societal level (government, family, community). Some patients in abstinence-based recovery described other patients who still used substances as not having “strong enough” willpower; others criticized patients who only used methadone to stave off withdrawals but continued using other drugs as misusing methadone. Multiple patients discussed experiences with one staff member that regularly referred to them as “junkies.” Some patients also described stigmatizing views from their families towards methadone treatment as a barrier to reaching their goals, including encouragement to discontinue treatment. Finally, patients and staff both described stigma regarding low socio-economic status, racial/ethnic minority status, methadone, and substance use disorder. Participants described powerful negative attitudes toward each of these four statuses as existing at a general societal level as well as negative comments regarding methadone by government officials.
Patients and staff identified several ways that peer recovery specialists might shift stigma.
Staff and patient participants suggested that the shared experience between peer recovery specialists and patients could help normalize the patient’s experience, undercutting stigma, while providing patients someone to talk with who understand their experience in ways that a counselor without lived experience may not. Participants also suggested that peer recovery specialists might provide patients with a person that they can disclose information to safely without judgement—that type of safe and healthy relationship might promote engagement in treatment. Staff participants stated that many patients come into treatment with limited information around methadone treatment specifically. Staff members postulated peer recovery specialists might orient new patients to treatment and reduce misunderstandings, stigma, and confusion. Finally, staff and peer recovery specialist participants suggested that peer recovery specialists, by providing a model of someone in recovery contributing to the treatment center, might help reduce stigma within the organization.
Some peer specialists might reinforce stigma.
One patient respondent expressed the concern that peer recovery specialists with “differences in recovery paths” could cause the patient to feel like the peer recovery specialist is “looking down on them”. This concern may be connected with earlier expressions of judgement by patients practicing abstinence-based recovery towards patients that are still using or concerns by patients that they may not be seen as “clean” (i.e., genuinely in recovery) within 12-step mutual-help contexts.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study investigated the experiences of stigma among low-income, predominantly African American men in methadone treatment at one Maryland treatment center. In keeping with other studies, this study found that stigma regarding both substance use disorders and methadone operates on multiple levels, ranging from remarks by other patients and staff to broader social stereotypes voiced by family members and city officials. Staff members described a broader web of negative social attitudes towards individuals who are economically disadvantaged, African American or Latino, and on methadone. Future research should build on this work to better understand how these multiple levels interact in different contexts and influence treatment retention and outcomes. Given that stigma operates at multiple levels, it follows that strategies to combat stigma must intervene on each of these levels.
Participants and staff also underlined the ability of peer recovery specialists to create healthy relationships with clients, which they may not have in other aspects of their life and provide a safe space for clients to disclose where they will not encounter negative judgement. Staff participants, especially, stressed the potential role of peer recovery specialists in educating clients, emphasizing that patients often enter their program with little knowledge and much misinformation about methadone treatment. Peer recovery specialists from other programs spoke to the potential for the employment of people in recovery within treatment programs to challenge organizational stigma. By demonstrating the value of people in recovery to the organization, peer recovery specialists—according to some participants—may help challenge misconceptions among staff and demonstrate the value of lived experience, encouraging staff to perceive potential contributions of clients as well.
That being said, stigma may be one of the more difficult obstacles to ameliorate. Working closely with a person in recovery would be considered a “contact intervention,” that is, firsthand exposure to members of a stigmatized group. While one recent systematic review found that contact interventions did have some impact on stigma among providers, this was based on a relatively small number of studies, the majority of which were low-quality. It is important to emphasize that contact interventions seem to be successful only under certain conditions: members of the stigmatized group must have equal status, share goals with the contact group, and support from those with power or authority. Substantial institutional support for the goal of reducing stigma would likely be required for the presence of a peer specialist to result in a meaningful impact. Also of note is that short-term stigma interventions appear to produce short-term results. In this respect, the continual presence of peer-recovery specialists in organizations might lead to better results than standard interventions, although research would need to test this hypothesis.
One limitation of this study is that the authors did not develop a clear set of criteria that differentiated between negative judgements reflecting stigma and negative judgements reflecting personal experience or other sociocultural influences. The level of stigma encountered by people in methadone treatment, especially economically disadvantaged people who experience racism, is well documented. At the same time, stigma is not the only possible explanation for negative judgements about substance use disorder or methadone treatment. In some cases, study participants appeared to be making observations about negative impacts of substance use or methadone on their own lives, for example about the long-term cognitive effects of substance use. Future qualitative work in the area could inform interventions to enhance methadone engagement and retention by separating judgments linked to stigma from other reasons underlying negative perceptions of medication. For example, there is a history of suspicion about methadone in some African American communities that reflects racism and racial disparities in addiction treatment and medical care more broadly. These views might better be understood as medical mistrust; classifying them as stigma risks mischaracterizing responses that are more likely due to historical and contemporary racism.
The peer recovery specialists interviewed were not employed at the main study site but were recruited from other Maryland treatment programs. Given that that the main study site does not appear to employ peer recovery specialists, it is not clear what participant statements about the potential impact of peer recovery specialists on stigma are based on.
Influential critiques of the “attitudinal fallacy” in qualitative methodology have warned about the limits of utilizing semistructured interviews for making inferences about behaviors and social contexts without either additional observations or analytic justification. One potential shortfall is that basing analysis solely on semistructured interviews or focus groups might classify negative attitudes as stigma that, when their expression is analyzed within a broader social or institutional context, may be better understood as medical mistrust, or reflecting cultural beliefs, such as spirituality.
BOTTOM LINE
Agonist medications for opioid use disorder, such as methadone and buprenorphine, are effective treatments and reduce overdose mortality and opioid use. Individuals in methadone treatment, however, often face stigma from other people in recovery, family members, providers, and the broader public. This qualitative study of largely African American patients and providers at a Maryland treatment clinic found that people on methadone experience stigma from multiple sources, including family, other patients, providers, and in the media. It also underlined that methadone related stigma is compounded byotherforms of prejudice, including racism, perceptions that associate methadone with lower socio-economic status, and stigma against the medication itself. While further research is required, this study also suggests that employing peer recovery specialists with lived experience of medication-supported recovery may help reduce stigma by providing positive, non-judgmental role models and challenging prejudice against agonist medications within treatment organizations.
For individuals and families seeking recovery: While there are many reasons people may discontinue opioid use disorder medications, stigma (especially the idea that treatment with methadone or buprenorphine is “replacing one drug with another”) is a prominent concern. Addiction is a biopsychosocial illness and the use of medications to treat addiction is similar to using medications to treat other chronic illnesses. Medication assisted recovery is widely recognized as a valid pathway of recovery by addiction professionals and embraced in many parts of the recovery community. This study suggests that working with peer recovery specialists may help reduce stigma by providing positive, non-judgmental role models and a safe relationship for people taking opioid use disorder medications to talk about their experiences.
For treatment professionals and treatment systems: Patients facing multiple forms of stigma may require additional support. While the potential role of peer recovery specialists in counteracting stigma requires further research, the patients and staff interviewed in this article identify several areas where they may help with retaining patients on opioid use disorder medication, including by providing positive examples of people who have achieved long-term recovery using medications, building supportive and non-judgmental relationships based on common experience, and challenging stereotypes about methadone-supported recovery among both patients and staff.
For scientists:This qualitative study of providers and largely African American men in a Maryland methadone treatment program highlights several important directions for future research. First, it raises questions about the potential role of stigma from family, providers, other patients, and mutual-help groups in producing high levels of discontinuation from medications for opioid use disorder despite their established effectiveness. Second, it points to a potential role for peer recovery specialists working in methadone treatment programs in reducing stigma and promoting increased retention in treatment. Third, it underlines a general trend in research on stigma towards viewing stigma against substance use disorders as intersecting and interacting with other forms of social marginalization, such a racism, which can increase the overall burden associated with stigma. Thus, it raises useful questions about how such intersections can be modelled and accounted for in intervention design. Given the established effectiveness of medications for OUD and the high rates of discontinuation, all three areas are urgent directions for future research.
For policy makers: In the context of regulatory changes to methadone treatment introduced during COVID-19, advocates have argued for decreasing barriers to methadone treatment through expanding pharmacy or primary practice-based distribution, as well as increasing the amount of “take home” doses, as a way to increase retention. This qualitative study points to the possible strategy of employing peer recovery specialists (people with lived experience and training to provide non-clinical support) in order to reduce stigma and increase treatment retention.
CITATIONS
Anvari, M. S., Kleinman, M. B., Massey, E. C., Bradley, V. D., Felton, J. W., Belcher, A. M., & Magidson, J. F. (2022). “In their mind, they always felt less than”: The role of peers in shifting stigma as a barrier to opioid use disorder treatment retention. Journal of Substance Abuse Treatment, 138. doi: 10.1016/j.jsat.2022.108721
Agonist medications for opioid use disorder- methadone, and buprenorphine – are effective treatments that reduce overdose mortality and harmful opioid use. Recommendations vary as to how long individuals should continue to take opioid disorder medications and research is currently limited. The consensus amongmanyexperts is that patients should continue treatment long-term, if not indefinitely.
Multiple studies show that the majority of people return to opioid use after stopping medication and retention on medication is associated with decreased risk of overdose and all-cause mortality. It is therefore noteworthy that retention on opioid use disorder medications is generally low, with discontinuation rates ranging from 20 to 80 percent of individuals depending on the study. There are several factors that likely contribute to low retention on these medications, including side-effects, recurrences of substance use (“relapses”), methadone treatment system restrictions, as well as housing and transport challenges.
Another addressable barrier may be the stigma people face who are taking these medications. Despite wide-spread acceptance that medication is a valid path of recovery by professionals, the perception still exists in some 12-step spaces, and among certain treatment providers as well as the general public that utilizing methadone or buprenorphine is “replacing one drug with another” and therefore not a genuine path of recovery.
There is little research on how to reduce stigma against opioid use disorder medications. Particularly challenging is how to address internalized stigma: the process where individuals accept stereotypes and negative perceptions and apply them to themselves. One recent study suggests that self-stigma among methadone users may impact people’s quality of life and social functioning largely through their experience of psychological distress. This finding aligns with a recent literature review that concluded that, with the exception of one study that showed a direct impact of stigma on treatment outcomes, most studies found an indirect effect of stigma on treatment outcomes via negative emotions and cognitive mechanisms such as reducing self-efficacy, that is, confidence in one’s ability to overcome challenges.
Peer recovery support specialists may be able to help reduce stigma toward opioid use disorder medication, both within treatment organizations and internalized stigma, by leveraging their lived experiences of medication-supported recovery. Peer recovery specialists are individuals in long-term recovery who are professionally trained to offer non-clinical support to people in or seeking recovery from substance use disorders. They can act as role models, link individuals to services and recovery supports, provide education and emotional support, and advocate for patients within treatments systems.
This qualitative study of providers and largely African American clients at one Maryland treatment program explores sources of stigma towards methadone and solicited ideas from both providers and patients about how peer recovery specialist might help address stigma directed towards methadone treatment.
HOW WAS THIS STUDY CONDUCTED?
This qualitative study distilled findings from interviews with 20 patients enrolled in methadone treatment as the University of Maryland Drug Treatment Center, 8 staff members in the same program (including case managers, physicians, nurses, and counselors), and 4 peer recovery specialists from other Baltimore programs. Interviews were conducted between September 2019 and March 2020. Participants were given the option of either participating in focus groups or being interviewed individually (but not both).
The majority of patient participants identified as African American and male. The interview guide was developed in collaboration with peer recovery specialists and was adapted iteratively throughout the research process based on feedback from participants. Thematic analysis (a method used to code interview transcripts) was used to extract themes from interviews. It is important to note that qualitative research does not generally seek to make generalizations from the particular study group to larger populations or establish causal connections. Qualitative methods allow researchers to explore specific contexts or communities to generate theories, develop new research questions, refine concepts, or document complex social processes that are difficult to research through other methods.
WHAT DID THIS STUDY FIND?
Patients reported internalized stigma about both methadone treatment and opioid use disorder.
Participants expressed that they had somehow been permanently changed or ruined by substance use. They also described feeling abnormal as a result of their substance use and they hoped that treatment would restore them to normality. Some patients also expressed negative views of themselves because they were on methadone treatment, perceiving methadone as replacing “one drug by another.” Providers described patients, even as they are “bounding back” into society still feeling “less than” because of their methadone use or worrying that they are still getting “high” on methadone and therefore are not really “clean” (that is, in recovery). Other staff members reported that patients worried that they would not be seen as “clean” in abstinence based mutual-help groups (such as Narcotics Anonymous and other 12-step groups).
Patients described experiencing enacted stigma at multiple levels.
Patients experiencing enacted stigma from multiple sources, including from other patients, providers/staff, family members, and the larger community. These experiences of stigma separated into three levels: patient-level (internalized stigma/other patients, organizational-level (the treatment center), and societal level (government, family, community). Some patients in abstinence-based recovery described other patients who still used substances as not having “strong enough” willpower; others criticized patients who only used methadone to stave off withdrawals but continued using other drugs as misusing methadone. Multiple patients discussed experiences with one staff member that regularly referred to them as “junkies.” Some patients also described stigmatizing views from their families towards methadone treatment as a barrier to reaching their goals, including encouragement to discontinue treatment. Finally, patients and staff both described stigma regarding low socio-economic status, racial/ethnic minority status, methadone, and substance use disorder. Participants described powerful negative attitudes toward each of these four statuses as existing at a general societal level as well as negative comments regarding methadone by government officials.
Patients and staff identified several ways that peer recovery specialists might shift stigma.
Staff and patient participants suggested that the shared experience between peer recovery specialists and patients could help normalize the patient’s experience, undercutting stigma, while providing patients someone to talk with who understand their experience in ways that a counselor without lived experience may not. Participants also suggested that peer recovery specialists might provide patients with a person that they can disclose information to safely without judgement—that type of safe and healthy relationship might promote engagement in treatment. Staff participants stated that many patients come into treatment with limited information around methadone treatment specifically. Staff members postulated peer recovery specialists might orient new patients to treatment and reduce misunderstandings, stigma, and confusion. Finally, staff and peer recovery specialist participants suggested that peer recovery specialists, by providing a model of someone in recovery contributing to the treatment center, might help reduce stigma within the organization.
Some peer specialists might reinforce stigma.
One patient respondent expressed the concern that peer recovery specialists with “differences in recovery paths” could cause the patient to feel like the peer recovery specialist is “looking down on them”. This concern may be connected with earlier expressions of judgement by patients practicing abstinence-based recovery towards patients that are still using or concerns by patients that they may not be seen as “clean” (i.e., genuinely in recovery) within 12-step mutual-help contexts.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study investigated the experiences of stigma among low-income, predominantly African American men in methadone treatment at one Maryland treatment center. In keeping with other studies, this study found that stigma regarding both substance use disorders and methadone operates on multiple levels, ranging from remarks by other patients and staff to broader social stereotypes voiced by family members and city officials. Staff members described a broader web of negative social attitudes towards individuals who are economically disadvantaged, African American or Latino, and on methadone. Future research should build on this work to better understand how these multiple levels interact in different contexts and influence treatment retention and outcomes. Given that stigma operates at multiple levels, it follows that strategies to combat stigma must intervene on each of these levels.
Participants and staff also underlined the ability of peer recovery specialists to create healthy relationships with clients, which they may not have in other aspects of their life and provide a safe space for clients to disclose where they will not encounter negative judgement. Staff participants, especially, stressed the potential role of peer recovery specialists in educating clients, emphasizing that patients often enter their program with little knowledge and much misinformation about methadone treatment. Peer recovery specialists from other programs spoke to the potential for the employment of people in recovery within treatment programs to challenge organizational stigma. By demonstrating the value of people in recovery to the organization, peer recovery specialists—according to some participants—may help challenge misconceptions among staff and demonstrate the value of lived experience, encouraging staff to perceive potential contributions of clients as well.
That being said, stigma may be one of the more difficult obstacles to ameliorate. Working closely with a person in recovery would be considered a “contact intervention,” that is, firsthand exposure to members of a stigmatized group. While one recent systematic review found that contact interventions did have some impact on stigma among providers, this was based on a relatively small number of studies, the majority of which were low-quality. It is important to emphasize that contact interventions seem to be successful only under certain conditions: members of the stigmatized group must have equal status, share goals with the contact group, and support from those with power or authority. Substantial institutional support for the goal of reducing stigma would likely be required for the presence of a peer specialist to result in a meaningful impact. Also of note is that short-term stigma interventions appear to produce short-term results. In this respect, the continual presence of peer-recovery specialists in organizations might lead to better results than standard interventions, although research would need to test this hypothesis.
One limitation of this study is that the authors did not develop a clear set of criteria that differentiated between negative judgements reflecting stigma and negative judgements reflecting personal experience or other sociocultural influences. The level of stigma encountered by people in methadone treatment, especially economically disadvantaged people who experience racism, is well documented. At the same time, stigma is not the only possible explanation for negative judgements about substance use disorder or methadone treatment. In some cases, study participants appeared to be making observations about negative impacts of substance use or methadone on their own lives, for example about the long-term cognitive effects of substance use. Future qualitative work in the area could inform interventions to enhance methadone engagement and retention by separating judgments linked to stigma from other reasons underlying negative perceptions of medication. For example, there is a history of suspicion about methadone in some African American communities that reflects racism and racial disparities in addiction treatment and medical care more broadly. These views might better be understood as medical mistrust; classifying them as stigma risks mischaracterizing responses that are more likely due to historical and contemporary racism.
The peer recovery specialists interviewed were not employed at the main study site but were recruited from other Maryland treatment programs. Given that that the main study site does not appear to employ peer recovery specialists, it is not clear what participant statements about the potential impact of peer recovery specialists on stigma are based on.
Influential critiques of the “attitudinal fallacy” in qualitative methodology have warned about the limits of utilizing semistructured interviews for making inferences about behaviors and social contexts without either additional observations or analytic justification. One potential shortfall is that basing analysis solely on semistructured interviews or focus groups might classify negative attitudes as stigma that, when their expression is analyzed within a broader social or institutional context, may be better understood as medical mistrust, or reflecting cultural beliefs, such as spirituality.
BOTTOM LINE
Agonist medications for opioid use disorder, such as methadone and buprenorphine, are effective treatments and reduce overdose mortality and opioid use. Individuals in methadone treatment, however, often face stigma from other people in recovery, family members, providers, and the broader public. This qualitative study of largely African American patients and providers at a Maryland treatment clinic found that people on methadone experience stigma from multiple sources, including family, other patients, providers, and in the media. It also underlined that methadone related stigma is compounded byotherforms of prejudice, including racism, perceptions that associate methadone with lower socio-economic status, and stigma against the medication itself. While further research is required, this study also suggests that employing peer recovery specialists with lived experience of medication-supported recovery may help reduce stigma by providing positive, non-judgmental role models and challenging prejudice against agonist medications within treatment organizations.
For individuals and families seeking recovery: While there are many reasons people may discontinue opioid use disorder medications, stigma (especially the idea that treatment with methadone or buprenorphine is “replacing one drug with another”) is a prominent concern. Addiction is a biopsychosocial illness and the use of medications to treat addiction is similar to using medications to treat other chronic illnesses. Medication assisted recovery is widely recognized as a valid pathway of recovery by addiction professionals and embraced in many parts of the recovery community. This study suggests that working with peer recovery specialists may help reduce stigma by providing positive, non-judgmental role models and a safe relationship for people taking opioid use disorder medications to talk about their experiences.
For treatment professionals and treatment systems: Patients facing multiple forms of stigma may require additional support. While the potential role of peer recovery specialists in counteracting stigma requires further research, the patients and staff interviewed in this article identify several areas where they may help with retaining patients on opioid use disorder medication, including by providing positive examples of people who have achieved long-term recovery using medications, building supportive and non-judgmental relationships based on common experience, and challenging stereotypes about methadone-supported recovery among both patients and staff.
For scientists:This qualitative study of providers and largely African American men in a Maryland methadone treatment program highlights several important directions for future research. First, it raises questions about the potential role of stigma from family, providers, other patients, and mutual-help groups in producing high levels of discontinuation from medications for opioid use disorder despite their established effectiveness. Second, it points to a potential role for peer recovery specialists working in methadone treatment programs in reducing stigma and promoting increased retention in treatment. Third, it underlines a general trend in research on stigma towards viewing stigma against substance use disorders as intersecting and interacting with other forms of social marginalization, such a racism, which can increase the overall burden associated with stigma. Thus, it raises useful questions about how such intersections can be modelled and accounted for in intervention design. Given the established effectiveness of medications for OUD and the high rates of discontinuation, all three areas are urgent directions for future research.
For policy makers: In the context of regulatory changes to methadone treatment introduced during COVID-19, advocates have argued for decreasing barriers to methadone treatment through expanding pharmacy or primary practice-based distribution, as well as increasing the amount of “take home” doses, as a way to increase retention. This qualitative study points to the possible strategy of employing peer recovery specialists (people with lived experience and training to provide non-clinical support) in order to reduce stigma and increase treatment retention.
CITATIONS
Anvari, M. S., Kleinman, M. B., Massey, E. C., Bradley, V. D., Felton, J. W., Belcher, A. M., & Magidson, J. F. (2022). “In their mind, they always felt less than”: The role of peers in shifting stigma as a barrier to opioid use disorder treatment retention. Journal of Substance Abuse Treatment, 138. doi: 10.1016/j.jsat.2022.108721