Peer recovery coaching reduces reliance on acute healthcare
Peer support specialists, also called “recovery coaches,” are individuals who have personal lived experience with substance use conditions and who have undergone training to support others experiencing similar challenges. This study examined health care utilization over time for patients receiving recovery coaching alongside other treatment compared to a matched group of participants receiving only outpatient treatment.
This study examined the transformative potential of peer support services, which leverage the lived experiences of individuals in recovery. By doing so, the study aims to address the challenges of maintaining continuity of care for individuals with substance use disorders following acute care interventions, such as hospitalization or withdrawal management. Specifically, the study investigates how peer support services can enhance treatment engagement, reduce rates of rehospitalization, and promote sustained recovery within the community.
HOW WAS THIS STUDY CONDUCTED?
The researchers used insurance claims data to compare acute care service utilization for either mental health or substance use for individuals receiving peer recovery support services versus those receiving outpatient treatment (and no peer recovery support) after an initial episode of hospitalization or medically supervised withdrawal management. The peer recovery support group could have received concurrent outpatient treatment. The study included adults aged 18 to 64 who had received a minimum of 2 paid claims for peer support for substance use disorder services within the Behavioral Health Managed Care Organization’s provider network during the period spanning from January 1, 2016, to December 31, 2019. These peer support services were provided by 11 different substance use disorder agencies across the state of Pennsylvania.
To establish meaningful comparisons, the researchers formed a comparison group of 698 individuals. This group comprised Medicaid-enrolled adults who received outpatient substance use disorder services within the provider network during the same study period. The researchers used a statistical technique commonly used in health services research to enhance matching precision and reduce bias so that the comparison group closely matched those in the study sample (those who received peer support) in terms of age, gender, race/ethnicity, diagnosis, and inpatient mental health and SUD services in the 90 days before the index episode of recovery support or, for the comparison, outpatient treatment.
“Service episodes” were periods during which individuals received peer support for substance use disorder or outpatient substance use disorder services. The start date of each episode was determined as the date of the first paid claim following a 90-day period with no paid claims for peer support for substance use disorder (in the study sample) or outpatient substance use disorder (in the comparison sample). The end date was considered as the date of the last paid claim before another 90-day period with no claims. In cases where individuals had multiple service episodes during the study period, only the first episode was considered for analysis.
The researchers found 2,667 people who had received treatment for substance use disorder during the study. Most of them were women (52.1%), of European American ethnicity (80.2%), and not of Hispanic background (96.9%). Most of those seeking substance use disorder services (75.0%) were under 45 years old. It is important to note that many participants (78.1%) seeking substance use disorder treatment also had a mental health diagnosis. Among those with both kinds of diagnoses, the researchers found that 72.2% had serious mental illnesses, 71% dealt with conditions like depression or anxiety, and 18.7% had diagnoses like attention deficit disorder. Peer support associated with greater reduction in acute care.
WHAT DID THIS STUDY FIND?
Fewer emergency and acute care visits for those receiving peer support.
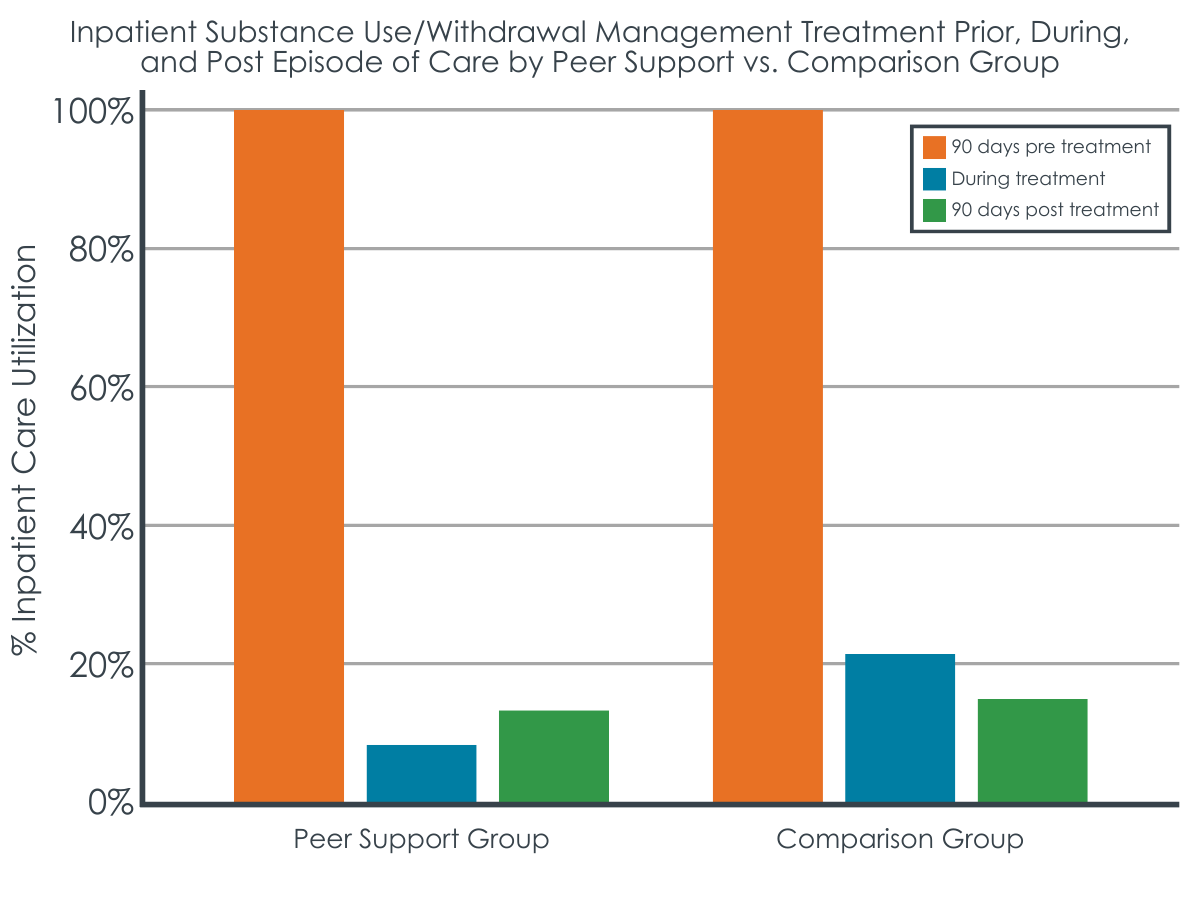
Individuals engaging with peer support alongside other treatments experienced fewer emergency and acute care visits, with 8.6%, compared to 21.2% in the group only receiving outpatient services . Importantly, this improved outcome was maintained in the 90 days following the end of peer support.
Enhanced engagement with community services.
Post-discharge, individuals from the peer support group were more likely to stay connected with community-based services. About 45% continued receiving outpatient SUD services, compared to 49% in the outpatient alone group. 31.8% of the peer support group engaged with outpatient mental health services , compared to 35.7% in the outpatient alone group, highlighting the role of peer support in fostering continued care and support networks.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined how individuals on Medicaid, seeking support for substance use and mental health challenges, utilize substance use and other behavioral health services over time. People receiving peer support, where individuals with lived experience provide assistance, tended to use inpatient services less often whereby a following hospitalization for a significant substance use event, engaging with peer support is linked to reduced subsequent inpatient service use. This finding is significant because it suggests that connecting with peer support immediately after a crisis can help people stay engaged in community-based care, which is often preferable from both individual (e.g., functioning) and societal (e.g., cost) perspectives.
Also, even though many individuals only received peer support for a short time (e.g., 1 or fewer months was the most common “dose” received), positive changes in service use were observed, including a reduced utilization of inpatient services and an increased connection to community-based care after discharge. This suggests that even a minimal engagement with peer support can have a beneficial impact on the continuity of care for individuals recovering from substance use events.
This study differs from earlier research by showing lower healthcare utilization for those with peer support compared to those without, particularly in terms of substance use services like rehabilitation and halfway houses.
One limitation is that this study did not use direct observation or other assessments to determine the specific elements of peer support services. It also did not examine how peers worked together with outpatient clinicians and counselors in a team-based approach. This means we do not have a detailed understanding of how these services were provided.
Another limitation is that the people receiving peer support were also getting other therapeutic services, including outpatient substance use disorder treatment, which the comparison group all received. Without randomization (a more controlled study design), the study cannot say that peer support directly caused the outcomes observed.
Additionally, this study relied on data from insurance claims, which did not provide information about individuals’ level of functioning or other characteristics that might have affected how they used services. This is important because it could mean that the groups being compared may not have been comparable in different ways.
Findings are based on data from Pennsylvania, which has a well-established behavioral health system. These results might not apply to areas with fewer services or different populations.
BOTTOM LINE
Peer support services for substance use disorder may help lower acute care utilization and enhanced connections to community-based services following discharge. While findings are consistent with potential benefits in promoting effective treatment and care continuity, the study did not examine substance use and other recovery outcomes. Future research is needed to determine the effects of peer recovery support specialist services on substance use and other recovery outcomes.
For individuals and families seeking recovery: For individuals and families seeking recovery, results here provide hope and practical guidance. They underscore the potential importance of considering peer support services as a key part of the recovery process. These services, delivered by individuals who have personally overcome similar challenges, offer a unique source of encouragement, understanding, and connection. Engaging with peer support may lead to reduced likelihood of hospitalization and better access to community-based care.
For treatment professionals and treatment systems: This study underscores the potential for peer support services to enhance the overall effectiveness of substance use disorder and mental health treatment programs. Treatment providers may consider integrating peer support specialists into their teams, leading potentially to more comprehensive and patient-centered care, addressing the complex needs of individuals dealing with substance use disorders and mental health challenges.
For scientists: This study offers insights into the real-world impact of peer support services in the context of substance use disorder and mental health treatment. It highlights the need for further investigation into the impact of peer support services on substance use and recovery capital.
For policy makers: Integrating peer support services into health care systems may reduce utilization of costly acute care services while promoting better linkage to community-based care. This suggests that policy initiatives aimed at expanding and reimbursing peer support services, similar to what has been done for Medicaid-funded mental health services in Pennsylvania, could yield positive outcomes. Policy makers should also consider strategies to enhance training, supervision, and resources for peer programs, which could ultimately lead to improved access and outcomes for individuals seeking recovery that is likely to be highly cost-effective.
This study examined the transformative potential of peer support services, which leverage the lived experiences of individuals in recovery. By doing so, the study aims to address the challenges of maintaining continuity of care for individuals with substance use disorders following acute care interventions, such as hospitalization or withdrawal management. Specifically, the study investigates how peer support services can enhance treatment engagement, reduce rates of rehospitalization, and promote sustained recovery within the community.
HOW WAS THIS STUDY CONDUCTED?
The researchers used insurance claims data to compare acute care service utilization for either mental health or substance use for individuals receiving peer recovery support services versus those receiving outpatient treatment (and no peer recovery support) after an initial episode of hospitalization or medically supervised withdrawal management. The peer recovery support group could have received concurrent outpatient treatment. The study included adults aged 18 to 64 who had received a minimum of 2 paid claims for peer support for substance use disorder services within the Behavioral Health Managed Care Organization’s provider network during the period spanning from January 1, 2016, to December 31, 2019. These peer support services were provided by 11 different substance use disorder agencies across the state of Pennsylvania.
To establish meaningful comparisons, the researchers formed a comparison group of 698 individuals. This group comprised Medicaid-enrolled adults who received outpatient substance use disorder services within the provider network during the same study period. The researchers used a statistical technique commonly used in health services research to enhance matching precision and reduce bias so that the comparison group closely matched those in the study sample (those who received peer support) in terms of age, gender, race/ethnicity, diagnosis, and inpatient mental health and SUD services in the 90 days before the index episode of recovery support or, for the comparison, outpatient treatment.
“Service episodes” were periods during which individuals received peer support for substance use disorder or outpatient substance use disorder services. The start date of each episode was determined as the date of the first paid claim following a 90-day period with no paid claims for peer support for substance use disorder (in the study sample) or outpatient substance use disorder (in the comparison sample). The end date was considered as the date of the last paid claim before another 90-day period with no claims. In cases where individuals had multiple service episodes during the study period, only the first episode was considered for analysis.
The researchers found 2,667 people who had received treatment for substance use disorder during the study. Most of them were women (52.1%), of European American ethnicity (80.2%), and not of Hispanic background (96.9%). Most of those seeking substance use disorder services (75.0%) were under 45 years old. It is important to note that many participants (78.1%) seeking substance use disorder treatment also had a mental health diagnosis. Among those with both kinds of diagnoses, the researchers found that 72.2% had serious mental illnesses, 71% dealt with conditions like depression or anxiety, and 18.7% had diagnoses like attention deficit disorder. Peer support associated with greater reduction in acute care.
WHAT DID THIS STUDY FIND?
Fewer emergency and acute care visits for those receiving peer support.
Individuals engaging with peer support alongside other treatments experienced fewer emergency and acute care visits, with 8.6%, compared to 21.2% in the group only receiving outpatient services . Importantly, this improved outcome was maintained in the 90 days following the end of peer support.
Enhanced engagement with community services.
Post-discharge, individuals from the peer support group were more likely to stay connected with community-based services. About 45% continued receiving outpatient SUD services, compared to 49% in the outpatient alone group. 31.8% of the peer support group engaged with outpatient mental health services , compared to 35.7% in the outpatient alone group, highlighting the role of peer support in fostering continued care and support networks.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined how individuals on Medicaid, seeking support for substance use and mental health challenges, utilize substance use and other behavioral health services over time. People receiving peer support, where individuals with lived experience provide assistance, tended to use inpatient services less often whereby a following hospitalization for a significant substance use event, engaging with peer support is linked to reduced subsequent inpatient service use. This finding is significant because it suggests that connecting with peer support immediately after a crisis can help people stay engaged in community-based care, which is often preferable from both individual (e.g., functioning) and societal (e.g., cost) perspectives.
Also, even though many individuals only received peer support for a short time (e.g., 1 or fewer months was the most common “dose” received), positive changes in service use were observed, including a reduced utilization of inpatient services and an increased connection to community-based care after discharge. This suggests that even a minimal engagement with peer support can have a beneficial impact on the continuity of care for individuals recovering from substance use events.
This study differs from earlier research by showing lower healthcare utilization for those with peer support compared to those without, particularly in terms of substance use services like rehabilitation and halfway houses.
One limitation is that this study did not use direct observation or other assessments to determine the specific elements of peer support services. It also did not examine how peers worked together with outpatient clinicians and counselors in a team-based approach. This means we do not have a detailed understanding of how these services were provided.
Another limitation is that the people receiving peer support were also getting other therapeutic services, including outpatient substance use disorder treatment, which the comparison group all received. Without randomization (a more controlled study design), the study cannot say that peer support directly caused the outcomes observed.
Additionally, this study relied on data from insurance claims, which did not provide information about individuals’ level of functioning or other characteristics that might have affected how they used services. This is important because it could mean that the groups being compared may not have been comparable in different ways.
Findings are based on data from Pennsylvania, which has a well-established behavioral health system. These results might not apply to areas with fewer services or different populations.
BOTTOM LINE
Peer support services for substance use disorder may help lower acute care utilization and enhanced connections to community-based services following discharge. While findings are consistent with potential benefits in promoting effective treatment and care continuity, the study did not examine substance use and other recovery outcomes. Future research is needed to determine the effects of peer recovery support specialist services on substance use and other recovery outcomes.
For individuals and families seeking recovery: For individuals and families seeking recovery, results here provide hope and practical guidance. They underscore the potential importance of considering peer support services as a key part of the recovery process. These services, delivered by individuals who have personally overcome similar challenges, offer a unique source of encouragement, understanding, and connection. Engaging with peer support may lead to reduced likelihood of hospitalization and better access to community-based care.
For treatment professionals and treatment systems: This study underscores the potential for peer support services to enhance the overall effectiveness of substance use disorder and mental health treatment programs. Treatment providers may consider integrating peer support specialists into their teams, leading potentially to more comprehensive and patient-centered care, addressing the complex needs of individuals dealing with substance use disorders and mental health challenges.
For scientists: This study offers insights into the real-world impact of peer support services in the context of substance use disorder and mental health treatment. It highlights the need for further investigation into the impact of peer support services on substance use and recovery capital.
For policy makers: Integrating peer support services into health care systems may reduce utilization of costly acute care services while promoting better linkage to community-based care. This suggests that policy initiatives aimed at expanding and reimbursing peer support services, similar to what has been done for Medicaid-funded mental health services in Pennsylvania, could yield positive outcomes. Policy makers should also consider strategies to enhance training, supervision, and resources for peer programs, which could ultimately lead to improved access and outcomes for individuals seeking recovery that is likely to be highly cost-effective.
This study examined the transformative potential of peer support services, which leverage the lived experiences of individuals in recovery. By doing so, the study aims to address the challenges of maintaining continuity of care for individuals with substance use disorders following acute care interventions, such as hospitalization or withdrawal management. Specifically, the study investigates how peer support services can enhance treatment engagement, reduce rates of rehospitalization, and promote sustained recovery within the community.
HOW WAS THIS STUDY CONDUCTED?
The researchers used insurance claims data to compare acute care service utilization for either mental health or substance use for individuals receiving peer recovery support services versus those receiving outpatient treatment (and no peer recovery support) after an initial episode of hospitalization or medically supervised withdrawal management. The peer recovery support group could have received concurrent outpatient treatment. The study included adults aged 18 to 64 who had received a minimum of 2 paid claims for peer support for substance use disorder services within the Behavioral Health Managed Care Organization’s provider network during the period spanning from January 1, 2016, to December 31, 2019. These peer support services were provided by 11 different substance use disorder agencies across the state of Pennsylvania.
To establish meaningful comparisons, the researchers formed a comparison group of 698 individuals. This group comprised Medicaid-enrolled adults who received outpatient substance use disorder services within the provider network during the same study period. The researchers used a statistical technique commonly used in health services research to enhance matching precision and reduce bias so that the comparison group closely matched those in the study sample (those who received peer support) in terms of age, gender, race/ethnicity, diagnosis, and inpatient mental health and SUD services in the 90 days before the index episode of recovery support or, for the comparison, outpatient treatment.
“Service episodes” were periods during which individuals received peer support for substance use disorder or outpatient substance use disorder services. The start date of each episode was determined as the date of the first paid claim following a 90-day period with no paid claims for peer support for substance use disorder (in the study sample) or outpatient substance use disorder (in the comparison sample). The end date was considered as the date of the last paid claim before another 90-day period with no claims. In cases where individuals had multiple service episodes during the study period, only the first episode was considered for analysis.
The researchers found 2,667 people who had received treatment for substance use disorder during the study. Most of them were women (52.1%), of European American ethnicity (80.2%), and not of Hispanic background (96.9%). Most of those seeking substance use disorder services (75.0%) were under 45 years old. It is important to note that many participants (78.1%) seeking substance use disorder treatment also had a mental health diagnosis. Among those with both kinds of diagnoses, the researchers found that 72.2% had serious mental illnesses, 71% dealt with conditions like depression or anxiety, and 18.7% had diagnoses like attention deficit disorder. Peer support associated with greater reduction in acute care.
WHAT DID THIS STUDY FIND?
Fewer emergency and acute care visits for those receiving peer support.
Individuals engaging with peer support alongside other treatments experienced fewer emergency and acute care visits, with 8.6%, compared to 21.2% in the group only receiving outpatient services . Importantly, this improved outcome was maintained in the 90 days following the end of peer support.
Enhanced engagement with community services.
Post-discharge, individuals from the peer support group were more likely to stay connected with community-based services. About 45% continued receiving outpatient SUD services, compared to 49% in the outpatient alone group. 31.8% of the peer support group engaged with outpatient mental health services , compared to 35.7% in the outpatient alone group, highlighting the role of peer support in fostering continued care and support networks.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study examined how individuals on Medicaid, seeking support for substance use and mental health challenges, utilize substance use and other behavioral health services over time. People receiving peer support, where individuals with lived experience provide assistance, tended to use inpatient services less often whereby a following hospitalization for a significant substance use event, engaging with peer support is linked to reduced subsequent inpatient service use. This finding is significant because it suggests that connecting with peer support immediately after a crisis can help people stay engaged in community-based care, which is often preferable from both individual (e.g., functioning) and societal (e.g., cost) perspectives.
Also, even though many individuals only received peer support for a short time (e.g., 1 or fewer months was the most common “dose” received), positive changes in service use were observed, including a reduced utilization of inpatient services and an increased connection to community-based care after discharge. This suggests that even a minimal engagement with peer support can have a beneficial impact on the continuity of care for individuals recovering from substance use events.
This study differs from earlier research by showing lower healthcare utilization for those with peer support compared to those without, particularly in terms of substance use services like rehabilitation and halfway houses.
One limitation is that this study did not use direct observation or other assessments to determine the specific elements of peer support services. It also did not examine how peers worked together with outpatient clinicians and counselors in a team-based approach. This means we do not have a detailed understanding of how these services were provided.
Another limitation is that the people receiving peer support were also getting other therapeutic services, including outpatient substance use disorder treatment, which the comparison group all received. Without randomization (a more controlled study design), the study cannot say that peer support directly caused the outcomes observed.
Additionally, this study relied on data from insurance claims, which did not provide information about individuals’ level of functioning or other characteristics that might have affected how they used services. This is important because it could mean that the groups being compared may not have been comparable in different ways.
Findings are based on data from Pennsylvania, which has a well-established behavioral health system. These results might not apply to areas with fewer services or different populations.
BOTTOM LINE
Peer support services for substance use disorder may help lower acute care utilization and enhanced connections to community-based services following discharge. While findings are consistent with potential benefits in promoting effective treatment and care continuity, the study did not examine substance use and other recovery outcomes. Future research is needed to determine the effects of peer recovery support specialist services on substance use and other recovery outcomes.
For individuals and families seeking recovery: For individuals and families seeking recovery, results here provide hope and practical guidance. They underscore the potential importance of considering peer support services as a key part of the recovery process. These services, delivered by individuals who have personally overcome similar challenges, offer a unique source of encouragement, understanding, and connection. Engaging with peer support may lead to reduced likelihood of hospitalization and better access to community-based care.
For treatment professionals and treatment systems: This study underscores the potential for peer support services to enhance the overall effectiveness of substance use disorder and mental health treatment programs. Treatment providers may consider integrating peer support specialists into their teams, leading potentially to more comprehensive and patient-centered care, addressing the complex needs of individuals dealing with substance use disorders and mental health challenges.
For scientists: This study offers insights into the real-world impact of peer support services in the context of substance use disorder and mental health treatment. It highlights the need for further investigation into the impact of peer support services on substance use and recovery capital.
For policy makers: Integrating peer support services into health care systems may reduce utilization of costly acute care services while promoting better linkage to community-based care. This suggests that policy initiatives aimed at expanding and reimbursing peer support services, similar to what has been done for Medicaid-funded mental health services in Pennsylvania, could yield positive outcomes. Policy makers should also consider strategies to enhance training, supervision, and resources for peer programs, which could ultimately lead to improved access and outcomes for individuals seeking recovery that is likely to be highly cost-effective.