To disclose or not to disclose (opioid use disorder history)
Sharing information about one’s addiction history (i.e., disclosure) might benefit individuals interpersonally but could also pose risks. In this study, researchers characterized disclosure goals among individuals receiving opioid use disorder treatment, whether certain disclosure goals were associated with future disclosure to loved ones, and the quality of their relationships after such disclosure.
Interpersonal relationships and social support play important roles in the recovery process. Positive social support is associated with positive changes and behaviors that facilitate recovery, such as reduced substance use disorder severity and better treatment retention. One potential way to enhance social support is by disclosing or sharing information about one’s substance use disorder history, treatment, and recovery. However, disclosing this information might make individuals vulnerable to experiencing stigma and discrimination (e.g., mistreatment), which is associated with treatment drop-out and ongoing substance misuse.
One component of disclosure that has yet to be studied among individuals with opioid use disorder is disclosure goals. Different reasons for disclosing one’s recovery status are thought to influence whether a person will actually disclose and how they go about disclosing, as well as their relationship and health outcomes after they disclose to others.
Disclosure goals consist of approach goals (pursuing desirable outcomes of disclosure like social support and feelings of social closeness) and avoidance goals (avoiding undesirable outcomes of disclosure like experiencing stigma or mistreatment). Whereas approach goals are linked to an increased likelihood of disclosing and more desirable responses among those who are disclosed to (providing more trust/social support), avoidance goals are linked to more social conflict and distant relationships. This study characterized disclosure goals among individuals receiving treatment for opioid use disorder and examined whether these goals are associated with future acts of disclosure and relationship outcomes after disclosure (i.e., social support, relationship closeness, and the experience of unfair treatment by others, also known as enacted stigma).
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal naturalistic investigation of adult outpatients receiving medication for opioid use disorder in the state of Delaware, in which patients completed qualitative interviews and questionnaires about their disclosure plans and social relationships over the course of three months. Individuals were recruited between 2018 and 2019 from 2 behavioral health clinics, including 1 suburban clinic and 1 urban clinic. All participants planned to disclose their substance use disorder history and/or treatment for the first time to at least 1 person (i.e. disclosure recipient) within the 3-month study timeframe.
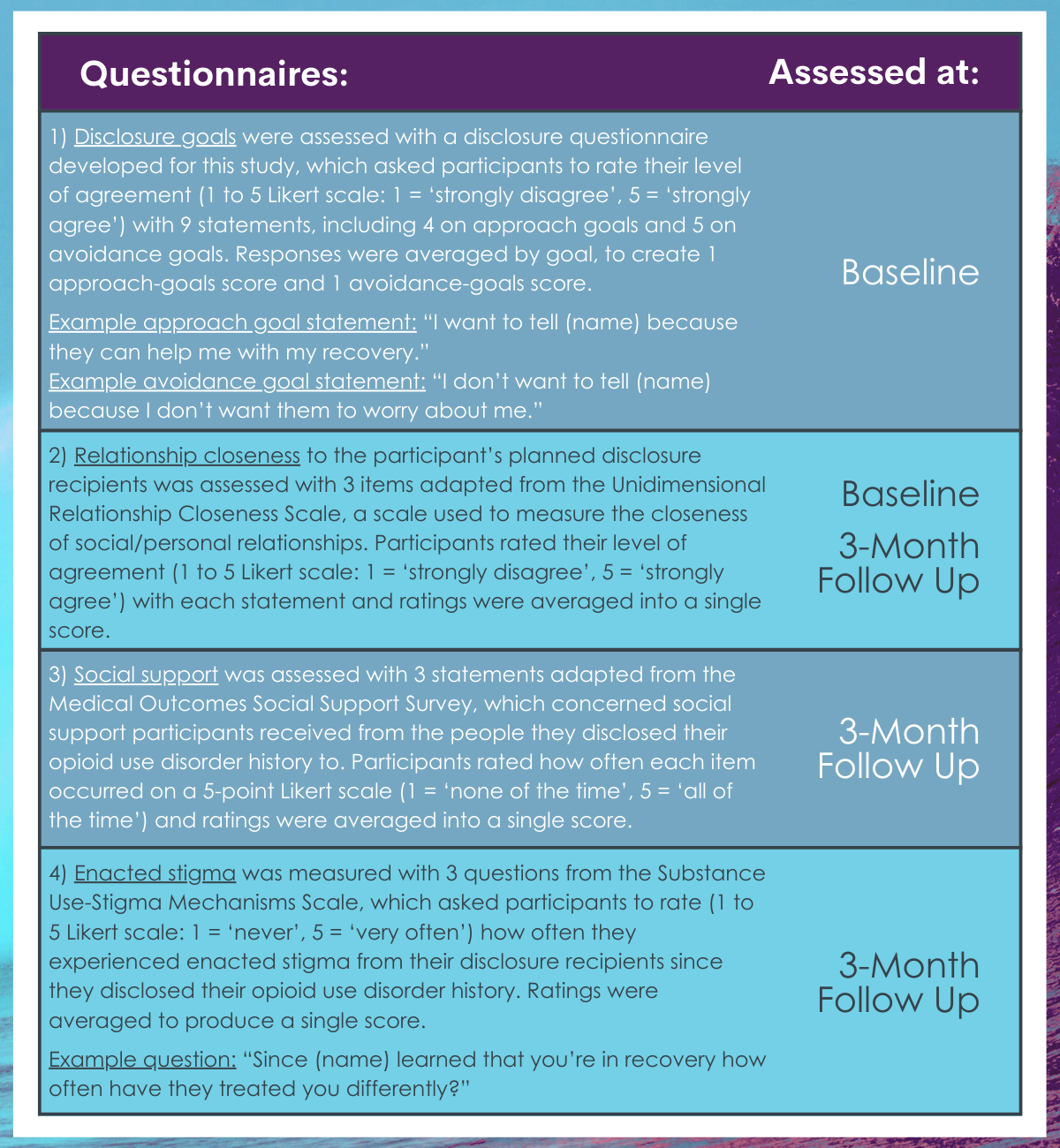
The initial study assessments examined disclosure goals and relationship status before disclosure via qualitative interviews and questionnaires. At the 3-month follow up, participants completed questionnaires about their relationship status with disclosure recipients after they had disclosed their opioid use disorder history. During the initial interview assessments, participants answered questions regarding plans to disclose to up to 3 people. Interviews asked about: (1) approach goals (i.e., their reasons to disclose) and (2) avoidance goals (i.e., their reasons to not disclose). Questionnaires at baseline and follow up concerned 4 topics: (1) disclosure goals, (2) relationship closeness to disclosure recipients, (3) social support from disclosure recipients, and (4) enacted stigma from disclosure recipients.
Participants completed four questionnaires regarding disclosure goals, relationship closeness, social support, and enacted stigma.
Qualitative baseline interviews were analyzed and reasons to disclose and not to disclose were identified. Predictors of participant’s disclosing within 3-months were examined among those who completed the follow-up assessment. Predictors of social support, relationship closeness, and enacted stigma were examined among individuals who disclosed their opioid use disorder history. Predictors for both analyses included disclosure-goal scores on the disclosure questionnaire (approach & avoidance) and relationship closeness at baseline, controlling for all other variables (e.g., demographics, recovery factors). Analyses also examined the potential influence of socio-demographic (e.g., race, age) and recovery (e.g., recovery duration) factors.
One hundred and forty-six individuals participated in the initial study session, of which 124 (85%) completed the month-3 follow up. All participants were undergoing methadone (87%) or buprenorphine (13%) treatment for opioid use disorder. On average, participants reported being in recovery for 4 years (range: 0 to 32 years). The majority of participants were White (75%), middle-aged (average: 40 years old), unemployed (64%) patients attending a suburban treatment clinic (65%), with a history of incarceration (70%) and, consistent with their current treatment participation, had mild opioid dependence, on average, according to the Leeds Dependence Questionnaire. About half of the participants were women (53%). On average, participants planned to disclose to one person, and this was most commonly a parent (22%), friend (16%), or sibling (10%).
WHAT DID THIS STUDY FIND?
Approach goals for planned disclosures included a desire for recovery support, honesty, amends, and education of loved ones, while avoidance goals included fear of judgement privacy, and concern for others.
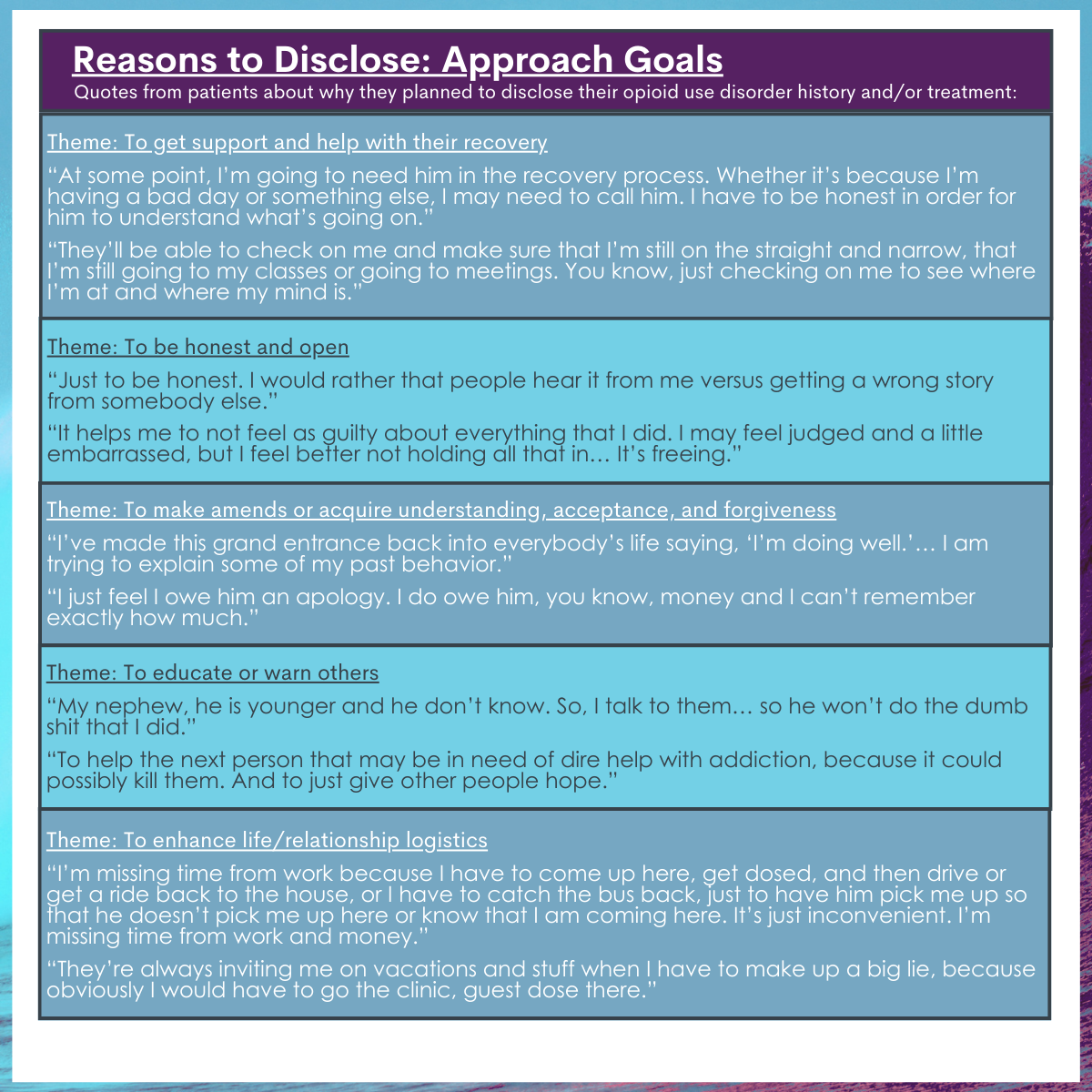
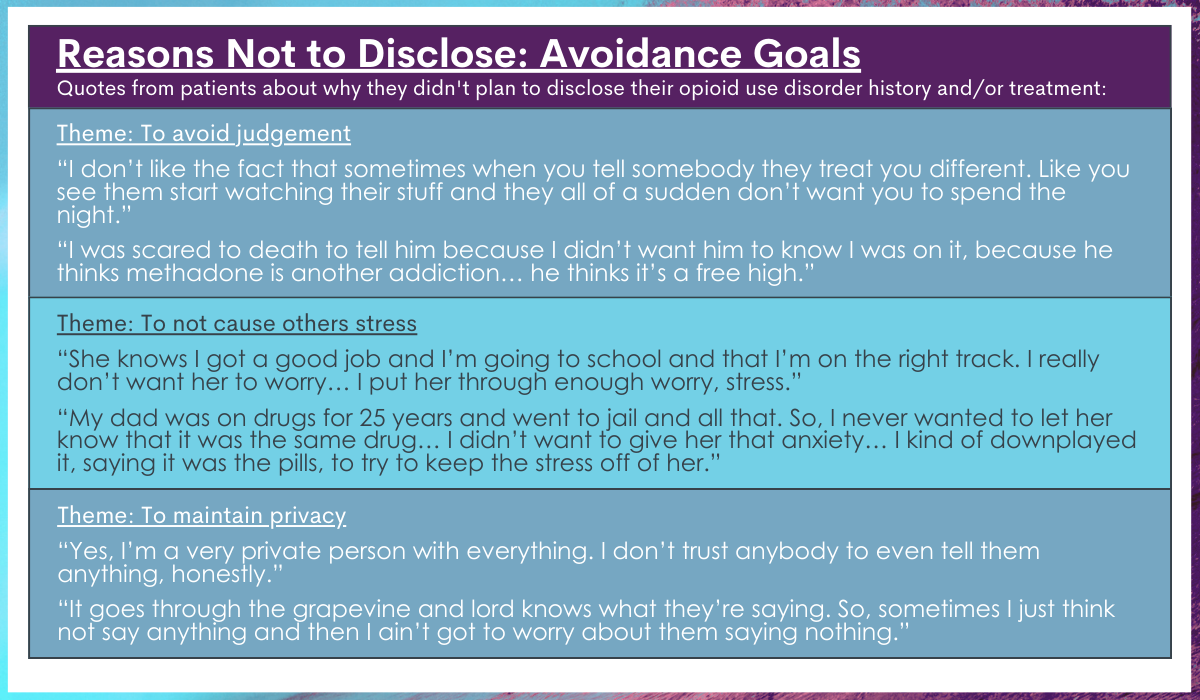
Several approach goals for disclosure were identified. Some patients reported plans to disclose their opioid use disorder history/treatment to family or friends to get support and help with their recovery. Others planned to disclose to be honest and open with loved ones, to make amends, or to acquire understanding, acceptance, or forgiveness from their family and friends. Some also wanted to educate or warn others about addiction and the consequences of substance use. Many individuals also felt that disclosing would make their lives and relationships logistically easier. Fewer avoidance goals were noted, but many participants were concerned about judgement from loved ones and causing them stress. Some also noted privacy as a concern.
Approach goals predicted greater likelihood of following through with disclosure.
Among participants who completed the study, 67% disclosed their opioid use disorder history or treatment to at least one planned disclosure recipient by 3-month follow up. This constituted 66% of the total number of planned disclosures. Participants with higher approach-goal scores were more likely to disclose, with the odds of disclosure approximately doubled with each point gained on the approach-goal scale. Those who were employed were 4.2 times less likely to disclose than those who were unemployed.
Approach goals at baseline were associated with stronger interpersonal relationships after disclosure.
Among the 83 individuals who disclosed their opioid use disorder history or treatment to at least one planned disclosure recipient, higher approach-goal scores at baseline were associated with greater social support from disclosure recipients and greater relationship closeness with disclosure recipients at follow up. Conversely, higher avoidance-goal scores at baseline were associated with more frequent experiences of enacted stigma from disclosure recipients at follow up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand disclosure goals (i.e., reasons to disclose [approach goals] and reasons not to disclose [avoidance goals] one’s opioid use disorder history/treatment) among individuals who are on their path to recovery from opioid use disorder. It also reveals how these goals relate to future disclosure to loved ones and the quality of relationships after disclosure. This research is important because it can ultimately help identify new approaches to help individuals rebuild interpersonal relationships that are negatively affected during active addiction, thereby supporting positive treatment and recovery outcomes.
Findings regarding disclosure goals are consistent with prior research on disclosure among individuals with other stigmatized identities, such as those living with HIV and individuals identifying as sexual minorities. This study also expands on disclosure goals among individuals with stigmatized identities by revealing goals more particular to individuals receiving treatment for opioid use disorder. Consistent with models on disclosure, greater approach goals (reasons to disclose) were associated with a higher likelihood of disclosing in the near future. The finding that avoidance goals (reasons not to disclose) did not predict whether individuals would disclose may be because all participants were planning to disclose to at least one person at the start of the study. It is possible that avoidance goals might emerge as a predictor of non-disclosure among individuals who are uncertain about disclosing, requiring further study. Nonetheless, this study suggests the more motivated someone is to disclose in order to accomplish or gain something the more likely they are to follow through with their plan to disclose their opioid use disorder history/treatment.
Approach goals appeared to be associated with healthier relationships after disclosing opioid use disorder history, while avoidance goals seem to be linked to less healthy relationships after disclosing. Perhaps the reasons for not disclosing (i.e. avoidance goals) influence the disclosure process (e.g., negatively affecting the tone or content of discussions/interactions during disclosure) to somehow promote or prompt more stigma. However, these data do not speak to causal relationships. Thus, stigma toward opioid use disorder may have existed among the disclosure recipient before disclosure and, if this was observed by the participant prior to disclosure, it could promote greater avoidance goals and result in more reasons to avoid disclosure in the first place. Regardless, stigma hinders recovery and is therefore important to address in social relationships to better support recovery among individuals with opioid use disorder.
Given the correlation-based data and lack of baseline social support measures, it is unclear if approach goals lead to greater social support after disclosure, or if high social support from a loved one prior to disclosure contributes to greater approach goals for disclosure and subsequent maintenance of that social support after disclosure. Nonetheless, this finding reveals opportunities to test new interventions that target approach goals before disclosure and study their impact on social support outcomes (e.g., cognitive behavioral therapies).
Because this study controlled for relationship closeness at baseline, the association between greater approach goals and closer relationships suggests that relationship closeness increases after disclosure, among those who have more reasons for disclosing. This is significant because relationship closeness is a key indicator of strong social bonds, which may work to reduce social isolation, rebuild relationships, and enhance social capital to support recovery. Since many individuals in recovery from opioid use disorder are not comfortable disclosing their history, understanding methods for enhancing disclosure comfort and promoting positive disclosure outcomes is essential for promoting healthy relationships for ongoing recovery.
The latter may be particularly true for people who are currently employed as these individuals were much less likely to disclose. Although more research is needed here to understand exactly why this is the case, it could be that such individuals fear negative job-related repercussions resulting from such disclosure and that such fears are weighed as more important as the potential benefits of disclosure. Future research will hopefully uncover whether there is a benefit in this regard or whether such non-disclosure among employed persons results in further self-stigma and isolation that may hinder ultimate recovery.
Given the weakened interpersonal relationships and social isolation that often accompanies opioid use disorder, as well as the importance of social relationships and disclosure in social bonds and recovery, additional study is needed. Doing so can ultimately lead to novel approaches for rebuilding healthy interpersonal relationships to support treatment and long-term recovery from opioid use disorder.
This study was conducted in a single state (Delaware) and in 2 suburban clinics, limiting conclusions about the applicability of these results in other states, treatment settings, and urban-dwelling patient samples. Moreover, all participants were receiving outpatient treatment with methadone or buprenorphine. Additional research is needed to determine if these findings are consistent in other treatment settings, in patients receiving treatment without medication, and among individuals in longer-term recovery from opioid use disorder.
Outcomes concerned social relationships and did not concern other recovery outcomes. Additional prospective research is needed to better understand relationships between disclosure, social relationships, and other recovery outcomes (e.g., ongoing illicit opioid use, quality of life, physical health, etc.). The relationship between disclosure goals and social relationships was also only assessed among those who disclosed, and this may have influenced study outcomes.
BOTTOM LINE
Individuals receiving medication treatment for opioid use disorder reported several reasons to disclose their opioid use disorder history/treatment to loved ones (i.e. approach goals), including to get recovery support, be open and honest, make amends, and educate others. Though fewer reasons to not disclose (i.e. avoidance goals) were identified, many individuals reported a desire to avoid judgement, maintain privacy, and avoid causing unnecessary stress among loved ones. The stronger one’s approach goals are, the more likely they are to disclose their opioid use disorder history to loved ones, and to have stronger social support from and relationship closeness to disclosure recipients after disclosing. Though additional research is needed, individuals seeking recovery from opioid use disorder and wishing to disclose their disorder history might benefit from identifying positive reasons for disclosure, which could possibly enhance their interpersonal relationships with disclosure recipients after disclosure.
For individuals and families seeking recovery: Individuals who are seeking to rebuild their social relationships by disclosing their opioid use disorder history or treatment to family and friends, and that have identified reasons to disclose, might experience healthy relationship outcomes after disclosure, including social support and enhanced relationship closeness. In this study, individuals with greater reasons not to disclose were more likely to experience stigma from loved ones after disclosing. Individuals who experience stigma from family or friends after disclosing their history might benefit from seeking help and support from the recovery community to educate loved ones and ensure this stigma does not hinder their recovery progress.
For treatment professionals and treatment systems: According to this study, individuals with more reasons not to disclose might be more likely to experience stigma after disclosing. Providing patients the support they need to combat experienced stigma and continue their treatment and recovery progress may help to partially offset any negative consequences of disclosure. This study also found that those with greater reasons to disclose were more likely to disclose thereafter, and to have better social support and closer relationships after disclosure. Individuals who have positive support systems and a desire to disclose to loved ones might improve their interpersonal relationships by disclosing their status, thereby facilitating positive treatment and recovery outcomes. However, these data only speak to relationships, not cause and effect, and additional research will help us better understand this important area of research.
For scientists:Additional research is needed to replicate and extend these findings in different states and treatment settings, and to identify additional predictors of disclosure and relationship outcomes post disclosure across various treatment and recovery populations. Studies conducted among individuals who are uncertain about disclosing are needed to determine whether or not avoidance goals can predict non-disclosure or relationship outcomes post disclosure. Investigations that incorporate baseline measures of social support and stigma, as well as studies that examine the relationship context of disclosure recipients (e.g., siblings vs. friends vs. parents & reasons for disclosure to each) and that incorporate other recovery outcomes will help advance this area of research. Research among individuals who are receiving treatment without medication and who have less variability in their recovery durations will also help to clarify disclosure processes and their relationship to acts of disclosure and relationship outcomes post disclosure.
For policy makers: Interpersonal relationships and disclosure of opioid use disorder history may influence how individuals fare in their recovery Studies like this that examine disclosure processes and their impact on relationship outcomes like social support and stigma are essential to advancing treatment and recovery among individuals with opioid use disorder. This is because chronic opioid misuse negatively affects interpersonal relationships and healthy interpersonal relationships are a key component to successful recovery. Additional funding for this area of research can ultimately help identify new interventions to help individuals rebuild their social relationships, thereby supporting their long-term recovery.
Interpersonal relationships and social support play important roles in the recovery process. Positive social support is associated with positive changes and behaviors that facilitate recovery, such as reduced substance use disorder severity and better treatment retention. One potential way to enhance social support is by disclosing or sharing information about one’s substance use disorder history, treatment, and recovery. However, disclosing this information might make individuals vulnerable to experiencing stigma and discrimination (e.g., mistreatment), which is associated with treatment drop-out and ongoing substance misuse.
One component of disclosure that has yet to be studied among individuals with opioid use disorder is disclosure goals. Different reasons for disclosing one’s recovery status are thought to influence whether a person will actually disclose and how they go about disclosing, as well as their relationship and health outcomes after they disclose to others.
Disclosure goals consist of approach goals (pursuing desirable outcomes of disclosure like social support and feelings of social closeness) and avoidance goals (avoiding undesirable outcomes of disclosure like experiencing stigma or mistreatment). Whereas approach goals are linked to an increased likelihood of disclosing and more desirable responses among those who are disclosed to (providing more trust/social support), avoidance goals are linked to more social conflict and distant relationships. This study characterized disclosure goals among individuals receiving treatment for opioid use disorder and examined whether these goals are associated with future acts of disclosure and relationship outcomes after disclosure (i.e., social support, relationship closeness, and the experience of unfair treatment by others, also known as enacted stigma).
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal naturalistic investigation of adult outpatients receiving medication for opioid use disorder in the state of Delaware, in which patients completed qualitative interviews and questionnaires about their disclosure plans and social relationships over the course of three months. Individuals were recruited between 2018 and 2019 from 2 behavioral health clinics, including 1 suburban clinic and 1 urban clinic. All participants planned to disclose their substance use disorder history and/or treatment for the first time to at least 1 person (i.e. disclosure recipient) within the 3-month study timeframe.
The initial study assessments examined disclosure goals and relationship status before disclosure via qualitative interviews and questionnaires. At the 3-month follow up, participants completed questionnaires about their relationship status with disclosure recipients after they had disclosed their opioid use disorder history. During the initial interview assessments, participants answered questions regarding plans to disclose to up to 3 people. Interviews asked about: (1) approach goals (i.e., their reasons to disclose) and (2) avoidance goals (i.e., their reasons to not disclose). Questionnaires at baseline and follow up concerned 4 topics: (1) disclosure goals, (2) relationship closeness to disclosure recipients, (3) social support from disclosure recipients, and (4) enacted stigma from disclosure recipients.
Participants completed four questionnaires regarding disclosure goals, relationship closeness, social support, and enacted stigma.
Qualitative baseline interviews were analyzed and reasons to disclose and not to disclose were identified. Predictors of participant’s disclosing within 3-months were examined among those who completed the follow-up assessment. Predictors of social support, relationship closeness, and enacted stigma were examined among individuals who disclosed their opioid use disorder history. Predictors for both analyses included disclosure-goal scores on the disclosure questionnaire (approach & avoidance) and relationship closeness at baseline, controlling for all other variables (e.g., demographics, recovery factors). Analyses also examined the potential influence of socio-demographic (e.g., race, age) and recovery (e.g., recovery duration) factors.
One hundred and forty-six individuals participated in the initial study session, of which 124 (85%) completed the month-3 follow up. All participants were undergoing methadone (87%) or buprenorphine (13%) treatment for opioid use disorder. On average, participants reported being in recovery for 4 years (range: 0 to 32 years). The majority of participants were White (75%), middle-aged (average: 40 years old), unemployed (64%) patients attending a suburban treatment clinic (65%), with a history of incarceration (70%) and, consistent with their current treatment participation, had mild opioid dependence, on average, according to the Leeds Dependence Questionnaire. About half of the participants were women (53%). On average, participants planned to disclose to one person, and this was most commonly a parent (22%), friend (16%), or sibling (10%).
WHAT DID THIS STUDY FIND?
Approach goals for planned disclosures included a desire for recovery support, honesty, amends, and education of loved ones, while avoidance goals included fear of judgement privacy, and concern for others.
Several approach goals for disclosure were identified. Some patients reported plans to disclose their opioid use disorder history/treatment to family or friends to get support and help with their recovery. Others planned to disclose to be honest and open with loved ones, to make amends, or to acquire understanding, acceptance, or forgiveness from their family and friends. Some also wanted to educate or warn others about addiction and the consequences of substance use. Many individuals also felt that disclosing would make their lives and relationships logistically easier. Fewer avoidance goals were noted, but many participants were concerned about judgement from loved ones and causing them stress. Some also noted privacy as a concern.
Approach goals predicted greater likelihood of following through with disclosure.
Among participants who completed the study, 67% disclosed their opioid use disorder history or treatment to at least one planned disclosure recipient by 3-month follow up. This constituted 66% of the total number of planned disclosures. Participants with higher approach-goal scores were more likely to disclose, with the odds of disclosure approximately doubled with each point gained on the approach-goal scale. Those who were employed were 4.2 times less likely to disclose than those who were unemployed.
Approach goals at baseline were associated with stronger interpersonal relationships after disclosure.
Among the 83 individuals who disclosed their opioid use disorder history or treatment to at least one planned disclosure recipient, higher approach-goal scores at baseline were associated with greater social support from disclosure recipients and greater relationship closeness with disclosure recipients at follow up. Conversely, higher avoidance-goal scores at baseline were associated with more frequent experiences of enacted stigma from disclosure recipients at follow up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand disclosure goals (i.e., reasons to disclose [approach goals] and reasons not to disclose [avoidance goals] one’s opioid use disorder history/treatment) among individuals who are on their path to recovery from opioid use disorder. It also reveals how these goals relate to future disclosure to loved ones and the quality of relationships after disclosure. This research is important because it can ultimately help identify new approaches to help individuals rebuild interpersonal relationships that are negatively affected during active addiction, thereby supporting positive treatment and recovery outcomes.
Findings regarding disclosure goals are consistent with prior research on disclosure among individuals with other stigmatized identities, such as those living with HIV and individuals identifying as sexual minorities. This study also expands on disclosure goals among individuals with stigmatized identities by revealing goals more particular to individuals receiving treatment for opioid use disorder. Consistent with models on disclosure, greater approach goals (reasons to disclose) were associated with a higher likelihood of disclosing in the near future. The finding that avoidance goals (reasons not to disclose) did not predict whether individuals would disclose may be because all participants were planning to disclose to at least one person at the start of the study. It is possible that avoidance goals might emerge as a predictor of non-disclosure among individuals who are uncertain about disclosing, requiring further study. Nonetheless, this study suggests the more motivated someone is to disclose in order to accomplish or gain something the more likely they are to follow through with their plan to disclose their opioid use disorder history/treatment.
Approach goals appeared to be associated with healthier relationships after disclosing opioid use disorder history, while avoidance goals seem to be linked to less healthy relationships after disclosing. Perhaps the reasons for not disclosing (i.e. avoidance goals) influence the disclosure process (e.g., negatively affecting the tone or content of discussions/interactions during disclosure) to somehow promote or prompt more stigma. However, these data do not speak to causal relationships. Thus, stigma toward opioid use disorder may have existed among the disclosure recipient before disclosure and, if this was observed by the participant prior to disclosure, it could promote greater avoidance goals and result in more reasons to avoid disclosure in the first place. Regardless, stigma hinders recovery and is therefore important to address in social relationships to better support recovery among individuals with opioid use disorder.
Given the correlation-based data and lack of baseline social support measures, it is unclear if approach goals lead to greater social support after disclosure, or if high social support from a loved one prior to disclosure contributes to greater approach goals for disclosure and subsequent maintenance of that social support after disclosure. Nonetheless, this finding reveals opportunities to test new interventions that target approach goals before disclosure and study their impact on social support outcomes (e.g., cognitive behavioral therapies).
Because this study controlled for relationship closeness at baseline, the association between greater approach goals and closer relationships suggests that relationship closeness increases after disclosure, among those who have more reasons for disclosing. This is significant because relationship closeness is a key indicator of strong social bonds, which may work to reduce social isolation, rebuild relationships, and enhance social capital to support recovery. Since many individuals in recovery from opioid use disorder are not comfortable disclosing their history, understanding methods for enhancing disclosure comfort and promoting positive disclosure outcomes is essential for promoting healthy relationships for ongoing recovery.
The latter may be particularly true for people who are currently employed as these individuals were much less likely to disclose. Although more research is needed here to understand exactly why this is the case, it could be that such individuals fear negative job-related repercussions resulting from such disclosure and that such fears are weighed as more important as the potential benefits of disclosure. Future research will hopefully uncover whether there is a benefit in this regard or whether such non-disclosure among employed persons results in further self-stigma and isolation that may hinder ultimate recovery.
Given the weakened interpersonal relationships and social isolation that often accompanies opioid use disorder, as well as the importance of social relationships and disclosure in social bonds and recovery, additional study is needed. Doing so can ultimately lead to novel approaches for rebuilding healthy interpersonal relationships to support treatment and long-term recovery from opioid use disorder.
This study was conducted in a single state (Delaware) and in 2 suburban clinics, limiting conclusions about the applicability of these results in other states, treatment settings, and urban-dwelling patient samples. Moreover, all participants were receiving outpatient treatment with methadone or buprenorphine. Additional research is needed to determine if these findings are consistent in other treatment settings, in patients receiving treatment without medication, and among individuals in longer-term recovery from opioid use disorder.
Outcomes concerned social relationships and did not concern other recovery outcomes. Additional prospective research is needed to better understand relationships between disclosure, social relationships, and other recovery outcomes (e.g., ongoing illicit opioid use, quality of life, physical health, etc.). The relationship between disclosure goals and social relationships was also only assessed among those who disclosed, and this may have influenced study outcomes.
BOTTOM LINE
Individuals receiving medication treatment for opioid use disorder reported several reasons to disclose their opioid use disorder history/treatment to loved ones (i.e. approach goals), including to get recovery support, be open and honest, make amends, and educate others. Though fewer reasons to not disclose (i.e. avoidance goals) were identified, many individuals reported a desire to avoid judgement, maintain privacy, and avoid causing unnecessary stress among loved ones. The stronger one’s approach goals are, the more likely they are to disclose their opioid use disorder history to loved ones, and to have stronger social support from and relationship closeness to disclosure recipients after disclosing. Though additional research is needed, individuals seeking recovery from opioid use disorder and wishing to disclose their disorder history might benefit from identifying positive reasons for disclosure, which could possibly enhance their interpersonal relationships with disclosure recipients after disclosure.
For individuals and families seeking recovery: Individuals who are seeking to rebuild their social relationships by disclosing their opioid use disorder history or treatment to family and friends, and that have identified reasons to disclose, might experience healthy relationship outcomes after disclosure, including social support and enhanced relationship closeness. In this study, individuals with greater reasons not to disclose were more likely to experience stigma from loved ones after disclosing. Individuals who experience stigma from family or friends after disclosing their history might benefit from seeking help and support from the recovery community to educate loved ones and ensure this stigma does not hinder their recovery progress.
For treatment professionals and treatment systems: According to this study, individuals with more reasons not to disclose might be more likely to experience stigma after disclosing. Providing patients the support they need to combat experienced stigma and continue their treatment and recovery progress may help to partially offset any negative consequences of disclosure. This study also found that those with greater reasons to disclose were more likely to disclose thereafter, and to have better social support and closer relationships after disclosure. Individuals who have positive support systems and a desire to disclose to loved ones might improve their interpersonal relationships by disclosing their status, thereby facilitating positive treatment and recovery outcomes. However, these data only speak to relationships, not cause and effect, and additional research will help us better understand this important area of research.
For scientists:Additional research is needed to replicate and extend these findings in different states and treatment settings, and to identify additional predictors of disclosure and relationship outcomes post disclosure across various treatment and recovery populations. Studies conducted among individuals who are uncertain about disclosing are needed to determine whether or not avoidance goals can predict non-disclosure or relationship outcomes post disclosure. Investigations that incorporate baseline measures of social support and stigma, as well as studies that examine the relationship context of disclosure recipients (e.g., siblings vs. friends vs. parents & reasons for disclosure to each) and that incorporate other recovery outcomes will help advance this area of research. Research among individuals who are receiving treatment without medication and who have less variability in their recovery durations will also help to clarify disclosure processes and their relationship to acts of disclosure and relationship outcomes post disclosure.
For policy makers: Interpersonal relationships and disclosure of opioid use disorder history may influence how individuals fare in their recovery Studies like this that examine disclosure processes and their impact on relationship outcomes like social support and stigma are essential to advancing treatment and recovery among individuals with opioid use disorder. This is because chronic opioid misuse negatively affects interpersonal relationships and healthy interpersonal relationships are a key component to successful recovery. Additional funding for this area of research can ultimately help identify new interventions to help individuals rebuild their social relationships, thereby supporting their long-term recovery.
Interpersonal relationships and social support play important roles in the recovery process. Positive social support is associated with positive changes and behaviors that facilitate recovery, such as reduced substance use disorder severity and better treatment retention. One potential way to enhance social support is by disclosing or sharing information about one’s substance use disorder history, treatment, and recovery. However, disclosing this information might make individuals vulnerable to experiencing stigma and discrimination (e.g., mistreatment), which is associated with treatment drop-out and ongoing substance misuse.
One component of disclosure that has yet to be studied among individuals with opioid use disorder is disclosure goals. Different reasons for disclosing one’s recovery status are thought to influence whether a person will actually disclose and how they go about disclosing, as well as their relationship and health outcomes after they disclose to others.
Disclosure goals consist of approach goals (pursuing desirable outcomes of disclosure like social support and feelings of social closeness) and avoidance goals (avoiding undesirable outcomes of disclosure like experiencing stigma or mistreatment). Whereas approach goals are linked to an increased likelihood of disclosing and more desirable responses among those who are disclosed to (providing more trust/social support), avoidance goals are linked to more social conflict and distant relationships. This study characterized disclosure goals among individuals receiving treatment for opioid use disorder and examined whether these goals are associated with future acts of disclosure and relationship outcomes after disclosure (i.e., social support, relationship closeness, and the experience of unfair treatment by others, also known as enacted stigma).
HOW WAS THIS STUDY CONDUCTED?
This study was a longitudinal naturalistic investigation of adult outpatients receiving medication for opioid use disorder in the state of Delaware, in which patients completed qualitative interviews and questionnaires about their disclosure plans and social relationships over the course of three months. Individuals were recruited between 2018 and 2019 from 2 behavioral health clinics, including 1 suburban clinic and 1 urban clinic. All participants planned to disclose their substance use disorder history and/or treatment for the first time to at least 1 person (i.e. disclosure recipient) within the 3-month study timeframe.
The initial study assessments examined disclosure goals and relationship status before disclosure via qualitative interviews and questionnaires. At the 3-month follow up, participants completed questionnaires about their relationship status with disclosure recipients after they had disclosed their opioid use disorder history. During the initial interview assessments, participants answered questions regarding plans to disclose to up to 3 people. Interviews asked about: (1) approach goals (i.e., their reasons to disclose) and (2) avoidance goals (i.e., their reasons to not disclose). Questionnaires at baseline and follow up concerned 4 topics: (1) disclosure goals, (2) relationship closeness to disclosure recipients, (3) social support from disclosure recipients, and (4) enacted stigma from disclosure recipients.
Participants completed four questionnaires regarding disclosure goals, relationship closeness, social support, and enacted stigma.
Qualitative baseline interviews were analyzed and reasons to disclose and not to disclose were identified. Predictors of participant’s disclosing within 3-months were examined among those who completed the follow-up assessment. Predictors of social support, relationship closeness, and enacted stigma were examined among individuals who disclosed their opioid use disorder history. Predictors for both analyses included disclosure-goal scores on the disclosure questionnaire (approach & avoidance) and relationship closeness at baseline, controlling for all other variables (e.g., demographics, recovery factors). Analyses also examined the potential influence of socio-demographic (e.g., race, age) and recovery (e.g., recovery duration) factors.
One hundred and forty-six individuals participated in the initial study session, of which 124 (85%) completed the month-3 follow up. All participants were undergoing methadone (87%) or buprenorphine (13%) treatment for opioid use disorder. On average, participants reported being in recovery for 4 years (range: 0 to 32 years). The majority of participants were White (75%), middle-aged (average: 40 years old), unemployed (64%) patients attending a suburban treatment clinic (65%), with a history of incarceration (70%) and, consistent with their current treatment participation, had mild opioid dependence, on average, according to the Leeds Dependence Questionnaire. About half of the participants were women (53%). On average, participants planned to disclose to one person, and this was most commonly a parent (22%), friend (16%), or sibling (10%).
WHAT DID THIS STUDY FIND?
Approach goals for planned disclosures included a desire for recovery support, honesty, amends, and education of loved ones, while avoidance goals included fear of judgement privacy, and concern for others.
Several approach goals for disclosure were identified. Some patients reported plans to disclose their opioid use disorder history/treatment to family or friends to get support and help with their recovery. Others planned to disclose to be honest and open with loved ones, to make amends, or to acquire understanding, acceptance, or forgiveness from their family and friends. Some also wanted to educate or warn others about addiction and the consequences of substance use. Many individuals also felt that disclosing would make their lives and relationships logistically easier. Fewer avoidance goals were noted, but many participants were concerned about judgement from loved ones and causing them stress. Some also noted privacy as a concern.
Approach goals predicted greater likelihood of following through with disclosure.
Among participants who completed the study, 67% disclosed their opioid use disorder history or treatment to at least one planned disclosure recipient by 3-month follow up. This constituted 66% of the total number of planned disclosures. Participants with higher approach-goal scores were more likely to disclose, with the odds of disclosure approximately doubled with each point gained on the approach-goal scale. Those who were employed were 4.2 times less likely to disclose than those who were unemployed.
Approach goals at baseline were associated with stronger interpersonal relationships after disclosure.
Among the 83 individuals who disclosed their opioid use disorder history or treatment to at least one planned disclosure recipient, higher approach-goal scores at baseline were associated with greater social support from disclosure recipients and greater relationship closeness with disclosure recipients at follow up. Conversely, higher avoidance-goal scores at baseline were associated with more frequent experiences of enacted stigma from disclosure recipients at follow up.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study helps us better understand disclosure goals (i.e., reasons to disclose [approach goals] and reasons not to disclose [avoidance goals] one’s opioid use disorder history/treatment) among individuals who are on their path to recovery from opioid use disorder. It also reveals how these goals relate to future disclosure to loved ones and the quality of relationships after disclosure. This research is important because it can ultimately help identify new approaches to help individuals rebuild interpersonal relationships that are negatively affected during active addiction, thereby supporting positive treatment and recovery outcomes.
Findings regarding disclosure goals are consistent with prior research on disclosure among individuals with other stigmatized identities, such as those living with HIV and individuals identifying as sexual minorities. This study also expands on disclosure goals among individuals with stigmatized identities by revealing goals more particular to individuals receiving treatment for opioid use disorder. Consistent with models on disclosure, greater approach goals (reasons to disclose) were associated with a higher likelihood of disclosing in the near future. The finding that avoidance goals (reasons not to disclose) did not predict whether individuals would disclose may be because all participants were planning to disclose to at least one person at the start of the study. It is possible that avoidance goals might emerge as a predictor of non-disclosure among individuals who are uncertain about disclosing, requiring further study. Nonetheless, this study suggests the more motivated someone is to disclose in order to accomplish or gain something the more likely they are to follow through with their plan to disclose their opioid use disorder history/treatment.
Approach goals appeared to be associated with healthier relationships after disclosing opioid use disorder history, while avoidance goals seem to be linked to less healthy relationships after disclosing. Perhaps the reasons for not disclosing (i.e. avoidance goals) influence the disclosure process (e.g., negatively affecting the tone or content of discussions/interactions during disclosure) to somehow promote or prompt more stigma. However, these data do not speak to causal relationships. Thus, stigma toward opioid use disorder may have existed among the disclosure recipient before disclosure and, if this was observed by the participant prior to disclosure, it could promote greater avoidance goals and result in more reasons to avoid disclosure in the first place. Regardless, stigma hinders recovery and is therefore important to address in social relationships to better support recovery among individuals with opioid use disorder.
Given the correlation-based data and lack of baseline social support measures, it is unclear if approach goals lead to greater social support after disclosure, or if high social support from a loved one prior to disclosure contributes to greater approach goals for disclosure and subsequent maintenance of that social support after disclosure. Nonetheless, this finding reveals opportunities to test new interventions that target approach goals before disclosure and study their impact on social support outcomes (e.g., cognitive behavioral therapies).
Because this study controlled for relationship closeness at baseline, the association between greater approach goals and closer relationships suggests that relationship closeness increases after disclosure, among those who have more reasons for disclosing. This is significant because relationship closeness is a key indicator of strong social bonds, which may work to reduce social isolation, rebuild relationships, and enhance social capital to support recovery. Since many individuals in recovery from opioid use disorder are not comfortable disclosing their history, understanding methods for enhancing disclosure comfort and promoting positive disclosure outcomes is essential for promoting healthy relationships for ongoing recovery.
The latter may be particularly true for people who are currently employed as these individuals were much less likely to disclose. Although more research is needed here to understand exactly why this is the case, it could be that such individuals fear negative job-related repercussions resulting from such disclosure and that such fears are weighed as more important as the potential benefits of disclosure. Future research will hopefully uncover whether there is a benefit in this regard or whether such non-disclosure among employed persons results in further self-stigma and isolation that may hinder ultimate recovery.
Given the weakened interpersonal relationships and social isolation that often accompanies opioid use disorder, as well as the importance of social relationships and disclosure in social bonds and recovery, additional study is needed. Doing so can ultimately lead to novel approaches for rebuilding healthy interpersonal relationships to support treatment and long-term recovery from opioid use disorder.
This study was conducted in a single state (Delaware) and in 2 suburban clinics, limiting conclusions about the applicability of these results in other states, treatment settings, and urban-dwelling patient samples. Moreover, all participants were receiving outpatient treatment with methadone or buprenorphine. Additional research is needed to determine if these findings are consistent in other treatment settings, in patients receiving treatment without medication, and among individuals in longer-term recovery from opioid use disorder.
Outcomes concerned social relationships and did not concern other recovery outcomes. Additional prospective research is needed to better understand relationships between disclosure, social relationships, and other recovery outcomes (e.g., ongoing illicit opioid use, quality of life, physical health, etc.). The relationship between disclosure goals and social relationships was also only assessed among those who disclosed, and this may have influenced study outcomes.
BOTTOM LINE
Individuals receiving medication treatment for opioid use disorder reported several reasons to disclose their opioid use disorder history/treatment to loved ones (i.e. approach goals), including to get recovery support, be open and honest, make amends, and educate others. Though fewer reasons to not disclose (i.e. avoidance goals) were identified, many individuals reported a desire to avoid judgement, maintain privacy, and avoid causing unnecessary stress among loved ones. The stronger one’s approach goals are, the more likely they are to disclose their opioid use disorder history to loved ones, and to have stronger social support from and relationship closeness to disclosure recipients after disclosing. Though additional research is needed, individuals seeking recovery from opioid use disorder and wishing to disclose their disorder history might benefit from identifying positive reasons for disclosure, which could possibly enhance their interpersonal relationships with disclosure recipients after disclosure.
For individuals and families seeking recovery: Individuals who are seeking to rebuild their social relationships by disclosing their opioid use disorder history or treatment to family and friends, and that have identified reasons to disclose, might experience healthy relationship outcomes after disclosure, including social support and enhanced relationship closeness. In this study, individuals with greater reasons not to disclose were more likely to experience stigma from loved ones after disclosing. Individuals who experience stigma from family or friends after disclosing their history might benefit from seeking help and support from the recovery community to educate loved ones and ensure this stigma does not hinder their recovery progress.
For treatment professionals and treatment systems: According to this study, individuals with more reasons not to disclose might be more likely to experience stigma after disclosing. Providing patients the support they need to combat experienced stigma and continue their treatment and recovery progress may help to partially offset any negative consequences of disclosure. This study also found that those with greater reasons to disclose were more likely to disclose thereafter, and to have better social support and closer relationships after disclosure. Individuals who have positive support systems and a desire to disclose to loved ones might improve their interpersonal relationships by disclosing their status, thereby facilitating positive treatment and recovery outcomes. However, these data only speak to relationships, not cause and effect, and additional research will help us better understand this important area of research.
For scientists:Additional research is needed to replicate and extend these findings in different states and treatment settings, and to identify additional predictors of disclosure and relationship outcomes post disclosure across various treatment and recovery populations. Studies conducted among individuals who are uncertain about disclosing are needed to determine whether or not avoidance goals can predict non-disclosure or relationship outcomes post disclosure. Investigations that incorporate baseline measures of social support and stigma, as well as studies that examine the relationship context of disclosure recipients (e.g., siblings vs. friends vs. parents & reasons for disclosure to each) and that incorporate other recovery outcomes will help advance this area of research. Research among individuals who are receiving treatment without medication and who have less variability in their recovery durations will also help to clarify disclosure processes and their relationship to acts of disclosure and relationship outcomes post disclosure.
For policy makers: Interpersonal relationships and disclosure of opioid use disorder history may influence how individuals fare in their recovery Studies like this that examine disclosure processes and their impact on relationship outcomes like social support and stigma are essential to advancing treatment and recovery among individuals with opioid use disorder. This is because chronic opioid misuse negatively affects interpersonal relationships and healthy interpersonal relationships are a key component to successful recovery. Additional funding for this area of research can ultimately help identify new interventions to help individuals rebuild their social relationships, thereby supporting their long-term recovery.