
Providing naloxone to people who are prescribed opioids is a cost-effective way of preventing opioid overdose deaths
Much of the research on the effects of naloxone distribution has focused on people with opioid use disorder. This study investigated the public health impact and cost-effectiveness of naloxone access for individuals prescribed opioid medications, more generally, to help inform a comprehensive naloxone distribution strategy.
WHAT PROBLEM DOES THIS STUDY ADDRESS?
With the rates of opioid overdose deaths continuing to increase, strategies are critically needed to prevent deaths. Naloxone is a medication that can rapidly reverse an overdose caused by opioids. “Take-home naloxone” is an intervention that combines naloxone provision with overdose response training. This intervention has been shown to be an effective and cost-efficient response to the overdose epidemic.
Statistical modeling approaches can estimate how cost-effective an intervention is, but many of the existing models have based their estimates on people with opioid use disorder and specifically those who inject heroin. Examining the public health impact of increasing naloxone access to the population of people who use prescription opioids more generally can potentially help to prevent opioid-related overdose deaths.
Although there are differences in the risk of overdose between people who use prescription opioids and people who inject heroin, the risk for people who use prescription opioids remains high because they often also have high rates of mental and physical conditions that increase their risk. Further, studies have shown that many people who have been prescribed opioids over a long period of time are at an increased risk for overdose, as outlined by the Centers for Disease Control and Prevention. These factors include being prescribed a high daily dose of opioids (50 milligrams or more of oral morphine equivalents), previously having a substance use disorder, being prescribed a benzodiazepine (i.e., a medicine for treating anxiety, such as Xanax and Valium) at the same time as the opioid, and having previously overdosed. Even though these individuals are at a high risk for experiencing an overdose, there have not yet been any studies that have investigated the impact of distributing take-home naloxone to people who are prescribed opioids. This study investigated the impact, cost, and cost per life saved from scaling up the distribution of naloxone to individuals living in Victoria, Australia, who are prescribed opioids. This research provides an important harm reduction example that can shed light on the public health impacts of naloxone distribution for this population.
HOW WAS THIS STUDY CONDUCTED?
The research team used simulation modeling to examine the impact on deaths prevented, costs, and cost per life saved from scaling up the distribution of naloxone to individuals who are prescribed opioids in Victoria, Australia. The researchers used a statistical modeling approach that classifies different outcomes for people experiencing a prescription opioid overdose. This model allows them to predict outcomes that have not actually occurred, but to simulate outcomes that can occur given a set of rules, or parameters, with estimates taken from real-world data as much as possible. Data for the model was drawn from people who use prescription opioids in Victoria, Australia, and was divided into medium dosage (50-100 milligrams of oral morphine equivalents per day) and high dosage (100 milligrams or more of oral morphine equivalents).
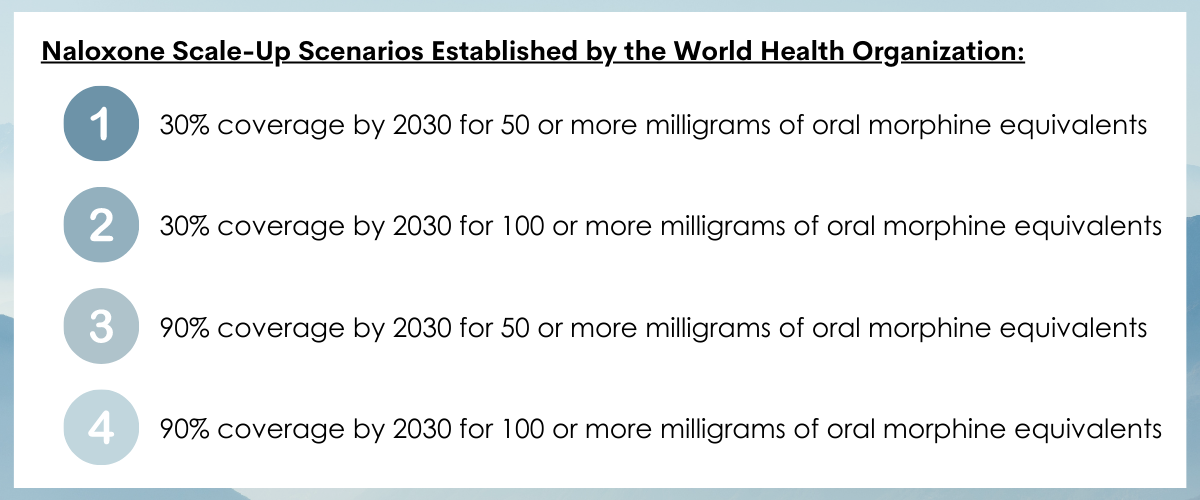
The outcomes of interest were the number of deaths prevented, additional costs for ambulance calls and naloxone distribution, and costs per life saved for four different scenarios of naloxone scale up. These scenarios were guided by the global targets the World Health Organization set for naloxone supply based on people who inject drugs or use heroin. Specifically, the four scenarios provided different levels of coverage: (1) 30% coverage by 2030 for 50 or more milligrams of oral morphine equivalents; (2) 30% coverage by 2030 for 100 or more milligrams of oral morphine equivalents; (3) 90% coverage by 2030 for 50 or more milligrams of oral morphine equivalents; and (4) 90% coverage by 2030 for 100 or more milligrams of oral morphine equivalents.
To conduct the simulation, the authors used several, current (i.e., at the time of the study) real-world data sources available to them: coverage of naloxone; percentage of overdoses that are witnessed; the probability that the naloxone kit would be accessible when needed; the probability that naloxone would be used correctly when available; and the probability that an ambulance would be called. From these data, they were able to simulate each of the outcomes. They compared the number of deaths prevented and the cost to prevent those deaths (e.g., cost per life saved) for each of the scenarios relative to the status quo of not providing naloxone to individuals prescribed opioids.
WHAT DID THIS STUDY FIND?
Distributing more naloxone resulted in the best public health outcomes.
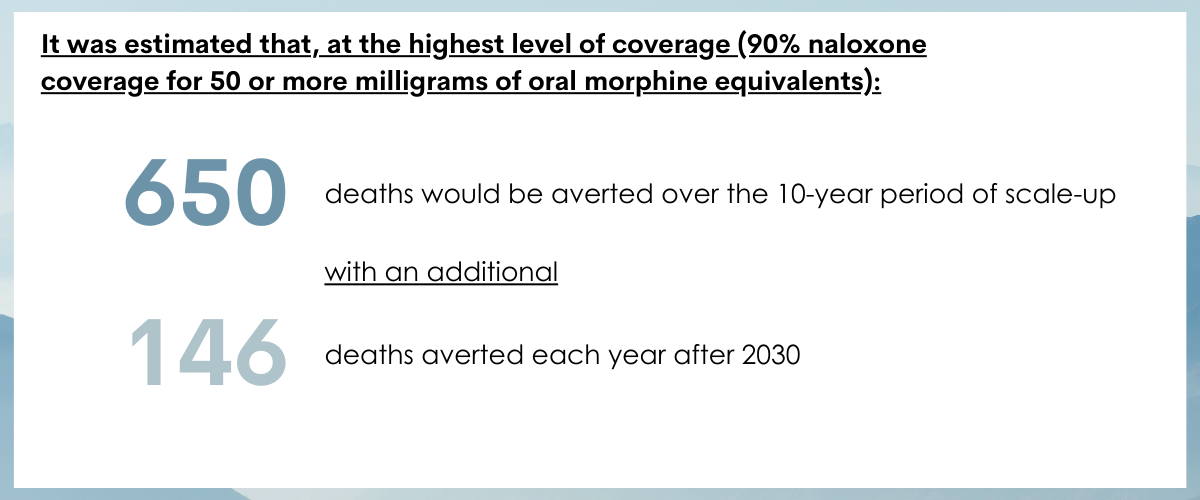
When compared to no or minimal naloxone distribution, each of the four scale-up scenarios resulted in fewer prescription opioid overdose deaths and more calls for ambulances. The biggest impact was seen with the highest level of coverage, which was 90% coverage for 50 or more milligrams of oral morphine equivalents. At this coverage level, it was estimated that more than 650 deaths would be prevented over the ten-year period, with an additional 146 deaths prevented each year after 2030.
As naloxone coverage increased, costs increased.
As naloxone coverage increased, costs were greater due to increases in ambulance calls and distributed naloxone kits. The cost per life saved for those in the 50 or more-milligram group was 43,600 Australian dollars, or approximately 31,331 US dollars. For those in the 100 or more-milligram group, the cost per life saved was 38,200 Australian dollars, or approximately 27,450 US dollars.
The variables that had the greatest impact on the estimated number of deaths prevented and cost per life saved differed.
The proportion of overdoses witnessed and recognized as overdoses had the greatest impact on the estimated number of deaths averted. Other influential variables included the annual probability of overdose, the likelihood of dying from a witnessed overdose, and the increase in overdose risk for those on higher doses of prescription.
The proportion of people who die from a witnessed overdose had the greatest impact on the estimated cost per life saved. Other influential variables included the proportion of cases where an ambulance was called without use of take-home naloxone, the annual probability of an overdose, and the proportion of overdoses that were witnessed and recognized as overdoses.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study investigated the impact, cost, and cost per life saved from scaling up the distribution of naloxone to individuals who are prescribed opioids. They showed that scaling up naloxone to coverage levels recommended by the World Health Organization may be a cost-effective intervention that can save lives. This builds on previous research demonstrating the cost-effectiveness and ability to save lives of providing other opioid medications, such as methadone, buprenorphine, and injectable naltrexone.
Further, the researchers showed that the proportion of overdoses witnessed and recognized had the greatest impact on the estimated number of deaths averted. If someone is around to see the overdose and recognizes it as such, they may be more likely to do something about it and the life can be saved. This builds on previous research that has showed that training bystanders (many of whom use opioids themselves) to use naloxone and recognize the signs of overdoses is associated with overdose reversals and an increase in their knowledge and ability to safely respond. While that research was primarily conducted with individuals who use heroin, the results from the current study suggest that individuals who are prescribed opioids are likely to benefit from similar strategies. However, it should be noted that confidence in the precision of the results in these kinds of modeling approaches is limited and may vary.
There are currently several barriers to increasing the supply of take-home naloxone to people who use prescription opioids in Australia, despite its effectiveness in preventing opioid overdose deaths. These include lack of pharmacist knowledge and confidence regarding their ability to educate patients on overdoses and naloxone use, pharmacists’ association of naloxone with illicit substance use, and lack of pharmacist awareness that naloxone can benefit people who are prescribed opioids. In the US, although the majority of states have laws that support some access to naloxone, they vary by state and still have restrictions. Accordingly, individual- and system-level strategies that address these barriers are needed, such as increasing pharmacists’ knowledge, training, and awareness, implementing campaigns to reduce stigma, and, in the US, writing policies into law that reduce legal restrictions to naloxone and increase access.
The study’s findings reflect one very concrete and effective harm reduction approach to reduce overdose deaths. However, in order to achieve maximum impact in alleviating the opioid crisis more generally, it needs to be used as part of a larger, multi-level national public health strategy. For example, to help prevent opioid misuse and opioid use disorder to begin with, such strategies might include: consideration of structural factors that increase risk, such as racism and poverty, and social factors that create isolation; improving data collection so that resources can be better allocated; safer prescribing; campaigns to reduce stigma; increased funding for additional harm reduction measures, treatment expansion, and community-based recovery support services; criminal justice reform that no longer criminalizes drug use and offers treatment and harm reduction services as alternatives; and regulatory changes. Importantly, however, there remain key empirical questions regarding what strategies should be used in an ideal public health approach to stem the overdose crisis. In addition to a comprehensive strategy to address the crisis, prevention of opioid use disorder is also critically important. Prevention strategies ideally would reduce known risk factors and increase protective factors, such as fostering the development of self-regulation and promoting environments that facilitate involved caregivers and neighborhood attachment.
To conclude, researchers in this study found that scaling up the distribution of take-home naloxone to individuals who are prescribed opioids was a cost-effective strategy to save lives from opioid overdoses. This strategy is a critically needed addition to a multi-level, public health approach for addressing the opioid overdose crisis and preventing opioid use disorder.
- LIMITATIONS
-
- The costs per life saved were only based on estimated costs of providing naloxone and ambulance calls. Actual costs may be higher because of other needs for scaling up naloxone provision that were not included, such as education campaigns and training for pharmacists and other prescribers.
- Individuals who were prescribed less than 50 milligrams of oral morphine equivalents were not included in the model. However, they may also be at risk for overdose and might benefit from being provided with naloxone.
- The costs of naloxone and the number of deaths from overdoses were based on current numbers. However, future changes in these variables could affect the cost per life saved.
- Because this study involved a simulation, the researchers needed to make a number of decisions for the model. If another research team conducted the same study, but made different decisions regarding the simulation, the results may have been different.
BOTTOM LINE
The study findings show that scaling up the distribution of take-home naloxone to individuals who are prescribed opioids is a cost-effective strategy to save lives from opioid overdoses. The cost per life saved is estimated to be approximately $30,000 (USD). This strategy appears to be an important addition to a comprehensive set of intervention and prevention efforts, as well as policy, to achieve maximum public health impact.
- For individuals and families seeking recovery: The study findings show that individuals who are prescribed opioids benefit from being provided with naloxone and overdose response training. While distribution of take-home naloxone is not routinely practiced yet, study results suggest that it would be beneficial for individuals who use prescription opioids and their loved ones to obtain naloxone and training for responding to an overdose. In the United States, access varies by state, but in many states naloxone can be obtained through a third-party prescription or without a prescription from a pharmacist. Further, these individuals and their families can consult online resources that provide information on how to safely respond to an overdose.
- For treatment professionals and treatment systems: Treatment professionals can encourage their patients who use prescription opioids and their families to obtain naloxone and training for responding to an overdose. Further, given the barriers to increasing the supply of naloxone to individuals who use prescription opioids that involve pharmacists’ lack of knowledge and awareness, healthcare and treatment systems can promote training and awareness-raising campaigns for pharmacists, as well as stigma reduction campaigns to unlink associations of naloxone with illicit substance use.
- For scientists: While there is a substantial amount of research evidence demonstrating the effectiveness of take-home naloxone in decreasing overdose deaths among people who use opioids outside of prescriptions, the current study is one of the first to examine its effectiveness among people who are prescribed opioids. Accordingly, much more research is needed to investigate the effectiveness of naloxone in decreasing deaths among this less often studied population, given that they are at high-risk for overdoses and the current study results suggesting that it may be a promising strategy. In addition, future research is needed to replicate and extend the findings here, given the number of decision points made in a simulation study like this one. Finally, research on best practices for increasing pharmacists’ knowledge and awareness about naloxone use may help to increase their confidence and decrease stigma.
- For policy makers: Given the promising results of this simulation study showing that distribution of take-home naloxone to individuals who are prescribed opioids is a cost-effective strategy that can save lives, funding is needed for research to replicate and extend these findings, and to investigate the impact and costs of implementing this intervention. Further, funding to promote training and awareness-raising campaigns for pharmacists, as well as stigma reduction campaigns to unlink associations of naloxone with illicit substance use, may lead to more naloxone distribution, which can save lives. Beyond this study, however, there is a substantial amount of research demonstrating the effectiveness of take-home naloxone in decreasing overdose deaths among people who use opioids outside of prescriptions. Accordingly, policies should support implementation of this approach at-scale, but as part of coordinated, multi-level public health approaches for addressing the opioid crisis and preventing opioid use disorder.
CITATIONS
Nielsen, S., Scott, N., Tidhar, T., del Mar Quiroga, M., Lenton, S., & Dietze, P. (2022). The cost and impact of distributing naloxone to people who are prescribed opioids to prevent opioid-related deaths: Findings from a modelling study. Addiction, 117(4), 1009-1019. doi: 10.1111/add.15727
