Provider knowledge about supervised consumption sites is associated with more positive attitudes
Healthcare providers’ knowledge about supervised consumption sites can influence their attitudes, which subsequently can influence their harm reduction practices. This study examined the association between supervised consumption site knowledge and attitudes, and which profession had the most knowledge and most positive attitudes.
Overdose prevention sites – also called supervised consumption sites – are one of several harm reduction approaches to help address the ongoing opioid overdose crisis. At these sites, people who use drugs are provided dedicated spaces where their drug use is monitored by trained staff and sterile equipment is provided. Staff are trained to monitor and intervene (e.g., by administering naloxone) if an overdose occurs. In addition to offering people who use drugs sterile equipment, they are also offered guidance for safer drug use, and education about infectious diseases, as well as linkage to healthcare, addiction treatment, and other social services. While research has been difficult to conduct in the US given drug use is illegal federally, existing studies suggest they are associated with a number of public health benefits, including a decrease in overdose deaths, safer injection practices, linkages to healthcare, greater engagement in addiction treatment, and decreases in reports of injecting drugs in public.
Despite these benefits, there is considerable pushback from communities due to concerns about potential increases in crime and drug use in the areas surrounding an overdose prevention site, as well as concerns about cost. While US research on supervised consumption sites is limited, a systematic review of research conducted in Canada, Australia, and Europe suggests that implementation of supervised consumption sites is not associated with increased crime and drug use and can be cost-effective.
Healthcare providers’ experience with people who use drugs and their knowledge about supervised consumption sites can influence their attitudes and views about these sites, which can, in turn, influence how likely they are to implement harm reduction strategies in their practice. Researchers in this study examined this possible association between providers’ knowledge and attitudes regarding supervised consumption sites and potential demographic differences. Such research can inform efforts to expand harm reduction strategies through a targeted effort to increase provider knowledge.
Survey data were collected from January 18, 2022 through March 21, 2022. The survey consisted of 21 items assessing demographic information (6 items, including 1 asking how many encounters they have with people who inject drugs daily) and knowledge about (7 items) and attitudes towards (8 items) overdose prevention sites.
Participants were asked to rate the extent to which they agreed with knowledge statements such as, “It is important to keep current on the literature regarding overdose prevention sites,” and “Overdose prevention sites are an effective way to decrease fatalities from drug overdose.” They were also asked to rate the extent to which they agreed with attitude statements such as, “I would volunteer at an overdose prevention site,” and “Overdose prevention sites are beneficial to people who inject drugs.” For completing the study, participants were given the option to be entered into a drawing for a monetary incentive.
The responses across items were averaged to create a score for knowledge and a score for attitudes. Higher average scores reflected more knowledge about supervised consumption sites and more positive attitudes. Analyses tested the correlation between the knowledge score and the attitude score, as well as differences between the scores and demographic groups.
Participants were recruited from the research team’s personal networks of healthcare providers currently practicing in Colorado. This included contacts from local and regional professional associations and health care systems. Providers who were currently licensed and were a doctor of osteopathic medicine, a doctor of medicine, a physician’s assistant, or a nurse practitioner were eligible to participate.
A total of 698 participants completed the survey. Of these, 39% identified as medical doctors, 27% as doctors of osteopathic medicine, 26% as physician’s assistants, and 7.5% as nurse practitioners. Most were between the ages of 25 and 35 (33%) or 36 and 45 (45%). The majority were affiliated with a harm reduction center (55%) and worked in an urban setting (68.5%). For specialty or department, participants were roughly equal across emergency medicine (23%), internal medicine (16%), urgent care (21%), and family medicine (15%). Fewer reported working in psychiatry (6%), pain management (8%), and surgery (10.5%). Less than 2% reported working in some other specialty.
WHAT DID THIS STUDY FIND?
Higher knowledge scores were associated with higher attitude scores; emergency medicine providers had the most positive attitudes
As providers’ knowledge scores increased, providers’ attitude scores also increased (reflecting more positive attitudes). This was shown to be a strong correlation.
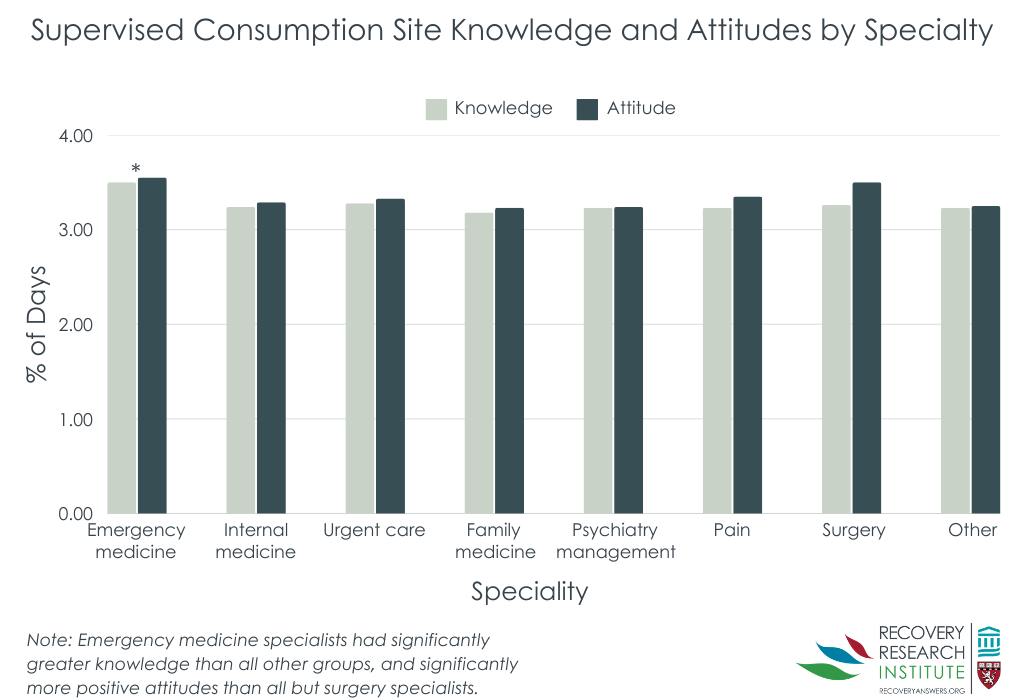
As shown in the figure below, emergency medicine providers had the highest knowledge and attitude scores when compared to all other specialties, while providers practicing in family medicine, psychiatry, and some other specialty had the lowest. Likewise, participants who were affiliated with a harm reduction center exhibited the highest knowledge and attitude scores, as compared to those who were not affiliated and when the affiliation was unknown.
There were no differences in either knowledge or attitude scores between professional disciplines (i.e., whether they were a doctor of osteopathic medicine, a doctor of medicine, a physician assistant, or a nurse practitioner). There were also no differences in knowledge scores across age groups, but there was a difference in attitude scores across age groups. Participants who were 56 to 65 reported less positive attitudes about supervised consumption sites than all other age groups.
Higher scores were associated with more encounters with people who use drugs, up to a point
As providers’ number of encounters with people who inject drugs during a typical workday increased, their knowledge and attitude scores also increased, plateauing at 8 encounters per day. At which point, those with 9 encounters per day with people who use drugs, their knowledge and attitude scores dropped substantially. These providers exhibited the lowest knowledge scores across providers who had all other numbers of encounters and lower attitude scores than providers who encountered 3-8 people who inject drugs in a typical workday (but there was no difference when the number of encounters was less than 3).
To further explore this trend, the research team tested potential differences among provider specialty and harm reduction center affiliation. There were no differences by provider specialty, but there was a difference by harm reduction center affiliation. The majority of providers (58%) who encountered less than 9 people who inject drugs in a typical workday know they are affiliated with a harm reduction center, while many (49%) who see more than 9 in a typical workday do not know if they are affiliated.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the association between healthcare providers’ knowledge and attitudes about supervised consumption sites and potential group differences by demographics. Results showed a strong association between knowledge and attitudes, such that as provider knowledge increased, so did their positive attitudes towards supervised consumption sites. It is also possible that those who have more positive attitudes about harm reduction and overdose prevention are more likely to show greater interest and educate themselves more about them. Nevertheless, the findings may suggest that efforts that target healthcare providers’ knowledge may influence their attitudes, which in turn, can help increase the implementation of harm reduction strategies. Indeed, research has identified that a lack of education was a significant barrier to implementing harm reduction strategies, such as prescribing take-home naloxone.
Among group differences, emergency medicine providers had the highest knowledge and attitude scores in comparison to all other specialties. This likely reflects their experience with opioid-related emergencies and suggests that the emergency department visits are opportune times to link individuals with harm reduction strategies and resources, which is consistent with prior research showing that offering people with substance use disorder who present to the emergency department addiction services reduces the likelihood that they will return. Likewise, providers affiliated with a harm reduction center also had the highest knowledge and attitude scores when compared to those not affiliated with a harm reduction center or when the affiliation was unknown. This suggests that increasing collaboration between healthcare centers and harm reduction centers may improve the knowledge and attitudes of providers not already affiliated with a harm reduction center.
Finally, higher knowledge and attitude scores were associated with the number of people who use drugs that providers encounter in a typical workday up until 8 people, at which point the trend reversed. This may reflect that exposure to people who use drugs increases understanding and empathy for them, but with the highest number of encounters, providers may have started experiencing burnout and compassion fatigue. This finding may also be partially explained by whether the provider had an understanding of whether they worked in a center affiliated with harm reduction, which further supports the potential value of increased collaboration between healthcare centers and harm reduction centers.
The study was conducted in Colorado, which has more progressive drug laws (e.g., for recreational cannabis) and more favorable views towards harm reduction, reflecting an openness toward public health approaches to opioid and other drug use. Results may therefore not generalize to other US states with less favorable views or to other countries.
Similarly, the study was conducted with healthcare providers who worked as doctors of osteopathic medicine, doctors of medicine, physician’s assistants, or nurse practitioners. Their knowledge and attitudes may not be reflective of other types of healthcare providers or mental health clinicians, especially those working in harm reduction or addiction counseling.
The study’s method of examining a correlation prevents the researchers from concluding that an increase in provider knowledge causes an increase in positive attitudes. As noted above, it is also possible that those who have more positive attitudes about harm reduction and overdose prevention are more likely to show greater interest and educate themselves more about them.
BOTTOM LINE
There was a strong association between providers’ knowledge of supervised consumption sites and their positive attitudes towards them. Emergency medicine providers had the highest knowledge and attitude scores compared to other disciplines, and those who were affiliated with a harm reduction center (versus not) also had greater knowledge and more positive attitudes. Higher knowledge and attitude scores were also associated with the number of people who use drugs that providers encounter in a typical workday up until 8 people, at which point the trend reversed, which may reflect burnout and compassion fatigue.
For individuals and families seeking recovery: This study found that healthcare providers’ knowledge of supervised consumption sites was associated with positive attitudes towards them. Emergency medicine providers, those who were affiliated with a harm reduction center, and those who had daily encounters with people who use drugs (until a point) had the most positive attitudes. This may suggest that exposure to people who use drugs, whether through an emergency department, harm reduction center, or otherwise, increases knowledge, which could in turn increases positive attitudes about harm reduction approaches. Accordingly, individuals and their families who speak out about their experiences may increase exposure and reduce stigma, thereby increasing provider knowledge and positive attitudes.
For treatment professionals and treatment systems: This study showed a strong association between healthcare providers’ knowledge of supervised consumption sites and positive attitudes towards them. Knowledge was highest and attitudes most positive especially among emergency medicine providers (compared to other disciplines) and those who were affiliated with a harm reduction center (versus not). Accordingly, treatment systems might leverage emergency department visits to link patients with harm reduction resources. Further, systems that aim to increase collaboration with harm reduction centers may increase knowledge and positive attitudes, which may in turn influence providers’ harm reduction practices.
For scientists: Because the current study was conducted in Colorado, which has progressive drug laws and generally favorable views of harm reduction, future research in other states with more negative views and restrictive policies would further explain how healthcare providers’ knowledge is associated with their attitudes, and whether the demographic differences generalize to other states. Additionally, more sophisticated study designs that go beyond correlations could help shed light on the extent to which knowledge causes attitude changes. Likewise, research that goes one step further to examine associations between knowledge and attitudes with actual harm reduction practices would inform efforts to improve implementation.
For policy makers: This study’s findings that healthcare providers’ knowledge of supervised consumption sites was associated with more positive attitudes towards them, and emergency medicine providers (versus other disciplines), those who were affiliated with a harm reduction center (versus not), and those who had daily encounters with people who use drugs (until a point) had the highest knowledge and most positive attitudes. This may suggest that exposure to people who use drugs increases knowledge, which increases positive attitudes about harm reduction approaches. This may be because exposure can help to reduce stigma and increase empathy. Accordingly, policies that help support people who use drugs in sharing their experiences and promoting collaboration with them may likewise increase provider knowledge and positive attitudes. Further, supervised consumption sites are currently not officially approved of in the US, but have shown to be associated with public health benefits without increasing crime and drug use in the surrounding areas. Therefore, policies that support implementation of these harm reduction resources may likewise be associated with public health benefits, such as reductions in overdose deaths.
Overdose prevention sites – also called supervised consumption sites – are one of several harm reduction approaches to help address the ongoing opioid overdose crisis. At these sites, people who use drugs are provided dedicated spaces where their drug use is monitored by trained staff and sterile equipment is provided. Staff are trained to monitor and intervene (e.g., by administering naloxone) if an overdose occurs. In addition to offering people who use drugs sterile equipment, they are also offered guidance for safer drug use, and education about infectious diseases, as well as linkage to healthcare, addiction treatment, and other social services. While research has been difficult to conduct in the US given drug use is illegal federally, existing studies suggest they are associated with a number of public health benefits, including a decrease in overdose deaths, safer injection practices, linkages to healthcare, greater engagement in addiction treatment, and decreases in reports of injecting drugs in public.
Despite these benefits, there is considerable pushback from communities due to concerns about potential increases in crime and drug use in the areas surrounding an overdose prevention site, as well as concerns about cost. While US research on supervised consumption sites is limited, a systematic review of research conducted in Canada, Australia, and Europe suggests that implementation of supervised consumption sites is not associated with increased crime and drug use and can be cost-effective.
Healthcare providers’ experience with people who use drugs and their knowledge about supervised consumption sites can influence their attitudes and views about these sites, which can, in turn, influence how likely they are to implement harm reduction strategies in their practice. Researchers in this study examined this possible association between providers’ knowledge and attitudes regarding supervised consumption sites and potential demographic differences. Such research can inform efforts to expand harm reduction strategies through a targeted effort to increase provider knowledge.
Survey data were collected from January 18, 2022 through March 21, 2022. The survey consisted of 21 items assessing demographic information (6 items, including 1 asking how many encounters they have with people who inject drugs daily) and knowledge about (7 items) and attitudes towards (8 items) overdose prevention sites.
Participants were asked to rate the extent to which they agreed with knowledge statements such as, “It is important to keep current on the literature regarding overdose prevention sites,” and “Overdose prevention sites are an effective way to decrease fatalities from drug overdose.” They were also asked to rate the extent to which they agreed with attitude statements such as, “I would volunteer at an overdose prevention site,” and “Overdose prevention sites are beneficial to people who inject drugs.” For completing the study, participants were given the option to be entered into a drawing for a monetary incentive.
The responses across items were averaged to create a score for knowledge and a score for attitudes. Higher average scores reflected more knowledge about supervised consumption sites and more positive attitudes. Analyses tested the correlation between the knowledge score and the attitude score, as well as differences between the scores and demographic groups.
Participants were recruited from the research team’s personal networks of healthcare providers currently practicing in Colorado. This included contacts from local and regional professional associations and health care systems. Providers who were currently licensed and were a doctor of osteopathic medicine, a doctor of medicine, a physician’s assistant, or a nurse practitioner were eligible to participate.
A total of 698 participants completed the survey. Of these, 39% identified as medical doctors, 27% as doctors of osteopathic medicine, 26% as physician’s assistants, and 7.5% as nurse practitioners. Most were between the ages of 25 and 35 (33%) or 36 and 45 (45%). The majority were affiliated with a harm reduction center (55%) and worked in an urban setting (68.5%). For specialty or department, participants were roughly equal across emergency medicine (23%), internal medicine (16%), urgent care (21%), and family medicine (15%). Fewer reported working in psychiatry (6%), pain management (8%), and surgery (10.5%). Less than 2% reported working in some other specialty.
WHAT DID THIS STUDY FIND?
Higher knowledge scores were associated with higher attitude scores; emergency medicine providers had the most positive attitudes
As providers’ knowledge scores increased, providers’ attitude scores also increased (reflecting more positive attitudes). This was shown to be a strong correlation.
As shown in the figure below, emergency medicine providers had the highest knowledge and attitude scores when compared to all other specialties, while providers practicing in family medicine, psychiatry, and some other specialty had the lowest. Likewise, participants who were affiliated with a harm reduction center exhibited the highest knowledge and attitude scores, as compared to those who were not affiliated and when the affiliation was unknown.
There were no differences in either knowledge or attitude scores between professional disciplines (i.e., whether they were a doctor of osteopathic medicine, a doctor of medicine, a physician assistant, or a nurse practitioner). There were also no differences in knowledge scores across age groups, but there was a difference in attitude scores across age groups. Participants who were 56 to 65 reported less positive attitudes about supervised consumption sites than all other age groups.
Higher scores were associated with more encounters with people who use drugs, up to a point
As providers’ number of encounters with people who inject drugs during a typical workday increased, their knowledge and attitude scores also increased, plateauing at 8 encounters per day. At which point, those with 9 encounters per day with people who use drugs, their knowledge and attitude scores dropped substantially. These providers exhibited the lowest knowledge scores across providers who had all other numbers of encounters and lower attitude scores than providers who encountered 3-8 people who inject drugs in a typical workday (but there was no difference when the number of encounters was less than 3).
To further explore this trend, the research team tested potential differences among provider specialty and harm reduction center affiliation. There were no differences by provider specialty, but there was a difference by harm reduction center affiliation. The majority of providers (58%) who encountered less than 9 people who inject drugs in a typical workday know they are affiliated with a harm reduction center, while many (49%) who see more than 9 in a typical workday do not know if they are affiliated.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the association between healthcare providers’ knowledge and attitudes about supervised consumption sites and potential group differences by demographics. Results showed a strong association between knowledge and attitudes, such that as provider knowledge increased, so did their positive attitudes towards supervised consumption sites. It is also possible that those who have more positive attitudes about harm reduction and overdose prevention are more likely to show greater interest and educate themselves more about them. Nevertheless, the findings may suggest that efforts that target healthcare providers’ knowledge may influence their attitudes, which in turn, can help increase the implementation of harm reduction strategies. Indeed, research has identified that a lack of education was a significant barrier to implementing harm reduction strategies, such as prescribing take-home naloxone.
Among group differences, emergency medicine providers had the highest knowledge and attitude scores in comparison to all other specialties. This likely reflects their experience with opioid-related emergencies and suggests that the emergency department visits are opportune times to link individuals with harm reduction strategies and resources, which is consistent with prior research showing that offering people with substance use disorder who present to the emergency department addiction services reduces the likelihood that they will return. Likewise, providers affiliated with a harm reduction center also had the highest knowledge and attitude scores when compared to those not affiliated with a harm reduction center or when the affiliation was unknown. This suggests that increasing collaboration between healthcare centers and harm reduction centers may improve the knowledge and attitudes of providers not already affiliated with a harm reduction center.
Finally, higher knowledge and attitude scores were associated with the number of people who use drugs that providers encounter in a typical workday up until 8 people, at which point the trend reversed. This may reflect that exposure to people who use drugs increases understanding and empathy for them, but with the highest number of encounters, providers may have started experiencing burnout and compassion fatigue. This finding may also be partially explained by whether the provider had an understanding of whether they worked in a center affiliated with harm reduction, which further supports the potential value of increased collaboration between healthcare centers and harm reduction centers.
The study was conducted in Colorado, which has more progressive drug laws (e.g., for recreational cannabis) and more favorable views towards harm reduction, reflecting an openness toward public health approaches to opioid and other drug use. Results may therefore not generalize to other US states with less favorable views or to other countries.
Similarly, the study was conducted with healthcare providers who worked as doctors of osteopathic medicine, doctors of medicine, physician’s assistants, or nurse practitioners. Their knowledge and attitudes may not be reflective of other types of healthcare providers or mental health clinicians, especially those working in harm reduction or addiction counseling.
The study’s method of examining a correlation prevents the researchers from concluding that an increase in provider knowledge causes an increase in positive attitudes. As noted above, it is also possible that those who have more positive attitudes about harm reduction and overdose prevention are more likely to show greater interest and educate themselves more about them.
BOTTOM LINE
There was a strong association between providers’ knowledge of supervised consumption sites and their positive attitudes towards them. Emergency medicine providers had the highest knowledge and attitude scores compared to other disciplines, and those who were affiliated with a harm reduction center (versus not) also had greater knowledge and more positive attitudes. Higher knowledge and attitude scores were also associated with the number of people who use drugs that providers encounter in a typical workday up until 8 people, at which point the trend reversed, which may reflect burnout and compassion fatigue.
For individuals and families seeking recovery: This study found that healthcare providers’ knowledge of supervised consumption sites was associated with positive attitudes towards them. Emergency medicine providers, those who were affiliated with a harm reduction center, and those who had daily encounters with people who use drugs (until a point) had the most positive attitudes. This may suggest that exposure to people who use drugs, whether through an emergency department, harm reduction center, or otherwise, increases knowledge, which could in turn increases positive attitudes about harm reduction approaches. Accordingly, individuals and their families who speak out about their experiences may increase exposure and reduce stigma, thereby increasing provider knowledge and positive attitudes.
For treatment professionals and treatment systems: This study showed a strong association between healthcare providers’ knowledge of supervised consumption sites and positive attitudes towards them. Knowledge was highest and attitudes most positive especially among emergency medicine providers (compared to other disciplines) and those who were affiliated with a harm reduction center (versus not). Accordingly, treatment systems might leverage emergency department visits to link patients with harm reduction resources. Further, systems that aim to increase collaboration with harm reduction centers may increase knowledge and positive attitudes, which may in turn influence providers’ harm reduction practices.
For scientists: Because the current study was conducted in Colorado, which has progressive drug laws and generally favorable views of harm reduction, future research in other states with more negative views and restrictive policies would further explain how healthcare providers’ knowledge is associated with their attitudes, and whether the demographic differences generalize to other states. Additionally, more sophisticated study designs that go beyond correlations could help shed light on the extent to which knowledge causes attitude changes. Likewise, research that goes one step further to examine associations between knowledge and attitudes with actual harm reduction practices would inform efforts to improve implementation.
For policy makers: This study’s findings that healthcare providers’ knowledge of supervised consumption sites was associated with more positive attitudes towards them, and emergency medicine providers (versus other disciplines), those who were affiliated with a harm reduction center (versus not), and those who had daily encounters with people who use drugs (until a point) had the highest knowledge and most positive attitudes. This may suggest that exposure to people who use drugs increases knowledge, which increases positive attitudes about harm reduction approaches. This may be because exposure can help to reduce stigma and increase empathy. Accordingly, policies that help support people who use drugs in sharing their experiences and promoting collaboration with them may likewise increase provider knowledge and positive attitudes. Further, supervised consumption sites are currently not officially approved of in the US, but have shown to be associated with public health benefits without increasing crime and drug use in the surrounding areas. Therefore, policies that support implementation of these harm reduction resources may likewise be associated with public health benefits, such as reductions in overdose deaths.
Overdose prevention sites – also called supervised consumption sites – are one of several harm reduction approaches to help address the ongoing opioid overdose crisis. At these sites, people who use drugs are provided dedicated spaces where their drug use is monitored by trained staff and sterile equipment is provided. Staff are trained to monitor and intervene (e.g., by administering naloxone) if an overdose occurs. In addition to offering people who use drugs sterile equipment, they are also offered guidance for safer drug use, and education about infectious diseases, as well as linkage to healthcare, addiction treatment, and other social services. While research has been difficult to conduct in the US given drug use is illegal federally, existing studies suggest they are associated with a number of public health benefits, including a decrease in overdose deaths, safer injection practices, linkages to healthcare, greater engagement in addiction treatment, and decreases in reports of injecting drugs in public.
Despite these benefits, there is considerable pushback from communities due to concerns about potential increases in crime and drug use in the areas surrounding an overdose prevention site, as well as concerns about cost. While US research on supervised consumption sites is limited, a systematic review of research conducted in Canada, Australia, and Europe suggests that implementation of supervised consumption sites is not associated with increased crime and drug use and can be cost-effective.
Healthcare providers’ experience with people who use drugs and their knowledge about supervised consumption sites can influence their attitudes and views about these sites, which can, in turn, influence how likely they are to implement harm reduction strategies in their practice. Researchers in this study examined this possible association between providers’ knowledge and attitudes regarding supervised consumption sites and potential demographic differences. Such research can inform efforts to expand harm reduction strategies through a targeted effort to increase provider knowledge.
Survey data were collected from January 18, 2022 through March 21, 2022. The survey consisted of 21 items assessing demographic information (6 items, including 1 asking how many encounters they have with people who inject drugs daily) and knowledge about (7 items) and attitudes towards (8 items) overdose prevention sites.
Participants were asked to rate the extent to which they agreed with knowledge statements such as, “It is important to keep current on the literature regarding overdose prevention sites,” and “Overdose prevention sites are an effective way to decrease fatalities from drug overdose.” They were also asked to rate the extent to which they agreed with attitude statements such as, “I would volunteer at an overdose prevention site,” and “Overdose prevention sites are beneficial to people who inject drugs.” For completing the study, participants were given the option to be entered into a drawing for a monetary incentive.
The responses across items were averaged to create a score for knowledge and a score for attitudes. Higher average scores reflected more knowledge about supervised consumption sites and more positive attitudes. Analyses tested the correlation between the knowledge score and the attitude score, as well as differences between the scores and demographic groups.
Participants were recruited from the research team’s personal networks of healthcare providers currently practicing in Colorado. This included contacts from local and regional professional associations and health care systems. Providers who were currently licensed and were a doctor of osteopathic medicine, a doctor of medicine, a physician’s assistant, or a nurse practitioner were eligible to participate.
A total of 698 participants completed the survey. Of these, 39% identified as medical doctors, 27% as doctors of osteopathic medicine, 26% as physician’s assistants, and 7.5% as nurse practitioners. Most were between the ages of 25 and 35 (33%) or 36 and 45 (45%). The majority were affiliated with a harm reduction center (55%) and worked in an urban setting (68.5%). For specialty or department, participants were roughly equal across emergency medicine (23%), internal medicine (16%), urgent care (21%), and family medicine (15%). Fewer reported working in psychiatry (6%), pain management (8%), and surgery (10.5%). Less than 2% reported working in some other specialty.
WHAT DID THIS STUDY FIND?
Higher knowledge scores were associated with higher attitude scores; emergency medicine providers had the most positive attitudes
As providers’ knowledge scores increased, providers’ attitude scores also increased (reflecting more positive attitudes). This was shown to be a strong correlation.
As shown in the figure below, emergency medicine providers had the highest knowledge and attitude scores when compared to all other specialties, while providers practicing in family medicine, psychiatry, and some other specialty had the lowest. Likewise, participants who were affiliated with a harm reduction center exhibited the highest knowledge and attitude scores, as compared to those who were not affiliated and when the affiliation was unknown.
There were no differences in either knowledge or attitude scores between professional disciplines (i.e., whether they were a doctor of osteopathic medicine, a doctor of medicine, a physician assistant, or a nurse practitioner). There were also no differences in knowledge scores across age groups, but there was a difference in attitude scores across age groups. Participants who were 56 to 65 reported less positive attitudes about supervised consumption sites than all other age groups.
Higher scores were associated with more encounters with people who use drugs, up to a point
As providers’ number of encounters with people who inject drugs during a typical workday increased, their knowledge and attitude scores also increased, plateauing at 8 encounters per day. At which point, those with 9 encounters per day with people who use drugs, their knowledge and attitude scores dropped substantially. These providers exhibited the lowest knowledge scores across providers who had all other numbers of encounters and lower attitude scores than providers who encountered 3-8 people who inject drugs in a typical workday (but there was no difference when the number of encounters was less than 3).
To further explore this trend, the research team tested potential differences among provider specialty and harm reduction center affiliation. There were no differences by provider specialty, but there was a difference by harm reduction center affiliation. The majority of providers (58%) who encountered less than 9 people who inject drugs in a typical workday know they are affiliated with a harm reduction center, while many (49%) who see more than 9 in a typical workday do not know if they are affiliated.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team examined the association between healthcare providers’ knowledge and attitudes about supervised consumption sites and potential group differences by demographics. Results showed a strong association between knowledge and attitudes, such that as provider knowledge increased, so did their positive attitudes towards supervised consumption sites. It is also possible that those who have more positive attitudes about harm reduction and overdose prevention are more likely to show greater interest and educate themselves more about them. Nevertheless, the findings may suggest that efforts that target healthcare providers’ knowledge may influence their attitudes, which in turn, can help increase the implementation of harm reduction strategies. Indeed, research has identified that a lack of education was a significant barrier to implementing harm reduction strategies, such as prescribing take-home naloxone.
Among group differences, emergency medicine providers had the highest knowledge and attitude scores in comparison to all other specialties. This likely reflects their experience with opioid-related emergencies and suggests that the emergency department visits are opportune times to link individuals with harm reduction strategies and resources, which is consistent with prior research showing that offering people with substance use disorder who present to the emergency department addiction services reduces the likelihood that they will return. Likewise, providers affiliated with a harm reduction center also had the highest knowledge and attitude scores when compared to those not affiliated with a harm reduction center or when the affiliation was unknown. This suggests that increasing collaboration between healthcare centers and harm reduction centers may improve the knowledge and attitudes of providers not already affiliated with a harm reduction center.
Finally, higher knowledge and attitude scores were associated with the number of people who use drugs that providers encounter in a typical workday up until 8 people, at which point the trend reversed. This may reflect that exposure to people who use drugs increases understanding and empathy for them, but with the highest number of encounters, providers may have started experiencing burnout and compassion fatigue. This finding may also be partially explained by whether the provider had an understanding of whether they worked in a center affiliated with harm reduction, which further supports the potential value of increased collaboration between healthcare centers and harm reduction centers.
The study was conducted in Colorado, which has more progressive drug laws (e.g., for recreational cannabis) and more favorable views towards harm reduction, reflecting an openness toward public health approaches to opioid and other drug use. Results may therefore not generalize to other US states with less favorable views or to other countries.
Similarly, the study was conducted with healthcare providers who worked as doctors of osteopathic medicine, doctors of medicine, physician’s assistants, or nurse practitioners. Their knowledge and attitudes may not be reflective of other types of healthcare providers or mental health clinicians, especially those working in harm reduction or addiction counseling.
The study’s method of examining a correlation prevents the researchers from concluding that an increase in provider knowledge causes an increase in positive attitudes. As noted above, it is also possible that those who have more positive attitudes about harm reduction and overdose prevention are more likely to show greater interest and educate themselves more about them.
BOTTOM LINE
There was a strong association between providers’ knowledge of supervised consumption sites and their positive attitudes towards them. Emergency medicine providers had the highest knowledge and attitude scores compared to other disciplines, and those who were affiliated with a harm reduction center (versus not) also had greater knowledge and more positive attitudes. Higher knowledge and attitude scores were also associated with the number of people who use drugs that providers encounter in a typical workday up until 8 people, at which point the trend reversed, which may reflect burnout and compassion fatigue.
For individuals and families seeking recovery: This study found that healthcare providers’ knowledge of supervised consumption sites was associated with positive attitudes towards them. Emergency medicine providers, those who were affiliated with a harm reduction center, and those who had daily encounters with people who use drugs (until a point) had the most positive attitudes. This may suggest that exposure to people who use drugs, whether through an emergency department, harm reduction center, or otherwise, increases knowledge, which could in turn increases positive attitudes about harm reduction approaches. Accordingly, individuals and their families who speak out about their experiences may increase exposure and reduce stigma, thereby increasing provider knowledge and positive attitudes.
For treatment professionals and treatment systems: This study showed a strong association between healthcare providers’ knowledge of supervised consumption sites and positive attitudes towards them. Knowledge was highest and attitudes most positive especially among emergency medicine providers (compared to other disciplines) and those who were affiliated with a harm reduction center (versus not). Accordingly, treatment systems might leverage emergency department visits to link patients with harm reduction resources. Further, systems that aim to increase collaboration with harm reduction centers may increase knowledge and positive attitudes, which may in turn influence providers’ harm reduction practices.
For scientists: Because the current study was conducted in Colorado, which has progressive drug laws and generally favorable views of harm reduction, future research in other states with more negative views and restrictive policies would further explain how healthcare providers’ knowledge is associated with their attitudes, and whether the demographic differences generalize to other states. Additionally, more sophisticated study designs that go beyond correlations could help shed light on the extent to which knowledge causes attitude changes. Likewise, research that goes one step further to examine associations between knowledge and attitudes with actual harm reduction practices would inform efforts to improve implementation.
For policy makers: This study’s findings that healthcare providers’ knowledge of supervised consumption sites was associated with more positive attitudes towards them, and emergency medicine providers (versus other disciplines), those who were affiliated with a harm reduction center (versus not), and those who had daily encounters with people who use drugs (until a point) had the highest knowledge and most positive attitudes. This may suggest that exposure to people who use drugs increases knowledge, which increases positive attitudes about harm reduction approaches. This may be because exposure can help to reduce stigma and increase empathy. Accordingly, policies that help support people who use drugs in sharing their experiences and promoting collaboration with them may likewise increase provider knowledge and positive attitudes. Further, supervised consumption sites are currently not officially approved of in the US, but have shown to be associated with public health benefits without increasing crime and drug use in the surrounding areas. Therefore, policies that support implementation of these harm reduction resources may likewise be associated with public health benefits, such as reductions in overdose deaths.