Maybe you can always “get what you want”…if you ask: A study of what the American public wants to know about addiction
Prevention, treatment, and recovery outcomes may be improved if knowledge about addiction is increased. However, most clinical and public health communication is based on assumptions of what the general public needs or wants to know. This study systematically explored the types of questions the American public has about addiction, both for specific substances like alcohol, cocaine, and opioids, and for behavioral addictions like gambling.
In the late 1990s and early 2000s, millions of Americans watched a dramatic public serviceannouncement: a man held up an egg and declared, “This is your brain.” He then cracked it into a sizzling frying pan. “This is your brain on drugs,” he said, before turning to the camera and asking, “Any questions?” The campaign intended to prevent substance use among youth and cost the U.S. taxpayers approximately $1.4 billion in total. Although the campaign was widely viewed, youth who had seen the campaign were actually more likely to use substances later. This is only one example of an addiction-related messaging campaign that did not match or sync with the actual knowledge deficits or perceptions of harms held by the target audience.
Experts in addiction and public health often make assumptions about what information people want or require to change health behaviors, especially related to substance or behavioral addictions. The lack of alignment at best can be a poor use of financial resources and at worst can actually move the target audience away from the desired behavior change, such as the fried egg “brain on drugs” commercials. Instead, public health and policy communications should be grounded in data-driven understanding about what knowledge specific target populations may be lacking and on what specific dimensions for different types of addiction.
Addiction is a multidimensional and dynamic concept. There are both general aspects of addiction as well as specific components across different types of addictions, including within and across substances (e.g., alcohol, cannabis) and behaviors (e.g., gambling). Depending on the goal of public health and policy communications, the messaging may benefit from being tailored. For example, if the goal is universal prevention, the message may center on risk factors and harmful consequences. If the goal is stigma reduction, the messaging may highlight the biomedical and genetic aspects of addiction. Yet, if the focus is on harm reduction, the messaging may feature overdose prevention strategies and drug checking (e.g., with fentanyl test strips). However, there has not been a systematic investigation on the types of questions the public actually have.
Within and across specific addictions, designers of public health and policy communications could use empirical evidence of the knowledge gaps and desired knowledge to tailor their messaging campaigns, which may increase their impact. This study details qualitative findings from adult Americans that shared their top ten questions on addiction.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional analysis of open-ended survey questions asking the American public to list the top 10 things they wanted to know about addiction in general (n = 211), alcohol addiction (n = 209), cocaine addiction (n = 209), opioid addiction (n = 214), cannabis addiction (n = 209), and gambling addiction (n = 209). The 1,257 participants were recruited from the online crowd-sourcing platform Prolific, which uses word of mouth and social media to recruit participants). Participants were eligible if they were 18 years of age or older, could read and write, and lived in the United States. The survey was estimated to take 10-15 minutes, and participants were compensated $5 for participation. Recruitment took place over 6 days from July 22, 2020, to July 27, 2020.
Each participant was randomly assigned to 1 of the 6 addiction types and asked, “What are the top 10 things you want to know about [substance/behavior] addiction?” Participants that did not list at least 5 questions were excluded. After the approximately 12,000 questions were provided, the study team began a multi-step qualitative coding process whereby they formed domains and subdomains based on emergent themes, which were then confirmed to capture the themes by additional rounds of coding. Frequencies of the domains across each type of addiction were also calculated, and differences in the domains were explored within and across addiction types.
Of the 1,257 adults that participated, and provided at least 5 questions, the majority (51%) identified as female, followed by male (47%) and other (2%) gender identities. The average age was 32, and most (70%) were White identifying, following by Asian (11%), other (7%), and Black (6%). Most (89%) identified as non-Hispanic, and 75% identified as heterosexual. There were 5% that identified as homosexual, and 20% identified with another sexual orientation. The proportion of participants across yearly income amounts were 41% below $45,000, 23 greater than $45,000 but less than $75,000, 16% at least $75,000 but less than $105,000, and 20% greater than $105,000. The average years of education was 15, with 12 years being completed high school. Most (72%) lived with family or relatives, and 41% had a full-time job.
WHAT DID THIS STUDY FIND?
There were 9 unique categories of questions across addiction types
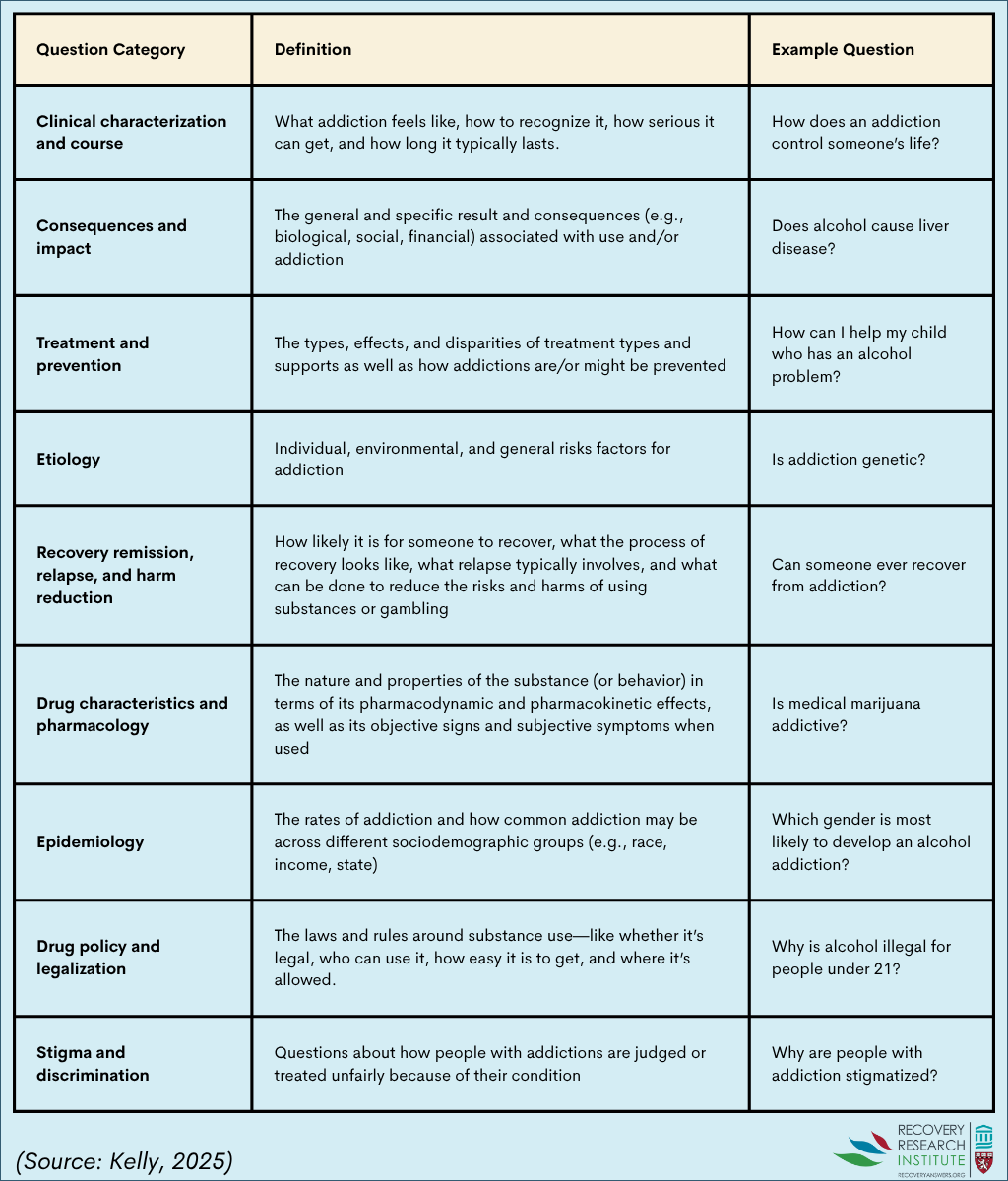
There were 9 unique categories of questions: 1) clinical characterization and course; 2) consequences and impact; 3) treatment and prevention; 4) etiology; 5) recovery remission, relapse, and harm reduction; 6) drug characteristics and pharmacology; 7) epidemiology; 8) drug policy and legalization; and 9) stigma and discrimination. See graphic below for a definition and an example question corresponding with each category.
The proportion of question categories varied depending on the type of addiction asked about
Within each type of addiction asked about (general, alcohol, cannabis, etc.), the proportion of question categories varied (see graphic below). For example, clinical characterization and course was the most common category when alcohol and gambling addiction were asked about. Yet, consequences and impact were the most common when cannabis and cocaine were specified. Treatment and prevention were the most common category when opioid and addiction in general were asked about. Stigma and discrimination ranked last across all addiction types, with drug and policy and legalization second to last in all addiction types except opioid addiction.
(Image source: Kelly, 2025)
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study highlights that the types of addiction-related information that the American public want to know about vary across different addictions and may differ from assumed knowledge gaps. There were 9 categories of questions that appeared across the 6 types of addiction that were asked about (general, alcohol, cannabis, opioid, cocaine, and gambling). The category clinical characterization and course was the most common when alcohol and gambling addiction were asked about. Yet, consequences and impact was the most common when the questions were related to cannabis and cocaine. Treatment and prevention was the most common category when opioid and addiction in general were asked about. Stigma and discrimination ranked last across all addiction types. The substantial variation across addictions and within domains suggests some questions – reflecting knowledge gaps in the American public – may be more pressing than others depending on the type of addiction and the intended audience.
The practice of “scare tactics” and assumed knowledge priorities in addiction messaging may limit effectiveness and, in some cases, lead to unintended consequences—especially when public information needs differ from policy makers’ assumptions. This study highlights the importance of tailoring clinical and public health messages to both the specific type of addiction and the intended audience. Communication and education may be more effective and captivating if tailored based on this systematic investigation of knowledge gaps. For example, stigma has long been a central concern for clinicians, advocates, and recovery support groups. Yet, in this study, questions about stigma and discrimination were the least asked across all addiction types. This may reflect a disconnect between expert priorities and public awareness, as well as a lack of understanding that addiction is among the most heavily stigmatized health conditions worldwide. The low prevalence of stigma-related questions might also point to how deeply stigma is embedded—evident in participants’ frequent use of stigmatizing terms like “addict” in other domains. These findings suggest that efforts to reduce stigma may need to start by addressing foundational gaps in public knowledge about addiction. For instance, messaging could emphasize that addiction is partly rooted in genetics and that repeated substance exposure can alter brain function, reducing a person’s ability to control use. Additional tailoring and language use specific to the type of addiction (e.g., opioid addiction) would likely benefit all messaging campaigns. More research is needed to explore the impact of designing messaging campaigns around the findings from this study.
1. The study participants were not representative of the entire population. Thus, caution should be taken when generalizing the findings to all people in the United States.
The data was collected in 2020 and may not represent the key questions for the public today. However, the study does suggest that more work is needed to identify desired knowledge and gaps in the process of developing messaging campaigns.
The study does not indicate who has which questions across addiction types, and there is likely variation across demographic characteristics for the types of questions individuals may have.
BOTTOM LINE
These findings indicate that the knowledge gaps and related questions the public may have about addiction likely vary across addiction types (e.g., alcohol, cannabis, opioid, cocaine, gambling, general). The categories of questions most prevalent for each substance or behavior could inform, more precisely, clinical and public health messaging campaigns, which may improve relevance, engagement, and ultimately effectiveness for prevention, treatment, and recovery.
For individuals and families seeking recovery: While there are many similarities across different types of addiction, there are also many differences in the different drug effects, clinical course, helpful treatment types and stigmas attached to them. Depending on what type of addictive drug or behavior you or your loved one may be affected by, these differences can influence the nature and types of treatment you engage with. Also, if you or a loved one are curious about addiction and recovery, it’s important to find reliable sources of information because there are a lot of misconceptions about the topic. The Recovery Research Institute’s website has a wealth of information that includes an “Addictionary” which is a free, user-friendly place to explore terms, concepts, and evidence related to addiction and recovery. The NIH and SAMHSA also has valuable information.
For treatment professionals and treatment systems: The public, including service professionals and participants, likely have knowledge gaps and related specific questions surrounding specific types of addictions which do not always align with those assumed by experts. The findings in this study highlight how the categories of addiction-related questions varied across the specific type of addiction asked about. Clinicians and treatment systems that provide person-centered care may benefit from systematically incorporating messaging that is initiated, developed, and informed by participants and those with lived or living experience.
For scientists: The findings from this study highlight how the questions the public may have about addiction varies substantially, particularly based on the type of the substance or behavior. Future research using a nationally representative sample would validate these findings and help understand how questions may also vary across demographic characteristics (e.g., age, education, experience with substances). Additional work is needed to investigate how integrating these findings into clinical and public health messaging campaigns may affect outcomes.
For policy makers: Public health messaging should be grounded in what people actually want to know. The findings in this study highlight 9 categories of questions the American public want to know about addiction. The findings also highlight that the types of knowledge gaps and related questions vary greatly depending on the type of addiction. Developing and funding public health campaigns that differentiate messaging by addiction type (e.g., cannabis, opioids, gambling) and the specific knowledge gaps within those addiction types, may help shift public support for policies and programs that address addiction.
In the late 1990s and early 2000s, millions of Americans watched a dramatic public serviceannouncement: a man held up an egg and declared, “This is your brain.” He then cracked it into a sizzling frying pan. “This is your brain on drugs,” he said, before turning to the camera and asking, “Any questions?” The campaign intended to prevent substance use among youth and cost the U.S. taxpayers approximately $1.4 billion in total. Although the campaign was widely viewed, youth who had seen the campaign were actually more likely to use substances later. This is only one example of an addiction-related messaging campaign that did not match or sync with the actual knowledge deficits or perceptions of harms held by the target audience.
Experts in addiction and public health often make assumptions about what information people want or require to change health behaviors, especially related to substance or behavioral addictions. The lack of alignment at best can be a poor use of financial resources and at worst can actually move the target audience away from the desired behavior change, such as the fried egg “brain on drugs” commercials. Instead, public health and policy communications should be grounded in data-driven understanding about what knowledge specific target populations may be lacking and on what specific dimensions for different types of addiction.
Addiction is a multidimensional and dynamic concept. There are both general aspects of addiction as well as specific components across different types of addictions, including within and across substances (e.g., alcohol, cannabis) and behaviors (e.g., gambling). Depending on the goal of public health and policy communications, the messaging may benefit from being tailored. For example, if the goal is universal prevention, the message may center on risk factors and harmful consequences. If the goal is stigma reduction, the messaging may highlight the biomedical and genetic aspects of addiction. Yet, if the focus is on harm reduction, the messaging may feature overdose prevention strategies and drug checking (e.g., with fentanyl test strips). However, there has not been a systematic investigation on the types of questions the public actually have.
Within and across specific addictions, designers of public health and policy communications could use empirical evidence of the knowledge gaps and desired knowledge to tailor their messaging campaigns, which may increase their impact. This study details qualitative findings from adult Americans that shared their top ten questions on addiction.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional analysis of open-ended survey questions asking the American public to list the top 10 things they wanted to know about addiction in general (n = 211), alcohol addiction (n = 209), cocaine addiction (n = 209), opioid addiction (n = 214), cannabis addiction (n = 209), and gambling addiction (n = 209). The 1,257 participants were recruited from the online crowd-sourcing platform Prolific, which uses word of mouth and social media to recruit participants). Participants were eligible if they were 18 years of age or older, could read and write, and lived in the United States. The survey was estimated to take 10-15 minutes, and participants were compensated $5 for participation. Recruitment took place over 6 days from July 22, 2020, to July 27, 2020.
Each participant was randomly assigned to 1 of the 6 addiction types and asked, “What are the top 10 things you want to know about [substance/behavior] addiction?” Participants that did not list at least 5 questions were excluded. After the approximately 12,000 questions were provided, the study team began a multi-step qualitative coding process whereby they formed domains and subdomains based on emergent themes, which were then confirmed to capture the themes by additional rounds of coding. Frequencies of the domains across each type of addiction were also calculated, and differences in the domains were explored within and across addiction types.
Of the 1,257 adults that participated, and provided at least 5 questions, the majority (51%) identified as female, followed by male (47%) and other (2%) gender identities. The average age was 32, and most (70%) were White identifying, following by Asian (11%), other (7%), and Black (6%). Most (89%) identified as non-Hispanic, and 75% identified as heterosexual. There were 5% that identified as homosexual, and 20% identified with another sexual orientation. The proportion of participants across yearly income amounts were 41% below $45,000, 23 greater than $45,000 but less than $75,000, 16% at least $75,000 but less than $105,000, and 20% greater than $105,000. The average years of education was 15, with 12 years being completed high school. Most (72%) lived with family or relatives, and 41% had a full-time job.
WHAT DID THIS STUDY FIND?
There were 9 unique categories of questions across addiction types
There were 9 unique categories of questions: 1) clinical characterization and course; 2) consequences and impact; 3) treatment and prevention; 4) etiology; 5) recovery remission, relapse, and harm reduction; 6) drug characteristics and pharmacology; 7) epidemiology; 8) drug policy and legalization; and 9) stigma and discrimination. See graphic below for a definition and an example question corresponding with each category.
The proportion of question categories varied depending on the type of addiction asked about
Within each type of addiction asked about (general, alcohol, cannabis, etc.), the proportion of question categories varied (see graphic below). For example, clinical characterization and course was the most common category when alcohol and gambling addiction were asked about. Yet, consequences and impact were the most common when cannabis and cocaine were specified. Treatment and prevention were the most common category when opioid and addiction in general were asked about. Stigma and discrimination ranked last across all addiction types, with drug and policy and legalization second to last in all addiction types except opioid addiction.
(Image source: Kelly, 2025)
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study highlights that the types of addiction-related information that the American public want to know about vary across different addictions and may differ from assumed knowledge gaps. There were 9 categories of questions that appeared across the 6 types of addiction that were asked about (general, alcohol, cannabis, opioid, cocaine, and gambling). The category clinical characterization and course was the most common when alcohol and gambling addiction were asked about. Yet, consequences and impact was the most common when the questions were related to cannabis and cocaine. Treatment and prevention was the most common category when opioid and addiction in general were asked about. Stigma and discrimination ranked last across all addiction types. The substantial variation across addictions and within domains suggests some questions – reflecting knowledge gaps in the American public – may be more pressing than others depending on the type of addiction and the intended audience.
The practice of “scare tactics” and assumed knowledge priorities in addiction messaging may limit effectiveness and, in some cases, lead to unintended consequences—especially when public information needs differ from policy makers’ assumptions. This study highlights the importance of tailoring clinical and public health messages to both the specific type of addiction and the intended audience. Communication and education may be more effective and captivating if tailored based on this systematic investigation of knowledge gaps. For example, stigma has long been a central concern for clinicians, advocates, and recovery support groups. Yet, in this study, questions about stigma and discrimination were the least asked across all addiction types. This may reflect a disconnect between expert priorities and public awareness, as well as a lack of understanding that addiction is among the most heavily stigmatized health conditions worldwide. The low prevalence of stigma-related questions might also point to how deeply stigma is embedded—evident in participants’ frequent use of stigmatizing terms like “addict” in other domains. These findings suggest that efforts to reduce stigma may need to start by addressing foundational gaps in public knowledge about addiction. For instance, messaging could emphasize that addiction is partly rooted in genetics and that repeated substance exposure can alter brain function, reducing a person’s ability to control use. Additional tailoring and language use specific to the type of addiction (e.g., opioid addiction) would likely benefit all messaging campaigns. More research is needed to explore the impact of designing messaging campaigns around the findings from this study.
1. The study participants were not representative of the entire population. Thus, caution should be taken when generalizing the findings to all people in the United States.
The data was collected in 2020 and may not represent the key questions for the public today. However, the study does suggest that more work is needed to identify desired knowledge and gaps in the process of developing messaging campaigns.
The study does not indicate who has which questions across addiction types, and there is likely variation across demographic characteristics for the types of questions individuals may have.
BOTTOM LINE
These findings indicate that the knowledge gaps and related questions the public may have about addiction likely vary across addiction types (e.g., alcohol, cannabis, opioid, cocaine, gambling, general). The categories of questions most prevalent for each substance or behavior could inform, more precisely, clinical and public health messaging campaigns, which may improve relevance, engagement, and ultimately effectiveness for prevention, treatment, and recovery.
For individuals and families seeking recovery: While there are many similarities across different types of addiction, there are also many differences in the different drug effects, clinical course, helpful treatment types and stigmas attached to them. Depending on what type of addictive drug or behavior you or your loved one may be affected by, these differences can influence the nature and types of treatment you engage with. Also, if you or a loved one are curious about addiction and recovery, it’s important to find reliable sources of information because there are a lot of misconceptions about the topic. The Recovery Research Institute’s website has a wealth of information that includes an “Addictionary” which is a free, user-friendly place to explore terms, concepts, and evidence related to addiction and recovery. The NIH and SAMHSA also has valuable information.
For treatment professionals and treatment systems: The public, including service professionals and participants, likely have knowledge gaps and related specific questions surrounding specific types of addictions which do not always align with those assumed by experts. The findings in this study highlight how the categories of addiction-related questions varied across the specific type of addiction asked about. Clinicians and treatment systems that provide person-centered care may benefit from systematically incorporating messaging that is initiated, developed, and informed by participants and those with lived or living experience.
For scientists: The findings from this study highlight how the questions the public may have about addiction varies substantially, particularly based on the type of the substance or behavior. Future research using a nationally representative sample would validate these findings and help understand how questions may also vary across demographic characteristics (e.g., age, education, experience with substances). Additional work is needed to investigate how integrating these findings into clinical and public health messaging campaigns may affect outcomes.
For policy makers: Public health messaging should be grounded in what people actually want to know. The findings in this study highlight 9 categories of questions the American public want to know about addiction. The findings also highlight that the types of knowledge gaps and related questions vary greatly depending on the type of addiction. Developing and funding public health campaigns that differentiate messaging by addiction type (e.g., cannabis, opioids, gambling) and the specific knowledge gaps within those addiction types, may help shift public support for policies and programs that address addiction.
In the late 1990s and early 2000s, millions of Americans watched a dramatic public serviceannouncement: a man held up an egg and declared, “This is your brain.” He then cracked it into a sizzling frying pan. “This is your brain on drugs,” he said, before turning to the camera and asking, “Any questions?” The campaign intended to prevent substance use among youth and cost the U.S. taxpayers approximately $1.4 billion in total. Although the campaign was widely viewed, youth who had seen the campaign were actually more likely to use substances later. This is only one example of an addiction-related messaging campaign that did not match or sync with the actual knowledge deficits or perceptions of harms held by the target audience.
Experts in addiction and public health often make assumptions about what information people want or require to change health behaviors, especially related to substance or behavioral addictions. The lack of alignment at best can be a poor use of financial resources and at worst can actually move the target audience away from the desired behavior change, such as the fried egg “brain on drugs” commercials. Instead, public health and policy communications should be grounded in data-driven understanding about what knowledge specific target populations may be lacking and on what specific dimensions for different types of addiction.
Addiction is a multidimensional and dynamic concept. There are both general aspects of addiction as well as specific components across different types of addictions, including within and across substances (e.g., alcohol, cannabis) and behaviors (e.g., gambling). Depending on the goal of public health and policy communications, the messaging may benefit from being tailored. For example, if the goal is universal prevention, the message may center on risk factors and harmful consequences. If the goal is stigma reduction, the messaging may highlight the biomedical and genetic aspects of addiction. Yet, if the focus is on harm reduction, the messaging may feature overdose prevention strategies and drug checking (e.g., with fentanyl test strips). However, there has not been a systematic investigation on the types of questions the public actually have.
Within and across specific addictions, designers of public health and policy communications could use empirical evidence of the knowledge gaps and desired knowledge to tailor their messaging campaigns, which may increase their impact. This study details qualitative findings from adult Americans that shared their top ten questions on addiction.
HOW WAS THIS STUDY CONDUCTED?
This study was a cross-sectional analysis of open-ended survey questions asking the American public to list the top 10 things they wanted to know about addiction in general (n = 211), alcohol addiction (n = 209), cocaine addiction (n = 209), opioid addiction (n = 214), cannabis addiction (n = 209), and gambling addiction (n = 209). The 1,257 participants were recruited from the online crowd-sourcing platform Prolific, which uses word of mouth and social media to recruit participants). Participants were eligible if they were 18 years of age or older, could read and write, and lived in the United States. The survey was estimated to take 10-15 minutes, and participants were compensated $5 for participation. Recruitment took place over 6 days from July 22, 2020, to July 27, 2020.
Each participant was randomly assigned to 1 of the 6 addiction types and asked, “What are the top 10 things you want to know about [substance/behavior] addiction?” Participants that did not list at least 5 questions were excluded. After the approximately 12,000 questions were provided, the study team began a multi-step qualitative coding process whereby they formed domains and subdomains based on emergent themes, which were then confirmed to capture the themes by additional rounds of coding. Frequencies of the domains across each type of addiction were also calculated, and differences in the domains were explored within and across addiction types.
Of the 1,257 adults that participated, and provided at least 5 questions, the majority (51%) identified as female, followed by male (47%) and other (2%) gender identities. The average age was 32, and most (70%) were White identifying, following by Asian (11%), other (7%), and Black (6%). Most (89%) identified as non-Hispanic, and 75% identified as heterosexual. There were 5% that identified as homosexual, and 20% identified with another sexual orientation. The proportion of participants across yearly income amounts were 41% below $45,000, 23 greater than $45,000 but less than $75,000, 16% at least $75,000 but less than $105,000, and 20% greater than $105,000. The average years of education was 15, with 12 years being completed high school. Most (72%) lived with family or relatives, and 41% had a full-time job.
WHAT DID THIS STUDY FIND?
There were 9 unique categories of questions across addiction types
There were 9 unique categories of questions: 1) clinical characterization and course; 2) consequences and impact; 3) treatment and prevention; 4) etiology; 5) recovery remission, relapse, and harm reduction; 6) drug characteristics and pharmacology; 7) epidemiology; 8) drug policy and legalization; and 9) stigma and discrimination. See graphic below for a definition and an example question corresponding with each category.
The proportion of question categories varied depending on the type of addiction asked about
Within each type of addiction asked about (general, alcohol, cannabis, etc.), the proportion of question categories varied (see graphic below). For example, clinical characterization and course was the most common category when alcohol and gambling addiction were asked about. Yet, consequences and impact were the most common when cannabis and cocaine were specified. Treatment and prevention were the most common category when opioid and addiction in general were asked about. Stigma and discrimination ranked last across all addiction types, with drug and policy and legalization second to last in all addiction types except opioid addiction.
(Image source: Kelly, 2025)
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study highlights that the types of addiction-related information that the American public want to know about vary across different addictions and may differ from assumed knowledge gaps. There were 9 categories of questions that appeared across the 6 types of addiction that were asked about (general, alcohol, cannabis, opioid, cocaine, and gambling). The category clinical characterization and course was the most common when alcohol and gambling addiction were asked about. Yet, consequences and impact was the most common when the questions were related to cannabis and cocaine. Treatment and prevention was the most common category when opioid and addiction in general were asked about. Stigma and discrimination ranked last across all addiction types. The substantial variation across addictions and within domains suggests some questions – reflecting knowledge gaps in the American public – may be more pressing than others depending on the type of addiction and the intended audience.
The practice of “scare tactics” and assumed knowledge priorities in addiction messaging may limit effectiveness and, in some cases, lead to unintended consequences—especially when public information needs differ from policy makers’ assumptions. This study highlights the importance of tailoring clinical and public health messages to both the specific type of addiction and the intended audience. Communication and education may be more effective and captivating if tailored based on this systematic investigation of knowledge gaps. For example, stigma has long been a central concern for clinicians, advocates, and recovery support groups. Yet, in this study, questions about stigma and discrimination were the least asked across all addiction types. This may reflect a disconnect between expert priorities and public awareness, as well as a lack of understanding that addiction is among the most heavily stigmatized health conditions worldwide. The low prevalence of stigma-related questions might also point to how deeply stigma is embedded—evident in participants’ frequent use of stigmatizing terms like “addict” in other domains. These findings suggest that efforts to reduce stigma may need to start by addressing foundational gaps in public knowledge about addiction. For instance, messaging could emphasize that addiction is partly rooted in genetics and that repeated substance exposure can alter brain function, reducing a person’s ability to control use. Additional tailoring and language use specific to the type of addiction (e.g., opioid addiction) would likely benefit all messaging campaigns. More research is needed to explore the impact of designing messaging campaigns around the findings from this study.
1. The study participants were not representative of the entire population. Thus, caution should be taken when generalizing the findings to all people in the United States.
The data was collected in 2020 and may not represent the key questions for the public today. However, the study does suggest that more work is needed to identify desired knowledge and gaps in the process of developing messaging campaigns.
The study does not indicate who has which questions across addiction types, and there is likely variation across demographic characteristics for the types of questions individuals may have.
BOTTOM LINE
These findings indicate that the knowledge gaps and related questions the public may have about addiction likely vary across addiction types (e.g., alcohol, cannabis, opioid, cocaine, gambling, general). The categories of questions most prevalent for each substance or behavior could inform, more precisely, clinical and public health messaging campaigns, which may improve relevance, engagement, and ultimately effectiveness for prevention, treatment, and recovery.
For individuals and families seeking recovery: While there are many similarities across different types of addiction, there are also many differences in the different drug effects, clinical course, helpful treatment types and stigmas attached to them. Depending on what type of addictive drug or behavior you or your loved one may be affected by, these differences can influence the nature and types of treatment you engage with. Also, if you or a loved one are curious about addiction and recovery, it’s important to find reliable sources of information because there are a lot of misconceptions about the topic. The Recovery Research Institute’s website has a wealth of information that includes an “Addictionary” which is a free, user-friendly place to explore terms, concepts, and evidence related to addiction and recovery. The NIH and SAMHSA also has valuable information.
For treatment professionals and treatment systems: The public, including service professionals and participants, likely have knowledge gaps and related specific questions surrounding specific types of addictions which do not always align with those assumed by experts. The findings in this study highlight how the categories of addiction-related questions varied across the specific type of addiction asked about. Clinicians and treatment systems that provide person-centered care may benefit from systematically incorporating messaging that is initiated, developed, and informed by participants and those with lived or living experience.
For scientists: The findings from this study highlight how the questions the public may have about addiction varies substantially, particularly based on the type of the substance or behavior. Future research using a nationally representative sample would validate these findings and help understand how questions may also vary across demographic characteristics (e.g., age, education, experience with substances). Additional work is needed to investigate how integrating these findings into clinical and public health messaging campaigns may affect outcomes.
For policy makers: Public health messaging should be grounded in what people actually want to know. The findings in this study highlight 9 categories of questions the American public want to know about addiction. The findings also highlight that the types of knowledge gaps and related questions vary greatly depending on the type of addiction. Developing and funding public health campaigns that differentiate messaging by addiction type (e.g., cannabis, opioids, gambling) and the specific knowledge gaps within those addiction types, may help shift public support for policies and programs that address addiction.