Supervised consumption site participation unrelated to acute healthcare usage
Supervised consumption sites and embedded harm reduction services like sterile syringe programs could help reduce the use of acute healthcare services among people who inject drugs. This study examined the relationship between the use of supervised consumption sites and the frequency of acute healthcare usage.
Supervised consumption sites, also called overdose prevention sites or safe injection sites, may reduce the use of acute healthcare among people who inject drugs, since these sites can help link people to primary care. These sites also typically offer a number of other services such as provision of sterile drug use equipment, guidance about safer drug use, drug checking, distribution of naloxone, education about and testing for infectious disease, and linkage to addiction treatment and other social services that could potentially alleviate drug use harms and risk for emergency room visits. A recent systematic review of research suggests that supervised consumption sites may be associated with public health benefits.
However, there is some research that suggests that use of supervised consumption sites is associated instead with an increase in use of acute healthcare services, via nurses at the sites who refer people to the hospital after detecting a medical problem, which arguably would be seen as a positive outcome in helping to prevent more serious of life-threatening health harms. However, given the unclear nature of the association and potential benefit of supervised consumption sites reducing the use of acute healthcare, this quasi-experimental study examined the impact of supervised consumption services on the frequency of use of acute healthcare. Such research can help clarify the role that supervised consumption sites have in overall healthcare utilization among people who use drugs, which can highlight how to best provide care for this population and alleviate the demands placed on acute healthcare systems.
HOW WAS THIS STUDY CONDUCTED?
This quasi-experimental study used questionnaire and administrative data to investigate whether different levels of supervised consumption service use (vs. no use) reduced the acute care visits among people who inject drugs in Toronto, Canada, over 6 months, controlling simultaneously for a set of factors associated with the propensity to participate in the sites. A total of 467 participants were included in the current study. Of these, 66% identified as cisgender men and were, on average, 41 years old at baseline. The majority of participants reported injecting drugs daily (56%) and injecting opioids (85%).
The questionnaires assessed the frequency of participants’ use of supervised consumption services and the administrative data provided information about their use of acute care.
Questionnaires were administered as part of the ongoing Ontario Integrated Supervised Injection Services – Toronto study, which evaluated the impact of the first 3 supervised consumption sites that opened in Toronto on clients’ use of healthcare and health outcomes. While the specific services offered typically vary by site, all 3 sites in the study permitted injection use and 2 also allowed oral and intranasal use. People who were recruited for the questionnaire were also asked their permission to have their questionnaire data linked with administrative databases that provided information about their demographics, health (e.g., vitals, HIV status), and health care usage (e.g., emergency department visits, hospitalizations). As the study notes, participants from the supervised consumption site who were linked to records were similar to the overall group at the site on age, gender, injection frequency, and other psychosocial contexts such as recent incarceration. The questionnaire was administered by an interviewer and was completed at baseline and approximately every 6 months following.
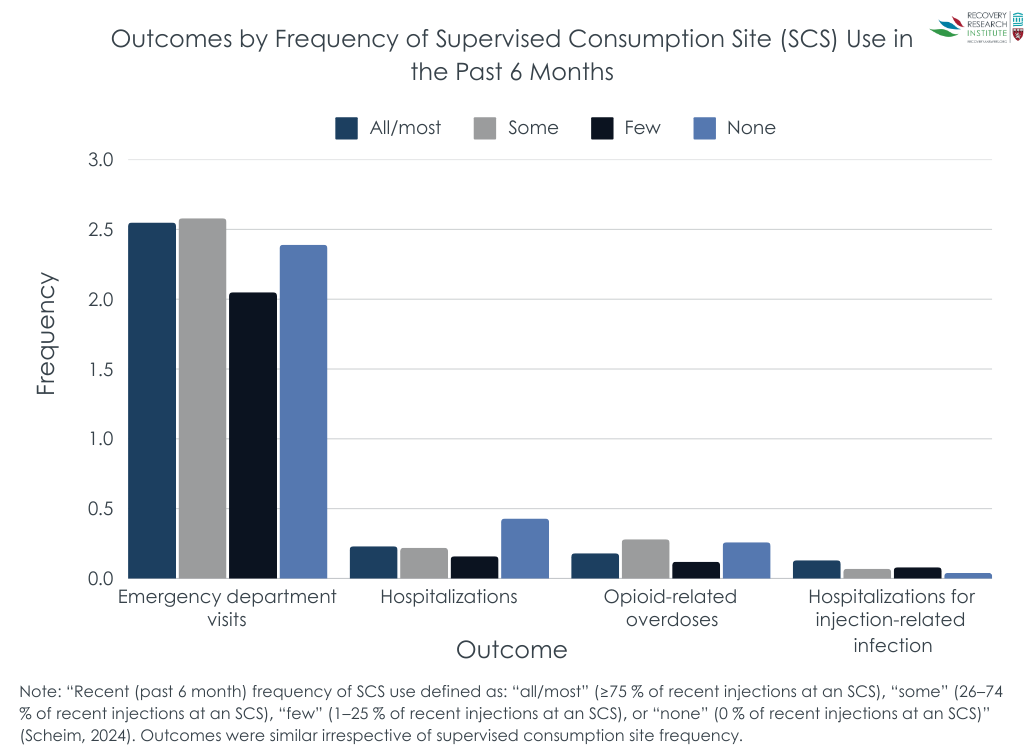
As part of the baseline questionnaire, participants were asked, “In the past six months, what proportion of your injections did you do at any supervised injection site or overdose prevention site?” Participants could respond with “all” (100% of their injections), “most” (75-99% of their injections), “some” (26-74% of their injections), “few” (1-25% of their injections), or “none” (0%). The “all” and “most” options were combined into one category to reflect participants who performed 75% or more of their injections at a supervised consumption site in the last 6 months. This item served as the main predictor variable in the study (i.e., baseline frequency of use of supervised consumptions services).
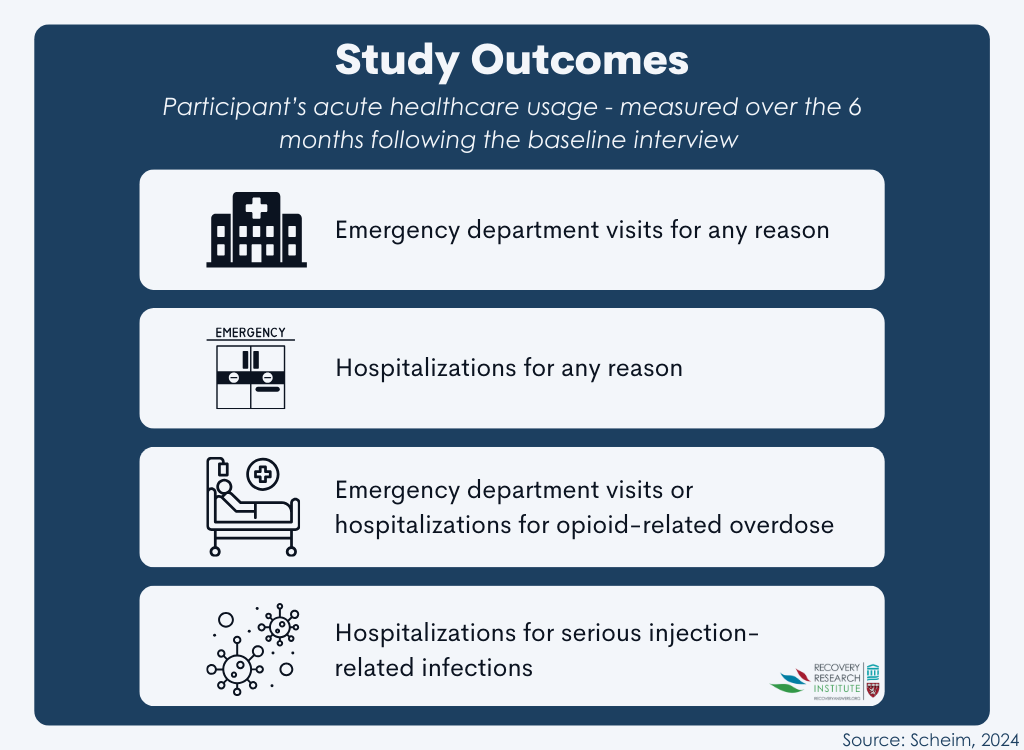
The main outcomes of interest were participants’ acute healthcare usage, which were obtained from the linked administrative data. These outcomes were measured over the 6 months following the baseline interview and included: emergency department visits for any reason; hospitalizations for any reason; emergency department visits or hospitalizations for opioid-related overdose; and hospitalizations for serious injection-related infections (see Figure below). The research team was also interested in the following variables that could confound, or bias, the results: age; sex; recent frequency of injection drug use of any kind; recent non-medical opioid injection drug use; recent homelessness; recent incarceration; prior HIV diagnosis; recent emergency department visit; recent hospitalization; recent emergency department visit or hospitalization for opioid-related overdose; and recent hospitalization for injection-related infection. These variables were pulled from both the questionnaire and administrative data.
For the analyses, the research team examined the effects of baseline frequency of use of supervised consumptions services on acute healthcare usage. Weights were applied to the models to reduce the potential effects of the confounding variables. This type of analytic modeling has a similar effect of randomizing participants within an experimental design, since both allow for the adjustment of potential confounds. Accordingly, this makes the current design quasi-experimental and helps the researchers make the case that any observed advantage for supervised consumption site use is due to the site itself and not other factors.
Participants were recruited into the broader Ontario Integrated Supervised Injection Services study by entering themselves, being referred by other participants, and through outreach within communities. They were eligible to participate if they were at least 18 years or older, lived in Toronto, and reported injecting drugs within the last 6 months. Participants were compensated $30 Canadian dollars per questionnaire. For the purposes of the current study, the research team included participants who completed a baseline interview between November 5th, 2018, and March 19th, 2020, consented to having their data linked with administrative databases and were successfully linked, and had data available for baseline frequency of use of supervised consumptions services, outcomes variables, and potentially confounding variables.
WHAT DID THIS STUDY FIND?
Most individuals used supervised consumption sites for at least some of their injections
Among all participants, 85% reported using supervised consumption services in the past 6 months. Overall, 26% used them for more than three-fourths of their injections (most/all), 30% for ¼ – ¾ of their injections (some), 29% for up to ¼ of their injections (few) and 15% did not use these services for their injections (none).
Use of acute healthcare was high, and frequency of use of supervised consumption services had little impact
Over the 6 months after baseline, 292 unique participants made 1302 emergency department visits; 83 unique participants were hospitalized 132 times; 71 unique participants visited the emergency department or were hospitalized 125 times for opioid-related overdoses; and 34 unique participants were hospitalized 46 times for serious injection-related infections.
After applying weights to adjust for imbalances between groups at baseline, frequency of use of supervised consumption services at baseline was not associated with emergency department visits, hospitalizations, and hospitalizations for injection-related infections over the following 6 months (see Figure below). Using a different approach to measuring supervised consumption site use – consistent (26% or more injections) vs. inconsistent (25% or fewer injections, including none) – led to the same results.
Though participants who reported “some” recent use of supervised consumption services for their injections at baseline had a 2.3 times higher rate of emergency department visits or hospitalizations for opioid-related overdose in the following 6 months compared to participants who reported using them for “few” of their injections, this was not the case in comparison to those who did not use the sites at all (their outcomes were similar).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team investigated whether using supervised consumption services reduced the use of acute care among people who inject drugs over 6 months. Results showed that there were high rates of emergency department visits, with over half of participants visiting the emergency department at least 2 times each. Further, frequency of use of supervised consumption services had little impact on acute healthcare usage. The only test that showed an association was that participants who used supervised consumption services for “some” of their injections had a rate of emergency department visits or hospitalizations for opioid-related overdose 2 times higher than those who reported using them for “few” of their injections. Given this modest effect size, and that this group had similar outcomes to the group with no site participation, this finding may be due to the probability of a chance difference when there is a high number of statistical tests conducted. Overall, supervised consumption site participation did not reduce healthcare utilization, but it is unlikely to have made it worse.
The high rates of emergency department visits observed in this study are higher than rates observed in a study that compiled results of 92 studies conducted between 2000 and 2018 and showed a rate of 29% among people who use drugs globally. This difference likely reflects greater health risks associated with injection drug use, as compared to drug use broadly, such as higher overdose risks and skin injections from the injection sites. It may also reflect the fact that people who inject drugs often are less likely to have or seek access to primary and preventive care.
Overall, the frequency of use of supervised consumption services was not associated with the frequency of acute healthcare usage. These findings from a study conducted in Canada, which has universal health care, differed from a study of participants in an unsanctioned supervised consumption site in the US, where those who used the service were 27% less likely to have an emergency room visit. Though the current study was more rigorous analytically, it is also possible that patterns of healthcare utilization in the US (e.g., high use of acute services) makes it easier to detect any effect of supervised consumption site participation. It is important to note, as might be expected, a neighborhood’s proximity to a supervised consumption site is associated with greater reductions in overdose rates in that area, as they are able to use it more frequently and access it more easily. While these harm reduction services may very well improve outcomes among those who use it, it is unclear whether individuals with active injection (or other) drug use, many of whom face psychosocial challenges, can use them daily or multiple times per day. How readily individuals who need supervised consumption sites can access them will affect their overall public health impact and cost-effectiveness.
While it is reasonable to expect that supervised consumption services may indirectly reduce acute healthcare usage by filling structural voids in care, these sites are not designed or funded to provide certain health services (e.g., antibiotics that may be needed to treat infections). It is possible that reductions in healthcare visits for some were offset by increases in healthcare visits for others. Increased healthcare utilization may be a good outcome for some – e.g., those with medical issues requiring hospitalization identified by the supervised consumption site staff. Opportunities remain to address these barriers and better care for people who use drugs.
The study was conducted in Toronto, Canada, where supervised consumption services are common in the downtown area and Canada has universal healthcare for all. Results may therefore not generalize to other Canadian provinces or other countries, where such services are less common and accessible.
The follow-up period was limited to 6 months. It is unclear whether longer timeframes would have produced different results.
Part of the study’s follow-up period overlapped with the beginning of the COVID-19 pandemic. Thus, use of supervised consumption services and acute healthcare may have been influenced by pandemic-related restrictions, though it is unclear in which direction the pandemic may have affected these study outcomes.
Analyses did not include chronic illnesses apart from HIV which are likely to be related to healthcare utilization. If the groups with more injections had more chronic illness, that would inflate their healthcare utilization and make it harder to detect an advantage over groups with fewer injections – though this cannot be determined from the study data.
BOTTOM LINE
Contrary to predictions, supervised consumption site participation was not associated with the frequency of acute healthcare usage. However, high rates of visits to the emergency department among people who inject drugs were observed. It is possible that some reduced their reliance on health care while others increased their use of health care – for example, if supervised consumption site staff detected a medical issue that required hospitalization, ostensibly a good outcome. Especially given other research where participation in an unsanctioned US supervised consumption site was associated with reduced emergency room visits, continued, rigorous, quasi-experimental studies like these are needed to inform public health recommendations.
For individuals and families seeking recovery: This study did not find that supervised consumption site participation reduced acute healthcare usage – it did not decrease or increase it. However, high rates of visits to the emergency department were observed among the study participants, who are people who inject drugs. This finding, in combination with prior research, suggests that people who inject drugs who seek healthcare or treatment before there is an emergency may avoid visits to the emergency department.
For treatment professionals and treatment systems: While this study did not find use of supervised consumption sites reduced acute healthcare usage among people who inject drugs, it did show that there were high rates of visits to the emergency department. This likely reflects a gap in healthcare for people who use drugs stemming from salient, ongoing health risks related to injection drug use and barriers to care that are not directly or fully addressed by these harm reduction services. Accordingly, treatment systems that aim to address these barriers by, for instance, outreach services to meet people where they are, expanding hours of operation, and learning about the unique needs of this population, may help to decrease visits to the emergency department.
For scientists: The current study was conducted in Toronto, Canada, so future research that examines the relationship between supervised consumption services and acute healthcare usage in other locations would shed light on the extent to which the results generalize to other Canadian provinces and to areas of other countries like the US considering supervised consumption site implementation. Additionally, future research that examines the impact of supervised consumption services on acute healthcare usage, and other important health and recovery outcomes (e.g., opioid use, recovery capital, treatment participation, etc.) beyond 6 months would help us understand whether any relationship might be observed in the longer term. Likewise, replicating the study during a time when COVID-19 pandemic-related restrictions are not in place would highlight the extent to which the (lack of) results were a result of the pandemic.
For policy makers: This study did not find any association between the degree of use of supervised consumption sites and reduced acute healthcare usage – it did not decrease or increase it. However, it did show that there were high rates of visits to the emergency department among this population, which may reflect a gap in healthcare for people who use drugs stemming from their increased health risks alongside barriers to care that are not directly or fully addressed by supervised consumption services.
Supervised consumption sites, also called overdose prevention sites or safe injection sites, may reduce the use of acute healthcare among people who inject drugs, since these sites can help link people to primary care. These sites also typically offer a number of other services such as provision of sterile drug use equipment, guidance about safer drug use, drug checking, distribution of naloxone, education about and testing for infectious disease, and linkage to addiction treatment and other social services that could potentially alleviate drug use harms and risk for emergency room visits. A recent systematic review of research suggests that supervised consumption sites may be associated with public health benefits.
However, there is some research that suggests that use of supervised consumption sites is associated instead with an increase in use of acute healthcare services, via nurses at the sites who refer people to the hospital after detecting a medical problem, which arguably would be seen as a positive outcome in helping to prevent more serious of life-threatening health harms. However, given the unclear nature of the association and potential benefit of supervised consumption sites reducing the use of acute healthcare, this quasi-experimental study examined the impact of supervised consumption services on the frequency of use of acute healthcare. Such research can help clarify the role that supervised consumption sites have in overall healthcare utilization among people who use drugs, which can highlight how to best provide care for this population and alleviate the demands placed on acute healthcare systems.
HOW WAS THIS STUDY CONDUCTED?
This quasi-experimental study used questionnaire and administrative data to investigate whether different levels of supervised consumption service use (vs. no use) reduced the acute care visits among people who inject drugs in Toronto, Canada, over 6 months, controlling simultaneously for a set of factors associated with the propensity to participate in the sites. A total of 467 participants were included in the current study. Of these, 66% identified as cisgender men and were, on average, 41 years old at baseline. The majority of participants reported injecting drugs daily (56%) and injecting opioids (85%).
The questionnaires assessed the frequency of participants’ use of supervised consumption services and the administrative data provided information about their use of acute care.
Questionnaires were administered as part of the ongoing Ontario Integrated Supervised Injection Services – Toronto study, which evaluated the impact of the first 3 supervised consumption sites that opened in Toronto on clients’ use of healthcare and health outcomes. While the specific services offered typically vary by site, all 3 sites in the study permitted injection use and 2 also allowed oral and intranasal use. People who were recruited for the questionnaire were also asked their permission to have their questionnaire data linked with administrative databases that provided information about their demographics, health (e.g., vitals, HIV status), and health care usage (e.g., emergency department visits, hospitalizations). As the study notes, participants from the supervised consumption site who were linked to records were similar to the overall group at the site on age, gender, injection frequency, and other psychosocial contexts such as recent incarceration. The questionnaire was administered by an interviewer and was completed at baseline and approximately every 6 months following.
As part of the baseline questionnaire, participants were asked, “In the past six months, what proportion of your injections did you do at any supervised injection site or overdose prevention site?” Participants could respond with “all” (100% of their injections), “most” (75-99% of their injections), “some” (26-74% of their injections), “few” (1-25% of their injections), or “none” (0%). The “all” and “most” options were combined into one category to reflect participants who performed 75% or more of their injections at a supervised consumption site in the last 6 months. This item served as the main predictor variable in the study (i.e., baseline frequency of use of supervised consumptions services).
The main outcomes of interest were participants’ acute healthcare usage, which were obtained from the linked administrative data. These outcomes were measured over the 6 months following the baseline interview and included: emergency department visits for any reason; hospitalizations for any reason; emergency department visits or hospitalizations for opioid-related overdose; and hospitalizations for serious injection-related infections (see Figure below). The research team was also interested in the following variables that could confound, or bias, the results: age; sex; recent frequency of injection drug use of any kind; recent non-medical opioid injection drug use; recent homelessness; recent incarceration; prior HIV diagnosis; recent emergency department visit; recent hospitalization; recent emergency department visit or hospitalization for opioid-related overdose; and recent hospitalization for injection-related infection. These variables were pulled from both the questionnaire and administrative data.
For the analyses, the research team examined the effects of baseline frequency of use of supervised consumptions services on acute healthcare usage. Weights were applied to the models to reduce the potential effects of the confounding variables. This type of analytic modeling has a similar effect of randomizing participants within an experimental design, since both allow for the adjustment of potential confounds. Accordingly, this makes the current design quasi-experimental and helps the researchers make the case that any observed advantage for supervised consumption site use is due to the site itself and not other factors.
Participants were recruited into the broader Ontario Integrated Supervised Injection Services study by entering themselves, being referred by other participants, and through outreach within communities. They were eligible to participate if they were at least 18 years or older, lived in Toronto, and reported injecting drugs within the last 6 months. Participants were compensated $30 Canadian dollars per questionnaire. For the purposes of the current study, the research team included participants who completed a baseline interview between November 5th, 2018, and March 19th, 2020, consented to having their data linked with administrative databases and were successfully linked, and had data available for baseline frequency of use of supervised consumptions services, outcomes variables, and potentially confounding variables.
WHAT DID THIS STUDY FIND?
Most individuals used supervised consumption sites for at least some of their injections
Among all participants, 85% reported using supervised consumption services in the past 6 months. Overall, 26% used them for more than three-fourths of their injections (most/all), 30% for ¼ – ¾ of their injections (some), 29% for up to ¼ of their injections (few) and 15% did not use these services for their injections (none).
Use of acute healthcare was high, and frequency of use of supervised consumption services had little impact
Over the 6 months after baseline, 292 unique participants made 1302 emergency department visits; 83 unique participants were hospitalized 132 times; 71 unique participants visited the emergency department or were hospitalized 125 times for opioid-related overdoses; and 34 unique participants were hospitalized 46 times for serious injection-related infections.
After applying weights to adjust for imbalances between groups at baseline, frequency of use of supervised consumption services at baseline was not associated with emergency department visits, hospitalizations, and hospitalizations for injection-related infections over the following 6 months (see Figure below). Using a different approach to measuring supervised consumption site use – consistent (26% or more injections) vs. inconsistent (25% or fewer injections, including none) – led to the same results.
Though participants who reported “some” recent use of supervised consumption services for their injections at baseline had a 2.3 times higher rate of emergency department visits or hospitalizations for opioid-related overdose in the following 6 months compared to participants who reported using them for “few” of their injections, this was not the case in comparison to those who did not use the sites at all (their outcomes were similar).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team investigated whether using supervised consumption services reduced the use of acute care among people who inject drugs over 6 months. Results showed that there were high rates of emergency department visits, with over half of participants visiting the emergency department at least 2 times each. Further, frequency of use of supervised consumption services had little impact on acute healthcare usage. The only test that showed an association was that participants who used supervised consumption services for “some” of their injections had a rate of emergency department visits or hospitalizations for opioid-related overdose 2 times higher than those who reported using them for “few” of their injections. Given this modest effect size, and that this group had similar outcomes to the group with no site participation, this finding may be due to the probability of a chance difference when there is a high number of statistical tests conducted. Overall, supervised consumption site participation did not reduce healthcare utilization, but it is unlikely to have made it worse.
The high rates of emergency department visits observed in this study are higher than rates observed in a study that compiled results of 92 studies conducted between 2000 and 2018 and showed a rate of 29% among people who use drugs globally. This difference likely reflects greater health risks associated with injection drug use, as compared to drug use broadly, such as higher overdose risks and skin injections from the injection sites. It may also reflect the fact that people who inject drugs often are less likely to have or seek access to primary and preventive care.
Overall, the frequency of use of supervised consumption services was not associated with the frequency of acute healthcare usage. These findings from a study conducted in Canada, which has universal health care, differed from a study of participants in an unsanctioned supervised consumption site in the US, where those who used the service were 27% less likely to have an emergency room visit. Though the current study was more rigorous analytically, it is also possible that patterns of healthcare utilization in the US (e.g., high use of acute services) makes it easier to detect any effect of supervised consumption site participation. It is important to note, as might be expected, a neighborhood’s proximity to a supervised consumption site is associated with greater reductions in overdose rates in that area, as they are able to use it more frequently and access it more easily. While these harm reduction services may very well improve outcomes among those who use it, it is unclear whether individuals with active injection (or other) drug use, many of whom face psychosocial challenges, can use them daily or multiple times per day. How readily individuals who need supervised consumption sites can access them will affect their overall public health impact and cost-effectiveness.
While it is reasonable to expect that supervised consumption services may indirectly reduce acute healthcare usage by filling structural voids in care, these sites are not designed or funded to provide certain health services (e.g., antibiotics that may be needed to treat infections). It is possible that reductions in healthcare visits for some were offset by increases in healthcare visits for others. Increased healthcare utilization may be a good outcome for some – e.g., those with medical issues requiring hospitalization identified by the supervised consumption site staff. Opportunities remain to address these barriers and better care for people who use drugs.
The study was conducted in Toronto, Canada, where supervised consumption services are common in the downtown area and Canada has universal healthcare for all. Results may therefore not generalize to other Canadian provinces or other countries, where such services are less common and accessible.
The follow-up period was limited to 6 months. It is unclear whether longer timeframes would have produced different results.
Part of the study’s follow-up period overlapped with the beginning of the COVID-19 pandemic. Thus, use of supervised consumption services and acute healthcare may have been influenced by pandemic-related restrictions, though it is unclear in which direction the pandemic may have affected these study outcomes.
Analyses did not include chronic illnesses apart from HIV which are likely to be related to healthcare utilization. If the groups with more injections had more chronic illness, that would inflate their healthcare utilization and make it harder to detect an advantage over groups with fewer injections – though this cannot be determined from the study data.
BOTTOM LINE
Contrary to predictions, supervised consumption site participation was not associated with the frequency of acute healthcare usage. However, high rates of visits to the emergency department among people who inject drugs were observed. It is possible that some reduced their reliance on health care while others increased their use of health care – for example, if supervised consumption site staff detected a medical issue that required hospitalization, ostensibly a good outcome. Especially given other research where participation in an unsanctioned US supervised consumption site was associated with reduced emergency room visits, continued, rigorous, quasi-experimental studies like these are needed to inform public health recommendations.
For individuals and families seeking recovery: This study did not find that supervised consumption site participation reduced acute healthcare usage – it did not decrease or increase it. However, high rates of visits to the emergency department were observed among the study participants, who are people who inject drugs. This finding, in combination with prior research, suggests that people who inject drugs who seek healthcare or treatment before there is an emergency may avoid visits to the emergency department.
For treatment professionals and treatment systems: While this study did not find use of supervised consumption sites reduced acute healthcare usage among people who inject drugs, it did show that there were high rates of visits to the emergency department. This likely reflects a gap in healthcare for people who use drugs stemming from salient, ongoing health risks related to injection drug use and barriers to care that are not directly or fully addressed by these harm reduction services. Accordingly, treatment systems that aim to address these barriers by, for instance, outreach services to meet people where they are, expanding hours of operation, and learning about the unique needs of this population, may help to decrease visits to the emergency department.
For scientists: The current study was conducted in Toronto, Canada, so future research that examines the relationship between supervised consumption services and acute healthcare usage in other locations would shed light on the extent to which the results generalize to other Canadian provinces and to areas of other countries like the US considering supervised consumption site implementation. Additionally, future research that examines the impact of supervised consumption services on acute healthcare usage, and other important health and recovery outcomes (e.g., opioid use, recovery capital, treatment participation, etc.) beyond 6 months would help us understand whether any relationship might be observed in the longer term. Likewise, replicating the study during a time when COVID-19 pandemic-related restrictions are not in place would highlight the extent to which the (lack of) results were a result of the pandemic.
For policy makers: This study did not find any association between the degree of use of supervised consumption sites and reduced acute healthcare usage – it did not decrease or increase it. However, it did show that there were high rates of visits to the emergency department among this population, which may reflect a gap in healthcare for people who use drugs stemming from their increased health risks alongside barriers to care that are not directly or fully addressed by supervised consumption services.
Supervised consumption sites, also called overdose prevention sites or safe injection sites, may reduce the use of acute healthcare among people who inject drugs, since these sites can help link people to primary care. These sites also typically offer a number of other services such as provision of sterile drug use equipment, guidance about safer drug use, drug checking, distribution of naloxone, education about and testing for infectious disease, and linkage to addiction treatment and other social services that could potentially alleviate drug use harms and risk for emergency room visits. A recent systematic review of research suggests that supervised consumption sites may be associated with public health benefits.
However, there is some research that suggests that use of supervised consumption sites is associated instead with an increase in use of acute healthcare services, via nurses at the sites who refer people to the hospital after detecting a medical problem, which arguably would be seen as a positive outcome in helping to prevent more serious of life-threatening health harms. However, given the unclear nature of the association and potential benefit of supervised consumption sites reducing the use of acute healthcare, this quasi-experimental study examined the impact of supervised consumption services on the frequency of use of acute healthcare. Such research can help clarify the role that supervised consumption sites have in overall healthcare utilization among people who use drugs, which can highlight how to best provide care for this population and alleviate the demands placed on acute healthcare systems.
HOW WAS THIS STUDY CONDUCTED?
This quasi-experimental study used questionnaire and administrative data to investigate whether different levels of supervised consumption service use (vs. no use) reduced the acute care visits among people who inject drugs in Toronto, Canada, over 6 months, controlling simultaneously for a set of factors associated with the propensity to participate in the sites. A total of 467 participants were included in the current study. Of these, 66% identified as cisgender men and were, on average, 41 years old at baseline. The majority of participants reported injecting drugs daily (56%) and injecting opioids (85%).
The questionnaires assessed the frequency of participants’ use of supervised consumption services and the administrative data provided information about their use of acute care.
Questionnaires were administered as part of the ongoing Ontario Integrated Supervised Injection Services – Toronto study, which evaluated the impact of the first 3 supervised consumption sites that opened in Toronto on clients’ use of healthcare and health outcomes. While the specific services offered typically vary by site, all 3 sites in the study permitted injection use and 2 also allowed oral and intranasal use. People who were recruited for the questionnaire were also asked their permission to have their questionnaire data linked with administrative databases that provided information about their demographics, health (e.g., vitals, HIV status), and health care usage (e.g., emergency department visits, hospitalizations). As the study notes, participants from the supervised consumption site who were linked to records were similar to the overall group at the site on age, gender, injection frequency, and other psychosocial contexts such as recent incarceration. The questionnaire was administered by an interviewer and was completed at baseline and approximately every 6 months following.
As part of the baseline questionnaire, participants were asked, “In the past six months, what proportion of your injections did you do at any supervised injection site or overdose prevention site?” Participants could respond with “all” (100% of their injections), “most” (75-99% of their injections), “some” (26-74% of their injections), “few” (1-25% of their injections), or “none” (0%). The “all” and “most” options were combined into one category to reflect participants who performed 75% or more of their injections at a supervised consumption site in the last 6 months. This item served as the main predictor variable in the study (i.e., baseline frequency of use of supervised consumptions services).
The main outcomes of interest were participants’ acute healthcare usage, which were obtained from the linked administrative data. These outcomes were measured over the 6 months following the baseline interview and included: emergency department visits for any reason; hospitalizations for any reason; emergency department visits or hospitalizations for opioid-related overdose; and hospitalizations for serious injection-related infections (see Figure below). The research team was also interested in the following variables that could confound, or bias, the results: age; sex; recent frequency of injection drug use of any kind; recent non-medical opioid injection drug use; recent homelessness; recent incarceration; prior HIV diagnosis; recent emergency department visit; recent hospitalization; recent emergency department visit or hospitalization for opioid-related overdose; and recent hospitalization for injection-related infection. These variables were pulled from both the questionnaire and administrative data.
For the analyses, the research team examined the effects of baseline frequency of use of supervised consumptions services on acute healthcare usage. Weights were applied to the models to reduce the potential effects of the confounding variables. This type of analytic modeling has a similar effect of randomizing participants within an experimental design, since both allow for the adjustment of potential confounds. Accordingly, this makes the current design quasi-experimental and helps the researchers make the case that any observed advantage for supervised consumption site use is due to the site itself and not other factors.
Participants were recruited into the broader Ontario Integrated Supervised Injection Services study by entering themselves, being referred by other participants, and through outreach within communities. They were eligible to participate if they were at least 18 years or older, lived in Toronto, and reported injecting drugs within the last 6 months. Participants were compensated $30 Canadian dollars per questionnaire. For the purposes of the current study, the research team included participants who completed a baseline interview between November 5th, 2018, and March 19th, 2020, consented to having their data linked with administrative databases and were successfully linked, and had data available for baseline frequency of use of supervised consumptions services, outcomes variables, and potentially confounding variables.
WHAT DID THIS STUDY FIND?
Most individuals used supervised consumption sites for at least some of their injections
Among all participants, 85% reported using supervised consumption services in the past 6 months. Overall, 26% used them for more than three-fourths of their injections (most/all), 30% for ¼ – ¾ of their injections (some), 29% for up to ¼ of their injections (few) and 15% did not use these services for their injections (none).
Use of acute healthcare was high, and frequency of use of supervised consumption services had little impact
Over the 6 months after baseline, 292 unique participants made 1302 emergency department visits; 83 unique participants were hospitalized 132 times; 71 unique participants visited the emergency department or were hospitalized 125 times for opioid-related overdoses; and 34 unique participants were hospitalized 46 times for serious injection-related infections.
After applying weights to adjust for imbalances between groups at baseline, frequency of use of supervised consumption services at baseline was not associated with emergency department visits, hospitalizations, and hospitalizations for injection-related infections over the following 6 months (see Figure below). Using a different approach to measuring supervised consumption site use – consistent (26% or more injections) vs. inconsistent (25% or fewer injections, including none) – led to the same results.
Though participants who reported “some” recent use of supervised consumption services for their injections at baseline had a 2.3 times higher rate of emergency department visits or hospitalizations for opioid-related overdose in the following 6 months compared to participants who reported using them for “few” of their injections, this was not the case in comparison to those who did not use the sites at all (their outcomes were similar).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The research team investigated whether using supervised consumption services reduced the use of acute care among people who inject drugs over 6 months. Results showed that there were high rates of emergency department visits, with over half of participants visiting the emergency department at least 2 times each. Further, frequency of use of supervised consumption services had little impact on acute healthcare usage. The only test that showed an association was that participants who used supervised consumption services for “some” of their injections had a rate of emergency department visits or hospitalizations for opioid-related overdose 2 times higher than those who reported using them for “few” of their injections. Given this modest effect size, and that this group had similar outcomes to the group with no site participation, this finding may be due to the probability of a chance difference when there is a high number of statistical tests conducted. Overall, supervised consumption site participation did not reduce healthcare utilization, but it is unlikely to have made it worse.
The high rates of emergency department visits observed in this study are higher than rates observed in a study that compiled results of 92 studies conducted between 2000 and 2018 and showed a rate of 29% among people who use drugs globally. This difference likely reflects greater health risks associated with injection drug use, as compared to drug use broadly, such as higher overdose risks and skin injections from the injection sites. It may also reflect the fact that people who inject drugs often are less likely to have or seek access to primary and preventive care.
Overall, the frequency of use of supervised consumption services was not associated with the frequency of acute healthcare usage. These findings from a study conducted in Canada, which has universal health care, differed from a study of participants in an unsanctioned supervised consumption site in the US, where those who used the service were 27% less likely to have an emergency room visit. Though the current study was more rigorous analytically, it is also possible that patterns of healthcare utilization in the US (e.g., high use of acute services) makes it easier to detect any effect of supervised consumption site participation. It is important to note, as might be expected, a neighborhood’s proximity to a supervised consumption site is associated with greater reductions in overdose rates in that area, as they are able to use it more frequently and access it more easily. While these harm reduction services may very well improve outcomes among those who use it, it is unclear whether individuals with active injection (or other) drug use, many of whom face psychosocial challenges, can use them daily or multiple times per day. How readily individuals who need supervised consumption sites can access them will affect their overall public health impact and cost-effectiveness.
While it is reasonable to expect that supervised consumption services may indirectly reduce acute healthcare usage by filling structural voids in care, these sites are not designed or funded to provide certain health services (e.g., antibiotics that may be needed to treat infections). It is possible that reductions in healthcare visits for some were offset by increases in healthcare visits for others. Increased healthcare utilization may be a good outcome for some – e.g., those with medical issues requiring hospitalization identified by the supervised consumption site staff. Opportunities remain to address these barriers and better care for people who use drugs.
The study was conducted in Toronto, Canada, where supervised consumption services are common in the downtown area and Canada has universal healthcare for all. Results may therefore not generalize to other Canadian provinces or other countries, where such services are less common and accessible.
The follow-up period was limited to 6 months. It is unclear whether longer timeframes would have produced different results.
Part of the study’s follow-up period overlapped with the beginning of the COVID-19 pandemic. Thus, use of supervised consumption services and acute healthcare may have been influenced by pandemic-related restrictions, though it is unclear in which direction the pandemic may have affected these study outcomes.
Analyses did not include chronic illnesses apart from HIV which are likely to be related to healthcare utilization. If the groups with more injections had more chronic illness, that would inflate their healthcare utilization and make it harder to detect an advantage over groups with fewer injections – though this cannot be determined from the study data.
BOTTOM LINE
Contrary to predictions, supervised consumption site participation was not associated with the frequency of acute healthcare usage. However, high rates of visits to the emergency department among people who inject drugs were observed. It is possible that some reduced their reliance on health care while others increased their use of health care – for example, if supervised consumption site staff detected a medical issue that required hospitalization, ostensibly a good outcome. Especially given other research where participation in an unsanctioned US supervised consumption site was associated with reduced emergency room visits, continued, rigorous, quasi-experimental studies like these are needed to inform public health recommendations.
For individuals and families seeking recovery: This study did not find that supervised consumption site participation reduced acute healthcare usage – it did not decrease or increase it. However, high rates of visits to the emergency department were observed among the study participants, who are people who inject drugs. This finding, in combination with prior research, suggests that people who inject drugs who seek healthcare or treatment before there is an emergency may avoid visits to the emergency department.
For treatment professionals and treatment systems: While this study did not find use of supervised consumption sites reduced acute healthcare usage among people who inject drugs, it did show that there were high rates of visits to the emergency department. This likely reflects a gap in healthcare for people who use drugs stemming from salient, ongoing health risks related to injection drug use and barriers to care that are not directly or fully addressed by these harm reduction services. Accordingly, treatment systems that aim to address these barriers by, for instance, outreach services to meet people where they are, expanding hours of operation, and learning about the unique needs of this population, may help to decrease visits to the emergency department.
For scientists: The current study was conducted in Toronto, Canada, so future research that examines the relationship between supervised consumption services and acute healthcare usage in other locations would shed light on the extent to which the results generalize to other Canadian provinces and to areas of other countries like the US considering supervised consumption site implementation. Additionally, future research that examines the impact of supervised consumption services on acute healthcare usage, and other important health and recovery outcomes (e.g., opioid use, recovery capital, treatment participation, etc.) beyond 6 months would help us understand whether any relationship might be observed in the longer term. Likewise, replicating the study during a time when COVID-19 pandemic-related restrictions are not in place would highlight the extent to which the (lack of) results were a result of the pandemic.
For policy makers: This study did not find any association between the degree of use of supervised consumption sites and reduced acute healthcare usage – it did not decrease or increase it. However, it did show that there were high rates of visits to the emergency department among this population, which may reflect a gap in healthcare for people who use drugs stemming from their increased health risks alongside barriers to care that are not directly or fully addressed by supervised consumption services.