An innovative method to track stigmatizing language in addiction treatment clinical notes
The language used to describe people with substance usedisorder influences our attitudes, and could impact clinical decision making in healthcare settings. Thisstudy used an innovative approach to identify stigmatizing language in clinicalprovider notes and patient factors associated with the use of such language.
There are many studies showing that negative attitudes of healthcare providers towards people with substance use disorders are common and contribute to suboptimal health outcomes for these individuals. For example, in a large systematic review, healthcare providers often attributed blame to the patients themselves as barriers to treatment engagement, citing reasons such as perceived violence, manipulation, and lack of motivation. Healthcare providers also demonstrated inadequate knowledge, training, and support to treat individuals with substance use disorder. These negative attitudes and lack of adequate training among providers coincide with disempowerment of patients and result in substandard healthcare, including diminished collaboration between patients and providers.
Stigma can be experienced and communicated in various forms, including in the language that medical personnel use when referring to individuals with substance use disorder. Just small differences, such as referring to an individual as “a substance abuser” versus “having a substance use disorder,” can lead to differential judgments – in both clinical experts and the general public – about whether the individual with substance use disorder is to blame for their condition and their likelihood of recovery.
Stigmatizing language in general is pervasive in medical records, which may impact patients as well as healthcare team members. It applies not only to individuals with substance use disorder but also to other conditions including chronic pain and diabetes. In a large study of individuals (not just those with substance use disorder) who read at least one of their outpatient medical notes, more than 10% reported feeling judged and/or offended.
One key aim of the US Department of Health and Human Services’ harm reduction pillar is to “develop educational materials and programs to reduce stigma.” Training for providers that addresses this stigma has increased in recent years, although some research suggests that negative attitudes toward people who use drugs are still pervasive among healthcare providers. One recent study, for example, showed that 75% of primary care physicians surveyed reported high levels of stigma towards individuals with opioid use disorder, on par with stigma toward these individuals in the general population. It can be difficult to monitor and measure stigma in large healthcare systems – examining clinical notes is one innovative, unobtrusive way to do this. In turn, these data can inform content for stigma reduction interventions among healthcare providers.
In this study, the researchers examined the incidence of stigmatizing language in clinical notes of a large healthcare system specific to patients with substance-related diagnoses and reported on any disparities associated with demographic characteristics of patients (e.g., race/ethnicity, gender).
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional, observational, retrospective study from December 1, 2020 to November 30, 2021 of hospital notes contained in the electronic health record (EHR) of Mass General Brigham, a large healthcare system in Massachusetts and New Hampshire. The study identified 546,309 clinical notes for review for the use of stigmatizing language in the body of the note from 30,391 patients with at least one substance-related diagnosis code. The incidence of stigmatizing language in medical notes (i.e., how common it was for stigmatizing language to be present in the medical notes) was reported by patient characteristics (e.g., race, ethnicity, socioeconomic status) and provider characteristics (e.g., physicians, physician assistants, nurses, etc.) to identify any disparities (i.e., undue or preventable differences by group).
Hospital notes included for analysis were all free-text notes from patients who had at least one inpatient and/or outpatient visit(s) in the Mass General Brigham health system during the 1-year period between December 1, 2020 and November 30, 2021, and whose encounter diagnosis contained at least one substance-related diagnosis code. The researchers used a list of 24 ICD-10 (International Classification of Diseases, Tenth Revision) codes that capture substance use disorders, as well as codes associated with overdose of drugs and alcohol. Medical notes from a range of providers were included: physicians, physicians, advanced-practice providers, nurses, social workers, and others who interact with patients and document the encounter. Types of notes included: history and physicals, consults, discharge summaries, emergency department (ED) notes, group therapy notes, transfer/sign-off notes, progress notes, ED nurse triage notes, nursing notes, assessment/plan notes, nursing summaries, plan of care, and opioid notes (a special note type created by the healthcare facility, which lists the indication for opioid prescriptions, the primary prescriber, and substance use disorder-related risk factors). Patient-reported demographic data, including age, sex, race, and ethnicity were also recorded for each note.
The researchers developed a natural language processing algorithm using the National Institute on Drug Abuse’s “Words Matter” list to identify use of stigmatizing language in context. The researchers randomly selected 10,000 clinical notes with stigmatizing key words to develop the algorithm and extract information from the notes to determine the semantic meaning based on the context. For example, (1) the use of the word “alcoholic” is discouraged, yet there are uses of the word which are deemed clinically acceptable, such as “alcoholic cirrhosis” or “alcoholic hepatitis.” In these cases, “alcoholic” was deemed stigma only if it was used as a noun, for example, “the patient is an alcoholic” (note that the term was considered stigmatizing when used to describe the 12-step mutual-help organization Alcoholics Anonymous); (2) use of the word “abuse” is discouraged, yet it can be acceptable in some cases. If “abuse” was used in “drug abuse” or “alcohol abuse,” it was categorized as stigma, but if it was “emotional abuse” or “physical abuse,” it was not; and (3) the word “user” is discouraged, yet the word is commonly used in other contexts, such as “her user login name is.” Therefore, the researchers included the word as stigmatizing if it followed a drug name, such as “he is a marijuana user” or “she is a heroin user.” Based on the context of that language in the sentence, the algorithm identified sentences containing a stigmatizing keyword(s) and determined whether the sentence contained stigmatization meaning or not. If a clinical note had at least one stigmatizing sentence, it was regarded as a stigmatizing note.
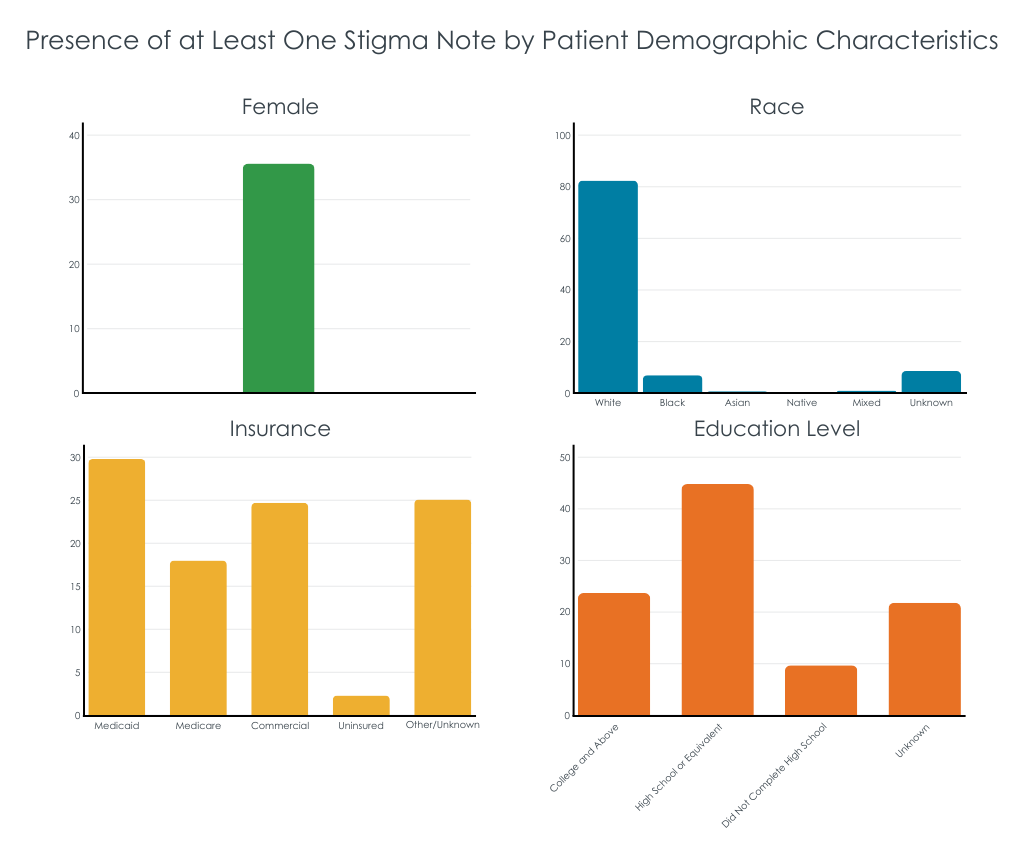
During the 1-year study period, there were 30,391 patients seen in the healthcare system who had both a substance-related encounter (e.g., outpatient treatment) and at least one clinical note recorded. Patients were on average 47.7 years old at the time of the encounter, 38% were female, 81% were White, and 9% reported Hispanic ethnicity. Overall, the algorithm determined that 62% of patients had at least one note containing stigmatizing language. Black patients (65%) and patients with Medicaid insurance (70%) had disproportionately higher percentages of stigmatizing language in their medical notes.
WHAT DID THIS STUDY FIND?
Notes with stigmatizing terms were common
There were 546,309 notes for 30,391 patients, of which 100,792 (18%) contained stigmatizing language. A total of 18,727 patients (62%) had at least one note with stigmatizing language. Hospital encounters (20%) were more likely to contain stigmatizing language than were office visits (14%). About a quarter of physician (26%) and nurse practitioner notes (24%) were stigmatizing, physician assistants had a higher proportion of stigmatizing language (47%), and nurses had a lower rate (4%). The most common note type was “progress note,” for which 15% contained stigmatizing language. History and physical notes were most likely to contain stigmatizing language (59%). In general, nursing notes, including ED triage notes (6%), nursing summaries (2%), and nursing notes (2%), had lower incidences of stigma.
Medicaid patients had disproportionately higher rates of stigmatizing notes
When controlling for the effect of other factors including age, sex, race, ethnicity, marital status, education level, and veteran status, patients with Medicaid or Medicare insurance were 1.5 times more likely to have stigmatizing notes than those with commercial insurance; 70% of Medicaid patients had at least one stigmatizing note, compared to only 57% of commercially-insured patients. Patients with a greater number of encounters were more likely to have stigmatizing notes, with the greatest number experienced by patients with 20 or more encounters who were 6.6 times more likely to have a stigmatizing note, indicating that the more patients interacted with the health system, the greater the odds of having at least one note containing stigmatizing language.
Certain gender, age, and racial/ethnicgroups were more likely to have stigmatizing language in their notes than their counterparts
When controlling for the effect of other demographic and socioeconomic factors, male patients were 17% more likely to have stigmatizing language in their notes than female patients. Younger patients aged 18-24 were 45% less likely to have stigmatizing notes than middle aged (45-54) patients. Hispanic patients were 12% less likely to have stigmatizing notes than non-Hispanic patients, and Asian patients were 55% less likely to have stigmatizing notes than White patients. Black patients had roughly the same amount of stigmatizing notes (65%) as White patients (63%).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
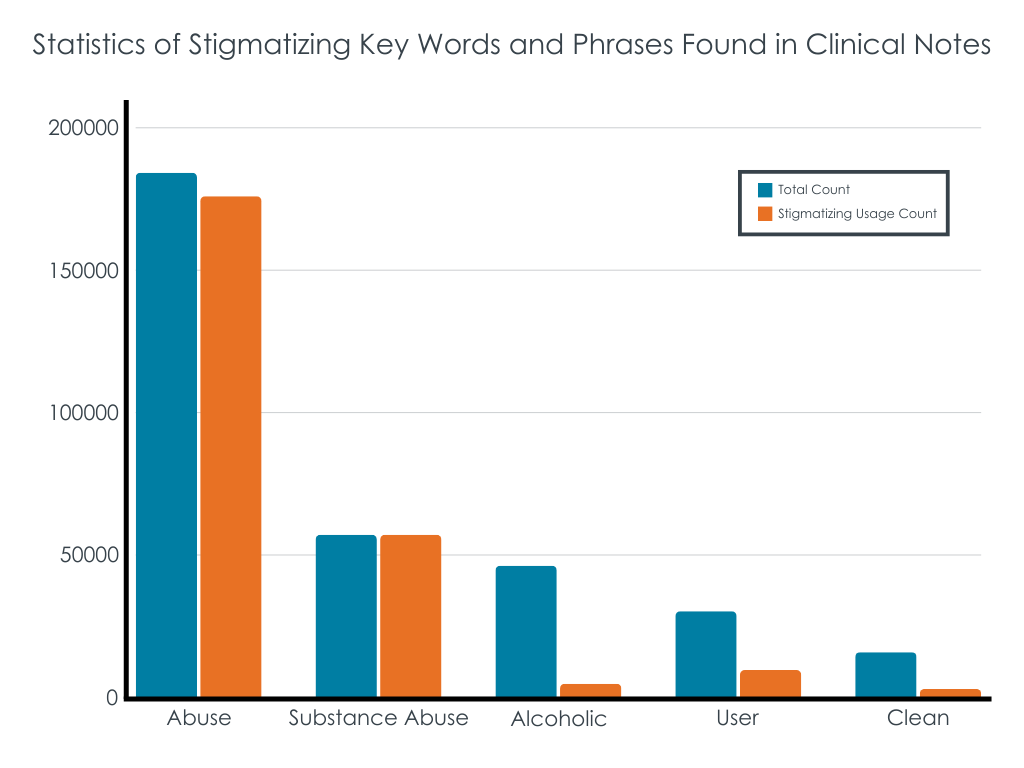
This study showed that a majority of patients with substance-related diagnoses in the Mass General Brigham health system have stigmatizing language in their medical records, most notably “abuse”, “substance abuse”, “alcoholic”, “user”, and “clean”. “Abuse” and “substance abuse” may remain in the medical vernacular given their presence in recent medical diagnostic nomenclature and language norms change gradually over time. For example, some notes seemed to use a premade template that said “substance abuse evaluation” followed by free text from the note author, which were included as stigmatizing language in the current study.
Clinicians may view these terms as acceptable, especially since federal agencies (e.g., the National Institute on Drug Abuse, the National Institute on Alcohol Abuse and Alcoholism, and the Substance Abuse and Mental Health Services Administration) continue to use these terms in their titles and they appear in common screening tools, like the Drug Abuse Screening Test (DAST-10). Additionally, there may have been cases where a patient reported a stigmatizing word that was recorded in the medical record as a quote (e.g., “the patient reports that she is a ‘junkie’” – “junkie” appeared 55 times in medical notes), which would be included as a phrase containing stigma. Unfortunately, the researchers also did not exclude the phrase “alcoholics anonymous,” from the count of stigmatizing language, of which there were 635 instances, despite it being an established name of a known organization and a proper noun. Nonetheless, stigmatizing communications can promote inaccurate and harmful stereotypes about individuals with substance use disorder. At the same time, stigma from healthcare providers is a significant barrier to patients receiving substance use disorder treatment.
Notes commonly used for inpatient hospital and emergency room visits were more likely to contain stigmatizing language compared to office visit notes.
The findings make the case for more in-hospital education about stigma, as providers who do not consistently or commonly work in substance use disorder treatment settings may be less aware to the effect stigmatizing language has on patients with substance-related diagnoses.
Notes written by physician assistants had a much higher incidence of stigmatizing language (47%) than physicians (26%) and nurses (4%). Its not clear what explains this difference, however one possibility is that physician assistants are less likely to have been trained on the new DSM-5 criteria published in 2013 for diagnosing a substance use disorder. The newer diagnostic criteria no longer use the terms “abuse” or “dependence,” whereas the previous DSM (DSM-IV-TR, published in 2000) did. Continuing education for the healthcare system on the new DSM-5 criteria and the importance of language may be helpful to reduce stigma.
Patient-level factors that indicate someone’s socioeconomic status (such as being less educated compared to higher degrees of education, with Medicaid or Medicare insurance compared with commercial, being a veteran, or being single or divorced compared to married) were all associated with increased presence of stigmatizing language. Also, Black patients had the highest proportion of 1 or more notes with stigmatizing language (65%) compared to other racial groups (White, 63%; Asian, 40%; Native American, 56%; mixed race, 54%), however the difference between White and Black patients was not statistically significant when controlling for other socioeconomic and patient factors, meaning that it’s likely an intersection of factors (e.g., someone’s race and their socioeconomic status) explaining stigmatizing language in medical notes. These findings highlight the intersectionality between substance use, stigma, racism, and social determinants of health and should serve as important reminders to clinical staff to assess their biases and be aware of how words used may affect all patients with substance use disorder.
Although this study provided important information about how common stigmatizing language is in medical notes in a large healthcare system in New England, which indicates the need for continuing education and training, the study did not measure healthcare provider behavior or patient experiences. Given that, we do not actually know how stigmatizing language in medical notes actually affected patient care. Future research should examine the association between stigmatizing language in medical notes and the quality of care from the patient’s perspective.
The type of statistical analysis used in this study is very common for examining health disparities in particular groups, however, is limited in that it “partials out” the effect of other factors that could be influencing the presence of stigmatizing language. For example, this type of analysis can tell us if there were differences between White patients and Black patients on stigmatizing notes, and the differences between male and female patients on stigmatizing notes, while controlling for or “partialling out” the effect of the other factor. However, the analysis does not tell us if there were disproportionately higher likelihood of stigma notes for certain intersections of these groups, e.g., Black male patients. In the case of the current findings, this could be important as systemic racism and substance use stigma have down-stream effects on socioeconomic factors and social determinants of health, such as insurance type and education. Thus, it may be that Black men with Medicaid insurance experienced disproportionately higher likelihood of stigma notes than White women with commercial insurance, but the current analysis does not allow for this type of comparison. Future research should consider using intersectional analyses to examine health disparities.
Finally, as the researchers acknowledge, they were unable to ascertain the gender identity of patients (e.g., transgender or gender diverse identities) as this is not currently recorded in their medical notes. This is a major limitation give the tremendous stigma that transgender patients face and could have also influenced the incidence of stigmatizing language in notes.
BOTTOM LINE
Using an innovative machine learning approach this study showed almost two-thirds of patients with substance-related diagnoses (62%) had at least one note containing stigmatizing language. While the model accounted for the context of the term to determine whether it was, in fact, stigmatizing, other contexts were not accounted for including providers quoting the patient’s own words. There were also several patient characteristic disparities associated with patients having stigmatizing language in their notes, including Medicaid or Medicare insurance compared to commercial insurance. The work suggests that more clinician interventions about use of stigmatizing language are needed.
For individuals and families seeking recovery: Often patients with substance use disorder who anticipate or have experienced stigma in healthcare settings develop negative attitudes toward seeking care and earned distrust of the healthcare system. Seeking care from substance use treatment providers with the most up-to-date training in evidence-supported care may reduce the likelihood of stigmatizing interactions. Learn more about indicators of quality addiction treatment here.
For treatment professionals and treatment systems: Language and imagery could influence a person’s willingness to initiate treatment, as well as a patient’s experience in treatment. It’s important for healthcare providers to use non-stigmatizing language in their direct patient care and clinical notes. Check out NIDA’s Words Matter list for language recommendations for healthcare providers.
For scientists:The study used a multivariate regression analysis to identify stigmatizing language disparities by patient characteristics. However, the limitation of this type of analysis is it precludes interpretation of any intersectional effects (e.g., race and insurance type, primary substance). Future research should consider using intersectional analyses to examine health disparities, as disparities for certain groups (e.g., Black male patients with Medicaid) could be washed out using multivariate regression. Additionally, although this study provided important information about how common stigmatizing language is in medical notes in a large healthcare system in New England, which indicates the need for continuing education and training, the study did not measure healthcare provider behavior or patient experiences. Future research should examine the association between stigmatizing language in medical notes and the quality of care from the patient’s perspective.
For policy makers: Continuing education for healthcare providers in all healthcare settings (i.e., not only in substance use treatment settings) could be an important intervention to reduce stigma via reductions in stigmatizing language in medical notes. Language used in medical records is increasingly important as patients have access to some of their medical records through the 21st Century Cures Act. These “open notes” have created controversy for patients with behavioral health conditions, for example when patients find in their medical record inaccurate notes, disrespectful language, or undiscussed diagnoses. Stigmatizing communications can promote inaccurate and harmful stereotypes about individuals with substance use disorder and stigma from healthcare providers is a significant barrier to patients receiving substance use disorder treatment. Policies that support healthcare provider training could reduce substance use stigma and could reduce barriers to treatment for patients with substance use disorder. Check out NIDA’s Words Matter list for language recommendations appropriate for professionals and the images from this study for ideas on non-stigmatizing images.
There are many studies showing that negative attitudes of healthcare providers towards people with substance use disorders are common and contribute to suboptimal health outcomes for these individuals. For example, in a large systematic review, healthcare providers often attributed blame to the patients themselves as barriers to treatment engagement, citing reasons such as perceived violence, manipulation, and lack of motivation. Healthcare providers also demonstrated inadequate knowledge, training, and support to treat individuals with substance use disorder. These negative attitudes and lack of adequate training among providers coincide with disempowerment of patients and result in substandard healthcare, including diminished collaboration between patients and providers.
Stigma can be experienced and communicated in various forms, including in the language that medical personnel use when referring to individuals with substance use disorder. Just small differences, such as referring to an individual as “a substance abuser” versus “having a substance use disorder,” can lead to differential judgments – in both clinical experts and the general public – about whether the individual with substance use disorder is to blame for their condition and their likelihood of recovery.
Stigmatizing language in general is pervasive in medical records, which may impact patients as well as healthcare team members. It applies not only to individuals with substance use disorder but also to other conditions including chronic pain and diabetes. In a large study of individuals (not just those with substance use disorder) who read at least one of their outpatient medical notes, more than 10% reported feeling judged and/or offended.
One key aim of the US Department of Health and Human Services’ harm reduction pillar is to “develop educational materials and programs to reduce stigma.” Training for providers that addresses this stigma has increased in recent years, although some research suggests that negative attitudes toward people who use drugs are still pervasive among healthcare providers. One recent study, for example, showed that 75% of primary care physicians surveyed reported high levels of stigma towards individuals with opioid use disorder, on par with stigma toward these individuals in the general population. It can be difficult to monitor and measure stigma in large healthcare systems – examining clinical notes is one innovative, unobtrusive way to do this. In turn, these data can inform content for stigma reduction interventions among healthcare providers.
In this study, the researchers examined the incidence of stigmatizing language in clinical notes of a large healthcare system specific to patients with substance-related diagnoses and reported on any disparities associated with demographic characteristics of patients (e.g., race/ethnicity, gender).
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional, observational, retrospective study from December 1, 2020 to November 30, 2021 of hospital notes contained in the electronic health record (EHR) of Mass General Brigham, a large healthcare system in Massachusetts and New Hampshire. The study identified 546,309 clinical notes for review for the use of stigmatizing language in the body of the note from 30,391 patients with at least one substance-related diagnosis code. The incidence of stigmatizing language in medical notes (i.e., how common it was for stigmatizing language to be present in the medical notes) was reported by patient characteristics (e.g., race, ethnicity, socioeconomic status) and provider characteristics (e.g., physicians, physician assistants, nurses, etc.) to identify any disparities (i.e., undue or preventable differences by group).
Hospital notes included for analysis were all free-text notes from patients who had at least one inpatient and/or outpatient visit(s) in the Mass General Brigham health system during the 1-year period between December 1, 2020 and November 30, 2021, and whose encounter diagnosis contained at least one substance-related diagnosis code. The researchers used a list of 24 ICD-10 (International Classification of Diseases, Tenth Revision) codes that capture substance use disorders, as well as codes associated with overdose of drugs and alcohol. Medical notes from a range of providers were included: physicians, physicians, advanced-practice providers, nurses, social workers, and others who interact with patients and document the encounter. Types of notes included: history and physicals, consults, discharge summaries, emergency department (ED) notes, group therapy notes, transfer/sign-off notes, progress notes, ED nurse triage notes, nursing notes, assessment/plan notes, nursing summaries, plan of care, and opioid notes (a special note type created by the healthcare facility, which lists the indication for opioid prescriptions, the primary prescriber, and substance use disorder-related risk factors). Patient-reported demographic data, including age, sex, race, and ethnicity were also recorded for each note.
The researchers developed a natural language processing algorithm using the National Institute on Drug Abuse’s “Words Matter” list to identify use of stigmatizing language in context. The researchers randomly selected 10,000 clinical notes with stigmatizing key words to develop the algorithm and extract information from the notes to determine the semantic meaning based on the context. For example, (1) the use of the word “alcoholic” is discouraged, yet there are uses of the word which are deemed clinically acceptable, such as “alcoholic cirrhosis” or “alcoholic hepatitis.” In these cases, “alcoholic” was deemed stigma only if it was used as a noun, for example, “the patient is an alcoholic” (note that the term was considered stigmatizing when used to describe the 12-step mutual-help organization Alcoholics Anonymous); (2) use of the word “abuse” is discouraged, yet it can be acceptable in some cases. If “abuse” was used in “drug abuse” or “alcohol abuse,” it was categorized as stigma, but if it was “emotional abuse” or “physical abuse,” it was not; and (3) the word “user” is discouraged, yet the word is commonly used in other contexts, such as “her user login name is.” Therefore, the researchers included the word as stigmatizing if it followed a drug name, such as “he is a marijuana user” or “she is a heroin user.” Based on the context of that language in the sentence, the algorithm identified sentences containing a stigmatizing keyword(s) and determined whether the sentence contained stigmatization meaning or not. If a clinical note had at least one stigmatizing sentence, it was regarded as a stigmatizing note.
During the 1-year study period, there were 30,391 patients seen in the healthcare system who had both a substance-related encounter (e.g., outpatient treatment) and at least one clinical note recorded. Patients were on average 47.7 years old at the time of the encounter, 38% were female, 81% were White, and 9% reported Hispanic ethnicity. Overall, the algorithm determined that 62% of patients had at least one note containing stigmatizing language. Black patients (65%) and patients with Medicaid insurance (70%) had disproportionately higher percentages of stigmatizing language in their medical notes.
WHAT DID THIS STUDY FIND?
Notes with stigmatizing terms were common
There were 546,309 notes for 30,391 patients, of which 100,792 (18%) contained stigmatizing language. A total of 18,727 patients (62%) had at least one note with stigmatizing language. Hospital encounters (20%) were more likely to contain stigmatizing language than were office visits (14%). About a quarter of physician (26%) and nurse practitioner notes (24%) were stigmatizing, physician assistants had a higher proportion of stigmatizing language (47%), and nurses had a lower rate (4%). The most common note type was “progress note,” for which 15% contained stigmatizing language. History and physical notes were most likely to contain stigmatizing language (59%). In general, nursing notes, including ED triage notes (6%), nursing summaries (2%), and nursing notes (2%), had lower incidences of stigma.
Medicaid patients had disproportionately higher rates of stigmatizing notes
When controlling for the effect of other factors including age, sex, race, ethnicity, marital status, education level, and veteran status, patients with Medicaid or Medicare insurance were 1.5 times more likely to have stigmatizing notes than those with commercial insurance; 70% of Medicaid patients had at least one stigmatizing note, compared to only 57% of commercially-insured patients. Patients with a greater number of encounters were more likely to have stigmatizing notes, with the greatest number experienced by patients with 20 or more encounters who were 6.6 times more likely to have a stigmatizing note, indicating that the more patients interacted with the health system, the greater the odds of having at least one note containing stigmatizing language.
Certain gender, age, and racial/ethnicgroups were more likely to have stigmatizing language in their notes than their counterparts
When controlling for the effect of other demographic and socioeconomic factors, male patients were 17% more likely to have stigmatizing language in their notes than female patients. Younger patients aged 18-24 were 45% less likely to have stigmatizing notes than middle aged (45-54) patients. Hispanic patients were 12% less likely to have stigmatizing notes than non-Hispanic patients, and Asian patients were 55% less likely to have stigmatizing notes than White patients. Black patients had roughly the same amount of stigmatizing notes (65%) as White patients (63%).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study showed that a majority of patients with substance-related diagnoses in the Mass General Brigham health system have stigmatizing language in their medical records, most notably “abuse”, “substance abuse”, “alcoholic”, “user”, and “clean”. “Abuse” and “substance abuse” may remain in the medical vernacular given their presence in recent medical diagnostic nomenclature and language norms change gradually over time. For example, some notes seemed to use a premade template that said “substance abuse evaluation” followed by free text from the note author, which were included as stigmatizing language in the current study.
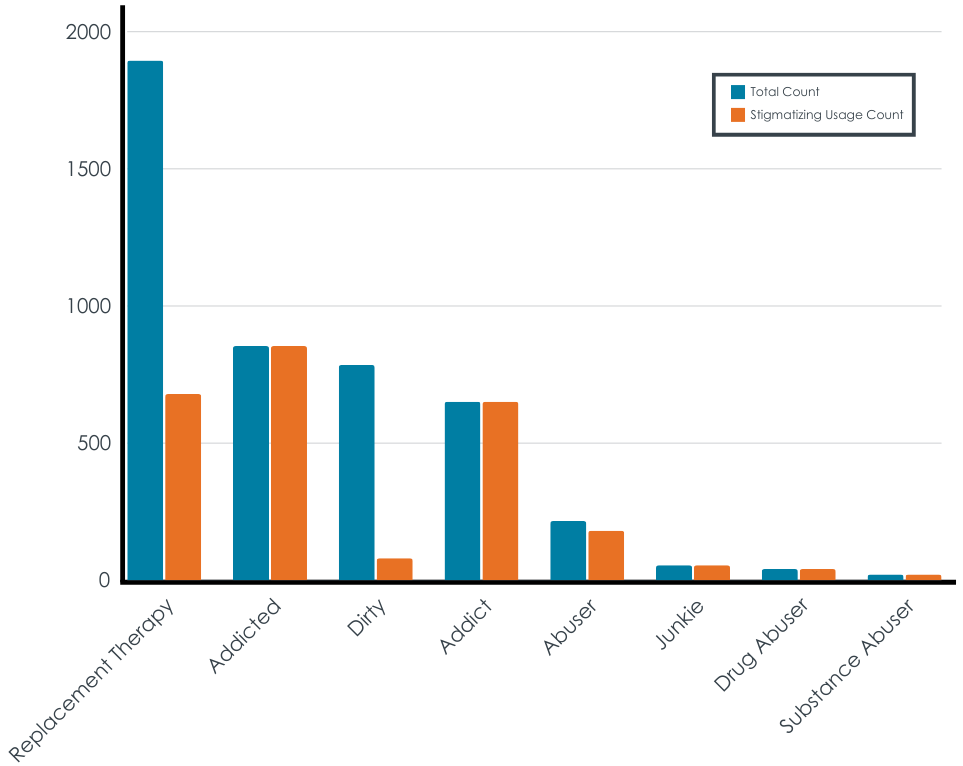
Clinicians may view these terms as acceptable, especially since federal agencies (e.g., the National Institute on Drug Abuse, the National Institute on Alcohol Abuse and Alcoholism, and the Substance Abuse and Mental Health Services Administration) continue to use these terms in their titles and they appear in common screening tools, like the Drug Abuse Screening Test (DAST-10). Additionally, there may have been cases where a patient reported a stigmatizing word that was recorded in the medical record as a quote (e.g., “the patient reports that she is a ‘junkie’” – “junkie” appeared 55 times in medical notes), which would be included as a phrase containing stigma. Unfortunately, the researchers also did not exclude the phrase “alcoholics anonymous,” from the count of stigmatizing language, of which there were 635 instances, despite it being an established name of a known organization and a proper noun. Nonetheless, stigmatizing communications can promote inaccurate and harmful stereotypes about individuals with substance use disorder. At the same time, stigma from healthcare providers is a significant barrier to patients receiving substance use disorder treatment.
Notes commonly used for inpatient hospital and emergency room visits were more likely to contain stigmatizing language compared to office visit notes.
The findings make the case for more in-hospital education about stigma, as providers who do not consistently or commonly work in substance use disorder treatment settings may be less aware to the effect stigmatizing language has on patients with substance-related diagnoses.
Notes written by physician assistants had a much higher incidence of stigmatizing language (47%) than physicians (26%) and nurses (4%). Its not clear what explains this difference, however one possibility is that physician assistants are less likely to have been trained on the new DSM-5 criteria published in 2013 for diagnosing a substance use disorder. The newer diagnostic criteria no longer use the terms “abuse” or “dependence,” whereas the previous DSM (DSM-IV-TR, published in 2000) did. Continuing education for the healthcare system on the new DSM-5 criteria and the importance of language may be helpful to reduce stigma.
Patient-level factors that indicate someone’s socioeconomic status (such as being less educated compared to higher degrees of education, with Medicaid or Medicare insurance compared with commercial, being a veteran, or being single or divorced compared to married) were all associated with increased presence of stigmatizing language. Also, Black patients had the highest proportion of 1 or more notes with stigmatizing language (65%) compared to other racial groups (White, 63%; Asian, 40%; Native American, 56%; mixed race, 54%), however the difference between White and Black patients was not statistically significant when controlling for other socioeconomic and patient factors, meaning that it’s likely an intersection of factors (e.g., someone’s race and their socioeconomic status) explaining stigmatizing language in medical notes. These findings highlight the intersectionality between substance use, stigma, racism, and social determinants of health and should serve as important reminders to clinical staff to assess their biases and be aware of how words used may affect all patients with substance use disorder.
Although this study provided important information about how common stigmatizing language is in medical notes in a large healthcare system in New England, which indicates the need for continuing education and training, the study did not measure healthcare provider behavior or patient experiences. Given that, we do not actually know how stigmatizing language in medical notes actually affected patient care. Future research should examine the association between stigmatizing language in medical notes and the quality of care from the patient’s perspective.
The type of statistical analysis used in this study is very common for examining health disparities in particular groups, however, is limited in that it “partials out” the effect of other factors that could be influencing the presence of stigmatizing language. For example, this type of analysis can tell us if there were differences between White patients and Black patients on stigmatizing notes, and the differences between male and female patients on stigmatizing notes, while controlling for or “partialling out” the effect of the other factor. However, the analysis does not tell us if there were disproportionately higher likelihood of stigma notes for certain intersections of these groups, e.g., Black male patients. In the case of the current findings, this could be important as systemic racism and substance use stigma have down-stream effects on socioeconomic factors and social determinants of health, such as insurance type and education. Thus, it may be that Black men with Medicaid insurance experienced disproportionately higher likelihood of stigma notes than White women with commercial insurance, but the current analysis does not allow for this type of comparison. Future research should consider using intersectional analyses to examine health disparities.
Finally, as the researchers acknowledge, they were unable to ascertain the gender identity of patients (e.g., transgender or gender diverse identities) as this is not currently recorded in their medical notes. This is a major limitation give the tremendous stigma that transgender patients face and could have also influenced the incidence of stigmatizing language in notes.
BOTTOM LINE
Using an innovative machine learning approach this study showed almost two-thirds of patients with substance-related diagnoses (62%) had at least one note containing stigmatizing language. While the model accounted for the context of the term to determine whether it was, in fact, stigmatizing, other contexts were not accounted for including providers quoting the patient’s own words. There were also several patient characteristic disparities associated with patients having stigmatizing language in their notes, including Medicaid or Medicare insurance compared to commercial insurance. The work suggests that more clinician interventions about use of stigmatizing language are needed.
For individuals and families seeking recovery: Often patients with substance use disorder who anticipate or have experienced stigma in healthcare settings develop negative attitudes toward seeking care and earned distrust of the healthcare system. Seeking care from substance use treatment providers with the most up-to-date training in evidence-supported care may reduce the likelihood of stigmatizing interactions. Learn more about indicators of quality addiction treatment here.
For treatment professionals and treatment systems: Language and imagery could influence a person’s willingness to initiate treatment, as well as a patient’s experience in treatment. It’s important for healthcare providers to use non-stigmatizing language in their direct patient care and clinical notes. Check out NIDA’s Words Matter list for language recommendations for healthcare providers.
For scientists:The study used a multivariate regression analysis to identify stigmatizing language disparities by patient characteristics. However, the limitation of this type of analysis is it precludes interpretation of any intersectional effects (e.g., race and insurance type, primary substance). Future research should consider using intersectional analyses to examine health disparities, as disparities for certain groups (e.g., Black male patients with Medicaid) could be washed out using multivariate regression. Additionally, although this study provided important information about how common stigmatizing language is in medical notes in a large healthcare system in New England, which indicates the need for continuing education and training, the study did not measure healthcare provider behavior or patient experiences. Future research should examine the association between stigmatizing language in medical notes and the quality of care from the patient’s perspective.
For policy makers: Continuing education for healthcare providers in all healthcare settings (i.e., not only in substance use treatment settings) could be an important intervention to reduce stigma via reductions in stigmatizing language in medical notes. Language used in medical records is increasingly important as patients have access to some of their medical records through the 21st Century Cures Act. These “open notes” have created controversy for patients with behavioral health conditions, for example when patients find in their medical record inaccurate notes, disrespectful language, or undiscussed diagnoses. Stigmatizing communications can promote inaccurate and harmful stereotypes about individuals with substance use disorder and stigma from healthcare providers is a significant barrier to patients receiving substance use disorder treatment. Policies that support healthcare provider training could reduce substance use stigma and could reduce barriers to treatment for patients with substance use disorder. Check out NIDA’s Words Matter list for language recommendations appropriate for professionals and the images from this study for ideas on non-stigmatizing images.
There are many studies showing that negative attitudes of healthcare providers towards people with substance use disorders are common and contribute to suboptimal health outcomes for these individuals. For example, in a large systematic review, healthcare providers often attributed blame to the patients themselves as barriers to treatment engagement, citing reasons such as perceived violence, manipulation, and lack of motivation. Healthcare providers also demonstrated inadequate knowledge, training, and support to treat individuals with substance use disorder. These negative attitudes and lack of adequate training among providers coincide with disempowerment of patients and result in substandard healthcare, including diminished collaboration between patients and providers.
Stigma can be experienced and communicated in various forms, including in the language that medical personnel use when referring to individuals with substance use disorder. Just small differences, such as referring to an individual as “a substance abuser” versus “having a substance use disorder,” can lead to differential judgments – in both clinical experts and the general public – about whether the individual with substance use disorder is to blame for their condition and their likelihood of recovery.
Stigmatizing language in general is pervasive in medical records, which may impact patients as well as healthcare team members. It applies not only to individuals with substance use disorder but also to other conditions including chronic pain and diabetes. In a large study of individuals (not just those with substance use disorder) who read at least one of their outpatient medical notes, more than 10% reported feeling judged and/or offended.
One key aim of the US Department of Health and Human Services’ harm reduction pillar is to “develop educational materials and programs to reduce stigma.” Training for providers that addresses this stigma has increased in recent years, although some research suggests that negative attitudes toward people who use drugs are still pervasive among healthcare providers. One recent study, for example, showed that 75% of primary care physicians surveyed reported high levels of stigma towards individuals with opioid use disorder, on par with stigma toward these individuals in the general population. It can be difficult to monitor and measure stigma in large healthcare systems – examining clinical notes is one innovative, unobtrusive way to do this. In turn, these data can inform content for stigma reduction interventions among healthcare providers.
In this study, the researchers examined the incidence of stigmatizing language in clinical notes of a large healthcare system specific to patients with substance-related diagnoses and reported on any disparities associated with demographic characteristics of patients (e.g., race/ethnicity, gender).
HOW WAS THIS STUDY CONDUCTED?
This was a cross-sectional, observational, retrospective study from December 1, 2020 to November 30, 2021 of hospital notes contained in the electronic health record (EHR) of Mass General Brigham, a large healthcare system in Massachusetts and New Hampshire. The study identified 546,309 clinical notes for review for the use of stigmatizing language in the body of the note from 30,391 patients with at least one substance-related diagnosis code. The incidence of stigmatizing language in medical notes (i.e., how common it was for stigmatizing language to be present in the medical notes) was reported by patient characteristics (e.g., race, ethnicity, socioeconomic status) and provider characteristics (e.g., physicians, physician assistants, nurses, etc.) to identify any disparities (i.e., undue or preventable differences by group).
Hospital notes included for analysis were all free-text notes from patients who had at least one inpatient and/or outpatient visit(s) in the Mass General Brigham health system during the 1-year period between December 1, 2020 and November 30, 2021, and whose encounter diagnosis contained at least one substance-related diagnosis code. The researchers used a list of 24 ICD-10 (International Classification of Diseases, Tenth Revision) codes that capture substance use disorders, as well as codes associated with overdose of drugs and alcohol. Medical notes from a range of providers were included: physicians, physicians, advanced-practice providers, nurses, social workers, and others who interact with patients and document the encounter. Types of notes included: history and physicals, consults, discharge summaries, emergency department (ED) notes, group therapy notes, transfer/sign-off notes, progress notes, ED nurse triage notes, nursing notes, assessment/plan notes, nursing summaries, plan of care, and opioid notes (a special note type created by the healthcare facility, which lists the indication for opioid prescriptions, the primary prescriber, and substance use disorder-related risk factors). Patient-reported demographic data, including age, sex, race, and ethnicity were also recorded for each note.
The researchers developed a natural language processing algorithm using the National Institute on Drug Abuse’s “Words Matter” list to identify use of stigmatizing language in context. The researchers randomly selected 10,000 clinical notes with stigmatizing key words to develop the algorithm and extract information from the notes to determine the semantic meaning based on the context. For example, (1) the use of the word “alcoholic” is discouraged, yet there are uses of the word which are deemed clinically acceptable, such as “alcoholic cirrhosis” or “alcoholic hepatitis.” In these cases, “alcoholic” was deemed stigma only if it was used as a noun, for example, “the patient is an alcoholic” (note that the term was considered stigmatizing when used to describe the 12-step mutual-help organization Alcoholics Anonymous); (2) use of the word “abuse” is discouraged, yet it can be acceptable in some cases. If “abuse” was used in “drug abuse” or “alcohol abuse,” it was categorized as stigma, but if it was “emotional abuse” or “physical abuse,” it was not; and (3) the word “user” is discouraged, yet the word is commonly used in other contexts, such as “her user login name is.” Therefore, the researchers included the word as stigmatizing if it followed a drug name, such as “he is a marijuana user” or “she is a heroin user.” Based on the context of that language in the sentence, the algorithm identified sentences containing a stigmatizing keyword(s) and determined whether the sentence contained stigmatization meaning or not. If a clinical note had at least one stigmatizing sentence, it was regarded as a stigmatizing note.
During the 1-year study period, there were 30,391 patients seen in the healthcare system who had both a substance-related encounter (e.g., outpatient treatment) and at least one clinical note recorded. Patients were on average 47.7 years old at the time of the encounter, 38% were female, 81% were White, and 9% reported Hispanic ethnicity. Overall, the algorithm determined that 62% of patients had at least one note containing stigmatizing language. Black patients (65%) and patients with Medicaid insurance (70%) had disproportionately higher percentages of stigmatizing language in their medical notes.
WHAT DID THIS STUDY FIND?
Notes with stigmatizing terms were common
There were 546,309 notes for 30,391 patients, of which 100,792 (18%) contained stigmatizing language. A total of 18,727 patients (62%) had at least one note with stigmatizing language. Hospital encounters (20%) were more likely to contain stigmatizing language than were office visits (14%). About a quarter of physician (26%) and nurse practitioner notes (24%) were stigmatizing, physician assistants had a higher proportion of stigmatizing language (47%), and nurses had a lower rate (4%). The most common note type was “progress note,” for which 15% contained stigmatizing language. History and physical notes were most likely to contain stigmatizing language (59%). In general, nursing notes, including ED triage notes (6%), nursing summaries (2%), and nursing notes (2%), had lower incidences of stigma.
Medicaid patients had disproportionately higher rates of stigmatizing notes
When controlling for the effect of other factors including age, sex, race, ethnicity, marital status, education level, and veteran status, patients with Medicaid or Medicare insurance were 1.5 times more likely to have stigmatizing notes than those with commercial insurance; 70% of Medicaid patients had at least one stigmatizing note, compared to only 57% of commercially-insured patients. Patients with a greater number of encounters were more likely to have stigmatizing notes, with the greatest number experienced by patients with 20 or more encounters who were 6.6 times more likely to have a stigmatizing note, indicating that the more patients interacted with the health system, the greater the odds of having at least one note containing stigmatizing language.
Certain gender, age, and racial/ethnicgroups were more likely to have stigmatizing language in their notes than their counterparts
When controlling for the effect of other demographic and socioeconomic factors, male patients were 17% more likely to have stigmatizing language in their notes than female patients. Younger patients aged 18-24 were 45% less likely to have stigmatizing notes than middle aged (45-54) patients. Hispanic patients were 12% less likely to have stigmatizing notes than non-Hispanic patients, and Asian patients were 55% less likely to have stigmatizing notes than White patients. Black patients had roughly the same amount of stigmatizing notes (65%) as White patients (63%).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study showed that a majority of patients with substance-related diagnoses in the Mass General Brigham health system have stigmatizing language in their medical records, most notably “abuse”, “substance abuse”, “alcoholic”, “user”, and “clean”. “Abuse” and “substance abuse” may remain in the medical vernacular given their presence in recent medical diagnostic nomenclature and language norms change gradually over time. For example, some notes seemed to use a premade template that said “substance abuse evaluation” followed by free text from the note author, which were included as stigmatizing language in the current study.
Clinicians may view these terms as acceptable, especially since federal agencies (e.g., the National Institute on Drug Abuse, the National Institute on Alcohol Abuse and Alcoholism, and the Substance Abuse and Mental Health Services Administration) continue to use these terms in their titles and they appear in common screening tools, like the Drug Abuse Screening Test (DAST-10). Additionally, there may have been cases where a patient reported a stigmatizing word that was recorded in the medical record as a quote (e.g., “the patient reports that she is a ‘junkie’” – “junkie” appeared 55 times in medical notes), which would be included as a phrase containing stigma. Unfortunately, the researchers also did not exclude the phrase “alcoholics anonymous,” from the count of stigmatizing language, of which there were 635 instances, despite it being an established name of a known organization and a proper noun. Nonetheless, stigmatizing communications can promote inaccurate and harmful stereotypes about individuals with substance use disorder. At the same time, stigma from healthcare providers is a significant barrier to patients receiving substance use disorder treatment.
Notes commonly used for inpatient hospital and emergency room visits were more likely to contain stigmatizing language compared to office visit notes.
The findings make the case for more in-hospital education about stigma, as providers who do not consistently or commonly work in substance use disorder treatment settings may be less aware to the effect stigmatizing language has on patients with substance-related diagnoses.
Notes written by physician assistants had a much higher incidence of stigmatizing language (47%) than physicians (26%) and nurses (4%). Its not clear what explains this difference, however one possibility is that physician assistants are less likely to have been trained on the new DSM-5 criteria published in 2013 for diagnosing a substance use disorder. The newer diagnostic criteria no longer use the terms “abuse” or “dependence,” whereas the previous DSM (DSM-IV-TR, published in 2000) did. Continuing education for the healthcare system on the new DSM-5 criteria and the importance of language may be helpful to reduce stigma.
Patient-level factors that indicate someone’s socioeconomic status (such as being less educated compared to higher degrees of education, with Medicaid or Medicare insurance compared with commercial, being a veteran, or being single or divorced compared to married) were all associated with increased presence of stigmatizing language. Also, Black patients had the highest proportion of 1 or more notes with stigmatizing language (65%) compared to other racial groups (White, 63%; Asian, 40%; Native American, 56%; mixed race, 54%), however the difference between White and Black patients was not statistically significant when controlling for other socioeconomic and patient factors, meaning that it’s likely an intersection of factors (e.g., someone’s race and their socioeconomic status) explaining stigmatizing language in medical notes. These findings highlight the intersectionality between substance use, stigma, racism, and social determinants of health and should serve as important reminders to clinical staff to assess their biases and be aware of how words used may affect all patients with substance use disorder.
Although this study provided important information about how common stigmatizing language is in medical notes in a large healthcare system in New England, which indicates the need for continuing education and training, the study did not measure healthcare provider behavior or patient experiences. Given that, we do not actually know how stigmatizing language in medical notes actually affected patient care. Future research should examine the association between stigmatizing language in medical notes and the quality of care from the patient’s perspective.
The type of statistical analysis used in this study is very common for examining health disparities in particular groups, however, is limited in that it “partials out” the effect of other factors that could be influencing the presence of stigmatizing language. For example, this type of analysis can tell us if there were differences between White patients and Black patients on stigmatizing notes, and the differences between male and female patients on stigmatizing notes, while controlling for or “partialling out” the effect of the other factor. However, the analysis does not tell us if there were disproportionately higher likelihood of stigma notes for certain intersections of these groups, e.g., Black male patients. In the case of the current findings, this could be important as systemic racism and substance use stigma have down-stream effects on socioeconomic factors and social determinants of health, such as insurance type and education. Thus, it may be that Black men with Medicaid insurance experienced disproportionately higher likelihood of stigma notes than White women with commercial insurance, but the current analysis does not allow for this type of comparison. Future research should consider using intersectional analyses to examine health disparities.
Finally, as the researchers acknowledge, they were unable to ascertain the gender identity of patients (e.g., transgender or gender diverse identities) as this is not currently recorded in their medical notes. This is a major limitation give the tremendous stigma that transgender patients face and could have also influenced the incidence of stigmatizing language in notes.
BOTTOM LINE
Using an innovative machine learning approach this study showed almost two-thirds of patients with substance-related diagnoses (62%) had at least one note containing stigmatizing language. While the model accounted for the context of the term to determine whether it was, in fact, stigmatizing, other contexts were not accounted for including providers quoting the patient’s own words. There were also several patient characteristic disparities associated with patients having stigmatizing language in their notes, including Medicaid or Medicare insurance compared to commercial insurance. The work suggests that more clinician interventions about use of stigmatizing language are needed.
For individuals and families seeking recovery: Often patients with substance use disorder who anticipate or have experienced stigma in healthcare settings develop negative attitudes toward seeking care and earned distrust of the healthcare system. Seeking care from substance use treatment providers with the most up-to-date training in evidence-supported care may reduce the likelihood of stigmatizing interactions. Learn more about indicators of quality addiction treatment here.
For treatment professionals and treatment systems: Language and imagery could influence a person’s willingness to initiate treatment, as well as a patient’s experience in treatment. It’s important for healthcare providers to use non-stigmatizing language in their direct patient care and clinical notes. Check out NIDA’s Words Matter list for language recommendations for healthcare providers.
For scientists:The study used a multivariate regression analysis to identify stigmatizing language disparities by patient characteristics. However, the limitation of this type of analysis is it precludes interpretation of any intersectional effects (e.g., race and insurance type, primary substance). Future research should consider using intersectional analyses to examine health disparities, as disparities for certain groups (e.g., Black male patients with Medicaid) could be washed out using multivariate regression. Additionally, although this study provided important information about how common stigmatizing language is in medical notes in a large healthcare system in New England, which indicates the need for continuing education and training, the study did not measure healthcare provider behavior or patient experiences. Future research should examine the association between stigmatizing language in medical notes and the quality of care from the patient’s perspective.
For policy makers: Continuing education for healthcare providers in all healthcare settings (i.e., not only in substance use treatment settings) could be an important intervention to reduce stigma via reductions in stigmatizing language in medical notes. Language used in medical records is increasingly important as patients have access to some of their medical records through the 21st Century Cures Act. These “open notes” have created controversy for patients with behavioral health conditions, for example when patients find in their medical record inaccurate notes, disrespectful language, or undiscussed diagnoses. Stigmatizing communications can promote inaccurate and harmful stereotypes about individuals with substance use disorder and stigma from healthcare providers is a significant barrier to patients receiving substance use disorder treatment. Policies that support healthcare provider training could reduce substance use stigma and could reduce barriers to treatment for patients with substance use disorder. Check out NIDA’s Words Matter list for language recommendations appropriate for professionals and the images from this study for ideas on non-stigmatizing images.