“Paperwork vs progress”: The real-world barriers and facilitators of patient-reported outcome measures
Measuring patient outcomes with brief questionnaires, sometimes referred to as “measurement-based practice”, can improve treatment effects because it engages patients better and sensitizes therapists to key changes. Yet, there are often barriers to its implementation. This study examined staff reactions to outcome measurement in their clinical program.
Measurement-based practice is an evidence-based approach that involves ongoing assessment of treatment targets to guide clinical decisions, empower patients, and enhance health outcomes. The process of incorporating systematic outcome measures into treatment has been referred to as progress monitoring, outcome monitoring, measurement-based care, and the use of feedback systems.
Patient-reported outcome measures are a widely used method for administering assessments and providing feedback in alcohol and other drug treatment. In contrast, measurement-based care that does not rely on patient reports may include objective indicators, such as toxicology screens. However, adopting patient-reported outcome measures into regular care is a challenge for many substance use treatment centers.
Many efforts to implement evidence-based practices fail, despite carefully laid plans. Understanding the barriers and facilitators within a specific organization(s) can highlight future innovation tailoring, resource management, and staff trainings to successfully implement an innovation and see positive outcomes for individuals receiving services.
Understanding the barriers and facilitators of patient-reported outcome measures within substance use treatment may help improve patients’ outcomes. This study investigated the implementation of patient-reported outcome measures through interviews and surveys among substance use treatment counselors.
HOW WAS THIS STUDY CONDUCTED?
This study included interviews as well as quantitative surveys to apply the Consolidated Framework for Implementation Research to understand barriers and facilitators to implementing patient-reported outcome measures in substance use treatment. All data was collected from a large non-profit provider of inpatient and outpatient substance use treatment in Australia. The organization mainly provides counseling services and has collected patient-reported outcome measures electronically as standard practice since April 2020.
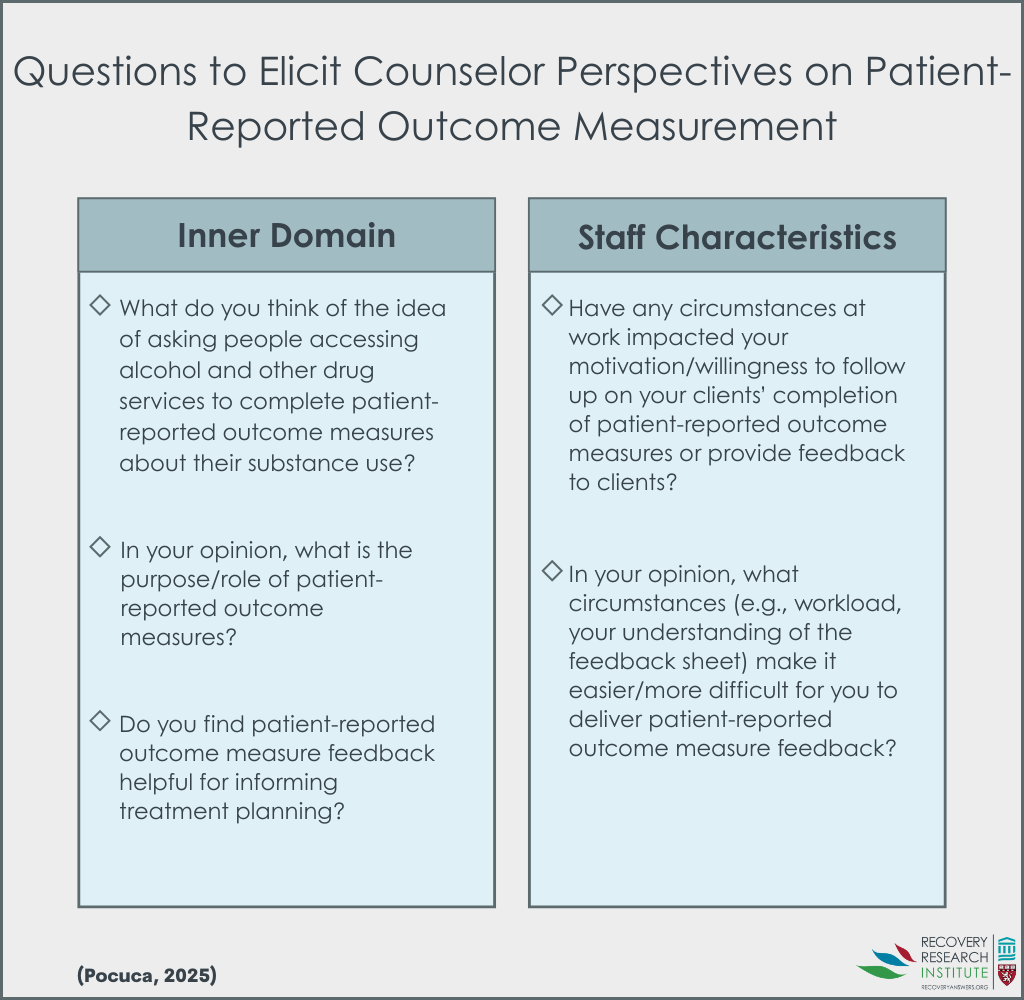
There were 23 counselors who participated; they were mostly female (78%), and the average age was 43 years old. The interviews featured questions designed to understand barriers and facilitators to the implementation of patient-reported outcome measures and feedback based on the Inner Setting and Individual Characteristic domains from the Consolidated Framework for Implementation Research (Figure below).
Each interview was recorded and then transcribed for analysis. The interviews ranged in length from 29 to 74 minutes, and they were conducted until no new themes were identified (i.e., “thematic saturation”). Then the qualitative analysis team iteratively developed a codebook based of the Framework, interview guide, and emergent themes found in the interviews. The team then met to discuss and arrive at a group of final themes.
There were 108 counselors who were part of the original rollout of the patient-reported outcome measure implementation that participated in the quantitative survey (out of a possible 141 counselors). The study team developed 4 survey measures: knowledge and beliefs regarding patient-reported outcome measures and feedback; patient-reported outcome measures and self-efficacy; leadership support for patient-reported outcome measures; and available resources for patient-reported outcome measures. The first comprised 10 questions asking how much participants agreed (on a scale from 1 [strongly disagree] to 7 [ strongly agree]) with statements about patient-reported outcome measures and feedback (e.g., “Outcome measures take into consideration the needs and preferences of clients”). The second included 7 items assessing how confident participants were with aspects of patient-reported outcome measures on a scale from 1 [not confident] to 5 [very confident] (e.g., “motivating clients to complete outcome measures”). The third featured 2 items that assess organizational leadership and direct supervisor support for patient-reported outcome measures on a scale from 1 [strongly disagree] to 7 [strongly agree]. The fourth asked participants on a scale from 1 [strongly disagree] to 7 [ strongly agree] their level of agreement with the availability of 6 resources to deliver patient-reported outcome measures and related feedback (e.g., equipment and materials). Analyses examined the relationship between leadership support and available resources with participant knowledge, beliefs, and self-efficacy, while accounting for participant demographics.
Participants of the survey were, on average, 41 years old and mostly female (79%). About half completed a Bachelors (53%), while 18% completed a master’s and 29% completed a Certificate or diploma. There were 71% who reported working in the substance use sector for 3 or more years, and 41% reported working at the treatment service for 3 or more years.
WHAT DID THIS STUDY FIND?
Most staff thought patient-reported outcome measures were valuable
There were 17 participants that focused on the benefits of patient-reported outcomes measures in several ways: 1) provide staff with a snapshot of a client’s situation; 2) help facilitate dialogue; 3) promote client self-reflection and insight; 4) allow for progress tracking.
“[Patient-reported outcome measures give] us a bit of a picture of how the client presents, where they’re at, sort of cuts through a little bit of rapport work.’
Staff resistance to patient-reported outcome measures hinders implementation
Many participants felt patient-reported outcomes offered little advantage and actually hindered their treatment, which lead them to resist implementation. In particular participants 1) believed the information collected from the measures was already collected through discussions with the client; 2) the measures were too rigid and did not align with their clinical style; 3) felt the measures were complex and time-consuming, which diverted time away from delivering treatment to the clients; 4) saw the patient-reported outcome measures at odds with their norms, values, and beliefs, particularly around the need for client-centered treatment.
“There’s an expectation that we’ll use a session to complete an outcome measure, which I think, while there’s some really valuable data, it easily takes up the best part of a session, because most people will talk through it. When considering we only have five or six sessions, basically a session is gone…”
Competing interests, logistical issues, and resource limitations hinder implementation
There were 14 staff that discussed competing interests and logistical issues related to the lack of time to implement patient-reported outcome measures during treatment. Participants expressed that the patient-reported outcome measures were an organizational expectation that did not always align with the client needs in the session. The organizational versus client expectations would, at times, be at odds, which limited staffs’ full engagement in the patient-reported outcome measure process. They also noted that the organization lacked the resources to facilitate smooth administration and reflection of the measures. Staff had to spend time organizing results and feedback, which further limited their availability.
“Well, often, you have an idea of what you’re going to do in the session, but [the client] might come to you in crisis, and the last thing they want to do is discuss outcome measure results. So it can be like—not even necessarily crisis, but that’s not on their agenda. They want to talk about their feelings. They want to talk about what’s happened. So, I haven’t really gotten into great practice of going through [outcome measure feedback] with them.”’
Staff perceived patient-reported outcomes measures to be a burden for clients and may disengage them from treatment
There were 16 participants who felt that patient-reported outcome measures may be a burden for clients due to their time requirement, complexity, and resource requirement (e.g., needing to have internet access). Staff also observed low client motivation, ambivalence, and even resistance to completing the measures, which leads directly to clients disengaging from treatment.
“I have had some [clients] that just don’t want to do [patient-reported outcome measures]. They just want to come in and talk to somebody … So, I probably had three that have refused the service due to the outcome measures.”
Staff perceptions of organizational factors was related to knowledge and beliefs, as well as self-efficacy to implement, patient-reported outcome measures
Survey results showed that higher perceived leadership support and available resources were associated with increased knowledge and beliefs about patient-reported outcome measures and feedback. These effects were medium in size. Age, gender, highest degree completed, and length of time working at the treatment service were not related to knowledge and beliefs. In contrast, only perception of available resources for patient-reported outcome measure implementation was connected to staff’s self-efficacy to implement the measures and their feedback. As perceived resources increased, so too did the self-efficacy to implement the measures; however, the effect was small in magnitude.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The use of regular assessment of clinical targets often improves patient outcomes and helps get patients with worsening symptoms back on track. However, the real-world implementation of patient-reported outcome measures and feedback in substance use treatment services has faced barriers. Findings from this mixed-method study suggest that although patient-reported outcome measures and related feedback provide benefits, several staff and organizational characteristics hinder the implementation of patient-reported outcome measures and feedback in substance use treatment. The findings underscore the importance of understanding where and for whom an innovation (i.e., intervention) is being implemented. In the treatment system in Australia that was part of this study, staff and organizational characteristics specifically were seen to hinder the implementation of patient-reported outcome measures, despite most study participants seeing their value.
The study found that improved support from leadership, effective training on patient-reported outcome measures, and the provision of adequate resources would likely improve patient-reported outcome measure implementation in this specific treatment system in Australia. While not mentioned in the study, if resources permit, hiring one or more staff members whose job is dedicated to patient-reported outcome measures may help address clinical/time barriers and ultimately improve implementation. There are other key domains that, if better understood and addressed, may improve uptake of patient reported outcome measures and thus patient outcomes. For example, state policies and reporting requirements (i.e., the outer setting) may impact the extent to which organizations and staff have the time and resources to implement patient-reported outcome measures. The methods by which patient-reported outcome measures are collected and reviewed are also likely to influence their impact. The use of enhanced technology to collect and analyze patient-reported outcome measures, for example, may lead to more successful implementation. Further research is needed to identify the barriers and facilitators of implementation and to tailor innovations that address challenges and leverage opportunities.
Caution should be taken when trying to generalize these findings to other treatment centers inside and outside of Australia. The treatment system in this study is likely to be qualitatively different from others, which would impact the implementation domains explored and their findings.
This study only explored client-facing staff perceptions, which may not be representative of client or other key stakeholder perceptions. The study also does not specify whether participants in the qualitative and quantitative parts of the study were representative of the wider staff population in the treatment.
There are no validated measures for the implementation indicators used in this study, which may limit the accuracy of the results in representing the intended concepts.
BOTTOM LINE
Going beyond “what works” to “what works where, why, by whom, and for whom” is a key step in improving outcomes in substance use treatment services. Results from this study highlighted that although many staff viewed patient-reported outcome measures as valuable to the treatment process, there were staff and organizational characteristics that hindered their implementation. Negative perceptions of patient-reported outcome measures, low relative priority, and lack of time and resources were some of the key barriers to implementation. At the same time, support from leadership, effective training on patient-reported outcome measures, and the provision of adequate resources may improve implementation.
For individuals and families seeking recovery: The researchers in this study identified facilitators and barriers to implementing patient-reported outcome measures in substance use treatment settings. They found that staff perceptions and organizational resources may hinder their implementation. When evaluating treatment programs, inquire whether patient progress is systematically and regularly assessed.
For treatment professionals and treatment systems: The researchers in this study found that staff and organizational characteristics could hinder the implementation of evidence-based patient-reported outcome measures. Specifically, negative staff views and a lack of available time and resources were barriers to implementation. Prior to implementing an evidence-based practice, it would be helpful to examine how the context of implementation may impact the success of that intervention. For example, if there is not enough time to provide client-driven discussions as well as patient-reported outcomes, then exploring how they might complete the measures prior to session may help. Similarly, a treatment system may benefit from providing tailored trainings to their staff on how and why an intervention may benefit patients, even if it is not part of their routine practice. If resources permit, hiring staff whose job is dedicated to patient-reported outcome measures may help address clinical barriers.
For scientists: The research findings suggested that patient-reported outcome measures were seen as potentially valuable; however, there were staff and organizational barriers to implementation. For example, negative views of the measures, competing interests, and a lack of resources are barriers to implementing measures and feedback. This implementation study focused specially on individual and inner setting indicators from the perception of client-facing treatment staff. Future work is needed to see how these specific domains and indicators are influential in other treatment and recovery spaces as well as how other domains (e.g., outer setting, innovation characteristics) impact patient outcomes.
For policy makers: Moving beyond what works to what works, why, for whom, and by whom will help improve treatment outcomes. This study showed that negative staff views and a lack of available time and resources were barriers to implementing patient reported outcome measures. Policies that provide treatment systems with more resources to provide tailored trainings to their staff and to hire staff whose job is dedicated to patient-reported outcome measures may help address these clinical barriers to implementation.
Measurement-based practice is an evidence-based approach that involves ongoing assessment of treatment targets to guide clinical decisions, empower patients, and enhance health outcomes. The process of incorporating systematic outcome measures into treatment has been referred to as progress monitoring, outcome monitoring, measurement-based care, and the use of feedback systems.
Patient-reported outcome measures are a widely used method for administering assessments and providing feedback in alcohol and other drug treatment. In contrast, measurement-based care that does not rely on patient reports may include objective indicators, such as toxicology screens. However, adopting patient-reported outcome measures into regular care is a challenge for many substance use treatment centers.
Many efforts to implement evidence-based practices fail, despite carefully laid plans. Understanding the barriers and facilitators within a specific organization(s) can highlight future innovation tailoring, resource management, and staff trainings to successfully implement an innovation and see positive outcomes for individuals receiving services.
Understanding the barriers and facilitators of patient-reported outcome measures within substance use treatment may help improve patients’ outcomes. This study investigated the implementation of patient-reported outcome measures through interviews and surveys among substance use treatment counselors.
HOW WAS THIS STUDY CONDUCTED?
This study included interviews as well as quantitative surveys to apply the Consolidated Framework for Implementation Research to understand barriers and facilitators to implementing patient-reported outcome measures in substance use treatment. All data was collected from a large non-profit provider of inpatient and outpatient substance use treatment in Australia. The organization mainly provides counseling services and has collected patient-reported outcome measures electronically as standard practice since April 2020.
There were 23 counselors who participated; they were mostly female (78%), and the average age was 43 years old. The interviews featured questions designed to understand barriers and facilitators to the implementation of patient-reported outcome measures and feedback based on the Inner Setting and Individual Characteristic domains from the Consolidated Framework for Implementation Research (Figure below).
Each interview was recorded and then transcribed for analysis. The interviews ranged in length from 29 to 74 minutes, and they were conducted until no new themes were identified (i.e., “thematic saturation”). Then the qualitative analysis team iteratively developed a codebook based of the Framework, interview guide, and emergent themes found in the interviews. The team then met to discuss and arrive at a group of final themes.
There were 108 counselors who were part of the original rollout of the patient-reported outcome measure implementation that participated in the quantitative survey (out of a possible 141 counselors). The study team developed 4 survey measures: knowledge and beliefs regarding patient-reported outcome measures and feedback; patient-reported outcome measures and self-efficacy; leadership support for patient-reported outcome measures; and available resources for patient-reported outcome measures. The first comprised 10 questions asking how much participants agreed (on a scale from 1 [strongly disagree] to 7 [ strongly agree]) with statements about patient-reported outcome measures and feedback (e.g., “Outcome measures take into consideration the needs and preferences of clients”). The second included 7 items assessing how confident participants were with aspects of patient-reported outcome measures on a scale from 1 [not confident] to 5 [very confident] (e.g., “motivating clients to complete outcome measures”). The third featured 2 items that assess organizational leadership and direct supervisor support for patient-reported outcome measures on a scale from 1 [strongly disagree] to 7 [strongly agree]. The fourth asked participants on a scale from 1 [strongly disagree] to 7 [ strongly agree] their level of agreement with the availability of 6 resources to deliver patient-reported outcome measures and related feedback (e.g., equipment and materials). Analyses examined the relationship between leadership support and available resources with participant knowledge, beliefs, and self-efficacy, while accounting for participant demographics.
Participants of the survey were, on average, 41 years old and mostly female (79%). About half completed a Bachelors (53%), while 18% completed a master’s and 29% completed a Certificate or diploma. There were 71% who reported working in the substance use sector for 3 or more years, and 41% reported working at the treatment service for 3 or more years.
WHAT DID THIS STUDY FIND?
Most staff thought patient-reported outcome measures were valuable
There were 17 participants that focused on the benefits of patient-reported outcomes measures in several ways: 1) provide staff with a snapshot of a client’s situation; 2) help facilitate dialogue; 3) promote client self-reflection and insight; 4) allow for progress tracking.
“[Patient-reported outcome measures give] us a bit of a picture of how the client presents, where they’re at, sort of cuts through a little bit of rapport work.’
Staff resistance to patient-reported outcome measures hinders implementation
Many participants felt patient-reported outcomes offered little advantage and actually hindered their treatment, which lead them to resist implementation. In particular participants 1) believed the information collected from the measures was already collected through discussions with the client; 2) the measures were too rigid and did not align with their clinical style; 3) felt the measures were complex and time-consuming, which diverted time away from delivering treatment to the clients; 4) saw the patient-reported outcome measures at odds with their norms, values, and beliefs, particularly around the need for client-centered treatment.
“There’s an expectation that we’ll use a session to complete an outcome measure, which I think, while there’s some really valuable data, it easily takes up the best part of a session, because most people will talk through it. When considering we only have five or six sessions, basically a session is gone…”
Competing interests, logistical issues, and resource limitations hinder implementation
There were 14 staff that discussed competing interests and logistical issues related to the lack of time to implement patient-reported outcome measures during treatment. Participants expressed that the patient-reported outcome measures were an organizational expectation that did not always align with the client needs in the session. The organizational versus client expectations would, at times, be at odds, which limited staffs’ full engagement in the patient-reported outcome measure process. They also noted that the organization lacked the resources to facilitate smooth administration and reflection of the measures. Staff had to spend time organizing results and feedback, which further limited their availability.
“Well, often, you have an idea of what you’re going to do in the session, but [the client] might come to you in crisis, and the last thing they want to do is discuss outcome measure results. So it can be like—not even necessarily crisis, but that’s not on their agenda. They want to talk about their feelings. They want to talk about what’s happened. So, I haven’t really gotten into great practice of going through [outcome measure feedback] with them.”’
Staff perceived patient-reported outcomes measures to be a burden for clients and may disengage them from treatment
There were 16 participants who felt that patient-reported outcome measures may be a burden for clients due to their time requirement, complexity, and resource requirement (e.g., needing to have internet access). Staff also observed low client motivation, ambivalence, and even resistance to completing the measures, which leads directly to clients disengaging from treatment.
“I have had some [clients] that just don’t want to do [patient-reported outcome measures]. They just want to come in and talk to somebody … So, I probably had three that have refused the service due to the outcome measures.”
Staff perceptions of organizational factors was related to knowledge and beliefs, as well as self-efficacy to implement, patient-reported outcome measures
Survey results showed that higher perceived leadership support and available resources were associated with increased knowledge and beliefs about patient-reported outcome measures and feedback. These effects were medium in size. Age, gender, highest degree completed, and length of time working at the treatment service were not related to knowledge and beliefs. In contrast, only perception of available resources for patient-reported outcome measure implementation was connected to staff’s self-efficacy to implement the measures and their feedback. As perceived resources increased, so too did the self-efficacy to implement the measures; however, the effect was small in magnitude.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The use of regular assessment of clinical targets often improves patient outcomes and helps get patients with worsening symptoms back on track. However, the real-world implementation of patient-reported outcome measures and feedback in substance use treatment services has faced barriers. Findings from this mixed-method study suggest that although patient-reported outcome measures and related feedback provide benefits, several staff and organizational characteristics hinder the implementation of patient-reported outcome measures and feedback in substance use treatment. The findings underscore the importance of understanding where and for whom an innovation (i.e., intervention) is being implemented. In the treatment system in Australia that was part of this study, staff and organizational characteristics specifically were seen to hinder the implementation of patient-reported outcome measures, despite most study participants seeing their value.
The study found that improved support from leadership, effective training on patient-reported outcome measures, and the provision of adequate resources would likely improve patient-reported outcome measure implementation in this specific treatment system in Australia. While not mentioned in the study, if resources permit, hiring one or more staff members whose job is dedicated to patient-reported outcome measures may help address clinical/time barriers and ultimately improve implementation. There are other key domains that, if better understood and addressed, may improve uptake of patient reported outcome measures and thus patient outcomes. For example, state policies and reporting requirements (i.e., the outer setting) may impact the extent to which organizations and staff have the time and resources to implement patient-reported outcome measures. The methods by which patient-reported outcome measures are collected and reviewed are also likely to influence their impact. The use of enhanced technology to collect and analyze patient-reported outcome measures, for example, may lead to more successful implementation. Further research is needed to identify the barriers and facilitators of implementation and to tailor innovations that address challenges and leverage opportunities.
Caution should be taken when trying to generalize these findings to other treatment centers inside and outside of Australia. The treatment system in this study is likely to be qualitatively different from others, which would impact the implementation domains explored and their findings.
This study only explored client-facing staff perceptions, which may not be representative of client or other key stakeholder perceptions. The study also does not specify whether participants in the qualitative and quantitative parts of the study were representative of the wider staff population in the treatment.
There are no validated measures for the implementation indicators used in this study, which may limit the accuracy of the results in representing the intended concepts.
BOTTOM LINE
Going beyond “what works” to “what works where, why, by whom, and for whom” is a key step in improving outcomes in substance use treatment services. Results from this study highlighted that although many staff viewed patient-reported outcome measures as valuable to the treatment process, there were staff and organizational characteristics that hindered their implementation. Negative perceptions of patient-reported outcome measures, low relative priority, and lack of time and resources were some of the key barriers to implementation. At the same time, support from leadership, effective training on patient-reported outcome measures, and the provision of adequate resources may improve implementation.
For individuals and families seeking recovery: The researchers in this study identified facilitators and barriers to implementing patient-reported outcome measures in substance use treatment settings. They found that staff perceptions and organizational resources may hinder their implementation. When evaluating treatment programs, inquire whether patient progress is systematically and regularly assessed.
For treatment professionals and treatment systems: The researchers in this study found that staff and organizational characteristics could hinder the implementation of evidence-based patient-reported outcome measures. Specifically, negative staff views and a lack of available time and resources were barriers to implementation. Prior to implementing an evidence-based practice, it would be helpful to examine how the context of implementation may impact the success of that intervention. For example, if there is not enough time to provide client-driven discussions as well as patient-reported outcomes, then exploring how they might complete the measures prior to session may help. Similarly, a treatment system may benefit from providing tailored trainings to their staff on how and why an intervention may benefit patients, even if it is not part of their routine practice. If resources permit, hiring staff whose job is dedicated to patient-reported outcome measures may help address clinical barriers.
For scientists: The research findings suggested that patient-reported outcome measures were seen as potentially valuable; however, there were staff and organizational barriers to implementation. For example, negative views of the measures, competing interests, and a lack of resources are barriers to implementing measures and feedback. This implementation study focused specially on individual and inner setting indicators from the perception of client-facing treatment staff. Future work is needed to see how these specific domains and indicators are influential in other treatment and recovery spaces as well as how other domains (e.g., outer setting, innovation characteristics) impact patient outcomes.
For policy makers: Moving beyond what works to what works, why, for whom, and by whom will help improve treatment outcomes. This study showed that negative staff views and a lack of available time and resources were barriers to implementing patient reported outcome measures. Policies that provide treatment systems with more resources to provide tailored trainings to their staff and to hire staff whose job is dedicated to patient-reported outcome measures may help address these clinical barriers to implementation.
Measurement-based practice is an evidence-based approach that involves ongoing assessment of treatment targets to guide clinical decisions, empower patients, and enhance health outcomes. The process of incorporating systematic outcome measures into treatment has been referred to as progress monitoring, outcome monitoring, measurement-based care, and the use of feedback systems.
Patient-reported outcome measures are a widely used method for administering assessments and providing feedback in alcohol and other drug treatment. In contrast, measurement-based care that does not rely on patient reports may include objective indicators, such as toxicology screens. However, adopting patient-reported outcome measures into regular care is a challenge for many substance use treatment centers.
Many efforts to implement evidence-based practices fail, despite carefully laid plans. Understanding the barriers and facilitators within a specific organization(s) can highlight future innovation tailoring, resource management, and staff trainings to successfully implement an innovation and see positive outcomes for individuals receiving services.
Understanding the barriers and facilitators of patient-reported outcome measures within substance use treatment may help improve patients’ outcomes. This study investigated the implementation of patient-reported outcome measures through interviews and surveys among substance use treatment counselors.
HOW WAS THIS STUDY CONDUCTED?
This study included interviews as well as quantitative surveys to apply the Consolidated Framework for Implementation Research to understand barriers and facilitators to implementing patient-reported outcome measures in substance use treatment. All data was collected from a large non-profit provider of inpatient and outpatient substance use treatment in Australia. The organization mainly provides counseling services and has collected patient-reported outcome measures electronically as standard practice since April 2020.
There were 23 counselors who participated; they were mostly female (78%), and the average age was 43 years old. The interviews featured questions designed to understand barriers and facilitators to the implementation of patient-reported outcome measures and feedback based on the Inner Setting and Individual Characteristic domains from the Consolidated Framework for Implementation Research (Figure below).
Each interview was recorded and then transcribed for analysis. The interviews ranged in length from 29 to 74 minutes, and they were conducted until no new themes were identified (i.e., “thematic saturation”). Then the qualitative analysis team iteratively developed a codebook based of the Framework, interview guide, and emergent themes found in the interviews. The team then met to discuss and arrive at a group of final themes.
There were 108 counselors who were part of the original rollout of the patient-reported outcome measure implementation that participated in the quantitative survey (out of a possible 141 counselors). The study team developed 4 survey measures: knowledge and beliefs regarding patient-reported outcome measures and feedback; patient-reported outcome measures and self-efficacy; leadership support for patient-reported outcome measures; and available resources for patient-reported outcome measures. The first comprised 10 questions asking how much participants agreed (on a scale from 1 [strongly disagree] to 7 [ strongly agree]) with statements about patient-reported outcome measures and feedback (e.g., “Outcome measures take into consideration the needs and preferences of clients”). The second included 7 items assessing how confident participants were with aspects of patient-reported outcome measures on a scale from 1 [not confident] to 5 [very confident] (e.g., “motivating clients to complete outcome measures”). The third featured 2 items that assess organizational leadership and direct supervisor support for patient-reported outcome measures on a scale from 1 [strongly disagree] to 7 [strongly agree]. The fourth asked participants on a scale from 1 [strongly disagree] to 7 [ strongly agree] their level of agreement with the availability of 6 resources to deliver patient-reported outcome measures and related feedback (e.g., equipment and materials). Analyses examined the relationship between leadership support and available resources with participant knowledge, beliefs, and self-efficacy, while accounting for participant demographics.
Participants of the survey were, on average, 41 years old and mostly female (79%). About half completed a Bachelors (53%), while 18% completed a master’s and 29% completed a Certificate or diploma. There were 71% who reported working in the substance use sector for 3 or more years, and 41% reported working at the treatment service for 3 or more years.
WHAT DID THIS STUDY FIND?
Most staff thought patient-reported outcome measures were valuable
There were 17 participants that focused on the benefits of patient-reported outcomes measures in several ways: 1) provide staff with a snapshot of a client’s situation; 2) help facilitate dialogue; 3) promote client self-reflection and insight; 4) allow for progress tracking.
“[Patient-reported outcome measures give] us a bit of a picture of how the client presents, where they’re at, sort of cuts through a little bit of rapport work.’
Staff resistance to patient-reported outcome measures hinders implementation
Many participants felt patient-reported outcomes offered little advantage and actually hindered their treatment, which lead them to resist implementation. In particular participants 1) believed the information collected from the measures was already collected through discussions with the client; 2) the measures were too rigid and did not align with their clinical style; 3) felt the measures were complex and time-consuming, which diverted time away from delivering treatment to the clients; 4) saw the patient-reported outcome measures at odds with their norms, values, and beliefs, particularly around the need for client-centered treatment.
“There’s an expectation that we’ll use a session to complete an outcome measure, which I think, while there’s some really valuable data, it easily takes up the best part of a session, because most people will talk through it. When considering we only have five or six sessions, basically a session is gone…”
Competing interests, logistical issues, and resource limitations hinder implementation
There were 14 staff that discussed competing interests and logistical issues related to the lack of time to implement patient-reported outcome measures during treatment. Participants expressed that the patient-reported outcome measures were an organizational expectation that did not always align with the client needs in the session. The organizational versus client expectations would, at times, be at odds, which limited staffs’ full engagement in the patient-reported outcome measure process. They also noted that the organization lacked the resources to facilitate smooth administration and reflection of the measures. Staff had to spend time organizing results and feedback, which further limited their availability.
“Well, often, you have an idea of what you’re going to do in the session, but [the client] might come to you in crisis, and the last thing they want to do is discuss outcome measure results. So it can be like—not even necessarily crisis, but that’s not on their agenda. They want to talk about their feelings. They want to talk about what’s happened. So, I haven’t really gotten into great practice of going through [outcome measure feedback] with them.”’
Staff perceived patient-reported outcomes measures to be a burden for clients and may disengage them from treatment
There were 16 participants who felt that patient-reported outcome measures may be a burden for clients due to their time requirement, complexity, and resource requirement (e.g., needing to have internet access). Staff also observed low client motivation, ambivalence, and even resistance to completing the measures, which leads directly to clients disengaging from treatment.
“I have had some [clients] that just don’t want to do [patient-reported outcome measures]. They just want to come in and talk to somebody … So, I probably had three that have refused the service due to the outcome measures.”
Staff perceptions of organizational factors was related to knowledge and beliefs, as well as self-efficacy to implement, patient-reported outcome measures
Survey results showed that higher perceived leadership support and available resources were associated with increased knowledge and beliefs about patient-reported outcome measures and feedback. These effects were medium in size. Age, gender, highest degree completed, and length of time working at the treatment service were not related to knowledge and beliefs. In contrast, only perception of available resources for patient-reported outcome measure implementation was connected to staff’s self-efficacy to implement the measures and their feedback. As perceived resources increased, so too did the self-efficacy to implement the measures; however, the effect was small in magnitude.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The use of regular assessment of clinical targets often improves patient outcomes and helps get patients with worsening symptoms back on track. However, the real-world implementation of patient-reported outcome measures and feedback in substance use treatment services has faced barriers. Findings from this mixed-method study suggest that although patient-reported outcome measures and related feedback provide benefits, several staff and organizational characteristics hinder the implementation of patient-reported outcome measures and feedback in substance use treatment. The findings underscore the importance of understanding where and for whom an innovation (i.e., intervention) is being implemented. In the treatment system in Australia that was part of this study, staff and organizational characteristics specifically were seen to hinder the implementation of patient-reported outcome measures, despite most study participants seeing their value.
The study found that improved support from leadership, effective training on patient-reported outcome measures, and the provision of adequate resources would likely improve patient-reported outcome measure implementation in this specific treatment system in Australia. While not mentioned in the study, if resources permit, hiring one or more staff members whose job is dedicated to patient-reported outcome measures may help address clinical/time barriers and ultimately improve implementation. There are other key domains that, if better understood and addressed, may improve uptake of patient reported outcome measures and thus patient outcomes. For example, state policies and reporting requirements (i.e., the outer setting) may impact the extent to which organizations and staff have the time and resources to implement patient-reported outcome measures. The methods by which patient-reported outcome measures are collected and reviewed are also likely to influence their impact. The use of enhanced technology to collect and analyze patient-reported outcome measures, for example, may lead to more successful implementation. Further research is needed to identify the barriers and facilitators of implementation and to tailor innovations that address challenges and leverage opportunities.
Caution should be taken when trying to generalize these findings to other treatment centers inside and outside of Australia. The treatment system in this study is likely to be qualitatively different from others, which would impact the implementation domains explored and their findings.
This study only explored client-facing staff perceptions, which may not be representative of client or other key stakeholder perceptions. The study also does not specify whether participants in the qualitative and quantitative parts of the study were representative of the wider staff population in the treatment.
There are no validated measures for the implementation indicators used in this study, which may limit the accuracy of the results in representing the intended concepts.
BOTTOM LINE
Going beyond “what works” to “what works where, why, by whom, and for whom” is a key step in improving outcomes in substance use treatment services. Results from this study highlighted that although many staff viewed patient-reported outcome measures as valuable to the treatment process, there were staff and organizational characteristics that hindered their implementation. Negative perceptions of patient-reported outcome measures, low relative priority, and lack of time and resources were some of the key barriers to implementation. At the same time, support from leadership, effective training on patient-reported outcome measures, and the provision of adequate resources may improve implementation.
For individuals and families seeking recovery: The researchers in this study identified facilitators and barriers to implementing patient-reported outcome measures in substance use treatment settings. They found that staff perceptions and organizational resources may hinder their implementation. When evaluating treatment programs, inquire whether patient progress is systematically and regularly assessed.
For treatment professionals and treatment systems: The researchers in this study found that staff and organizational characteristics could hinder the implementation of evidence-based patient-reported outcome measures. Specifically, negative staff views and a lack of available time and resources were barriers to implementation. Prior to implementing an evidence-based practice, it would be helpful to examine how the context of implementation may impact the success of that intervention. For example, if there is not enough time to provide client-driven discussions as well as patient-reported outcomes, then exploring how they might complete the measures prior to session may help. Similarly, a treatment system may benefit from providing tailored trainings to their staff on how and why an intervention may benefit patients, even if it is not part of their routine practice. If resources permit, hiring staff whose job is dedicated to patient-reported outcome measures may help address clinical barriers.
For scientists: The research findings suggested that patient-reported outcome measures were seen as potentially valuable; however, there were staff and organizational barriers to implementation. For example, negative views of the measures, competing interests, and a lack of resources are barriers to implementing measures and feedback. This implementation study focused specially on individual and inner setting indicators from the perception of client-facing treatment staff. Future work is needed to see how these specific domains and indicators are influential in other treatment and recovery spaces as well as how other domains (e.g., outer setting, innovation characteristics) impact patient outcomes.
For policy makers: Moving beyond what works to what works, why, for whom, and by whom will help improve treatment outcomes. This study showed that negative staff views and a lack of available time and resources were barriers to implementing patient reported outcome measures. Policies that provide treatment systems with more resources to provide tailored trainings to their staff and to hire staff whose job is dedicated to patient-reported outcome measures may help address these clinical barriers to implementation.