What is unclear is the degree to which patients with substance use disorders want to be involved in the treatment decision making process. Evidence suggests that some patients prefer to be provided with information about treatment options but prefer the actual decision making to come from the provider. Evidence also suggests, however, that other substance use disorder patients prefer to take a more active role in deciding what treatment options to pursue. Furthermore, it is unknown how discrepancy between a patient’s preferred communication style and that used by providers may impact the therapeutic relationship or treatment outcomes. To this end, the present study examined substance use disorder treatment patients’ preferences in clinical decision making and how they were associated with retention in care and substance use outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a single-group, prospective observational study. Participants were 214 patients seeking substance use treatment services from the outpatient service for addictions of the Hospital d’Hebron (Barcelona, Spain). Patients who met the eligibility criteria were invited to participate by trained psychiatrists and psychologists. Participant recruitment occurred from March 2019 – June 2021. Eligible participants were: 1) between 18 and 65 years of age; 2) met substance use disorder criteria according to DSM-5; 3) able to understand and fill out the research questionnaire (in the opinion of the physician); and 4) able to give informed consent. Both new patients and patients who already were under treatment at the center were included. Participants were excluded if they: 1) were intoxicated at the time of the interview, 2) had a decompensated psychiatric disorder (i.e., the patient had previously managed their mental health disorder but has since gotten worse), and 3) were not fluent in Spanish. Patients were assessed once at baseline then again after 6 and 12 months.
Variables for the present study were derived via self-report measures as well as medical records. Participants completed the Control Preference Scale– a self-report scale that evaluates patient’s preferences and perceptions about their involvement in the decision-making process. Options range from a completely active role (the patient makes the decision) to a completely passive one (the doctor decides without the participation of the patient), with a shared decision in the midpoint. Patients also completed the Shared Decision-Making Questionnaire, which measured patients’ perception of provider’s use of shared decision-making techniques. Participants also completed the Patient Activation Measure to assess their self-perceived knowledge, skills, confidence, and involvement in managing chronic disease. Only patients who had not discontinued treatment at both 6- and 12-month follow-ups completed these survey measures.
The dependent variables for this study were derived via objective and self-report measures. Retention in treatment was dichotomized (yes or no). Treatment was considered discontinued if a patient did not attend a scheduled appointment without prior justification or during the subsequent 30 days. Adherence to medication was assessed via the Simplified Medication Adherence Questionnaire. Patients were deemed non-adherent to their medication regimen if they reported missing more than 2 doses of medications in the past week, or more than 2 full days not taking prescribed medications in the past 3 months. Substance use was assessed via urine drug screening and alcohol breathalyzer. These tests were conducted twice weekly during the follow-up. Participants were considered to have relapsed if they had 3 consecutive positive urine tests. The study examined whether role alignment in treatment decision making (less than desired, matched, or more than desired) was associated with outcomes, controlling for other factors correlated with the outcome.
Participants in the sample were mostly male (66.4%) with a mean age of 44 years. Over half of the sample had less than a high school education (56.8%). Most of the sample was not employed (69.4%) and not married (59.4%). The most common substance for which participants sought treatment was alcohol (49.1%) followed by cocaine (28.5%) and opioids (7.9%). Most participants were diagnosed with dependence for alcohol (57.9%), or cocaine (45.8%) followed by opioids (13.1%).
WHAT DID THIS STUDY FIND?
Most patients had desired amount of control in their therapeutic relationship with providers
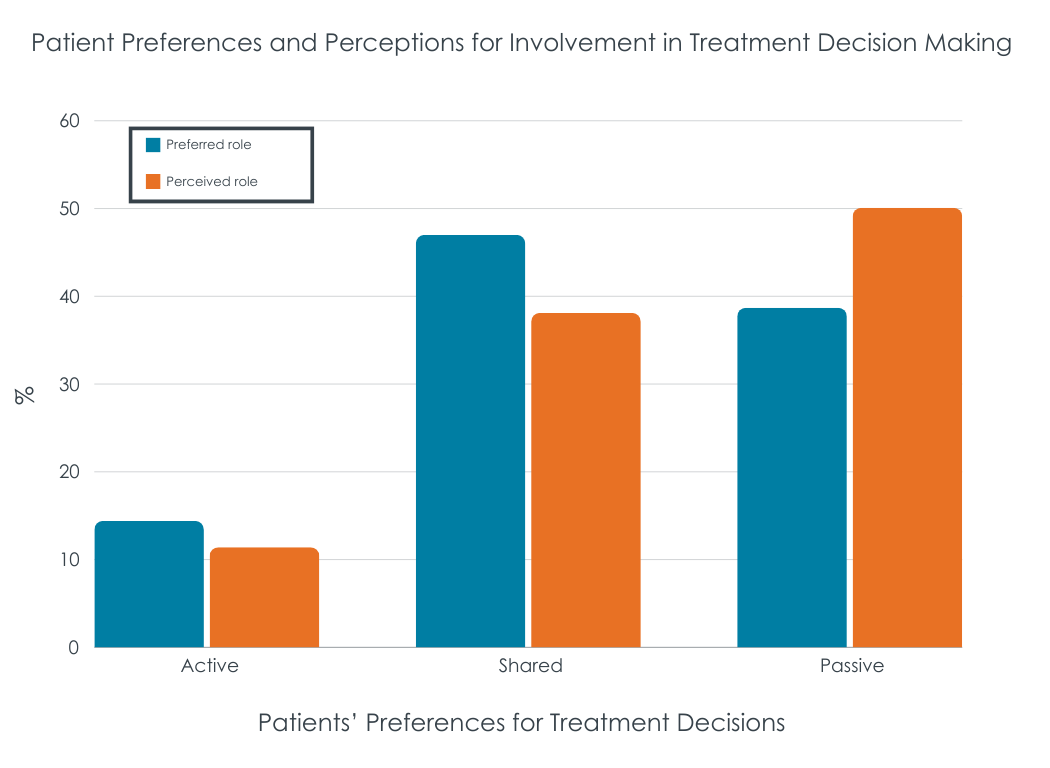
Most participants (66.5%) reported that the therapeutic relationship they had with their provider was in sync with their preferred role (e.g., shared decision-making). Many patients preferred to share decision making with their providers (46.9%) while 38.7% preferred their providers to make decisions regarding care. The remaining participants (14.4%) preferred to exclusively make decisions regarding their treatment.
Patients had worse outcomes if their involvement in treatment decisions was more than they wanted
Patients who reported more of their own personal involvement in their treatment decision making than they wanted – were more likely to test positive for substances at 6- and 12-month follow-ups. That is, patients that had a greater preference for providers to make decisions than was the actual case (i.e., providers were not as directive as they wanted), had worse outcomes than those where preference for involvement and actual involvement in decision making were aligned. However, the association between role alignment and outcomes – retention, medication adherence, and substance use – each became nonsignificant when other variables were included in the models.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that patients’ preferred level of involvement in clinical decision-making impacts substance use disorder treatment success. When patients are asked to be more involved in treatment than they would prefer, treatment was less successful.
The researchers found that most substance use disorder patients preferred a shared or passive role in the clinical decision-making process. They also found that one-third of patients had a mismatch between their preference for decision making and actual decision making – that is, they perceived more or less involvement in the clinical decision-making process than they would prefer. While these results could suggest that tailoring the clinical decision-making process in accordance with the desires of the patient may help facilitate substance use treatment efficacy., the association between role alignment and outcomes was not present in the model that included other clinical variables. This suggests that other factors, including baseline substance use and the presence of co-occurring psychiatric disorders may be explaining the association between role alignment and outcomes.
That said, there is a litany of research showing the therapist-patient working alliance – being on the same page with respect to treatment goals, approaches, etc. – predicts patient outcomes beyond many individual factors. It is plausible that role misalignment – where patients have more decision making power than desired – could result in worse treatment outcomes for them. Though in this study, the association between role misalignment and worse outcomes appeared to be explained potentially by additional patient factors.
Also, the results of this research may also suggest that substance use disorder patients may not benefit as much as other chronic illness patients from active decision-making in treatment. In this study a minority of patients endorsed wanting to actively make decisions regarding their treatment – most preferred to either share decision-making with their clinician or to defer to their physician entirely. Those who were asked to participate more actively in the treatment process, but did not want to, had higher relapse and attrition rates. In contrast, in other research, two-thirds of patients with other chronic psychiatric disorders preferred an active role in decision-making. It is unclear why substance use treatment patients may be more inclined to share or defer decision-making to their healthcare provider. These findings may suggest that providing an overabundance of autonomy to substance use disorder patents may be detrimental to treatment efficacy. This is odd, as it seems to contradict the very essence of popular patient-centered substance use interventions, such as Motivational Interviewing, which empowers patients to have decision-making autonomy. Of note, this study was conducted in Barcelona, Spain. Given differing cultures regarding interactions with medical providers and other authority figures, this study should be extended and replicated in other countries and cultures to help determine whether findings generalize beyond this study.
The present study utilized a convenience sample of treatment seeking adults from Spain, limiting our ability to make inferences about how decision-making style may impact treatment efficacy among patients in countries without universal healthcare (e.g., the US). The generalizability of these results is further limited as the study excluded patients with concurrent decompensated psychiatric disorder. That is, psychiatric comorbidity is common among substance use disorder patients.
The study analyzed patients without stratifying by the type of substance use used. This is relevant as evidence suggests that patients who use certain substances (e.g., heroin) may be more prone to relapse than others. As such, it is possible that the importance of the decision-making style in the therapeutic relationship between clinicians and patients may be of varying relevance for treatment success depending on what substances are being used by the patient. In addition, the authors did not consider how treatment success varied across different types of treatment (e.g., medications).
BOTTOM LINE
Preferences in decision making styles among substance use treatment seeking patients may impact treatment efficacy. The present study found that patients who reported being more active in treatment decision-making than they preferred were more likely to discontinue treatment and to relapse. However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. It could be, for example, that patients with more severe clinical profiles have higher levels of depression, and prefer a more directive approach. It could also be that severity is associated with a history of more treatment episodes, such that these patients prefer professional direction because their prior, more self-directed, approaches did not lead to sustained recovery. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For individuals and families seeking recovery: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For treatment professionals and treatment systems: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For scientists: Further research is needed to investigate how clinical decision-making may impact substance use treatment effectiveness. For example, it is important for future research to utilize non-convenience sampling and/or randomized clinical trial methodology to better understand how substance use patients may respond differently to treatment based on clinical decision-making strategies. For example, future research might randomly assign patients to different levels of decision making (i.e., active, shared, passive) in relation to their provider. . In addition, a better understanding of the psychological factors underlying patient engagement in care (e.g., motivation, self-efficacy, etc.) could elucidate how best to engage patients in clinical decision making.
For policy makers: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they may be explaining the worse outcomes rather than role misalignment, per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
What is unclear is the degree to which patients with substance use disorders want to be involved in the treatment decision making process. Evidence suggests that some patients prefer to be provided with information about treatment options but prefer the actual decision making to come from the provider. Evidence also suggests, however, that other substance use disorder patients prefer to take a more active role in deciding what treatment options to pursue. Furthermore, it is unknown how discrepancy between a patient’s preferred communication style and that used by providers may impact the therapeutic relationship or treatment outcomes. To this end, the present study examined substance use disorder treatment patients’ preferences in clinical decision making and how they were associated with retention in care and substance use outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a single-group, prospective observational study. Participants were 214 patients seeking substance use treatment services from the outpatient service for addictions of the Hospital d’Hebron (Barcelona, Spain). Patients who met the eligibility criteria were invited to participate by trained psychiatrists and psychologists. Participant recruitment occurred from March 2019 – June 2021. Eligible participants were: 1) between 18 and 65 years of age; 2) met substance use disorder criteria according to DSM-5; 3) able to understand and fill out the research questionnaire (in the opinion of the physician); and 4) able to give informed consent. Both new patients and patients who already were under treatment at the center were included. Participants were excluded if they: 1) were intoxicated at the time of the interview, 2) had a decompensated psychiatric disorder (i.e., the patient had previously managed their mental health disorder but has since gotten worse), and 3) were not fluent in Spanish. Patients were assessed once at baseline then again after 6 and 12 months.
Variables for the present study were derived via self-report measures as well as medical records. Participants completed the Control Preference Scale– a self-report scale that evaluates patient’s preferences and perceptions about their involvement in the decision-making process. Options range from a completely active role (the patient makes the decision) to a completely passive one (the doctor decides without the participation of the patient), with a shared decision in the midpoint. Patients also completed the Shared Decision-Making Questionnaire, which measured patients’ perception of provider’s use of shared decision-making techniques. Participants also completed the Patient Activation Measure to assess their self-perceived knowledge, skills, confidence, and involvement in managing chronic disease. Only patients who had not discontinued treatment at both 6- and 12-month follow-ups completed these survey measures.
The dependent variables for this study were derived via objective and self-report measures. Retention in treatment was dichotomized (yes or no). Treatment was considered discontinued if a patient did not attend a scheduled appointment without prior justification or during the subsequent 30 days. Adherence to medication was assessed via the Simplified Medication Adherence Questionnaire. Patients were deemed non-adherent to their medication regimen if they reported missing more than 2 doses of medications in the past week, or more than 2 full days not taking prescribed medications in the past 3 months. Substance use was assessed via urine drug screening and alcohol breathalyzer. These tests were conducted twice weekly during the follow-up. Participants were considered to have relapsed if they had 3 consecutive positive urine tests. The study examined whether role alignment in treatment decision making (less than desired, matched, or more than desired) was associated with outcomes, controlling for other factors correlated with the outcome.
Participants in the sample were mostly male (66.4%) with a mean age of 44 years. Over half of the sample had less than a high school education (56.8%). Most of the sample was not employed (69.4%) and not married (59.4%). The most common substance for which participants sought treatment was alcohol (49.1%) followed by cocaine (28.5%) and opioids (7.9%). Most participants were diagnosed with dependence for alcohol (57.9%), or cocaine (45.8%) followed by opioids (13.1%).
WHAT DID THIS STUDY FIND?
Most patients had desired amount of control in their therapeutic relationship with providers
Most participants (66.5%) reported that the therapeutic relationship they had with their provider was in sync with their preferred role (e.g., shared decision-making). Many patients preferred to share decision making with their providers (46.9%) while 38.7% preferred their providers to make decisions regarding care. The remaining participants (14.4%) preferred to exclusively make decisions regarding their treatment.
Patients had worse outcomes if their involvement in treatment decisions was more than they wanted
Patients who reported more of their own personal involvement in their treatment decision making than they wanted – were more likely to test positive for substances at 6- and 12-month follow-ups. That is, patients that had a greater preference for providers to make decisions than was the actual case (i.e., providers were not as directive as they wanted), had worse outcomes than those where preference for involvement and actual involvement in decision making were aligned. However, the association between role alignment and outcomes – retention, medication adherence, and substance use – each became nonsignificant when other variables were included in the models.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that patients’ preferred level of involvement in clinical decision-making impacts substance use disorder treatment success. When patients are asked to be more involved in treatment than they would prefer, treatment was less successful.
The researchers found that most substance use disorder patients preferred a shared or passive role in the clinical decision-making process. They also found that one-third of patients had a mismatch between their preference for decision making and actual decision making – that is, they perceived more or less involvement in the clinical decision-making process than they would prefer. While these results could suggest that tailoring the clinical decision-making process in accordance with the desires of the patient may help facilitate substance use treatment efficacy., the association between role alignment and outcomes was not present in the model that included other clinical variables. This suggests that other factors, including baseline substance use and the presence of co-occurring psychiatric disorders may be explaining the association between role alignment and outcomes.
That said, there is a litany of research showing the therapist-patient working alliance – being on the same page with respect to treatment goals, approaches, etc. – predicts patient outcomes beyond many individual factors. It is plausible that role misalignment – where patients have more decision making power than desired – could result in worse treatment outcomes for them. Though in this study, the association between role misalignment and worse outcomes appeared to be explained potentially by additional patient factors.
Also, the results of this research may also suggest that substance use disorder patients may not benefit as much as other chronic illness patients from active decision-making in treatment. In this study a minority of patients endorsed wanting to actively make decisions regarding their treatment – most preferred to either share decision-making with their clinician or to defer to their physician entirely. Those who were asked to participate more actively in the treatment process, but did not want to, had higher relapse and attrition rates. In contrast, in other research, two-thirds of patients with other chronic psychiatric disorders preferred an active role in decision-making. It is unclear why substance use treatment patients may be more inclined to share or defer decision-making to their healthcare provider. These findings may suggest that providing an overabundance of autonomy to substance use disorder patents may be detrimental to treatment efficacy. This is odd, as it seems to contradict the very essence of popular patient-centered substance use interventions, such as Motivational Interviewing, which empowers patients to have decision-making autonomy. Of note, this study was conducted in Barcelona, Spain. Given differing cultures regarding interactions with medical providers and other authority figures, this study should be extended and replicated in other countries and cultures to help determine whether findings generalize beyond this study.
The present study utilized a convenience sample of treatment seeking adults from Spain, limiting our ability to make inferences about how decision-making style may impact treatment efficacy among patients in countries without universal healthcare (e.g., the US). The generalizability of these results is further limited as the study excluded patients with concurrent decompensated psychiatric disorder. That is, psychiatric comorbidity is common among substance use disorder patients.
The study analyzed patients without stratifying by the type of substance use used. This is relevant as evidence suggests that patients who use certain substances (e.g., heroin) may be more prone to relapse than others. As such, it is possible that the importance of the decision-making style in the therapeutic relationship between clinicians and patients may be of varying relevance for treatment success depending on what substances are being used by the patient. In addition, the authors did not consider how treatment success varied across different types of treatment (e.g., medications).
BOTTOM LINE
Preferences in decision making styles among substance use treatment seeking patients may impact treatment efficacy. The present study found that patients who reported being more active in treatment decision-making than they preferred were more likely to discontinue treatment and to relapse. However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. It could be, for example, that patients with more severe clinical profiles have higher levels of depression, and prefer a more directive approach. It could also be that severity is associated with a history of more treatment episodes, such that these patients prefer professional direction because their prior, more self-directed, approaches did not lead to sustained recovery. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For individuals and families seeking recovery: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For treatment professionals and treatment systems: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For scientists: Further research is needed to investigate how clinical decision-making may impact substance use treatment effectiveness. For example, it is important for future research to utilize non-convenience sampling and/or randomized clinical trial methodology to better understand how substance use patients may respond differently to treatment based on clinical decision-making strategies. For example, future research might randomly assign patients to different levels of decision making (i.e., active, shared, passive) in relation to their provider. . In addition, a better understanding of the psychological factors underlying patient engagement in care (e.g., motivation, self-efficacy, etc.) could elucidate how best to engage patients in clinical decision making.
For policy makers: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they may be explaining the worse outcomes rather than role misalignment, per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
What is unclear is the degree to which patients with substance use disorders want to be involved in the treatment decision making process. Evidence suggests that some patients prefer to be provided with information about treatment options but prefer the actual decision making to come from the provider. Evidence also suggests, however, that other substance use disorder patients prefer to take a more active role in deciding what treatment options to pursue. Furthermore, it is unknown how discrepancy between a patient’s preferred communication style and that used by providers may impact the therapeutic relationship or treatment outcomes. To this end, the present study examined substance use disorder treatment patients’ preferences in clinical decision making and how they were associated with retention in care and substance use outcomes.
HOW WAS THIS STUDY CONDUCTED?
This study was a single-group, prospective observational study. Participants were 214 patients seeking substance use treatment services from the outpatient service for addictions of the Hospital d’Hebron (Barcelona, Spain). Patients who met the eligibility criteria were invited to participate by trained psychiatrists and psychologists. Participant recruitment occurred from March 2019 – June 2021. Eligible participants were: 1) between 18 and 65 years of age; 2) met substance use disorder criteria according to DSM-5; 3) able to understand and fill out the research questionnaire (in the opinion of the physician); and 4) able to give informed consent. Both new patients and patients who already were under treatment at the center were included. Participants were excluded if they: 1) were intoxicated at the time of the interview, 2) had a decompensated psychiatric disorder (i.e., the patient had previously managed their mental health disorder but has since gotten worse), and 3) were not fluent in Spanish. Patients were assessed once at baseline then again after 6 and 12 months.
Variables for the present study were derived via self-report measures as well as medical records. Participants completed the Control Preference Scale– a self-report scale that evaluates patient’s preferences and perceptions about their involvement in the decision-making process. Options range from a completely active role (the patient makes the decision) to a completely passive one (the doctor decides without the participation of the patient), with a shared decision in the midpoint. Patients also completed the Shared Decision-Making Questionnaire, which measured patients’ perception of provider’s use of shared decision-making techniques. Participants also completed the Patient Activation Measure to assess their self-perceived knowledge, skills, confidence, and involvement in managing chronic disease. Only patients who had not discontinued treatment at both 6- and 12-month follow-ups completed these survey measures.
The dependent variables for this study were derived via objective and self-report measures. Retention in treatment was dichotomized (yes or no). Treatment was considered discontinued if a patient did not attend a scheduled appointment without prior justification or during the subsequent 30 days. Adherence to medication was assessed via the Simplified Medication Adherence Questionnaire. Patients were deemed non-adherent to their medication regimen if they reported missing more than 2 doses of medications in the past week, or more than 2 full days not taking prescribed medications in the past 3 months. Substance use was assessed via urine drug screening and alcohol breathalyzer. These tests were conducted twice weekly during the follow-up. Participants were considered to have relapsed if they had 3 consecutive positive urine tests. The study examined whether role alignment in treatment decision making (less than desired, matched, or more than desired) was associated with outcomes, controlling for other factors correlated with the outcome.
Participants in the sample were mostly male (66.4%) with a mean age of 44 years. Over half of the sample had less than a high school education (56.8%). Most of the sample was not employed (69.4%) and not married (59.4%). The most common substance for which participants sought treatment was alcohol (49.1%) followed by cocaine (28.5%) and opioids (7.9%). Most participants were diagnosed with dependence for alcohol (57.9%), or cocaine (45.8%) followed by opioids (13.1%).
WHAT DID THIS STUDY FIND?
Most patients had desired amount of control in their therapeutic relationship with providers
Most participants (66.5%) reported that the therapeutic relationship they had with their provider was in sync with their preferred role (e.g., shared decision-making). Many patients preferred to share decision making with their providers (46.9%) while 38.7% preferred their providers to make decisions regarding care. The remaining participants (14.4%) preferred to exclusively make decisions regarding their treatment.
Patients had worse outcomes if their involvement in treatment decisions was more than they wanted
Patients who reported more of their own personal involvement in their treatment decision making than they wanted – were more likely to test positive for substances at 6- and 12-month follow-ups. That is, patients that had a greater preference for providers to make decisions than was the actual case (i.e., providers were not as directive as they wanted), had worse outcomes than those where preference for involvement and actual involvement in decision making were aligned. However, the association between role alignment and outcomes – retention, medication adherence, and substance use – each became nonsignificant when other variables were included in the models.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that patients’ preferred level of involvement in clinical decision-making impacts substance use disorder treatment success. When patients are asked to be more involved in treatment than they would prefer, treatment was less successful.
The researchers found that most substance use disorder patients preferred a shared or passive role in the clinical decision-making process. They also found that one-third of patients had a mismatch between their preference for decision making and actual decision making – that is, they perceived more or less involvement in the clinical decision-making process than they would prefer. While these results could suggest that tailoring the clinical decision-making process in accordance with the desires of the patient may help facilitate substance use treatment efficacy., the association between role alignment and outcomes was not present in the model that included other clinical variables. This suggests that other factors, including baseline substance use and the presence of co-occurring psychiatric disorders may be explaining the association between role alignment and outcomes.
That said, there is a litany of research showing the therapist-patient working alliance – being on the same page with respect to treatment goals, approaches, etc. – predicts patient outcomes beyond many individual factors. It is plausible that role misalignment – where patients have more decision making power than desired – could result in worse treatment outcomes for them. Though in this study, the association between role misalignment and worse outcomes appeared to be explained potentially by additional patient factors.
Also, the results of this research may also suggest that substance use disorder patients may not benefit as much as other chronic illness patients from active decision-making in treatment. In this study a minority of patients endorsed wanting to actively make decisions regarding their treatment – most preferred to either share decision-making with their clinician or to defer to their physician entirely. Those who were asked to participate more actively in the treatment process, but did not want to, had higher relapse and attrition rates. In contrast, in other research, two-thirds of patients with other chronic psychiatric disorders preferred an active role in decision-making. It is unclear why substance use treatment patients may be more inclined to share or defer decision-making to their healthcare provider. These findings may suggest that providing an overabundance of autonomy to substance use disorder patents may be detrimental to treatment efficacy. This is odd, as it seems to contradict the very essence of popular patient-centered substance use interventions, such as Motivational Interviewing, which empowers patients to have decision-making autonomy. Of note, this study was conducted in Barcelona, Spain. Given differing cultures regarding interactions with medical providers and other authority figures, this study should be extended and replicated in other countries and cultures to help determine whether findings generalize beyond this study.
The present study utilized a convenience sample of treatment seeking adults from Spain, limiting our ability to make inferences about how decision-making style may impact treatment efficacy among patients in countries without universal healthcare (e.g., the US). The generalizability of these results is further limited as the study excluded patients with concurrent decompensated psychiatric disorder. That is, psychiatric comorbidity is common among substance use disorder patients.
The study analyzed patients without stratifying by the type of substance use used. This is relevant as evidence suggests that patients who use certain substances (e.g., heroin) may be more prone to relapse than others. As such, it is possible that the importance of the decision-making style in the therapeutic relationship between clinicians and patients may be of varying relevance for treatment success depending on what substances are being used by the patient. In addition, the authors did not consider how treatment success varied across different types of treatment (e.g., medications).
BOTTOM LINE
Preferences in decision making styles among substance use treatment seeking patients may impact treatment efficacy. The present study found that patients who reported being more active in treatment decision-making than they preferred were more likely to discontinue treatment and to relapse. However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. It could be, for example, that patients with more severe clinical profiles have higher levels of depression, and prefer a more directive approach. It could also be that severity is associated with a history of more treatment episodes, such that these patients prefer professional direction because their prior, more self-directed, approaches did not lead to sustained recovery. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For individuals and families seeking recovery: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For treatment professionals and treatment systems: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they are explaining the worse outcomes rather than role misalignment per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.
For scientists: Further research is needed to investigate how clinical decision-making may impact substance use treatment effectiveness. For example, it is important for future research to utilize non-convenience sampling and/or randomized clinical trial methodology to better understand how substance use patients may respond differently to treatment based on clinical decision-making strategies. For example, future research might randomly assign patients to different levels of decision making (i.e., active, shared, passive) in relation to their provider. . In addition, a better understanding of the psychological factors underlying patient engagement in care (e.g., motivation, self-efficacy, etc.) could elucidate how best to engage patients in clinical decision making.
For policy makers: Patients who perceived they were more involved in making treatment decisions for substance use disorder than they preferred were more likely to miss treatment appointments and use substances again (relapse). However, these relationships became nonsignificant when other variables like baseline substance use and co-occurring psychiatric disorders were added to the models, suggesting they may be explaining the worse outcomes rather than role misalignment, per se. More research is needed to understand how preferred decision-making style effects patient outcomes before conclusions can be drawn.