Naltrexone initiated in the emergency department: Why it’s underused and what to do about it
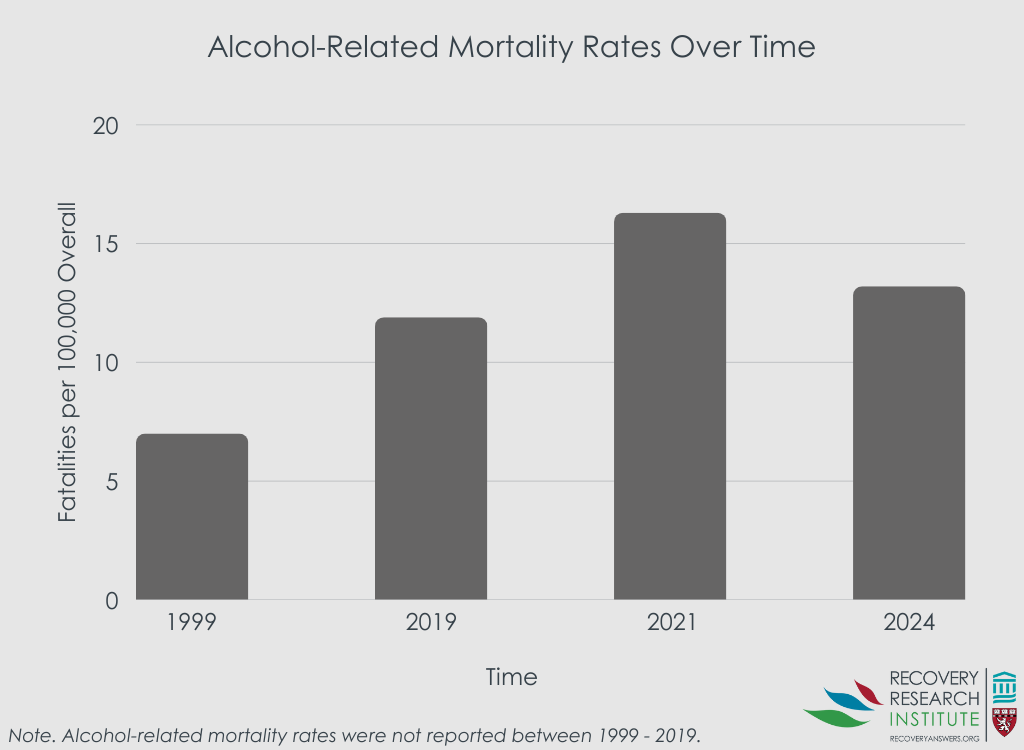
Emergency departments often care for individuals with alcohol use disorder, yet evidence-based medications like naltrexone are rarely initiated in this setting. This study examined real-world barriers faced by both clinicians and patients, and gathered feedback on strategies that could make prescribing naltrexone in the emergency department more routine.
This study used a 2-part design to examine barriers and facilitators to initiating naltrexone for alcohol use disorder in the emergency department. First, the researchers shadowed emergency department clinicians at multiple sites within a large northeastern healthcare system, observing workflows and conducting interviews with 3 physicians, 2 physician assistants, 4 nurses, a social worker, and 6 patients with alcohol use disorder. These observations and interviews were analyzed for key themes, which then informed the design of an online survey. The survey was distributed to all emergency medicine faculty and trainees across the healthcare system and was completed by 97 staff members (61% response rate). It asked about clinicians’ prior prescribing practices specifically for alcohol use disorder, their comfort level with treating alcohol use disorder, and perceived barriers to prescribing naltrexone (rated from 1 = “not at all a barrier” to 10 = “very significant barrier”). Respondents also rated the perceived helpfulness of different strategies for supporting emergency department-initiated naltrexone for patients with alcohol use disorder (from 1 = “not at all helpful” to 10 = “very helpful”).
WHAT DID THIS STUDY FIND?
Barriers to naltrexone initiation were widespread among both clinicians and patients
Clinicians in the emergency department reported several obstacles to prescribing naltrexone. Some noted inconsistent screening for alcohol use disorder due to the lack of a standardized protocol, meaning patients with alcohol use disorder often went unidentified. Even when identified, clinicians demonstrated limited knowledge about medications for alcohol use disorder. While most were familiar with naltrexone by name, they often confused it with other medications or misunderstood its purpose. Some expressed a lack of motivation to prescribe naltrexone, citing stigmatizing beliefs that patients rarely recover, which discouraged them from initiating treatment and led them to defer discussions to primary care or other providers. Patients also reported limited knowledge about naltrexone and sometimes confused it with other medications for alcohol use disorder, such as disulfiram, which works very differently and can cause unpleasant side effects when alcohol is consumed. Patients also described experiencing discomfort in the emergency department setting, difficulty navigating pharmacies, and limited follow-up resources, all of which posed barriers to initiating treatment.
Clinicians were comfortable identifying patients with alcohol use disorder, but not with prescribing naltrexone or answering questions about the medication
As shown in the graph below, survey responses highlighted that most physicians reported they felt comfortable identifying patients with alcohol use disorder (81%) and advising patients to cut down on their drinking (85%). Nearly 2/3 (62%) reported having prescribed benzodiazepines for alcohol withdrawal symptoms on discharge, yet only 3% reported prescribing naltrexone for alcohol use disorder. In contrast, most physicians expressed discomfort with prescribing naltrexone (91%), answering questions about the medication (87%), or arranging follow-up care (65%). When asked to rate barriers, clinicians identified all options – such as limited time, lack of patient knowledge, and lack of referral resources – as significant, with the lack of available follow-up treatment rated as the single most important barrier.
Streamlined prescribing processes and education were seen as the most valuable interventions
When asked about strategies to improve prescribing of naltrexone in emergency department patients, clinicians rated several system-level changes highly. The most valued interventions were creating a standardized pathway for naltrexone (a treatment protocol that outlines when and how to initiate the medication in the emergency department; 8.6 out of 10), adding naltrexone to standard discharge order sets for patents with mild-to-moderate alcohol withdrawal (8.6 out of 10), and employing substance use navigators in the emergency department to help patients engage in care (8.6). Other interventions were also perceived as valuable, including text message follow-up with navigators after discharge and educational efforts to increase knowledge about naltrexone (e.g., presentation on indications, dosing, and side effects of naltrexone; one-pager addressing common patient misconceptions about how naltrexone works).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Despite strong evidence that naltrexone is a helpful treatment for alcohol use disorder, its use in emergency department settings remains rare, underscoring a persistent gap between research and practice. Emergency departments are an important point of contact for individuals with alcohol use disorder and have long been recognized as an ideal setting for screening, brief interventions, and referrals to ongoing care. Yet, as findings from this study show, naltrexone prescribing in the emergency department is limited by barriers affecting both clinicians and patients. For clinicians, limited knowledge about naltrexone was a central barrier. Most physicians surveyed reported feeling uncomfortable prescribing naltrexone or answering patient questions about the medication, even though they routinely prescribed other medications such as benzodiazepines for alcohol withdrawal. For patients, barriers included limited awareness of medication options, confusion between naltrexone and other medications like disulfiram, discomfort in the emergency department setting, difficulty navigating pharmacies, and lack of follow-up resources. It is important to note, however, that naltrexone is typically prescribed as an extended-release injection formulation known by the brand name “Vivitrol”. Whether providers and patients would have different perceptions and/or reactions to this monthly injection of the medication is unclear.
Addressing these challenges will likely require system-level solutions. Clinicians themselves highlighted the value of streamlining the prescribing process, such as incorporating naltrexone into discharge order sets or standardized protocols, and enhancing education to reduce misunderstandings about the medication. Importantly, substance use treatment navigator support also emerged as a promising strategy. This aligns with a growing body of evidenceshowing that peer recovery support specialists can help connect patients to treatment,improve engagement and retention, and support recovery in real-world settings, including the emergency department. Expanding these roles, alongside low-barrier follow-up options and ongoing navigator support (e.g., via text messaging), may be especially critical in helping patients transition from an emergency department encounter into sustained care.
The qualitative portion of the study included a relatively small number of interviews with patients and healthcare staff, as well as a limited set of clinician observations during emergency department visits within a single northeastern health system. While this provided insights across different perspectives, the limited sample means the findings may not fully capture the range of experiences of patients or providers in other settings.
Because the online survey sample was drawn from a single healthcare system and relied on self-reports, the results may be influenced by selection and recall biases and have limited generalizability to other emergency department contexts.
Naltrexone is typically prescribed as an extended-release injection formulation known by the brand name “Vivitrol”. Whether providers and patients would have different perceptions and/or reactions to this monthly injection of the medication is unclear.
BOTTOM LINE
The underuse of medications like naltrexone in emergency department settings for patients with alcohol use disorder is a multifaceted issue shaped by barriers for both healthcare staff and patients. It underscores the need for greater education and more streamlined processes to increase access to and engagement with naltrexone. For clinicians, limited knowledge about naltrexone, discomfort with prescribing it, and lack of standardized workflows may be barriers to adoption. For patients, confusion about medications for alcohol use disorder, challenges navigating care, and limited follow-up resources make it harder to start and continue naltrexone. Promising strategies to increase naltrexone uptake include seamlessly integrating it into emergency department workflows and providing human patient navigation support. This support can come from substance use treatment navigators or peer recovery support specialists, who can guide patients, answer questions, and connect them to follow-up care. These approaches may increase engagement with evidence-based medications like naltrexone and, in turn, help reduce the burden of alcohol use disorder – both for individuals and for the healthcare system, where alcohol-related emergency department visits carry substantial costs.
For individuals and families seeking recovery: Emergency department visits can be a starting point for alcohol use disorder treatment. This study found that both patients and providers are sometimes unfamiliar with naltrexone or unsure about how it works, which means it may not always be discussed as an option. Asking about effective medications like naltrexone, along with follow-up care options, may help ensure these treatments are considered as part of a comprehensive recovery plan.
For treatment professionals and treatment systems: Clinicians in this study felt embedding naltrexone into streamlined discharge processes and standardized treatment pathways was among the most valuable ways to increase its use in the emergency department. Doing so can reduce uncertainty, save time, and ensure patients with alcohol use disorder are routinely offered this option. Findings from this study also indicated that patients commonly reported difficulties navigating care and accessing follow-up resources; substance use treatment navigators or peer recovery supports can help fill this gap by answering questions and connecting patients to ongoing treatment and recovery supports. Similarly, because both clinicians and patients reported limited knowledge about naltrexone, increasing education remains critical for improving understanding and uptake.
For scientists: More research is needed to test interventions that integrate naltrexone prescribing into emergency department workflows, to identify which approaches providers find most acceptable and which are most effective at increasing adoption. There is also a need to design and evaluate educational programs that build awareness and knowledge about naltrexone, including how it works, its efficacy for reducing heavy drinking and cravings, and its role in treatment. Such programs may help to ensure clinicians feel comfortable prescribing and discussing naltrexone, and that patients have the information needed to make informed decisions about their care.
For policy makers: Funding for treatment navigator and peer recovery support roles, along with clinician education, can expand access to medications for alcohol use disorder such as naltrexone. Ensuring that federal investments demonstrating the clinical efficacy of these medications translate into widespread adoption in practice could yield significant public health benefits. Broader use of naltrexone has the potential to reduce the burden of alcohol use disorder and the considerable societal costs tied to alcohol-related emergency department visits.
This study used a 2-part design to examine barriers and facilitators to initiating naltrexone for alcohol use disorder in the emergency department. First, the researchers shadowed emergency department clinicians at multiple sites within a large northeastern healthcare system, observing workflows and conducting interviews with 3 physicians, 2 physician assistants, 4 nurses, a social worker, and 6 patients with alcohol use disorder. These observations and interviews were analyzed for key themes, which then informed the design of an online survey. The survey was distributed to all emergency medicine faculty and trainees across the healthcare system and was completed by 97 staff members (61% response rate). It asked about clinicians’ prior prescribing practices specifically for alcohol use disorder, their comfort level with treating alcohol use disorder, and perceived barriers to prescribing naltrexone (rated from 1 = “not at all a barrier” to 10 = “very significant barrier”). Respondents also rated the perceived helpfulness of different strategies for supporting emergency department-initiated naltrexone for patients with alcohol use disorder (from 1 = “not at all helpful” to 10 = “very helpful”).
WHAT DID THIS STUDY FIND?
Barriers to naltrexone initiation were widespread among both clinicians and patients
Clinicians in the emergency department reported several obstacles to prescribing naltrexone. Some noted inconsistent screening for alcohol use disorder due to the lack of a standardized protocol, meaning patients with alcohol use disorder often went unidentified. Even when identified, clinicians demonstrated limited knowledge about medications for alcohol use disorder. While most were familiar with naltrexone by name, they often confused it with other medications or misunderstood its purpose. Some expressed a lack of motivation to prescribe naltrexone, citing stigmatizing beliefs that patients rarely recover, which discouraged them from initiating treatment and led them to defer discussions to primary care or other providers. Patients also reported limited knowledge about naltrexone and sometimes confused it with other medications for alcohol use disorder, such as disulfiram, which works very differently and can cause unpleasant side effects when alcohol is consumed. Patients also described experiencing discomfort in the emergency department setting, difficulty navigating pharmacies, and limited follow-up resources, all of which posed barriers to initiating treatment.
Clinicians were comfortable identifying patients with alcohol use disorder, but not with prescribing naltrexone or answering questions about the medication
As shown in the graph below, survey responses highlighted that most physicians reported they felt comfortable identifying patients with alcohol use disorder (81%) and advising patients to cut down on their drinking (85%). Nearly 2/3 (62%) reported having prescribed benzodiazepines for alcohol withdrawal symptoms on discharge, yet only 3% reported prescribing naltrexone for alcohol use disorder. In contrast, most physicians expressed discomfort with prescribing naltrexone (91%), answering questions about the medication (87%), or arranging follow-up care (65%). When asked to rate barriers, clinicians identified all options – such as limited time, lack of patient knowledge, and lack of referral resources – as significant, with the lack of available follow-up treatment rated as the single most important barrier.
Streamlined prescribing processes and education were seen as the most valuable interventions
When asked about strategies to improve prescribing of naltrexone in emergency department patients, clinicians rated several system-level changes highly. The most valued interventions were creating a standardized pathway for naltrexone (a treatment protocol that outlines when and how to initiate the medication in the emergency department; 8.6 out of 10), adding naltrexone to standard discharge order sets for patents with mild-to-moderate alcohol withdrawal (8.6 out of 10), and employing substance use navigators in the emergency department to help patients engage in care (8.6). Other interventions were also perceived as valuable, including text message follow-up with navigators after discharge and educational efforts to increase knowledge about naltrexone (e.g., presentation on indications, dosing, and side effects of naltrexone; one-pager addressing common patient misconceptions about how naltrexone works).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Despite strong evidence that naltrexone is a helpful treatment for alcohol use disorder, its use in emergency department settings remains rare, underscoring a persistent gap between research and practice. Emergency departments are an important point of contact for individuals with alcohol use disorder and have long been recognized as an ideal setting for screening, brief interventions, and referrals to ongoing care. Yet, as findings from this study show, naltrexone prescribing in the emergency department is limited by barriers affecting both clinicians and patients. For clinicians, limited knowledge about naltrexone was a central barrier. Most physicians surveyed reported feeling uncomfortable prescribing naltrexone or answering patient questions about the medication, even though they routinely prescribed other medications such as benzodiazepines for alcohol withdrawal. For patients, barriers included limited awareness of medication options, confusion between naltrexone and other medications like disulfiram, discomfort in the emergency department setting, difficulty navigating pharmacies, and lack of follow-up resources. It is important to note, however, that naltrexone is typically prescribed as an extended-release injection formulation known by the brand name “Vivitrol”. Whether providers and patients would have different perceptions and/or reactions to this monthly injection of the medication is unclear.
Addressing these challenges will likely require system-level solutions. Clinicians themselves highlighted the value of streamlining the prescribing process, such as incorporating naltrexone into discharge order sets or standardized protocols, and enhancing education to reduce misunderstandings about the medication. Importantly, substance use treatment navigator support also emerged as a promising strategy. This aligns with a growing body of evidenceshowing that peer recovery support specialists can help connect patients to treatment,improve engagement and retention, and support recovery in real-world settings, including the emergency department. Expanding these roles, alongside low-barrier follow-up options and ongoing navigator support (e.g., via text messaging), may be especially critical in helping patients transition from an emergency department encounter into sustained care.
The qualitative portion of the study included a relatively small number of interviews with patients and healthcare staff, as well as a limited set of clinician observations during emergency department visits within a single northeastern health system. While this provided insights across different perspectives, the limited sample means the findings may not fully capture the range of experiences of patients or providers in other settings.
Because the online survey sample was drawn from a single healthcare system and relied on self-reports, the results may be influenced by selection and recall biases and have limited generalizability to other emergency department contexts.
Naltrexone is typically prescribed as an extended-release injection formulation known by the brand name “Vivitrol”. Whether providers and patients would have different perceptions and/or reactions to this monthly injection of the medication is unclear.
BOTTOM LINE
The underuse of medications like naltrexone in emergency department settings for patients with alcohol use disorder is a multifaceted issue shaped by barriers for both healthcare staff and patients. It underscores the need for greater education and more streamlined processes to increase access to and engagement with naltrexone. For clinicians, limited knowledge about naltrexone, discomfort with prescribing it, and lack of standardized workflows may be barriers to adoption. For patients, confusion about medications for alcohol use disorder, challenges navigating care, and limited follow-up resources make it harder to start and continue naltrexone. Promising strategies to increase naltrexone uptake include seamlessly integrating it into emergency department workflows and providing human patient navigation support. This support can come from substance use treatment navigators or peer recovery support specialists, who can guide patients, answer questions, and connect them to follow-up care. These approaches may increase engagement with evidence-based medications like naltrexone and, in turn, help reduce the burden of alcohol use disorder – both for individuals and for the healthcare system, where alcohol-related emergency department visits carry substantial costs.
For individuals and families seeking recovery: Emergency department visits can be a starting point for alcohol use disorder treatment. This study found that both patients and providers are sometimes unfamiliar with naltrexone or unsure about how it works, which means it may not always be discussed as an option. Asking about effective medications like naltrexone, along with follow-up care options, may help ensure these treatments are considered as part of a comprehensive recovery plan.
For treatment professionals and treatment systems: Clinicians in this study felt embedding naltrexone into streamlined discharge processes and standardized treatment pathways was among the most valuable ways to increase its use in the emergency department. Doing so can reduce uncertainty, save time, and ensure patients with alcohol use disorder are routinely offered this option. Findings from this study also indicated that patients commonly reported difficulties navigating care and accessing follow-up resources; substance use treatment navigators or peer recovery supports can help fill this gap by answering questions and connecting patients to ongoing treatment and recovery supports. Similarly, because both clinicians and patients reported limited knowledge about naltrexone, increasing education remains critical for improving understanding and uptake.
For scientists: More research is needed to test interventions that integrate naltrexone prescribing into emergency department workflows, to identify which approaches providers find most acceptable and which are most effective at increasing adoption. There is also a need to design and evaluate educational programs that build awareness and knowledge about naltrexone, including how it works, its efficacy for reducing heavy drinking and cravings, and its role in treatment. Such programs may help to ensure clinicians feel comfortable prescribing and discussing naltrexone, and that patients have the information needed to make informed decisions about their care.
For policy makers: Funding for treatment navigator and peer recovery support roles, along with clinician education, can expand access to medications for alcohol use disorder such as naltrexone. Ensuring that federal investments demonstrating the clinical efficacy of these medications translate into widespread adoption in practice could yield significant public health benefits. Broader use of naltrexone has the potential to reduce the burden of alcohol use disorder and the considerable societal costs tied to alcohol-related emergency department visits.
This study used a 2-part design to examine barriers and facilitators to initiating naltrexone for alcohol use disorder in the emergency department. First, the researchers shadowed emergency department clinicians at multiple sites within a large northeastern healthcare system, observing workflows and conducting interviews with 3 physicians, 2 physician assistants, 4 nurses, a social worker, and 6 patients with alcohol use disorder. These observations and interviews were analyzed for key themes, which then informed the design of an online survey. The survey was distributed to all emergency medicine faculty and trainees across the healthcare system and was completed by 97 staff members (61% response rate). It asked about clinicians’ prior prescribing practices specifically for alcohol use disorder, their comfort level with treating alcohol use disorder, and perceived barriers to prescribing naltrexone (rated from 1 = “not at all a barrier” to 10 = “very significant barrier”). Respondents also rated the perceived helpfulness of different strategies for supporting emergency department-initiated naltrexone for patients with alcohol use disorder (from 1 = “not at all helpful” to 10 = “very helpful”).
WHAT DID THIS STUDY FIND?
Barriers to naltrexone initiation were widespread among both clinicians and patients
Clinicians in the emergency department reported several obstacles to prescribing naltrexone. Some noted inconsistent screening for alcohol use disorder due to the lack of a standardized protocol, meaning patients with alcohol use disorder often went unidentified. Even when identified, clinicians demonstrated limited knowledge about medications for alcohol use disorder. While most were familiar with naltrexone by name, they often confused it with other medications or misunderstood its purpose. Some expressed a lack of motivation to prescribe naltrexone, citing stigmatizing beliefs that patients rarely recover, which discouraged them from initiating treatment and led them to defer discussions to primary care or other providers. Patients also reported limited knowledge about naltrexone and sometimes confused it with other medications for alcohol use disorder, such as disulfiram, which works very differently and can cause unpleasant side effects when alcohol is consumed. Patients also described experiencing discomfort in the emergency department setting, difficulty navigating pharmacies, and limited follow-up resources, all of which posed barriers to initiating treatment.
Clinicians were comfortable identifying patients with alcohol use disorder, but not with prescribing naltrexone or answering questions about the medication
As shown in the graph below, survey responses highlighted that most physicians reported they felt comfortable identifying patients with alcohol use disorder (81%) and advising patients to cut down on their drinking (85%). Nearly 2/3 (62%) reported having prescribed benzodiazepines for alcohol withdrawal symptoms on discharge, yet only 3% reported prescribing naltrexone for alcohol use disorder. In contrast, most physicians expressed discomfort with prescribing naltrexone (91%), answering questions about the medication (87%), or arranging follow-up care (65%). When asked to rate barriers, clinicians identified all options – such as limited time, lack of patient knowledge, and lack of referral resources – as significant, with the lack of available follow-up treatment rated as the single most important barrier.
Streamlined prescribing processes and education were seen as the most valuable interventions
When asked about strategies to improve prescribing of naltrexone in emergency department patients, clinicians rated several system-level changes highly. The most valued interventions were creating a standardized pathway for naltrexone (a treatment protocol that outlines when and how to initiate the medication in the emergency department; 8.6 out of 10), adding naltrexone to standard discharge order sets for patents with mild-to-moderate alcohol withdrawal (8.6 out of 10), and employing substance use navigators in the emergency department to help patients engage in care (8.6). Other interventions were also perceived as valuable, including text message follow-up with navigators after discharge and educational efforts to increase knowledge about naltrexone (e.g., presentation on indications, dosing, and side effects of naltrexone; one-pager addressing common patient misconceptions about how naltrexone works).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Despite strong evidence that naltrexone is a helpful treatment for alcohol use disorder, its use in emergency department settings remains rare, underscoring a persistent gap between research and practice. Emergency departments are an important point of contact for individuals with alcohol use disorder and have long been recognized as an ideal setting for screening, brief interventions, and referrals to ongoing care. Yet, as findings from this study show, naltrexone prescribing in the emergency department is limited by barriers affecting both clinicians and patients. For clinicians, limited knowledge about naltrexone was a central barrier. Most physicians surveyed reported feeling uncomfortable prescribing naltrexone or answering patient questions about the medication, even though they routinely prescribed other medications such as benzodiazepines for alcohol withdrawal. For patients, barriers included limited awareness of medication options, confusion between naltrexone and other medications like disulfiram, discomfort in the emergency department setting, difficulty navigating pharmacies, and lack of follow-up resources. It is important to note, however, that naltrexone is typically prescribed as an extended-release injection formulation known by the brand name “Vivitrol”. Whether providers and patients would have different perceptions and/or reactions to this monthly injection of the medication is unclear.
Addressing these challenges will likely require system-level solutions. Clinicians themselves highlighted the value of streamlining the prescribing process, such as incorporating naltrexone into discharge order sets or standardized protocols, and enhancing education to reduce misunderstandings about the medication. Importantly, substance use treatment navigator support also emerged as a promising strategy. This aligns with a growing body of evidenceshowing that peer recovery support specialists can help connect patients to treatment,improve engagement and retention, and support recovery in real-world settings, including the emergency department. Expanding these roles, alongside low-barrier follow-up options and ongoing navigator support (e.g., via text messaging), may be especially critical in helping patients transition from an emergency department encounter into sustained care.
The qualitative portion of the study included a relatively small number of interviews with patients and healthcare staff, as well as a limited set of clinician observations during emergency department visits within a single northeastern health system. While this provided insights across different perspectives, the limited sample means the findings may not fully capture the range of experiences of patients or providers in other settings.
Because the online survey sample was drawn from a single healthcare system and relied on self-reports, the results may be influenced by selection and recall biases and have limited generalizability to other emergency department contexts.
Naltrexone is typically prescribed as an extended-release injection formulation known by the brand name “Vivitrol”. Whether providers and patients would have different perceptions and/or reactions to this monthly injection of the medication is unclear.
BOTTOM LINE
The underuse of medications like naltrexone in emergency department settings for patients with alcohol use disorder is a multifaceted issue shaped by barriers for both healthcare staff and patients. It underscores the need for greater education and more streamlined processes to increase access to and engagement with naltrexone. For clinicians, limited knowledge about naltrexone, discomfort with prescribing it, and lack of standardized workflows may be barriers to adoption. For patients, confusion about medications for alcohol use disorder, challenges navigating care, and limited follow-up resources make it harder to start and continue naltrexone. Promising strategies to increase naltrexone uptake include seamlessly integrating it into emergency department workflows and providing human patient navigation support. This support can come from substance use treatment navigators or peer recovery support specialists, who can guide patients, answer questions, and connect them to follow-up care. These approaches may increase engagement with evidence-based medications like naltrexone and, in turn, help reduce the burden of alcohol use disorder – both for individuals and for the healthcare system, where alcohol-related emergency department visits carry substantial costs.
For individuals and families seeking recovery: Emergency department visits can be a starting point for alcohol use disorder treatment. This study found that both patients and providers are sometimes unfamiliar with naltrexone or unsure about how it works, which means it may not always be discussed as an option. Asking about effective medications like naltrexone, along with follow-up care options, may help ensure these treatments are considered as part of a comprehensive recovery plan.
For treatment professionals and treatment systems: Clinicians in this study felt embedding naltrexone into streamlined discharge processes and standardized treatment pathways was among the most valuable ways to increase its use in the emergency department. Doing so can reduce uncertainty, save time, and ensure patients with alcohol use disorder are routinely offered this option. Findings from this study also indicated that patients commonly reported difficulties navigating care and accessing follow-up resources; substance use treatment navigators or peer recovery supports can help fill this gap by answering questions and connecting patients to ongoing treatment and recovery supports. Similarly, because both clinicians and patients reported limited knowledge about naltrexone, increasing education remains critical for improving understanding and uptake.
For scientists: More research is needed to test interventions that integrate naltrexone prescribing into emergency department workflows, to identify which approaches providers find most acceptable and which are most effective at increasing adoption. There is also a need to design and evaluate educational programs that build awareness and knowledge about naltrexone, including how it works, its efficacy for reducing heavy drinking and cravings, and its role in treatment. Such programs may help to ensure clinicians feel comfortable prescribing and discussing naltrexone, and that patients have the information needed to make informed decisions about their care.
For policy makers: Funding for treatment navigator and peer recovery support roles, along with clinician education, can expand access to medications for alcohol use disorder such as naltrexone. Ensuring that federal investments demonstrating the clinical efficacy of these medications translate into widespread adoption in practice could yield significant public health benefits. Broader use of naltrexone has the potential to reduce the burden of alcohol use disorder and the considerable societal costs tied to alcohol-related emergency department visits.