Black individuals’ attitudes toward opioid use disorder medications
Compared to White individuals, Black individuals are more likely to die from an opioid overdose and less likely to receive medication treatments for opioid use disorder. This study examined reasons that might underlie these disparities, by assessing medication treatment attitudes and experiences among Black people with a history of opioid use disorder.
Overdose death rates among Black individuals increased over 300% since 1999, surpassing death rates among White individuals in more recent years. Medication treatments for opioid use disorder (buprenorphine often prescribed as buprenorphine/naloxone known by the brand name “Suboxone”, methadone, naltrexone often prescribed in a monthly injection known by the brand name “Vivitrol”) are life-saving treatments that help to prevent opioid overdose and overdose deaths. Though policymakers have attempted to reduce barriers to medication treatment access (e.g., removing special training requirements and waivers to prescribe buprenorphine), rates of buprenorphine prescribing and uptake among patients with opioid use disorder are still lower than anticipated. This suggests the presence of multi-layered, ongoing barriers.
Research suggests potential disparities in medication treatment uptake by race – White Americans make up 75% of the population that qualifies for opioid use disorder medication treatment, but account for 90% of those who receive medication treatment. Research suggests several structural barriers accounting for these racial disparities, including physician bias and lack of available medication treatment in minority communities. Attitudinal barriers, such as patient preference for/against medication, are less well understood in the context of racial disparities.
Therefore, to improve overall rates of opioid use disorder medication use, it is essential to better understand the attitudes of Black individuals by revealing the reasons underlying lower uptake of medication treatment in Black communities and identifying whether there is an unmet need for medication and other treatment services within these communities. This study aimed to gain a better understanding of medication treatment attitudes, knowledge, and perceptions among Black people with lived experience of opioid use disorder in Minnesota.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of Black adult attitudes, knowledge, and perceptions toward opioid use disorder medication treatment (i.e. buprenorphine and methadone) in Minnesota.
Participants were recruited in partnership with African American Survivor Services, a recovery community organization that provides culturally sensitive navigation services for the Black community in Minnesota. Recruitment occurred at recovery programs, methadone clinics, temporary housing sites, and in the community. Eligible participants had a self-reported history of a past or current opioid use disorder, and had lived in Minneapolis or Saint Paul, Minnesota for at least 1 year at the time of enrollment.
Qualitative one-on-one semi-structured interviews were conducted with 28 participants between February and June of 2022. Interview questions concerned knowledge and experience with medication treatments (with emphasis on methadone and buprenorphine), facilitators and barriers to treatment, and the role of race and ethnicity in treatment barriers. Qualitative interviews were analyzed for relevant themes and coded. The research team also characterized participant’s overall attitude toward buprenorphine and methadone as “largely positive or neutral” or “largely negative”. Only individuals who were previously aware of these medication treatments were included in this analysis.
The majority of participants were men (68%), with an average age of 53 years. All participants had previously heard of methadone and nearly all had a lifetime history of taking methadone as prescribed in a clinical setting (96%). Regarding buprenorphine, 89% of participants were familiar with the medication and 75% had previously taken it (62% as prescribed, 38% non-prescription use). None of the participants had prior experience with naltrexone.
WHAT DID THIS STUDY FIND?
Most had negative attitudes toward medication treatment
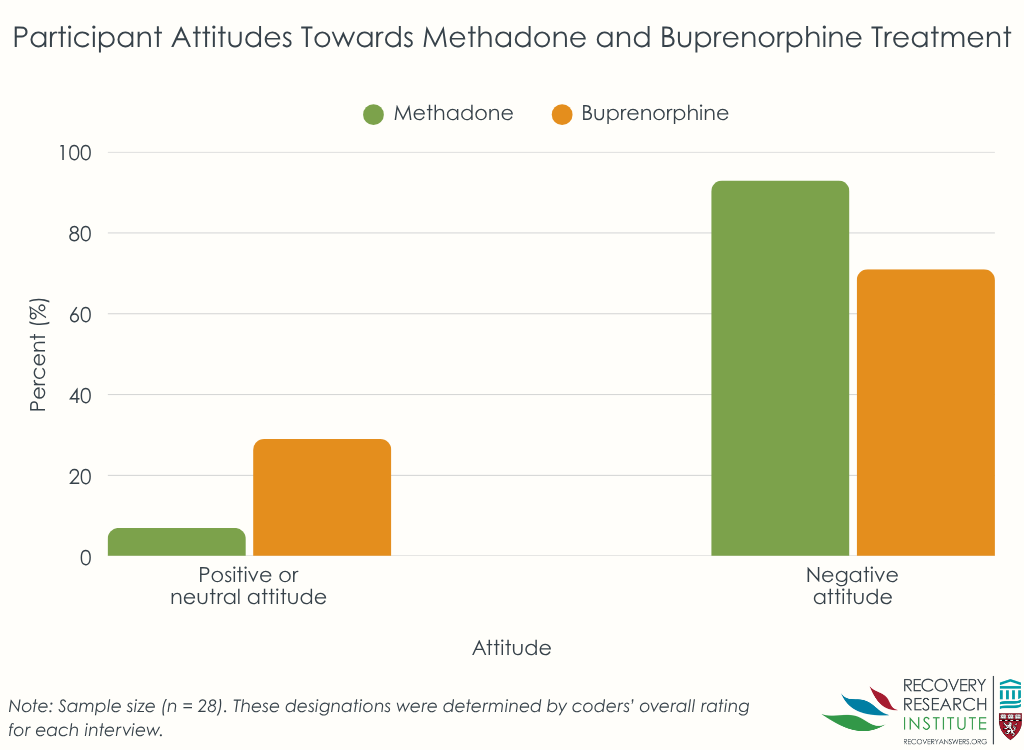
Few (7%) of the participants were categorized as having broadly positive or neutral attitudes toward methadone treatment (see Graph below) – most participants had negative attitudes (93%) toward methadone.
Twenty-nine percent of participants were categorized as having positive or neutral attitudes about buprenorphine treatment. The remaining participants (71%) had generally negative attitudes toward buprenorphine.
Buprenorphine was seen as less familiar and more complex than methadone
All participants were familiar with methadone, with most originally learning about it in social contexts or by seeing others use it within their community. Prior decisions to engage in methadone treatment or non-prescribed use were often described practically, with some saying they did it to save money, avoid withdrawal, or to stop using illicit drugs.
Though 90% of participants had previously heard of buprenorphine in some capacity, several described it as being a newer form of treatment that was less familiar, and even “confusing”. Participants noted the perceived complexity of buprenorphine initiation and maintenance, being uncertain about how you started it, how it worked pharmacologically, and what its purpose was clinically. This lack of familiarity and perceived complexity of buprenorphine was often noted as the reason that patients were reluctant to try it.
Negative past experiences with prescribed and non-prescribed buprenorphine were common
One-third of participants who had taken buprenorphine had prior experience with non-prescribed buprenorphine, (i.e. diverted or illegal buprenorphine often utilized as a short term aid for managing withdrawal symptoms from illicit opioids like heroin/fentanyl). In these cases, lack of clinical guidance often resulted in negative medication experiences because participants didn’t know how to properly initiate buprenorphine – many took it too soon after their last use of heroin/fentanyl, causing precipitated withdrawal.
Negative perceptions of buprenorphine were also common among those who received it under medical supervision. Over half of these participants (64%) noted they disliked buprenorphine or had an adverse event because of it. Participants noted pressure to initiate the medication in treatment settings, side effects that were acceptable/manageable to medical staff but unacceptable to the patient, and the perceived lack of treatment effectiveness for craving. Regardless of the context, negative buprenorphine experiences were almost always accompanied by an aversion to trying the medication again in the future.
Nearly all patients had negative past experiences and negative current perceptions of methadone
Of the participants who had a history of methadone treatment, most had negative perceptions of it. Many reported reduced quality of life, with reasons including the physiological need for the medication once stabilized on it, and the burdens of daily dosing at their methadone clinic. Stigma and other social/privacy concerns at their methadone clinic were also noted.
Negative experiences with methadone were often generalized to buprenorphine, with patients reluctant to try buprenorphine regardless of whether they had prior experience with it. Some noted that they had turned down buprenorphine treatment to remain on methadone treatment because they were unaware that buprenorphine could be prescribed in an office-based setting, which may have encouraged them to switch. Several individuals noted they were not yet ready for total abstinence and had chosen methadone over buprenorphine treatment because they assumed methadone’s full agonist properties might allow for greater psychoactive effects (e.g., a high from the medication), especially when large amounts of fentanyl were used on top of the methadone to displace methadone from receptors in the brain.
Participants had skepticism toward treatment industry motives and desired behavioral therapy as an alternative
Skepticism toward methadone treatment clinic motives was noted, particularly by individuals who had a history of methadone treatment, with many describing the idea of “liquid handcuffs”. Some individuals also thought psychosocial treatments were needed but less available than medication treatment, further driving skepticism toward the treatment industry and its financial motives. Despite the skepticism, fear of opioid overdose and related-death kept people retained in treatment or encouraged them to restart treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand the reasons underlying low rates of opioid use disorder medication treatment in populations that are at increased risk of opioid overdose, which can ultimately help guide population-specific initiatives that reduce overdose and related deaths. This particular study provides insight into the medication treatment attitudes and experiences of Black people with lived experience of opioid use disorder, a population that is less likely to engage in medication treatment.
Participants in this study had generally negative attitudes toward buprenorphine and methadone. Almost all participants had a history of methadone treatment and about three-fifths had experience with buprenorphine treatment – current negative attitudes toward these medications were largely driven by negative past experiences with them. This is important because the way in which medication treatment is delivered has implications for future treatment seeking and willingness, should individuals need additional treatment in the future.
Though the majority of the study sample had a history of buprenorphine treatment, about 25% of the sample had no experience with prescribed or non-prescribed buprenorphine, and some of these individuals noted a lack of knowledge about this medication. Given that the perceived novelty and complexity of buprenorphine was often noted as the reason why these individuals didn’t want to try it, there is a greater need for community education on buprenorphine treatment. Additional efforts may also be needed for those who decide to take the medication without a prescription, given that many individuals had negative experiences with the initiation of diverted/”street” buprenorphine taken without clinical guidance or supervision, and that this was a commonly cited reason for negative buprenorphine treatment attitudes. Educating the community about buprenorphine induction and the potential for precipitating withdrawal, and expanding low-barrier access to high quality buprenorphine treatment programs, may help reduce negative initiation experiences and, in turn, reduce negative perceptions of buprenorphine.
Findings also suggested that pressure to start buprenorphine treatment in clinical settings may facilitate negative perceptions of this medication and reluctance to try it in the future. Lack of adequate clinical management of medication side-effects during induction (e.g., prescribing adjunct clonidine) and craving during early treatment also resulted in negative opinions and may have perpetuated mistrust of treatment systems. Indeed, participants reported skepticism toward the motives of treatment programs – an expected finding in line with Black individuals’ greater medical mistrust than White individuals, on average. Offering high quality alternative and complementary treatment approaches (e.g., psychosocial treatments; faith-based treatments and services; adjunct medications to better address withdrawal) and linkages to community-based recovery support services as additional options for patients may help to establish trust between patients and providers and offer patients autonomy in their healthcare decisions.
Nearly all participants had methadone treatment experiences that resulted in negative perceptions of methadone. In addition, negative methadone experiences here were associated with negative perceptions of buprenorphine treatment, regardless of whether or not someone had a history of receiving it, emphasizing the generalized influence of medication treatment experiences on any future willingness to engage in treatment.
Finding ways to mitigate negative medication treatment experiences in clinical settings is necessary to avoid patient aversions to trying medication treatment again in the future, and to better address mistrust in healthcare systems and treatment programs. This is essential for both methadone and buprenorphine, as negative experiences with one can influence perceptions of the other.
Participants in this study didn’t have a diagnostically-confirmed opioid use disorder, as disorders were self reported.
In addition, the sample size was small (28), and recruitment occurred at recovery programs, methadone clinics, temporary housing sites, and in community settings within a single state, which may not reflect the attitudes and opinions of the broader population of Black individuals within that state or elsewhere. Generalizability to other racial groups is also unknown.
This study cohort consisted primarily of patients who had a history of opioid use disorder medication treatment and findings may not apply to those without medication treatment histories who are looking to start treatment for the first time.
BOTTOM LINE
Participants in this study had generally negative attitudes toward buprenorphine and methadone that stemmed from negative prior personal experiences with medication treatment. Negative experiences with buprenorphine included precipitated withdrawal without adequate clinical management of symptoms and perceived lack of buprenorphine’s effectiveness for treating craving. Negative methadone experiences included the need for daily dosing and clinic visits, stigma and privacy concerns. Mistrust of treatment programs and pressure from treatment systems to start medication were also noted as influencing medication treatment perceptions. Fear of overdose was a common factor that kept individuals engaged in treatment despite negative experiences, and negative experiences with one type of medication translated to negative perceptions of the other. Additional research is needed to identify best treatment practices that encourage positive experiences among Black populations to better engage them in opioid use disorder medication treatment and address high rates of overdose deaths.
For individuals and families seeking recovery: Medication treatment helps to prevent overdose death and can aid people in initiating and maintaining recovery from opioid use disorder. Given that someone’s first experience with medication treatment can influence their willingness to try these treatments in future, individuals and families seeking medication treatment are encouraged to find a treatment program that offers person-centered care and meets the needs of a person’s particular situation (limited transportation, ability to attend regular clinic visits, etc.) prior to starting medication treatment. Because many people have negative experiences with non-prescribed buprenorphine taken without clinical supervision, sending many people into withdrawal when it isn’t started correctly, individuals who are considering buprenorphine treatment are encouraged to seek out formal medical care to help avoid precipitated withdrawal and obtain adjunct medications that can help treat symptoms of withdrawal, should they occur.
For treatment professionals and treatment systems: Healthcare providers and systems are encouraged to educate their patients about medication treatments, including how they work and where they can be accessed/prescribed. Treatment providers are also encouraged to address programmatic barriers that may negatively affect patient’s treatment experiences, particularly within communities that have increased overdose risk, like Black communities. Since negative experiences with medication treatment can reduce a patient’s willingness to try the same, or an alternative, medication in the future, it is essential to provide patient-centered treatment that can help patients overcome personal and logistical concerns and barriers that help facilitate better patient experiences and outcomes in the long term. Given that not all patients will be willing to engage or re-engage with medication treatment and patients in this study did not like clinical pressure to take it, it may be essential to not pressure patients to take a medication and to also offer patients a variety of options for help seeking, including psychosocial treatments and recovery support services like mutual help groups.
For scientists: Additional qualitative and quantitative studies are needed in Black communities across different states, and within additional populations that have an increased risk of opioid overdose and related death. Research is needed to identify programmatic characteristics that promote positive treatment experiences to inform more effective standards and regulations across treatment systems. Randomized trials of novel interventions that enhance low-barrier access to medication treatment programs and that promote positive treatment experiences among populations at increased risk of overdose are needed to assess methods that enhance treatment experiences for Black patients and promote trust in medical systems.
For policy makers: Medication treatments for opioid use disorder are shown to be effective for reducing overdose deaths. These treatments may be able to address exceptionally high rates of opioid overdose deaths among Black individuals, but negative perceptions of medication treatment, driven by negative prior experiences with the treatment system, may deter such individuals from engaging in these lifesaving treatments. Funding for additional research will help reveal additional factors contributing to negative medication treatment attitudes and experiences, which can inform the development and testing of novel programmatic approaches to treatment that meet patient’s needs and promote positive treatment experiences. Doing so could prevent medical mistrust and aversion to future treatment seeking, to ultimately reduce overdose deaths within Black communities.
Overdose death rates among Black individuals increased over 300% since 1999, surpassing death rates among White individuals in more recent years. Medication treatments for opioid use disorder (buprenorphine often prescribed as buprenorphine/naloxone known by the brand name “Suboxone”, methadone, naltrexone often prescribed in a monthly injection known by the brand name “Vivitrol”) are life-saving treatments that help to prevent opioid overdose and overdose deaths. Though policymakers have attempted to reduce barriers to medication treatment access (e.g., removing special training requirements and waivers to prescribe buprenorphine), rates of buprenorphine prescribing and uptake among patients with opioid use disorder are still lower than anticipated. This suggests the presence of multi-layered, ongoing barriers.
Research suggests potential disparities in medication treatment uptake by race – White Americans make up 75% of the population that qualifies for opioid use disorder medication treatment, but account for 90% of those who receive medication treatment. Research suggests several structural barriers accounting for these racial disparities, including physician bias and lack of available medication treatment in minority communities. Attitudinal barriers, such as patient preference for/against medication, are less well understood in the context of racial disparities.
Therefore, to improve overall rates of opioid use disorder medication use, it is essential to better understand the attitudes of Black individuals by revealing the reasons underlying lower uptake of medication treatment in Black communities and identifying whether there is an unmet need for medication and other treatment services within these communities. This study aimed to gain a better understanding of medication treatment attitudes, knowledge, and perceptions among Black people with lived experience of opioid use disorder in Minnesota.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of Black adult attitudes, knowledge, and perceptions toward opioid use disorder medication treatment (i.e. buprenorphine and methadone) in Minnesota.
Participants were recruited in partnership with African American Survivor Services, a recovery community organization that provides culturally sensitive navigation services for the Black community in Minnesota. Recruitment occurred at recovery programs, methadone clinics, temporary housing sites, and in the community. Eligible participants had a self-reported history of a past or current opioid use disorder, and had lived in Minneapolis or Saint Paul, Minnesota for at least 1 year at the time of enrollment.
Qualitative one-on-one semi-structured interviews were conducted with 28 participants between February and June of 2022. Interview questions concerned knowledge and experience with medication treatments (with emphasis on methadone and buprenorphine), facilitators and barriers to treatment, and the role of race and ethnicity in treatment barriers. Qualitative interviews were analyzed for relevant themes and coded. The research team also characterized participant’s overall attitude toward buprenorphine and methadone as “largely positive or neutral” or “largely negative”. Only individuals who were previously aware of these medication treatments were included in this analysis.
The majority of participants were men (68%), with an average age of 53 years. All participants had previously heard of methadone and nearly all had a lifetime history of taking methadone as prescribed in a clinical setting (96%). Regarding buprenorphine, 89% of participants were familiar with the medication and 75% had previously taken it (62% as prescribed, 38% non-prescription use). None of the participants had prior experience with naltrexone.
WHAT DID THIS STUDY FIND?
Most had negative attitudes toward medication treatment
Few (7%) of the participants were categorized as having broadly positive or neutral attitudes toward methadone treatment (see Graph below) – most participants had negative attitudes (93%) toward methadone.
Twenty-nine percent of participants were categorized as having positive or neutral attitudes about buprenorphine treatment. The remaining participants (71%) had generally negative attitudes toward buprenorphine.
Buprenorphine was seen as less familiar and more complex than methadone
All participants were familiar with methadone, with most originally learning about it in social contexts or by seeing others use it within their community. Prior decisions to engage in methadone treatment or non-prescribed use were often described practically, with some saying they did it to save money, avoid withdrawal, or to stop using illicit drugs.
Though 90% of participants had previously heard of buprenorphine in some capacity, several described it as being a newer form of treatment that was less familiar, and even “confusing”. Participants noted the perceived complexity of buprenorphine initiation and maintenance, being uncertain about how you started it, how it worked pharmacologically, and what its purpose was clinically. This lack of familiarity and perceived complexity of buprenorphine was often noted as the reason that patients were reluctant to try it.
Negative past experiences with prescribed and non-prescribed buprenorphine were common
One-third of participants who had taken buprenorphine had prior experience with non-prescribed buprenorphine, (i.e. diverted or illegal buprenorphine often utilized as a short term aid for managing withdrawal symptoms from illicit opioids like heroin/fentanyl). In these cases, lack of clinical guidance often resulted in negative medication experiences because participants didn’t know how to properly initiate buprenorphine – many took it too soon after their last use of heroin/fentanyl, causing precipitated withdrawal.
Negative perceptions of buprenorphine were also common among those who received it under medical supervision. Over half of these participants (64%) noted they disliked buprenorphine or had an adverse event because of it. Participants noted pressure to initiate the medication in treatment settings, side effects that were acceptable/manageable to medical staff but unacceptable to the patient, and the perceived lack of treatment effectiveness for craving. Regardless of the context, negative buprenorphine experiences were almost always accompanied by an aversion to trying the medication again in the future.
Nearly all patients had negative past experiences and negative current perceptions of methadone
Of the participants who had a history of methadone treatment, most had negative perceptions of it. Many reported reduced quality of life, with reasons including the physiological need for the medication once stabilized on it, and the burdens of daily dosing at their methadone clinic. Stigma and other social/privacy concerns at their methadone clinic were also noted.
Negative experiences with methadone were often generalized to buprenorphine, with patients reluctant to try buprenorphine regardless of whether they had prior experience with it. Some noted that they had turned down buprenorphine treatment to remain on methadone treatment because they were unaware that buprenorphine could be prescribed in an office-based setting, which may have encouraged them to switch. Several individuals noted they were not yet ready for total abstinence and had chosen methadone over buprenorphine treatment because they assumed methadone’s full agonist properties might allow for greater psychoactive effects (e.g., a high from the medication), especially when large amounts of fentanyl were used on top of the methadone to displace methadone from receptors in the brain.
Participants had skepticism toward treatment industry motives and desired behavioral therapy as an alternative
Skepticism toward methadone treatment clinic motives was noted, particularly by individuals who had a history of methadone treatment, with many describing the idea of “liquid handcuffs”. Some individuals also thought psychosocial treatments were needed but less available than medication treatment, further driving skepticism toward the treatment industry and its financial motives. Despite the skepticism, fear of opioid overdose and related-death kept people retained in treatment or encouraged them to restart treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand the reasons underlying low rates of opioid use disorder medication treatment in populations that are at increased risk of opioid overdose, which can ultimately help guide population-specific initiatives that reduce overdose and related deaths. This particular study provides insight into the medication treatment attitudes and experiences of Black people with lived experience of opioid use disorder, a population that is less likely to engage in medication treatment.
Participants in this study had generally negative attitudes toward buprenorphine and methadone. Almost all participants had a history of methadone treatment and about three-fifths had experience with buprenorphine treatment – current negative attitudes toward these medications were largely driven by negative past experiences with them. This is important because the way in which medication treatment is delivered has implications for future treatment seeking and willingness, should individuals need additional treatment in the future.
Though the majority of the study sample had a history of buprenorphine treatment, about 25% of the sample had no experience with prescribed or non-prescribed buprenorphine, and some of these individuals noted a lack of knowledge about this medication. Given that the perceived novelty and complexity of buprenorphine was often noted as the reason why these individuals didn’t want to try it, there is a greater need for community education on buprenorphine treatment. Additional efforts may also be needed for those who decide to take the medication without a prescription, given that many individuals had negative experiences with the initiation of diverted/”street” buprenorphine taken without clinical guidance or supervision, and that this was a commonly cited reason for negative buprenorphine treatment attitudes. Educating the community about buprenorphine induction and the potential for precipitating withdrawal, and expanding low-barrier access to high quality buprenorphine treatment programs, may help reduce negative initiation experiences and, in turn, reduce negative perceptions of buprenorphine.
Findings also suggested that pressure to start buprenorphine treatment in clinical settings may facilitate negative perceptions of this medication and reluctance to try it in the future. Lack of adequate clinical management of medication side-effects during induction (e.g., prescribing adjunct clonidine) and craving during early treatment also resulted in negative opinions and may have perpetuated mistrust of treatment systems. Indeed, participants reported skepticism toward the motives of treatment programs – an expected finding in line with Black individuals’ greater medical mistrust than White individuals, on average. Offering high quality alternative and complementary treatment approaches (e.g., psychosocial treatments; faith-based treatments and services; adjunct medications to better address withdrawal) and linkages to community-based recovery support services as additional options for patients may help to establish trust between patients and providers and offer patients autonomy in their healthcare decisions.
Nearly all participants had methadone treatment experiences that resulted in negative perceptions of methadone. In addition, negative methadone experiences here were associated with negative perceptions of buprenorphine treatment, regardless of whether or not someone had a history of receiving it, emphasizing the generalized influence of medication treatment experiences on any future willingness to engage in treatment.
Finding ways to mitigate negative medication treatment experiences in clinical settings is necessary to avoid patient aversions to trying medication treatment again in the future, and to better address mistrust in healthcare systems and treatment programs. This is essential for both methadone and buprenorphine, as negative experiences with one can influence perceptions of the other.
Participants in this study didn’t have a diagnostically-confirmed opioid use disorder, as disorders were self reported.
In addition, the sample size was small (28), and recruitment occurred at recovery programs, methadone clinics, temporary housing sites, and in community settings within a single state, which may not reflect the attitudes and opinions of the broader population of Black individuals within that state or elsewhere. Generalizability to other racial groups is also unknown.
This study cohort consisted primarily of patients who had a history of opioid use disorder medication treatment and findings may not apply to those without medication treatment histories who are looking to start treatment for the first time.
BOTTOM LINE
Participants in this study had generally negative attitudes toward buprenorphine and methadone that stemmed from negative prior personal experiences with medication treatment. Negative experiences with buprenorphine included precipitated withdrawal without adequate clinical management of symptoms and perceived lack of buprenorphine’s effectiveness for treating craving. Negative methadone experiences included the need for daily dosing and clinic visits, stigma and privacy concerns. Mistrust of treatment programs and pressure from treatment systems to start medication were also noted as influencing medication treatment perceptions. Fear of overdose was a common factor that kept individuals engaged in treatment despite negative experiences, and negative experiences with one type of medication translated to negative perceptions of the other. Additional research is needed to identify best treatment practices that encourage positive experiences among Black populations to better engage them in opioid use disorder medication treatment and address high rates of overdose deaths.
For individuals and families seeking recovery: Medication treatment helps to prevent overdose death and can aid people in initiating and maintaining recovery from opioid use disorder. Given that someone’s first experience with medication treatment can influence their willingness to try these treatments in future, individuals and families seeking medication treatment are encouraged to find a treatment program that offers person-centered care and meets the needs of a person’s particular situation (limited transportation, ability to attend regular clinic visits, etc.) prior to starting medication treatment. Because many people have negative experiences with non-prescribed buprenorphine taken without clinical supervision, sending many people into withdrawal when it isn’t started correctly, individuals who are considering buprenorphine treatment are encouraged to seek out formal medical care to help avoid precipitated withdrawal and obtain adjunct medications that can help treat symptoms of withdrawal, should they occur.
For treatment professionals and treatment systems: Healthcare providers and systems are encouraged to educate their patients about medication treatments, including how they work and where they can be accessed/prescribed. Treatment providers are also encouraged to address programmatic barriers that may negatively affect patient’s treatment experiences, particularly within communities that have increased overdose risk, like Black communities. Since negative experiences with medication treatment can reduce a patient’s willingness to try the same, or an alternative, medication in the future, it is essential to provide patient-centered treatment that can help patients overcome personal and logistical concerns and barriers that help facilitate better patient experiences and outcomes in the long term. Given that not all patients will be willing to engage or re-engage with medication treatment and patients in this study did not like clinical pressure to take it, it may be essential to not pressure patients to take a medication and to also offer patients a variety of options for help seeking, including psychosocial treatments and recovery support services like mutual help groups.
For scientists: Additional qualitative and quantitative studies are needed in Black communities across different states, and within additional populations that have an increased risk of opioid overdose and related death. Research is needed to identify programmatic characteristics that promote positive treatment experiences to inform more effective standards and regulations across treatment systems. Randomized trials of novel interventions that enhance low-barrier access to medication treatment programs and that promote positive treatment experiences among populations at increased risk of overdose are needed to assess methods that enhance treatment experiences for Black patients and promote trust in medical systems.
For policy makers: Medication treatments for opioid use disorder are shown to be effective for reducing overdose deaths. These treatments may be able to address exceptionally high rates of opioid overdose deaths among Black individuals, but negative perceptions of medication treatment, driven by negative prior experiences with the treatment system, may deter such individuals from engaging in these lifesaving treatments. Funding for additional research will help reveal additional factors contributing to negative medication treatment attitudes and experiences, which can inform the development and testing of novel programmatic approaches to treatment that meet patient’s needs and promote positive treatment experiences. Doing so could prevent medical mistrust and aversion to future treatment seeking, to ultimately reduce overdose deaths within Black communities.
Overdose death rates among Black individuals increased over 300% since 1999, surpassing death rates among White individuals in more recent years. Medication treatments for opioid use disorder (buprenorphine often prescribed as buprenorphine/naloxone known by the brand name “Suboxone”, methadone, naltrexone often prescribed in a monthly injection known by the brand name “Vivitrol”) are life-saving treatments that help to prevent opioid overdose and overdose deaths. Though policymakers have attempted to reduce barriers to medication treatment access (e.g., removing special training requirements and waivers to prescribe buprenorphine), rates of buprenorphine prescribing and uptake among patients with opioid use disorder are still lower than anticipated. This suggests the presence of multi-layered, ongoing barriers.
Research suggests potential disparities in medication treatment uptake by race – White Americans make up 75% of the population that qualifies for opioid use disorder medication treatment, but account for 90% of those who receive medication treatment. Research suggests several structural barriers accounting for these racial disparities, including physician bias and lack of available medication treatment in minority communities. Attitudinal barriers, such as patient preference for/against medication, are less well understood in the context of racial disparities.
Therefore, to improve overall rates of opioid use disorder medication use, it is essential to better understand the attitudes of Black individuals by revealing the reasons underlying lower uptake of medication treatment in Black communities and identifying whether there is an unmet need for medication and other treatment services within these communities. This study aimed to gain a better understanding of medication treatment attitudes, knowledge, and perceptions among Black people with lived experience of opioid use disorder in Minnesota.
HOW WAS THIS STUDY CONDUCTED?
This study was a qualitative investigation of Black adult attitudes, knowledge, and perceptions toward opioid use disorder medication treatment (i.e. buprenorphine and methadone) in Minnesota.
Participants were recruited in partnership with African American Survivor Services, a recovery community organization that provides culturally sensitive navigation services for the Black community in Minnesota. Recruitment occurred at recovery programs, methadone clinics, temporary housing sites, and in the community. Eligible participants had a self-reported history of a past or current opioid use disorder, and had lived in Minneapolis or Saint Paul, Minnesota for at least 1 year at the time of enrollment.
Qualitative one-on-one semi-structured interviews were conducted with 28 participants between February and June of 2022. Interview questions concerned knowledge and experience with medication treatments (with emphasis on methadone and buprenorphine), facilitators and barriers to treatment, and the role of race and ethnicity in treatment barriers. Qualitative interviews were analyzed for relevant themes and coded. The research team also characterized participant’s overall attitude toward buprenorphine and methadone as “largely positive or neutral” or “largely negative”. Only individuals who were previously aware of these medication treatments were included in this analysis.
The majority of participants were men (68%), with an average age of 53 years. All participants had previously heard of methadone and nearly all had a lifetime history of taking methadone as prescribed in a clinical setting (96%). Regarding buprenorphine, 89% of participants were familiar with the medication and 75% had previously taken it (62% as prescribed, 38% non-prescription use). None of the participants had prior experience with naltrexone.
WHAT DID THIS STUDY FIND?
Most had negative attitudes toward medication treatment
Few (7%) of the participants were categorized as having broadly positive or neutral attitudes toward methadone treatment (see Graph below) – most participants had negative attitudes (93%) toward methadone.
Twenty-nine percent of participants were categorized as having positive or neutral attitudes about buprenorphine treatment. The remaining participants (71%) had generally negative attitudes toward buprenorphine.
Buprenorphine was seen as less familiar and more complex than methadone
All participants were familiar with methadone, with most originally learning about it in social contexts or by seeing others use it within their community. Prior decisions to engage in methadone treatment or non-prescribed use were often described practically, with some saying they did it to save money, avoid withdrawal, or to stop using illicit drugs.
Though 90% of participants had previously heard of buprenorphine in some capacity, several described it as being a newer form of treatment that was less familiar, and even “confusing”. Participants noted the perceived complexity of buprenorphine initiation and maintenance, being uncertain about how you started it, how it worked pharmacologically, and what its purpose was clinically. This lack of familiarity and perceived complexity of buprenorphine was often noted as the reason that patients were reluctant to try it.
Negative past experiences with prescribed and non-prescribed buprenorphine were common
One-third of participants who had taken buprenorphine had prior experience with non-prescribed buprenorphine, (i.e. diverted or illegal buprenorphine often utilized as a short term aid for managing withdrawal symptoms from illicit opioids like heroin/fentanyl). In these cases, lack of clinical guidance often resulted in negative medication experiences because participants didn’t know how to properly initiate buprenorphine – many took it too soon after their last use of heroin/fentanyl, causing precipitated withdrawal.
Negative perceptions of buprenorphine were also common among those who received it under medical supervision. Over half of these participants (64%) noted they disliked buprenorphine or had an adverse event because of it. Participants noted pressure to initiate the medication in treatment settings, side effects that were acceptable/manageable to medical staff but unacceptable to the patient, and the perceived lack of treatment effectiveness for craving. Regardless of the context, negative buprenorphine experiences were almost always accompanied by an aversion to trying the medication again in the future.
Nearly all patients had negative past experiences and negative current perceptions of methadone
Of the participants who had a history of methadone treatment, most had negative perceptions of it. Many reported reduced quality of life, with reasons including the physiological need for the medication once stabilized on it, and the burdens of daily dosing at their methadone clinic. Stigma and other social/privacy concerns at their methadone clinic were also noted.
Negative experiences with methadone were often generalized to buprenorphine, with patients reluctant to try buprenorphine regardless of whether they had prior experience with it. Some noted that they had turned down buprenorphine treatment to remain on methadone treatment because they were unaware that buprenorphine could be prescribed in an office-based setting, which may have encouraged them to switch. Several individuals noted they were not yet ready for total abstinence and had chosen methadone over buprenorphine treatment because they assumed methadone’s full agonist properties might allow for greater psychoactive effects (e.g., a high from the medication), especially when large amounts of fentanyl were used on top of the methadone to displace methadone from receptors in the brain.
Participants had skepticism toward treatment industry motives and desired behavioral therapy as an alternative
Skepticism toward methadone treatment clinic motives was noted, particularly by individuals who had a history of methadone treatment, with many describing the idea of “liquid handcuffs”. Some individuals also thought psychosocial treatments were needed but less available than medication treatment, further driving skepticism toward the treatment industry and its financial motives. Despite the skepticism, fear of opioid overdose and related-death kept people retained in treatment or encouraged them to restart treatment.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Studies like this help us better understand the reasons underlying low rates of opioid use disorder medication treatment in populations that are at increased risk of opioid overdose, which can ultimately help guide population-specific initiatives that reduce overdose and related deaths. This particular study provides insight into the medication treatment attitudes and experiences of Black people with lived experience of opioid use disorder, a population that is less likely to engage in medication treatment.
Participants in this study had generally negative attitudes toward buprenorphine and methadone. Almost all participants had a history of methadone treatment and about three-fifths had experience with buprenorphine treatment – current negative attitudes toward these medications were largely driven by negative past experiences with them. This is important because the way in which medication treatment is delivered has implications for future treatment seeking and willingness, should individuals need additional treatment in the future.
Though the majority of the study sample had a history of buprenorphine treatment, about 25% of the sample had no experience with prescribed or non-prescribed buprenorphine, and some of these individuals noted a lack of knowledge about this medication. Given that the perceived novelty and complexity of buprenorphine was often noted as the reason why these individuals didn’t want to try it, there is a greater need for community education on buprenorphine treatment. Additional efforts may also be needed for those who decide to take the medication without a prescription, given that many individuals had negative experiences with the initiation of diverted/”street” buprenorphine taken without clinical guidance or supervision, and that this was a commonly cited reason for negative buprenorphine treatment attitudes. Educating the community about buprenorphine induction and the potential for precipitating withdrawal, and expanding low-barrier access to high quality buprenorphine treatment programs, may help reduce negative initiation experiences and, in turn, reduce negative perceptions of buprenorphine.
Findings also suggested that pressure to start buprenorphine treatment in clinical settings may facilitate negative perceptions of this medication and reluctance to try it in the future. Lack of adequate clinical management of medication side-effects during induction (e.g., prescribing adjunct clonidine) and craving during early treatment also resulted in negative opinions and may have perpetuated mistrust of treatment systems. Indeed, participants reported skepticism toward the motives of treatment programs – an expected finding in line with Black individuals’ greater medical mistrust than White individuals, on average. Offering high quality alternative and complementary treatment approaches (e.g., psychosocial treatments; faith-based treatments and services; adjunct medications to better address withdrawal) and linkages to community-based recovery support services as additional options for patients may help to establish trust between patients and providers and offer patients autonomy in their healthcare decisions.
Nearly all participants had methadone treatment experiences that resulted in negative perceptions of methadone. In addition, negative methadone experiences here were associated with negative perceptions of buprenorphine treatment, regardless of whether or not someone had a history of receiving it, emphasizing the generalized influence of medication treatment experiences on any future willingness to engage in treatment.
Finding ways to mitigate negative medication treatment experiences in clinical settings is necessary to avoid patient aversions to trying medication treatment again in the future, and to better address mistrust in healthcare systems and treatment programs. This is essential for both methadone and buprenorphine, as negative experiences with one can influence perceptions of the other.
Participants in this study didn’t have a diagnostically-confirmed opioid use disorder, as disorders were self reported.
In addition, the sample size was small (28), and recruitment occurred at recovery programs, methadone clinics, temporary housing sites, and in community settings within a single state, which may not reflect the attitudes and opinions of the broader population of Black individuals within that state or elsewhere. Generalizability to other racial groups is also unknown.
This study cohort consisted primarily of patients who had a history of opioid use disorder medication treatment and findings may not apply to those without medication treatment histories who are looking to start treatment for the first time.
BOTTOM LINE
Participants in this study had generally negative attitudes toward buprenorphine and methadone that stemmed from negative prior personal experiences with medication treatment. Negative experiences with buprenorphine included precipitated withdrawal without adequate clinical management of symptoms and perceived lack of buprenorphine’s effectiveness for treating craving. Negative methadone experiences included the need for daily dosing and clinic visits, stigma and privacy concerns. Mistrust of treatment programs and pressure from treatment systems to start medication were also noted as influencing medication treatment perceptions. Fear of overdose was a common factor that kept individuals engaged in treatment despite negative experiences, and negative experiences with one type of medication translated to negative perceptions of the other. Additional research is needed to identify best treatment practices that encourage positive experiences among Black populations to better engage them in opioid use disorder medication treatment and address high rates of overdose deaths.
For individuals and families seeking recovery: Medication treatment helps to prevent overdose death and can aid people in initiating and maintaining recovery from opioid use disorder. Given that someone’s first experience with medication treatment can influence their willingness to try these treatments in future, individuals and families seeking medication treatment are encouraged to find a treatment program that offers person-centered care and meets the needs of a person’s particular situation (limited transportation, ability to attend regular clinic visits, etc.) prior to starting medication treatment. Because many people have negative experiences with non-prescribed buprenorphine taken without clinical supervision, sending many people into withdrawal when it isn’t started correctly, individuals who are considering buprenorphine treatment are encouraged to seek out formal medical care to help avoid precipitated withdrawal and obtain adjunct medications that can help treat symptoms of withdrawal, should they occur.
For treatment professionals and treatment systems: Healthcare providers and systems are encouraged to educate their patients about medication treatments, including how they work and where they can be accessed/prescribed. Treatment providers are also encouraged to address programmatic barriers that may negatively affect patient’s treatment experiences, particularly within communities that have increased overdose risk, like Black communities. Since negative experiences with medication treatment can reduce a patient’s willingness to try the same, or an alternative, medication in the future, it is essential to provide patient-centered treatment that can help patients overcome personal and logistical concerns and barriers that help facilitate better patient experiences and outcomes in the long term. Given that not all patients will be willing to engage or re-engage with medication treatment and patients in this study did not like clinical pressure to take it, it may be essential to not pressure patients to take a medication and to also offer patients a variety of options for help seeking, including psychosocial treatments and recovery support services like mutual help groups.
For scientists: Additional qualitative and quantitative studies are needed in Black communities across different states, and within additional populations that have an increased risk of opioid overdose and related death. Research is needed to identify programmatic characteristics that promote positive treatment experiences to inform more effective standards and regulations across treatment systems. Randomized trials of novel interventions that enhance low-barrier access to medication treatment programs and that promote positive treatment experiences among populations at increased risk of overdose are needed to assess methods that enhance treatment experiences for Black patients and promote trust in medical systems.
For policy makers: Medication treatments for opioid use disorder are shown to be effective for reducing overdose deaths. These treatments may be able to address exceptionally high rates of opioid overdose deaths among Black individuals, but negative perceptions of medication treatment, driven by negative prior experiences with the treatment system, may deter such individuals from engaging in these lifesaving treatments. Funding for additional research will help reveal additional factors contributing to negative medication treatment attitudes and experiences, which can inform the development and testing of novel programmatic approaches to treatment that meet patient’s needs and promote positive treatment experiences. Doing so could prevent medical mistrust and aversion to future treatment seeking, to ultimately reduce overdose deaths within Black communities.