WHAT PROBLEM DOES THIS STUDY ADDRESS?
In 2016, California passed a policy to legalize cannabis for adults, with implementation of legal sales beginning in 2018. It is unclear how these policy changes have affected alcohol use. One possibility is that people have started using cannabis in place of alcohol, which could result in reduced alcohol use. Alternatively, people may use cannabis to enhance the effects of alcohol or to reduce inhibitions making alcohol use more likely, which could result in increased alcohol use. Given the high rates of mortality and health consequences from alcohol use, and that co-use of alcohol and cannabis is associated with heavier drinking, it is important to understand these effects to be able to inform prevention and intervention efforts. This study examined whether cannabis policy changes were associated with changes in alcohol use among primary care patients in California.
HOW WAS THIS STUDY CONDUCTED?
Researchers used electronic health records from primary care patients in California to examine associations between cannabis policy changes and patterns of alcohol use among adults between 2015 and 2019. This timeframe captured the 2 key cannabis policy changes: legalization of cannabis for adults in 2016 and the beginning of legal sales in 2018. Patients were screened for alcohol use with 3 questions asking about their quantity and frequency of alcohol use. Their data was included in the study if the screen was positive, as indicated by 4 measures of unhealthy alcohol use following guidelines set by the National Institute of Health, which were the primary outcomes of interest: aggregated monthly rates of patients exceeding (1) daily limits (4+/5+ for women/men), (2) weekly limits (8+/15+ for women/men), (3) both daily and weekly limits, and (4) frequent heavy episodic drinking (5+ days exceeding daily limits). Importantly, because patients were screened during a primary care appointment, they may be under-reporting their actual alcohol use to avoid intervention or potential judgment.
Monthly changes in alcohol use were examined among all patients and then were stratified by age groups: 21-34, 35-49, 50-64, and 65 or older, which allowed the researchers to examine differences by age groups. While the main analyses were interested in those aged 21 or older, given the legal drinking age in the US, exploratory analyses tested associations among those 18-20 years old. Statistical analyses tested whether there were both immediate and gradual changes in monthly alcohol use as a result of cannabis policy changes. Analyses controlled for potential confounders (e.g., differences in the patient case-mix) but did not report the specific variables. Cannabis policy changes included adult cannabis legalization and implementation of legal sales, which were analyzed separately. A total of 3,525,493 patients who were 21 years old or older were screened, and of these, approximately 1.5 million screened positive (varied slightly by year) across the 4 outcomes and were included in the analyses.
Of note, because this research design is correlational and not experimental, the researchers cannot examine if the associations between cannabis policy changes and alcohol use are causal. This research design also does not allow the researchers to examine what mechanisms may be responsible for any potential associations between cannabis policy changes and alcohol use. Notably, we cannot know, if there are reductions in alcohol use, why this was the case. The implication from the study design is that people were using cannabis to substitute for alcohol (reducing overall harms), however this study does not address that directly because cannabis use wasn’t measured. Future research would be needed to understand the underlying mechanisms.
WHAT DID THIS STUDY FIND?
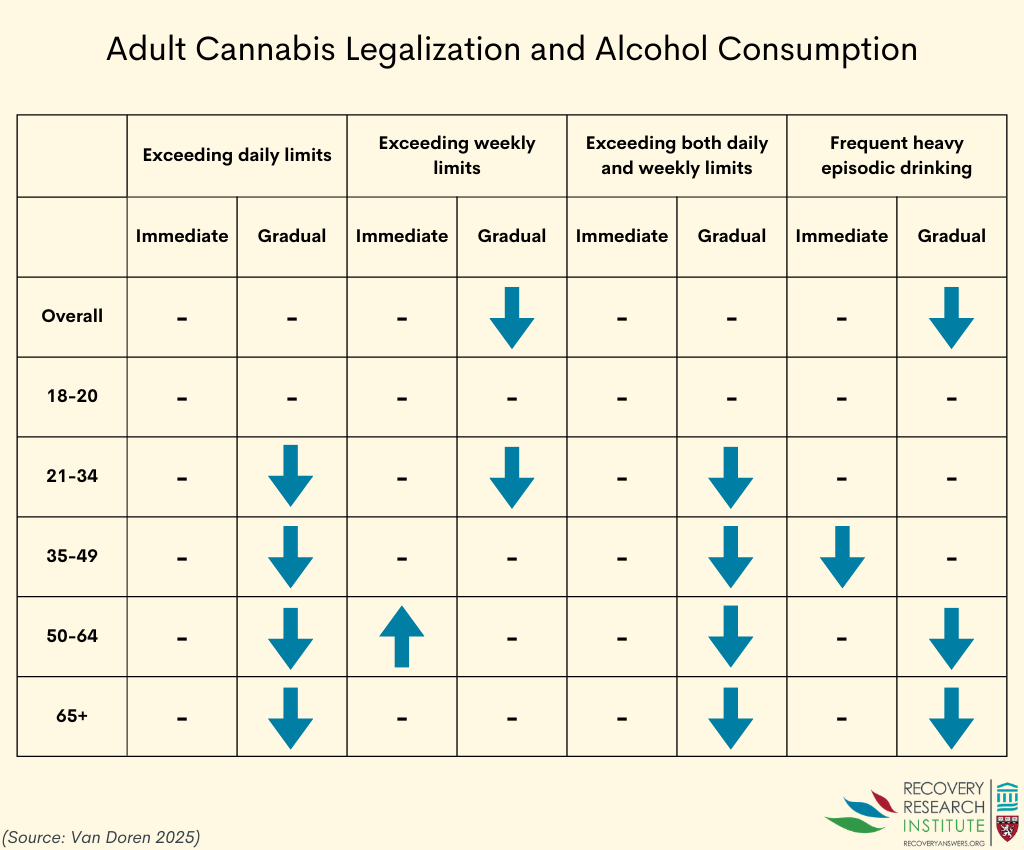
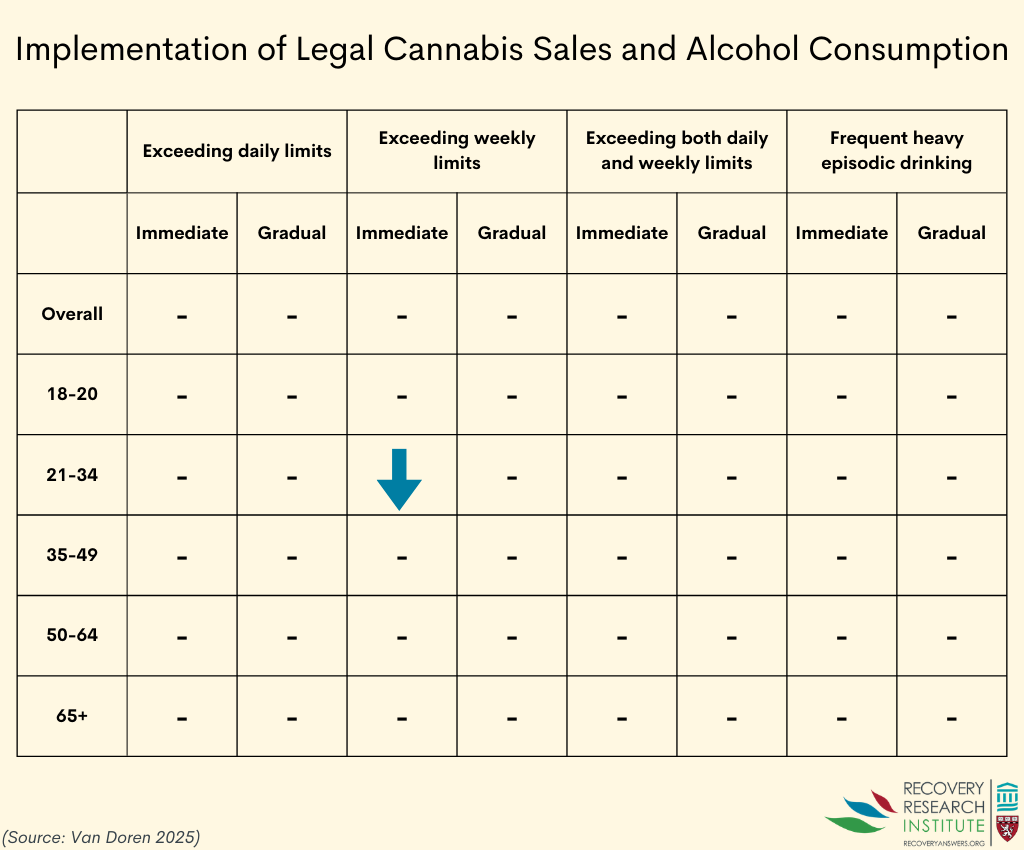
Adult cannabis legalization was associated with gradual reductions in the rates of people overall who reported exceeding weekly alcohol limits and rates of people reporting frequent heavy episodic drinking (see first graphic at the bottom of this section). Implementation of legal sales was not associated with any changes in alcohol use (see second graphic at the bottom of this section), suggesting that the reductions after legalization were maintained after the law was implemented. Reductions were very small – about .015% reduction per month.
Associations between cannabis policy changes and alcohol use varied by age, however. For people between the ages of 21-34, adult cannabis legalization was associated with gradual reductions in the rates of people exceeding daily limits, weekly limits, and both daily and weekly limits. Implementation of legal sales was also associated with an immediate decrease in the monthly rates of people who reported exceeding weekly limits.
For people between the ages of 35-49, adult cannabis legalization was associated with an immediate reduction in rates of frequent heavy episodic drinking. There were also gradual reductions in rates of people reporting exceeding daily limits and both daily and weekly limits. Implementation of legal sales was not associated with any changes in alcohol use among people in this age group.
For people between the ages of 50-64, adult cannabis legalization was associated with an immediate increase in rates of those who reported exceeding weekly limits. There were, however, gradual reductions in rates of those who reported exceeding daily limits, both daily and weekly limits, and frequent heavy episodic drinking. Implementation of legal sales was not associated with any changes in alcohol use in this age group.
Finally, for people 65 years old and older, adult cannabis legalization was associated with gradual reductions in rates of those who reported exceeding daily limits, exceeding both daily and weekly limits, and frequent heavy episodic drinking. Implementation of legal sales was not associated with any changes in alcohol use in this age group.
In the exploratory analyses testing associations between cannabis policy changes and alcohol use among those 18-20 years old, no associations were found (i.e., cannabis policy changes were not associated with either immediate or gradual changes in alcohol use).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that the 2016 legalization of cannabis for adults was associated with reductions in alcohol use among patients aged 21 years or older attending a primary care visit in California. While alcohol use changes varied slightly across age groups and by outcome, the overall pattern of results generally showed gradual reductions in alcohol use over time following cannabis legalization. The study did not, however, generally show any changes in alcohol use following the implementation of legal sales that began in 2018, suggesting that the reductions initially shown were sustained but not enhanced. The reductions were very small, but even small reductions across millions of people can have a meaningful impact from a public health perspective. The implication here is that changes in cannabis policy increased access to cannabis (e.g., through shifting attitudes given recreational cannabis was no longer illegal) which then led to decreased alcohol use (i.e., a substitution effect). However, it is possible that in California more generally, or in primary care practice around the same time, there was greater emphasis on reducing alcohol consumption for health reasons, given it is a group I carcinogen – known to increase the risk of several cancers. That said, the small decreases in alcohol use could indeed have resulted from individuals using cannabis to replace some of the alcohol they would normally consume. For instance, adults may have sought stress relief from cannabis rather than alcohol following legalization. More detailed studies are needed to understand cause and effect and whether use of cannabis actually results more directly in reduced consumption of alcohol.
Notably, this study assessed alcohol use among primary care patients who were not treatment-seeking and used an observational design. Not only does this prevent the researchers from being able to claim that the observed reductions in alcohol use were caused by cannabis legalization, but, given the primary care setting, patients may have under-reported their actual alcohol use. That said, if alcohol use was underreported, this would be the case both before and after the new cannabis laws, and the general trend would still hold up. Further, such reductions may not generalize to people with alcohol use disorder and those who are seeking treatment. However, a prior study among people who drank heavily and were in treatment showed that cannabis use was associated reduced alcohol use. Similarly, a laboratory study showed cannabis use results in decreased drinking among individuals with histories of frequent cannabis use and hazardous alcohol use. Still, future studies are needed to more fully understand the impact of cannabis legalization on alcohol use. Additional research is also needed to understand the impact of co-use of cannabis and alcohol, especially given that co-use has been found to be associated with heavier drinking.
BOTTOM LINE
Adult legalization of cannabis was associated with reductions in alcohol use among primary care patients in California. While alcohol use changes varied slightly across age groups and by outcome, the overall pattern of results generally showed gradual reductions in alcohol use over time following cannabis legalization. It is unclear whether cannabis use played a causal role in reducing heavier alcohol consumption or whether some other factor (e.g., greater emphasis on alcohol’s cancer-causing effects) in primary care around that time may be responsible for reductions in alcohol consumption.
- For individuals and families seeking recovery: Cannabis policy changes may reduce alcohol use patterns in the general adult population. However, replacing alcohol with cannabis does not necessarily reduce harm and improve well-being. Individuals may benefit from being mindful of unintended impacts of cannabis use, including co-use, and learning stress management techniques that do not rely on substances.
- For treatment professionals and treatment systems: These findings highlight the importance of screening for both alcohol and cannabis use in routine care, as legalization may shift substance use patterns. Treatment systems may also need to anticipate increases in cannabis use and adapt counseling approaches accordingly.
- For scientists: This study used a rigorous quasi-experimental design to examine the effects of cannabis legalization on harmful drinking in the general population. Studies that examine impacts among people with alcohol use disorder and explore the health consequences of substitution versus co-use are needed to comprehensively understand the impacts of cannabis legalization. It is unclear whether cannabis use played a causal role in reducing heavier alcohol consumption or whether some other factor (e.g., greater emphasis on alcohol’s cancer-causing effects) in primary care around that time may be responsible for reductions in alcohol consumption.
- For policy makers: Policies that monitor co-use trends of alcohol and cannabis are needed to keep tracking how cannabis legalization impacts alcohol use. Pairing cannabis legalization with public health messaging could mitigate problematic cannabis use and help the public understand potential risks.
CITATIONS
Van Doren, N., Chi, F. W., Young‐Wolff, K. C., Satre, D. D., & Sterling, S. A. (2025). Are cannabis policy changes associated with alcohol use patterns? Evidence for age‐group differences based on primary care screening data. Addiction, 120(11), 2282-2294. doi: 10.1111/add.70134.