WHAT PROBLEM DOES THIS STUDY ADDRESS?
Almost half of US adults aged 18-25 who reported past-month binge drinking also reported using cannabis. Although prior research suggests that individuals who co-use alcohol and cannabis drink more heavily and experience greater negative consequences than those who only use alcohol, the interaction between these two substances appears more complex than initially thought. Indeed, recent observational studies found an association between cannabis use and reduced alcohol consumption in certain populations and contexts, including heavy drinkers engaged in treatment and on days when cannabis is used before alcohol. The idea of cannabis as a tool to reduce harms associated with alcohol or substitute for alcohol is becoming increasingly visible with the rise of “Cali(fornia) sober,” where individuals replace alcohol with cannabis, and mocktails infused with THC (the primary active ingredient in cannabis) being advertised as alternatives to alcohol. However, despite these trends, no controlled human subjects experiments have directly tested the effects of cannabis on alcohol consumption. This study sought to understand more about this phenomenon by examining the dose-dependent effects of THC on alcohol craving and consumption among young adults who were co-using cannabis and alcohol.
HOW WAS THIS STUDY CONDUCTED?
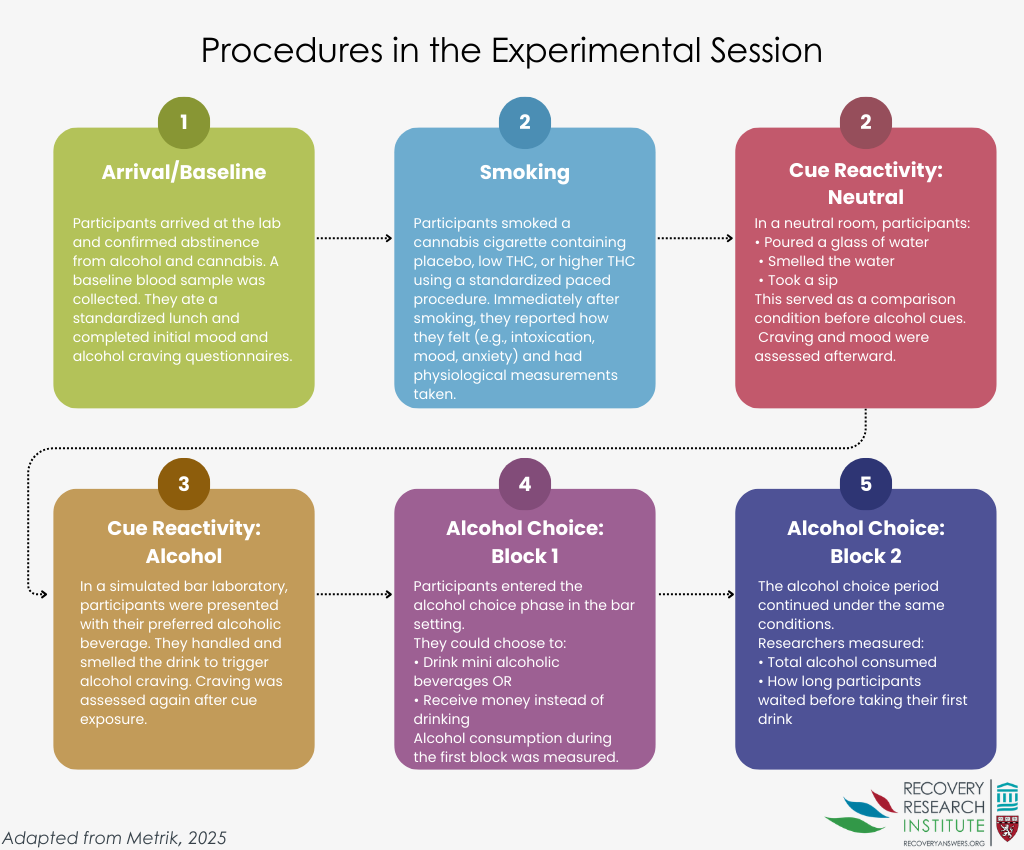
This crossover randomized trial tested the short-term, dose-dependent effects of THC on alcohol craving and consumption. The study’s sample was comprised of 157 adults (M = 25.6 years) who used cannabis at least twice per week and drank heavily (4+ for women; 5+ for men in one sitting) at least once per month. Three-fourths met DSM-5 criteria for current cannabis use disorder and almost half (43%) met for alcohol use disorder; severity indicators (mild/moderate/severe) were not reported. Participation was limited to individuals who had no intention to quit or enter treatment for an alcohol or cannabis use disorder, which limits the study’s generalizability to treatment-seeking populations. Participants attended three double-blinded experimental sessions (i.e., neither they nor the study staff knew which condition), during which they smoked a cannabis cigarette containing 0.03% THC (placebo), 3.1% THC, or 7.2% THC under standardized conditions, with the sequence counterbalanced to control for ordering effects. This rigorous design ensured participants were assigned to all three doses over the study period, allowing researchers to compare the dose-dependent effects within individuals. The graphic below summarizes the experimental procedures and corresponding data collected during each session. The primary outcome was self-reported alcohol craving, which also included a single-item measure of alcohol urgency. Alcohol consumption, the secondary outcome, was observed during a simulated alcohol choice task at a laboratory bar in which participants could choose to drink up to eight mini-drinks or receive monetary compensation for each drink they declined. In addition to the amount of alcohol participants drank, which was measured as the percent of available alcohol consumed, researchers also observed how long participants took to initiate drinking (i.e., latency). Although conducting the experiment in a laboratory setting strengthened the study’s internal validity, results may not reflect real-world drinking behavior.
WHAT DID THIS STUDY FIND?
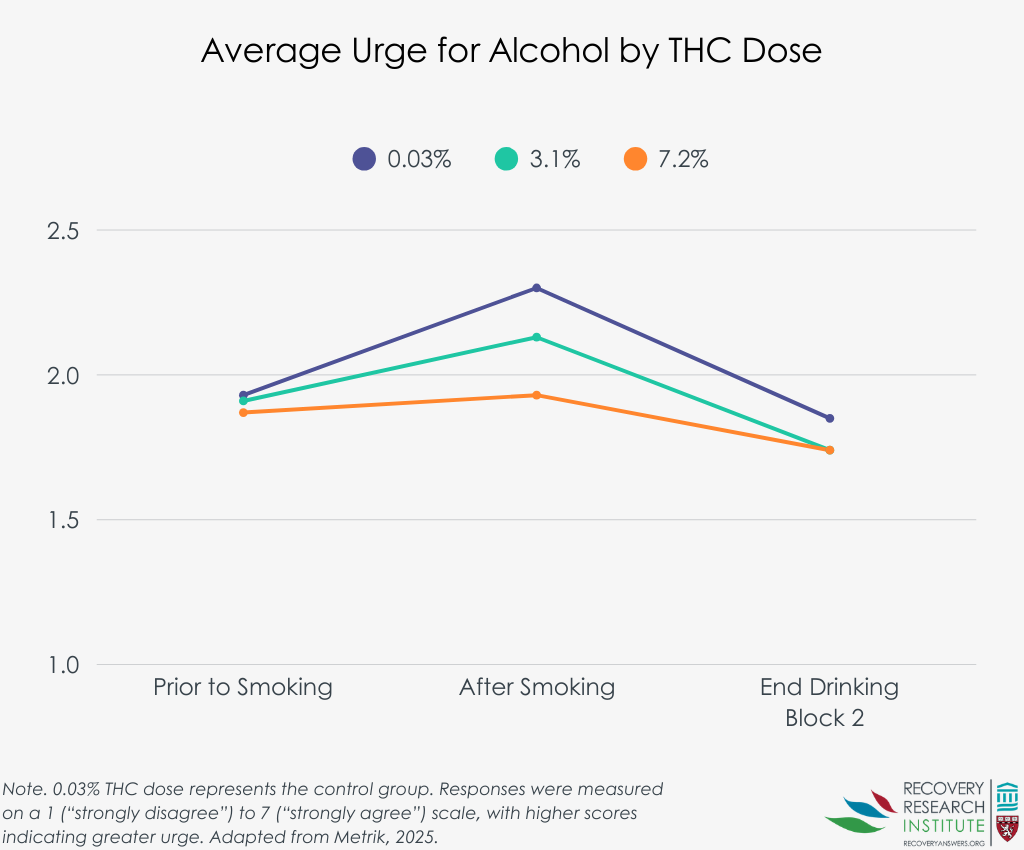
No effects on alcohol craving, but the higher THC dose reduced the urge to drink
Relative to placebo, neither active dose affected alcohol craving immediately after smoking or during alcohol cue exposure. However, the 7.2% THC dose reduced the urge to drink immediately after smoking compared to placebo, whereas the 3.1% THC dose did not (see graph below). There was no difference in craving or urge between the two active doses.
Participants drank less alcohol after smoking cannabis
Relative to placebo, both the 3.1% and 7.2% THC doses reduced the amount of alcohol participants consumed, with a 19% reduction for the lower dose and a 27% reduction for the higher dose. Although the higher dose had a larger reduction, the difference between the active doses was not significant. Notably, these reductions were consistent when limiting the analytic sample to only participants who chose to drink alcohol during a given session. The graph below illustrates these findings.

The higher THC dose delayed drinking initiation
The 7.2% THC dose increased the amount of time participants took to begin drinking compared to placebo (33.4 vs. 22.5 minutes, respectively). The 3.1% THC dose did not affect drinking initiation, and there was no significant difference between the active doses.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Smoking cannabis containing 3.1% or 7.2% THC reduced short-term alcohol consumption relative to placebo. This suggests that THC could help suppress drinking and, conversely, that alcohol intake may increase in the absence of cannabis as a compensatory behavior. Compared to placebo, neither active dose affected alcohol craving, but the higher dose reduced the immediate urge to drink and delayed drinking. Although this study provides preliminary evidence that smoking cannabis may reduce alcohol consumption, the findings are limited to acute effects in a tightly controlled laboratory setting among non-treatment-seeking adults. Additionally, half met criteria for alcohol use disorder, but the study did not specify the proportions of mild, moderate, and severe levels of the disorder. So, it is unclear whether these results would apply to individuals with addiction – i.e., on the more severe end of the spectrum. Also, it is unknown whether the effects would replicate over longer periods, in naturalistic settings, or in other populations. In other words, we do not know whether THC can serve as a real-world long-term aid to help people with severe alcohol use-related problems to stop their alcohol use. Finally, the THC content in this study was lower than the typical content for cannabis sold in recreational cannabis dispensaries (15-25% THC or more). It is possible that higher THC content would lead to a greater effect on reduced alcohol use; it is also possible that higher THC content could reduce inhibitions and impair judgment to a greater degree leading to increased alcohol use or lead to a new onset cannabis use disorder if used as a long-term solution. Overall, while these results are interesting, it remains unclear whether cannabis might be recommended as an alcohol “quit aid” or tool to reduce harms associated with alcohol based on this study alone.
BOTTOM LINE
Smoking cannabis could reduce alcohol consumption acutely and may have some beneficial effects on urges to drink. Given the lab-based nature of the study with non-treatment seeking individuals and lower THC content than for cannabis typically sold in recreational dispensaries, further research is needed before drawing conclusions or making any clinical recommendations about substituting cannabis for alcohol or adopting it as a tool to reduce harms associated with alcohol.
- For individuals and families seeking recovery: Using cannabis as a substitute for alcohol or a recovery strategy for alcohol use disorder is not currently recommended. Individuals pursuing alcohol use disorder recovery should prioritize evidence-based treatments and supports, such as cognitive behavioral therapy, approved medications, and mutual-help groups.
- For treatment professionals and treatment systems: Because the evidence for cannabis use as a tool to reduce harms associated with alcohol is limited and does not establish long-term safety or effectiveness, treatment professionals and systems should stick to recommending empirically supported treatments and recovery supports. When encountering patients who are substituting cannabis for alcohol, providers should monitor their cannabis use and counsel them on potential risks.
- For scientists: Future studies should test if the observed effects replicate in real-world settings and in other populations (particularly those seeking treatment) as well as whether the reductions persist over longer periods of time and produce a favorable risk ratio. Researchers should also evaluate potential consequences of substitution, including the risk for developing cannabis use disorder. If similar results are observed in future studies, researchers should consider examining alcohol urge reduction as a potential underlying mechanism.
- For policy makers: Public health messaging should avoid promoting cannabis as a substitute or tool to reduce harms associated with alcohol without stronger long-term evidence of its safety and effects on alcohol use. Policymakers may also consider implementing cannabis marketing/advertising regulations to prevent unsupported claims about substitution and warn of potential risks.
CITATIONS
Metrik, J., Aston, E. R., Gunn, R. L., Swift, R., MacKillop, J., & Kahler, C. W. (2026). Acute effects of cannabis on alcohol craving and consumption: A randomized controlled crossover trial. The American Journal of Psychiatry, 183(2), 134-143. doi: 10.1176/appi.ajp.20250115.