Female veteran survivors of sexual trauma die by suicide and overdose younger than their peers
Veterans who experience sexual trauma while in the military are more likely to have a substance use disorder and die at earlier ages than veterans who have not experienced sexual trauma. However, it is unclear if sexual trauma increases the risk of premature death specifically among veterans with substance use disorder. To examine this question, this study analyzed relationships between military sexual trauma and mortality across sex within the Veterans Health Administration.
This study analyzed data from the Veteran’s Health Administration Corporate Data Warehouse and Mortality Data Repository. The Veteran’s Health Administration Corporate Data Warehouse is a national repository of clinical data from the Veterans Health Information Systems and Technology Architecture and several other Veterans Health Administration clinical and administrative systems. The Veteran’s Health Administration Mortality Data Repository is a national repository of mortality data drawn from multiple sources (including the Department of Defense and the National Center for Health Statistics).
Data for the current study were restricted to veterans with an alcohol or opioid use disorder, as indicated by having at least 1 inpatient or 2 outpatient encounters with an International Classification of Disease code for either condition in any healthcare encounters. History of military sexual trauma was determined via indication of sexual harassment or assault during military service on the Veterans Health Administration military sexual trauma screener during a primary care or mental health appointment. All data for this study were from 2016-2022.
The main outcomes of the current study were age at death and death due to suicide or opioid overdose. To calculate age at death, the authors computed means and standard deviations for age at death for all deceased. Cause of death was determined by the presence of specific International Classification of Disease codes. Deaths due to opioid overdose were determined by the presence of International Classification of Disease codes indicating opioid poisoning (e.g., X40 “accidental self-poisoning by drugs…”). Deaths due to suicide were determined by presence of International Classification of Disease codes with the “intentional self-harm” qualifier, (e.g., X60 “intentional self-poisoning by drugs…”). The authors examined the differences in average age at death, and odds of dying via suicide or opioid overdose based on history of military sexual trauma and sex.
This study had a sample of 111,222 deceased veterans, including 108,309 male and 2,913 female veterans. The majority of the sample was White (66.9%), with remainder identifying as Black (20.4%), Hispanic or Latino (5.2%), unknown (5.0%), American Indian/Alaskan Native (1.0%), Asian (0.2%), multiple race/ethnicities (0.7%), or Native Hawaiian or Pacific Islander (0.6%). Analyses controlled statistically only for race/ethnicity to further isolate the effects of sexual trauma history and gender on outcomes. Over 80% of veterans had an alcohol use disorder, 9% had an opioid use disorder, and 10.8% had co-occurring alcohol and opioid use disorders. The average age at which veterans died was 66.8 years.
WHAT DID THIS STUDY FIND?
Veterans who experienced military sexual trauma were more likely to die by suicide and overdose
Compared to deceased veterans with an alcohol or opioid use disorder who did not experience military sexual trauma, those who did experience such trauma were 130% more likely to have died by suicide, compared to all other causes of death. In addition, those who experienced military sexual trauma died by suicide at younger ages relative to other veterans who died by suicide (46 vs 52 years of age, respectively). This risk of military sexual trauma on suicide did not differ by sex (i.e., there was no interaction effect).
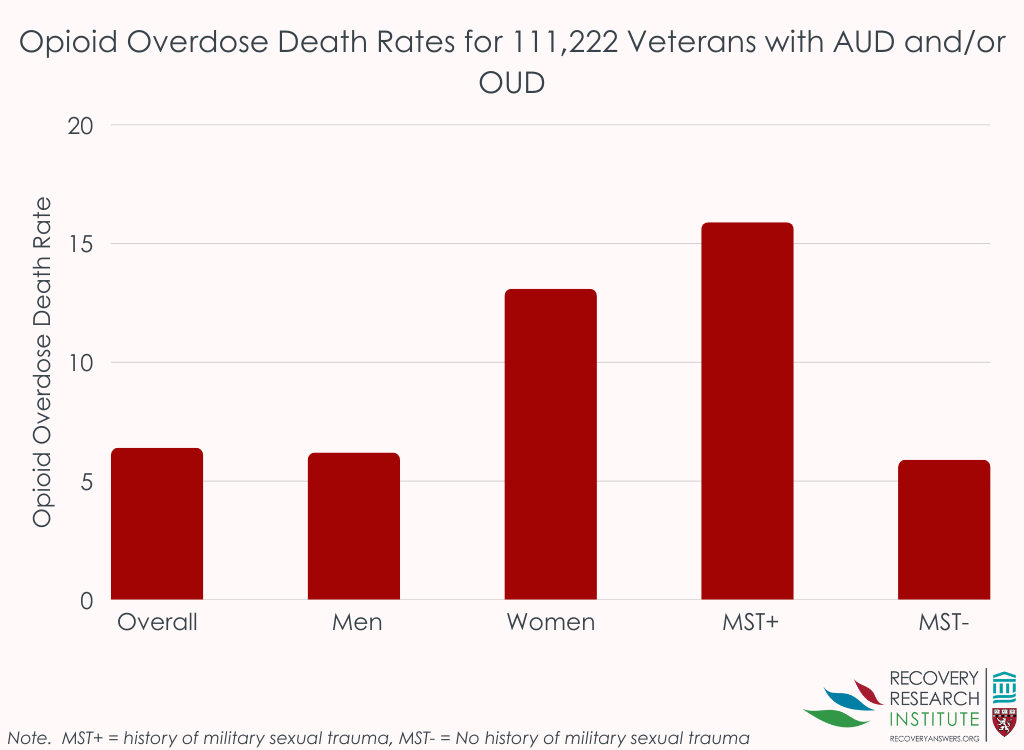
Compared to deceased veterans who did not experience military sexual trauma, those who did were 280% more likely to have died due to an opioid overdose compared to other causes (see graph below). In addition, veterans who experienced military sexual assault died at younger ages relative to other veterans who died by suicide (51.0 vs 52.7 years of age respectively).
Female veterans were more likely to die by suicide and overdose than male veterans
Relative to male veterans, deceased female veterans were 170% more likely to die by suicide compared to all other causes. As shown in the graph below, they were 160% more likely to die by opioid overdose than male veterans, relative to other causes. The effect of sex on suicide and overdose as causes of death did not differ by military sexual trauma history (i.e., there was no interaction effect).
Female veterans with history of military sexual trauma died earliest
Across all causes of death, the average age at death for female veterans who experienced military sexual trauma was 56.1 years. In contrast, male veterans who experienced military sexual trauma on average died at age 62.8 years. Men and women veterans who did not report past military sexual trauma on average died at the ages of 67.1 and 59.5 years respectively. Here – for all causes of death – the effect of military sexual trauma did differ by sex (i.e., there was an interaction effect). Women with a history of military sexual trauma died younger than women without a history of such trauma, as well as men, both with and without this history of trauma.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Experiencing military sexual trauma is associated with an increased risk of death due to suicide and opioid overdose among deceased veterans with alcohol or opioid use disorder, compared to all other causes of death. Veterans who experienced military sexual trauma were more likely to have died by suicide and died at younger ages than other deceased veterans. In addition, veterans who experienced military sexual trauma were more likely to have died due to an opioid overdose and died at younger ages relative to other deceased veterans. Taken together, these results demonstrate how military sexual trauma may explain increased risk of preventable causes of death like suicide and overdose. Importantly this study also highlights the increased impact of military sexual trauma on female veterans. Female veterans who experienced military sexual trauma died younger (of any cause) than all other veterans. This suggests that military sexual trauma may put female veterans at especially high risk of premature death. While these data point to risks of military sexual trauma on suicide and opioid overdose, importantly, it could also be that female deaths are more likely to result from suicide and overdose because men are at greater risk of other causes of death, like coronary disease, than women. Overall, men have higher rates of suicide and overdose than women; but these causes of death account for a larger share of female deaths, offering opportunities for prevention and intervention. Also of note, the study did not examine alcohol use-related death, which are greatest among men, but on the rise in women.
It is unclear from this study why military sexual trauma was associated with increased mortality among veterans (particularly among female veterans). However, it is likely that military sexual trauma impacts mortality in multiple ways, including negatively impacting mental health, increasing the severity of one’s substance use disorder, and reducing help seeking at Veteran’s Affair facilities. Female veterans may be especially deterred from seeking treatment since up to 42% of female veterans report experiencing sexual and gender-based harassment when seeking healthcare, which could cue a recurrence of trauma symptoms. This is speculative as the limitations of the data make it is impossible to determine how military sexual trauma impacted veterans’ mortality. Nevertheless, these results suggest veterans with substance use disorder who experienced military sexual trauma were at increased risk of premature death. Multi-pronged strategies are needed to ensure veterans receive the support and care they need. These may include, for example, female-specific treatment groups that offer empirically supported treatments for individuals who experienced sexual trauma (e.g., Seeking Safety).
The present data do not demonstrate temporality of substance use and military sexual trauma. That is, it is unclear if veterans’ substance use disorder symptomology occurred after or before their traumatic experiences. This is relevant as it has treatment implications: behavioral interventions may need to be tailored to account for if veterans began using alcohol/opioids because of their traumatic experiences (e.g., to cope) or if an already existing substance use disorder was compounded by traumatic sexual experiences.
Though all individuals in the sample received treatment at some point (i.e., to receive an alcohol or opioid use disorder diagnosis), the study does not present data on how many sampled veterans with substance use disorder were receiving addiction-specific treatment, such as medications for opioid use disorders. It is possible that receipt of treatment could have buffered the risk of military sexual trauma on premature death, for example, via overdose. Although it is likely many of these veterans were not receiving addiction-specific care (evidence suggests that only a fraction of veterans who could benefit from such treatments utilize it), this could have impacted the results.
The present study cannot elucidate why military sexual trauma impacted veterans’ (especially female veterans’) mortality. The authors speculate that a confluence of issues (e.g., avoiding care due to the triggering presence of military personnel and/or concerns about mixed gender group-based treatment) may be responsible. However, the nature of the data precludes an understanding of the mechanisms driving the observed trends.
The present study was limited to veterans with alcohol or opioid use disorder recorded on medical records. It is unclear how military sexual trauma may impact the mortality of veterans who either did not have a substance use disorder or did not disclose substance use disorder symptomology to Veteran’s Affairs personnel.
BOTTOM LINE
This study shows that deceased veterans with substance use disorder who experienced military sexual trauma were more likely to die by suicide and opioid overdose, relative to other causes of death, than their peers without such a trauma history. The study also shows that, among deceased veterans, female veterans who experienced military sexual trauma died significantly younger than all other veterans. It also found that female veterans overall were more likely to die from an opioid overdose compared to other causes of death than their male peers. Taken together, these results underscore the impact of military sexual trauma on the wellbeing of veterans and the need for improved prevention and intervention efforts.
For individuals and families seeking recovery: This study underscores that trauma can shape recovery outcomes among veterans with substance use disorder. Individuals and families should seek trauma-informed programs that integrate substance use and mental health care, recognizing how trauma can affect both relapse and engagement in treatment. Veterans and their loved ones can ask providers whether they have specific experience supporting military sexual trauma survivors or offer women-only or veteran-centered options. Because overdose and suicide risks are elevated, especially for female veterans, it is critical to ensure access to overdose prevention tools (e.g., naloxone) and supportive peer programs.
For treatment professionals and treatment systems: The present study highlights the need for clinicians to routinely assess for military sexual trauma and consider its lasting impact on recovery and treatment engagement. Survivors of military sexual trauma (particularly women) may avoid mixed-gender or group-based settings that feel unsafe or retraumatizing. Treatment systems should expand trauma-informed, gender-responsive care, including women-only services and telehealth options that improve accessibility. Increasing the use of medications for opioid use disorder distribution may prevent premature deaths.
For scientists: The present study shows there is a need to understand the mechanisms by which military sexual trauma and substance use disorder interact to impact mortality. Future research should examine how trauma-related avoidance, institutional mistrust, and limited access to gender-responsive treatment contribute to overdose and suicide risk. Longitudinal and mixed-methods studies could clarify how trauma-informed interventions influence both survival and recovery trajectories. It is also critical to include transgender and gender-diverse veterans, who face elevated sexual trauma risk but remain underrepresented in research. Advancing this work will be essential for developing evidence-based prevention and intervention strategies tailored to military sexual trauma survivors.
For policy makers: The present study shows there is a pressing need for policies that expand trauma-focused, veteran-centered care for military sexual trauma survivors. Policymakers should increase access to integrated mental health and substance use services, as well as medications for opioid use disorder and overdose prevention programs. Investments in peer-support initiatives and women-only treatment options within the Veteran’s Health Administration facilities could reduce barriers to care and improve engagement. Policies should also strengthen protections against harassment within these settings to make care environments safer. Expanding these supports can help mitigate the long-term health consequences of trauma and substance use among veterans.
This study analyzed data from the Veteran’s Health Administration Corporate Data Warehouse and Mortality Data Repository. The Veteran’s Health Administration Corporate Data Warehouse is a national repository of clinical data from the Veterans Health Information Systems and Technology Architecture and several other Veterans Health Administration clinical and administrative systems. The Veteran’s Health Administration Mortality Data Repository is a national repository of mortality data drawn from multiple sources (including the Department of Defense and the National Center for Health Statistics).
Data for the current study were restricted to veterans with an alcohol or opioid use disorder, as indicated by having at least 1 inpatient or 2 outpatient encounters with an International Classification of Disease code for either condition in any healthcare encounters. History of military sexual trauma was determined via indication of sexual harassment or assault during military service on the Veterans Health Administration military sexual trauma screener during a primary care or mental health appointment. All data for this study were from 2016-2022.
The main outcomes of the current study were age at death and death due to suicide or opioid overdose. To calculate age at death, the authors computed means and standard deviations for age at death for all deceased. Cause of death was determined by the presence of specific International Classification of Disease codes. Deaths due to opioid overdose were determined by the presence of International Classification of Disease codes indicating opioid poisoning (e.g., X40 “accidental self-poisoning by drugs…”). Deaths due to suicide were determined by presence of International Classification of Disease codes with the “intentional self-harm” qualifier, (e.g., X60 “intentional self-poisoning by drugs…”). The authors examined the differences in average age at death, and odds of dying via suicide or opioid overdose based on history of military sexual trauma and sex.
This study had a sample of 111,222 deceased veterans, including 108,309 male and 2,913 female veterans. The majority of the sample was White (66.9%), with remainder identifying as Black (20.4%), Hispanic or Latino (5.2%), unknown (5.0%), American Indian/Alaskan Native (1.0%), Asian (0.2%), multiple race/ethnicities (0.7%), or Native Hawaiian or Pacific Islander (0.6%). Analyses controlled statistically only for race/ethnicity to further isolate the effects of sexual trauma history and gender on outcomes. Over 80% of veterans had an alcohol use disorder, 9% had an opioid use disorder, and 10.8% had co-occurring alcohol and opioid use disorders. The average age at which veterans died was 66.8 years.
WHAT DID THIS STUDY FIND?
Veterans who experienced military sexual trauma were more likely to die by suicide and overdose
Compared to deceased veterans with an alcohol or opioid use disorder who did not experience military sexual trauma, those who did experience such trauma were 130% more likely to have died by suicide, compared to all other causes of death. In addition, those who experienced military sexual trauma died by suicide at younger ages relative to other veterans who died by suicide (46 vs 52 years of age, respectively). This risk of military sexual trauma on suicide did not differ by sex (i.e., there was no interaction effect).
Compared to deceased veterans who did not experience military sexual trauma, those who did were 280% more likely to have died due to an opioid overdose compared to other causes (see graph below). In addition, veterans who experienced military sexual assault died at younger ages relative to other veterans who died by suicide (51.0 vs 52.7 years of age respectively).
Female veterans were more likely to die by suicide and overdose than male veterans
Relative to male veterans, deceased female veterans were 170% more likely to die by suicide compared to all other causes. As shown in the graph below, they were 160% more likely to die by opioid overdose than male veterans, relative to other causes. The effect of sex on suicide and overdose as causes of death did not differ by military sexual trauma history (i.e., there was no interaction effect).
Female veterans with history of military sexual trauma died earliest
Across all causes of death, the average age at death for female veterans who experienced military sexual trauma was 56.1 years. In contrast, male veterans who experienced military sexual trauma on average died at age 62.8 years. Men and women veterans who did not report past military sexual trauma on average died at the ages of 67.1 and 59.5 years respectively. Here – for all causes of death – the effect of military sexual trauma did differ by sex (i.e., there was an interaction effect). Women with a history of military sexual trauma died younger than women without a history of such trauma, as well as men, both with and without this history of trauma.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Experiencing military sexual trauma is associated with an increased risk of death due to suicide and opioid overdose among deceased veterans with alcohol or opioid use disorder, compared to all other causes of death. Veterans who experienced military sexual trauma were more likely to have died by suicide and died at younger ages than other deceased veterans. In addition, veterans who experienced military sexual trauma were more likely to have died due to an opioid overdose and died at younger ages relative to other deceased veterans. Taken together, these results demonstrate how military sexual trauma may explain increased risk of preventable causes of death like suicide and overdose. Importantly this study also highlights the increased impact of military sexual trauma on female veterans. Female veterans who experienced military sexual trauma died younger (of any cause) than all other veterans. This suggests that military sexual trauma may put female veterans at especially high risk of premature death. While these data point to risks of military sexual trauma on suicide and opioid overdose, importantly, it could also be that female deaths are more likely to result from suicide and overdose because men are at greater risk of other causes of death, like coronary disease, than women. Overall, men have higher rates of suicide and overdose than women; but these causes of death account for a larger share of female deaths, offering opportunities for prevention and intervention. Also of note, the study did not examine alcohol use-related death, which are greatest among men, but on the rise in women.
It is unclear from this study why military sexual trauma was associated with increased mortality among veterans (particularly among female veterans). However, it is likely that military sexual trauma impacts mortality in multiple ways, including negatively impacting mental health, increasing the severity of one’s substance use disorder, and reducing help seeking at Veteran’s Affair facilities. Female veterans may be especially deterred from seeking treatment since up to 42% of female veterans report experiencing sexual and gender-based harassment when seeking healthcare, which could cue a recurrence of trauma symptoms. This is speculative as the limitations of the data make it is impossible to determine how military sexual trauma impacted veterans’ mortality. Nevertheless, these results suggest veterans with substance use disorder who experienced military sexual trauma were at increased risk of premature death. Multi-pronged strategies are needed to ensure veterans receive the support and care they need. These may include, for example, female-specific treatment groups that offer empirically supported treatments for individuals who experienced sexual trauma (e.g., Seeking Safety).
The present data do not demonstrate temporality of substance use and military sexual trauma. That is, it is unclear if veterans’ substance use disorder symptomology occurred after or before their traumatic experiences. This is relevant as it has treatment implications: behavioral interventions may need to be tailored to account for if veterans began using alcohol/opioids because of their traumatic experiences (e.g., to cope) or if an already existing substance use disorder was compounded by traumatic sexual experiences.
Though all individuals in the sample received treatment at some point (i.e., to receive an alcohol or opioid use disorder diagnosis), the study does not present data on how many sampled veterans with substance use disorder were receiving addiction-specific treatment, such as medications for opioid use disorders. It is possible that receipt of treatment could have buffered the risk of military sexual trauma on premature death, for example, via overdose. Although it is likely many of these veterans were not receiving addiction-specific care (evidence suggests that only a fraction of veterans who could benefit from such treatments utilize it), this could have impacted the results.
The present study cannot elucidate why military sexual trauma impacted veterans’ (especially female veterans’) mortality. The authors speculate that a confluence of issues (e.g., avoiding care due to the triggering presence of military personnel and/or concerns about mixed gender group-based treatment) may be responsible. However, the nature of the data precludes an understanding of the mechanisms driving the observed trends.
The present study was limited to veterans with alcohol or opioid use disorder recorded on medical records. It is unclear how military sexual trauma may impact the mortality of veterans who either did not have a substance use disorder or did not disclose substance use disorder symptomology to Veteran’s Affairs personnel.
BOTTOM LINE
This study shows that deceased veterans with substance use disorder who experienced military sexual trauma were more likely to die by suicide and opioid overdose, relative to other causes of death, than their peers without such a trauma history. The study also shows that, among deceased veterans, female veterans who experienced military sexual trauma died significantly younger than all other veterans. It also found that female veterans overall were more likely to die from an opioid overdose compared to other causes of death than their male peers. Taken together, these results underscore the impact of military sexual trauma on the wellbeing of veterans and the need for improved prevention and intervention efforts.
For individuals and families seeking recovery: This study underscores that trauma can shape recovery outcomes among veterans with substance use disorder. Individuals and families should seek trauma-informed programs that integrate substance use and mental health care, recognizing how trauma can affect both relapse and engagement in treatment. Veterans and their loved ones can ask providers whether they have specific experience supporting military sexual trauma survivors or offer women-only or veteran-centered options. Because overdose and suicide risks are elevated, especially for female veterans, it is critical to ensure access to overdose prevention tools (e.g., naloxone) and supportive peer programs.
For treatment professionals and treatment systems: The present study highlights the need for clinicians to routinely assess for military sexual trauma and consider its lasting impact on recovery and treatment engagement. Survivors of military sexual trauma (particularly women) may avoid mixed-gender or group-based settings that feel unsafe or retraumatizing. Treatment systems should expand trauma-informed, gender-responsive care, including women-only services and telehealth options that improve accessibility. Increasing the use of medications for opioid use disorder distribution may prevent premature deaths.
For scientists: The present study shows there is a need to understand the mechanisms by which military sexual trauma and substance use disorder interact to impact mortality. Future research should examine how trauma-related avoidance, institutional mistrust, and limited access to gender-responsive treatment contribute to overdose and suicide risk. Longitudinal and mixed-methods studies could clarify how trauma-informed interventions influence both survival and recovery trajectories. It is also critical to include transgender and gender-diverse veterans, who face elevated sexual trauma risk but remain underrepresented in research. Advancing this work will be essential for developing evidence-based prevention and intervention strategies tailored to military sexual trauma survivors.
For policy makers: The present study shows there is a pressing need for policies that expand trauma-focused, veteran-centered care for military sexual trauma survivors. Policymakers should increase access to integrated mental health and substance use services, as well as medications for opioid use disorder and overdose prevention programs. Investments in peer-support initiatives and women-only treatment options within the Veteran’s Health Administration facilities could reduce barriers to care and improve engagement. Policies should also strengthen protections against harassment within these settings to make care environments safer. Expanding these supports can help mitigate the long-term health consequences of trauma and substance use among veterans.
This study analyzed data from the Veteran’s Health Administration Corporate Data Warehouse and Mortality Data Repository. The Veteran’s Health Administration Corporate Data Warehouse is a national repository of clinical data from the Veterans Health Information Systems and Technology Architecture and several other Veterans Health Administration clinical and administrative systems. The Veteran’s Health Administration Mortality Data Repository is a national repository of mortality data drawn from multiple sources (including the Department of Defense and the National Center for Health Statistics).
Data for the current study were restricted to veterans with an alcohol or opioid use disorder, as indicated by having at least 1 inpatient or 2 outpatient encounters with an International Classification of Disease code for either condition in any healthcare encounters. History of military sexual trauma was determined via indication of sexual harassment or assault during military service on the Veterans Health Administration military sexual trauma screener during a primary care or mental health appointment. All data for this study were from 2016-2022.
The main outcomes of the current study were age at death and death due to suicide or opioid overdose. To calculate age at death, the authors computed means and standard deviations for age at death for all deceased. Cause of death was determined by the presence of specific International Classification of Disease codes. Deaths due to opioid overdose were determined by the presence of International Classification of Disease codes indicating opioid poisoning (e.g., X40 “accidental self-poisoning by drugs…”). Deaths due to suicide were determined by presence of International Classification of Disease codes with the “intentional self-harm” qualifier, (e.g., X60 “intentional self-poisoning by drugs…”). The authors examined the differences in average age at death, and odds of dying via suicide or opioid overdose based on history of military sexual trauma and sex.
This study had a sample of 111,222 deceased veterans, including 108,309 male and 2,913 female veterans. The majority of the sample was White (66.9%), with remainder identifying as Black (20.4%), Hispanic or Latino (5.2%), unknown (5.0%), American Indian/Alaskan Native (1.0%), Asian (0.2%), multiple race/ethnicities (0.7%), or Native Hawaiian or Pacific Islander (0.6%). Analyses controlled statistically only for race/ethnicity to further isolate the effects of sexual trauma history and gender on outcomes. Over 80% of veterans had an alcohol use disorder, 9% had an opioid use disorder, and 10.8% had co-occurring alcohol and opioid use disorders. The average age at which veterans died was 66.8 years.
WHAT DID THIS STUDY FIND?
Veterans who experienced military sexual trauma were more likely to die by suicide and overdose
Compared to deceased veterans with an alcohol or opioid use disorder who did not experience military sexual trauma, those who did experience such trauma were 130% more likely to have died by suicide, compared to all other causes of death. In addition, those who experienced military sexual trauma died by suicide at younger ages relative to other veterans who died by suicide (46 vs 52 years of age, respectively). This risk of military sexual trauma on suicide did not differ by sex (i.e., there was no interaction effect).
Compared to deceased veterans who did not experience military sexual trauma, those who did were 280% more likely to have died due to an opioid overdose compared to other causes (see graph below). In addition, veterans who experienced military sexual assault died at younger ages relative to other veterans who died by suicide (51.0 vs 52.7 years of age respectively).
Female veterans were more likely to die by suicide and overdose than male veterans
Relative to male veterans, deceased female veterans were 170% more likely to die by suicide compared to all other causes. As shown in the graph below, they were 160% more likely to die by opioid overdose than male veterans, relative to other causes. The effect of sex on suicide and overdose as causes of death did not differ by military sexual trauma history (i.e., there was no interaction effect).
Female veterans with history of military sexual trauma died earliest
Across all causes of death, the average age at death for female veterans who experienced military sexual trauma was 56.1 years. In contrast, male veterans who experienced military sexual trauma on average died at age 62.8 years. Men and women veterans who did not report past military sexual trauma on average died at the ages of 67.1 and 59.5 years respectively. Here – for all causes of death – the effect of military sexual trauma did differ by sex (i.e., there was an interaction effect). Women with a history of military sexual trauma died younger than women without a history of such trauma, as well as men, both with and without this history of trauma.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Experiencing military sexual trauma is associated with an increased risk of death due to suicide and opioid overdose among deceased veterans with alcohol or opioid use disorder, compared to all other causes of death. Veterans who experienced military sexual trauma were more likely to have died by suicide and died at younger ages than other deceased veterans. In addition, veterans who experienced military sexual trauma were more likely to have died due to an opioid overdose and died at younger ages relative to other deceased veterans. Taken together, these results demonstrate how military sexual trauma may explain increased risk of preventable causes of death like suicide and overdose. Importantly this study also highlights the increased impact of military sexual trauma on female veterans. Female veterans who experienced military sexual trauma died younger (of any cause) than all other veterans. This suggests that military sexual trauma may put female veterans at especially high risk of premature death. While these data point to risks of military sexual trauma on suicide and opioid overdose, importantly, it could also be that female deaths are more likely to result from suicide and overdose because men are at greater risk of other causes of death, like coronary disease, than women. Overall, men have higher rates of suicide and overdose than women; but these causes of death account for a larger share of female deaths, offering opportunities for prevention and intervention. Also of note, the study did not examine alcohol use-related death, which are greatest among men, but on the rise in women.
It is unclear from this study why military sexual trauma was associated with increased mortality among veterans (particularly among female veterans). However, it is likely that military sexual trauma impacts mortality in multiple ways, including negatively impacting mental health, increasing the severity of one’s substance use disorder, and reducing help seeking at Veteran’s Affair facilities. Female veterans may be especially deterred from seeking treatment since up to 42% of female veterans report experiencing sexual and gender-based harassment when seeking healthcare, which could cue a recurrence of trauma symptoms. This is speculative as the limitations of the data make it is impossible to determine how military sexual trauma impacted veterans’ mortality. Nevertheless, these results suggest veterans with substance use disorder who experienced military sexual trauma were at increased risk of premature death. Multi-pronged strategies are needed to ensure veterans receive the support and care they need. These may include, for example, female-specific treatment groups that offer empirically supported treatments for individuals who experienced sexual trauma (e.g., Seeking Safety).
The present data do not demonstrate temporality of substance use and military sexual trauma. That is, it is unclear if veterans’ substance use disorder symptomology occurred after or before their traumatic experiences. This is relevant as it has treatment implications: behavioral interventions may need to be tailored to account for if veterans began using alcohol/opioids because of their traumatic experiences (e.g., to cope) or if an already existing substance use disorder was compounded by traumatic sexual experiences.
Though all individuals in the sample received treatment at some point (i.e., to receive an alcohol or opioid use disorder diagnosis), the study does not present data on how many sampled veterans with substance use disorder were receiving addiction-specific treatment, such as medications for opioid use disorders. It is possible that receipt of treatment could have buffered the risk of military sexual trauma on premature death, for example, via overdose. Although it is likely many of these veterans were not receiving addiction-specific care (evidence suggests that only a fraction of veterans who could benefit from such treatments utilize it), this could have impacted the results.
The present study cannot elucidate why military sexual trauma impacted veterans’ (especially female veterans’) mortality. The authors speculate that a confluence of issues (e.g., avoiding care due to the triggering presence of military personnel and/or concerns about mixed gender group-based treatment) may be responsible. However, the nature of the data precludes an understanding of the mechanisms driving the observed trends.
The present study was limited to veterans with alcohol or opioid use disorder recorded on medical records. It is unclear how military sexual trauma may impact the mortality of veterans who either did not have a substance use disorder or did not disclose substance use disorder symptomology to Veteran’s Affairs personnel.
BOTTOM LINE
This study shows that deceased veterans with substance use disorder who experienced military sexual trauma were more likely to die by suicide and opioid overdose, relative to other causes of death, than their peers without such a trauma history. The study also shows that, among deceased veterans, female veterans who experienced military sexual trauma died significantly younger than all other veterans. It also found that female veterans overall were more likely to die from an opioid overdose compared to other causes of death than their male peers. Taken together, these results underscore the impact of military sexual trauma on the wellbeing of veterans and the need for improved prevention and intervention efforts.
For individuals and families seeking recovery: This study underscores that trauma can shape recovery outcomes among veterans with substance use disorder. Individuals and families should seek trauma-informed programs that integrate substance use and mental health care, recognizing how trauma can affect both relapse and engagement in treatment. Veterans and their loved ones can ask providers whether they have specific experience supporting military sexual trauma survivors or offer women-only or veteran-centered options. Because overdose and suicide risks are elevated, especially for female veterans, it is critical to ensure access to overdose prevention tools (e.g., naloxone) and supportive peer programs.
For treatment professionals and treatment systems: The present study highlights the need for clinicians to routinely assess for military sexual trauma and consider its lasting impact on recovery and treatment engagement. Survivors of military sexual trauma (particularly women) may avoid mixed-gender or group-based settings that feel unsafe or retraumatizing. Treatment systems should expand trauma-informed, gender-responsive care, including women-only services and telehealth options that improve accessibility. Increasing the use of medications for opioid use disorder distribution may prevent premature deaths.
For scientists: The present study shows there is a need to understand the mechanisms by which military sexual trauma and substance use disorder interact to impact mortality. Future research should examine how trauma-related avoidance, institutional mistrust, and limited access to gender-responsive treatment contribute to overdose and suicide risk. Longitudinal and mixed-methods studies could clarify how trauma-informed interventions influence both survival and recovery trajectories. It is also critical to include transgender and gender-diverse veterans, who face elevated sexual trauma risk but remain underrepresented in research. Advancing this work will be essential for developing evidence-based prevention and intervention strategies tailored to military sexual trauma survivors.
For policy makers: The present study shows there is a pressing need for policies that expand trauma-focused, veteran-centered care for military sexual trauma survivors. Policymakers should increase access to integrated mental health and substance use services, as well as medications for opioid use disorder and overdose prevention programs. Investments in peer-support initiatives and women-only treatment options within the Veteran’s Health Administration facilities could reduce barriers to care and improve engagement. Policies should also strengthen protections against harassment within these settings to make care environments safer. Expanding these supports can help mitigate the long-term health consequences of trauma and substance use among veterans.