
Peer-Based Recovery Support
(Related: mutual-help organizations, mutual aid, self-help)
Peer-based recovery support, known as mutual-help organizations (or self-help groups) – are free, peer-led (i.e., non-professional) organizations that developed to help individuals with substance use disorders and other addiction-related problems.
Mutual-help organizations focus on the socially-supportive communication and exchange of addiction and recovery experience and skills. Individuals participate in activities that engage, educate, and support patients recovering from substance use disorder from others facing similar challenges. Mutual help organizations include: Alcoholics Anonymous (AA), Narcotics Anonymous (NA), SMART Recovery, All Recovery groups, and online forums.
3 TYPES OF MUTUAL-HELP ORGANIZATIONS:
- TWELVE-STEP (traditional), like Alcoholics Anonymous (AA) and Narcotics Anonymous (NA)
- TWELVE-STEP (secular), like Secular AA and ICSAA
- NON TWELVE-STEP (secular), which are growing but smaller entities, such as SMART Recovery, Women for Sobriety, and LifeRing
- RELIGIOUS, such as Celebrate Recovery
12-STEP MUTUAL-HELP ORGANIZATIONS
12-step organizations like Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) are the largest and most widely-accessible mutual-help organizations in communities around the world. AA for example, has an estimated 67,000 groups, which serve 1.4 million members across the U.S. and Canada, and 120,000 groups serving over 2 million individuals worldwide. NA is comparatively smaller than AA, with 67,000 groups in total across 139 countries, and in every U.S. state and virtually all major cities. Of note, in contrast to AA, the majority of NA’s groups are located outside the United States.
- READ MORE ON 12-STEP MUTUAL-HELP ORGANIZATIONS
-
Alcoholics Anonymous (AA), Narcotics Anonymous (NA), and the plethora of other 12-step organizations (e.g., Marijuana Anonymous and Cocaine Anonymous) typically operate in 60-90 minute group meetings where attendees gather to share and exchange personal information regarding their lived experiences in active addiction and recovery, as well as learn how to apply the 12-step principles and practices in their day-to-day lives. This model of how people recover from substance use disorder is grounded in the acceptance of addiction as an illness that can be effectively addressed through abstinence and other behavior change, but not completely cured (i.e., regardless of how long one has been in recovery, the risk of escalation and serious consequences from alcohol or other drug use is never completely eradicated).
These organizations emphasize spiritual and emotional growth as tools to cope with the difficulties that may have originally contributed to the individual’s addiction, as well as to buffer against relapse. These coping skills are also intended to produce contented sobriety and enhanced psychological well-being. AA and NA promote a reciprocal helping model (“sponsorship”), whereby individuals serve as personal mentors to support newer members as they accrue time and experience in recovery. This arrangement helps both the helper and those helped. The reciprocal helping model is a cornerstone, not only of 12-step mutual-help philosophy and practice, but for many other types of mutual-help organizations as well. Major aspects of the 12-step program and philosophy are codified in readings and other written documents sanctioned and regulated by the organizations themselves (e.g., AA’s “Big Book” or NA’s “Basic Text”).
Alcoholics Anonymous and Narcotics Anonymous, as the most prominent examples of 12-step mutual-help organizations, are run by paid and volunteer members of “World Services.” They sanction literature used by the organizations, organize the annual convention, and oversee the hundreds of regional associations. In any given meeting, members volunteer to fulfill responsibilities (e.g., running the meeting, making coffee, giving out chips to mark lengths of sobriety). Service in AA and NA is highly valued, both in terms of offering support to new members, as well as providing practical support to meeting upkeep or to local, state, and regional committees that help organize events and community involvement.
While meetings are completely autonomous, and formats may differ from meeting to meeting, there are several 12-step mutual-help cultural traditions common to the vast majority of meetings. Such traditions include opening and closing statements or prayers (e.g., the “serenity prayer”), readings (e.g., an outline of the 12 steps), and recognition of individuals who have accrued varying amounts of time in recovery (e.g., 30, 60, 90 days) with chips or key-tags.
In many cases, Alcoholics Anonymous and Narcotics Anonymous offer a subset of its meetings for specific groups of individuals, ostensibly to enhance attendees’ sense of a “shared experience,” and increase cohesion and identification, including meetings for women, young people, and LGBTQ+ individuals.
- EVIDENCE BASE FOR TWELVE-STEP MUTUAL-HELP ORGANIZATIONS
-
12-STEP MUTUAL-HELP ORGANIZATIONS:
Studies examining the effects of 12-step mutual-help organizations generally show that participation is prospectively related to positive substance outcomes like abstinence over time (see evidence here, here, here, and here). Given that mutual-help organizations are accessible and freely available resources, it is impossible to completely separate the contribution of community-based mutual-help participation to positive outcomes from other factors that could be related both to mutual-help participation and positive outcomes. Scientists in the area have used statistical methods to address this challenge – these have gotten increasingly more sophisticated over time (e.g., propensity score matching and instrumental variables analysis) in order to isolate the unique impact of mutual-help participation. Overall, expert reviews of these sophisticated studies published in high-quality, peer-reviewed journals consistently show that AA participation helps promote better alcohol outcomes over time.
The 2016 United States’ Surgeon General’s Report on Alcohol, Drugs, and Health concluded that professional treatments that link and engage individuals with 12-step mutual-help groups, called 12-step facilitation approaches (outlined in greater detail in the “Clinical Pathways” section of the website) have good scientific support, and studies have shown these type of clinical treatments often work better than other approaches because they help to increase 12-step mutual-help participation. These studies also demonstrate scientifically that 12-step mutual-help participation helps reduce alcohol and other drug use among individuals with substance use disorder.
Research also shows that AA and NA participation confers benefit in ways similar to professional treatment engagement: by boosting coping skills, confidence in one’s ability to stay in recovery (known as abstinence self-efficacy), and recovery motivation, as well as by facilitating recovery-supportive changes in people’s social networks (e.g., dropping people that support their drinking or hinder their recovery from their networks).
While the limited number of studies on 12-step mutual-help for drugs apart from alcohol are promising, more research is needed on individuals with other drug use disorders, and specifically on whether NA can help individuals like AA has been shown to. More research is also needed on how individuals who have never sought professional treatment benefit from 12-step mutual-help groups, given that studies have largely focused on treatment-seeking individuals.
SECULAR MUTUAL-HELP ORGANIZATIONS
Non-12-step mutual-help organizations are often called “secular” mutual-help organizations given their intentional focus on non-spiritual aspects of addiction recovery. The notable, though modest, growth of secular mutual-help, coupled with the need to identify alternatives to 12-step mutual-help, has led to increased attention paid to these organizations in communities and clinical programs.
- READ MORE ON SECULAR MUTUAL-HELP ORGANIZATIONS
-
Regarding prevalence, their reach and accessibility are limited compared to AA and NA. Among the largest secular mutual-help organizations, for example, are:
- SMART Recovery (3200 weekly meetings worldwide and 2000 in the United States, 32 meetings online, with these meetings being run by trained facilitators)
- Women for Sobriety (for women only, with approximately 300 meetings in the United States and Canada)
- Secular Organizations for Sobriety
- LifeRing (with an estimated 150 meetings across a handful of U.S. states)
- Moderation management (30 online meetings per week, online courses for moderation and abstinence through the kickstart programs)
Tied together by their separation from 12-step models of how people recover, secular mutual-help organizations vary in the degree to which their recovery programs are delineated. SMART Recovery, for example, leans heavily on didactics to help people quit alcohol and other drugs (or to change other behavioral problems), grounded in motivational and cognitive-behavioral principles (e.g., coping with urges and problem solving). Secular Organizations for Sobriety, on the other hand, emphasizes an individual’s ability to map out his/her own path to abstain.
One unique resource offered by many of these mutual-help organizations are sanctioned online meetings and discussion groups (i.e., facilitated by the organizations themselves). Online meetings and other digital recovery management resources affiliated with 12-step mutual-help organizations (e.g., InTheRooms.com), however, are not typically sanctioned by the organizations themselves.
- EVIDENCE BASE FOR SECULAR MUTUAL-HELP ORGANIZATIONS
-
SECULAR MUTUAL-HELP:
Virtually all of the research on mutual-help organizations has focused on 12-step mutual-help, given that these groups are widespread, easily accessible in communities, and often serve as referral resources for treatment programs and providers. Research is needed to understand whether attending secular groups, like SMART Recovery, also helps promote substance-related benefit. In the few initial studies that have been conducted on SMART, findings have been positive, with the first systematic review showing that attending more SMART Recovery meetings is related to better alcohol outcomes. That said, review authors also concluded that higher-quality studies are needed to offer more definitive conclusions about whether SMART is a helpful recovery support service for individuals with substance use disorder.
RELIGIOUS MUTUAL-HELP ORGANIZATIONS
On the opposite end of the mutual-help spectrum from secular groups are religiously-affiliated mutual-help and other recovery support organizations. Among the largest and most well-known is Celebrate Recovery, a Christian-based recovery support organization with 17,000 groups worldwide that caters to individuals not only with substance use, but other behavioral problems as well. Unlike other recovery-related mutual-help organizations, in which meeting attendees typically remain together for the duration of any given meeting, Celebrate Recovery breaks into smaller gender-specific groups targeting a variety of issues. While it is relatively easy to start an AA or NA meeting, individual Celebrate Recovery meetings are closely monitored by the national organization. There are other, much smaller religious recovery support organizations, designed to help individuals with substance use problems, including those for individuals identifying as Jewish (e.g., Jewish Alcoholics, Chemically Dependent Persons, and Significant Others) or Muslim (Millati Islami).
Also of note, there has been tremendous grassroots growth in the use of Buddhism and its practices (e.g., meditation) for individuals seeking or currently in recovery from substance use disorder – sometimes affiliated with a 12-step program, though not in all cases.
- EVIDENCE BASE FOR RELIGIOUS MUTUAL-HELP ORGANIZATIONS
-
RELIGIOUS MUTUAL-HELP:
While the growth of religiously-affiliated groups like Celebrate Recovery suggest individuals may perceive it as helpful, little is known scientifically about these types of mutual-help organizations. Rigorous studies are needed to investigate how participation in religiously-affiliated mutual help organizations affects alcohol and other drug outcomes over time.
IN SUMMARY
In comparison to the horizontal governance structure in 12-step mutual-help groups – where meetings and other local organizations are overseen by volunteer individuals who are themselves in recovery – SMART and Celebrate Recovery, with their more vertical governance structure, have oversight and greater standardization in implementation of the meetings. Arguably, this means better “quality control” of these more standardized groups. On the other hand, the greater oversight and centralized management may constrain their ability to grow. It is not yet clear also whether this greater degree of quality control and oversight results in better engagement and recovery outcomes (Kelly & White, 2012).
Overall, each of these three types of mutual-help organizations are quite different in terms of their philosophy on how to help individuals recover from substance use disorder. At the same time, they virtually all share a central tenet of abstinence from alcohol and other drugs as the recovery goal. They may also help individuals reduce or abstain from alcohol and other drug use in similar ways, though research is needed to test this assumption.
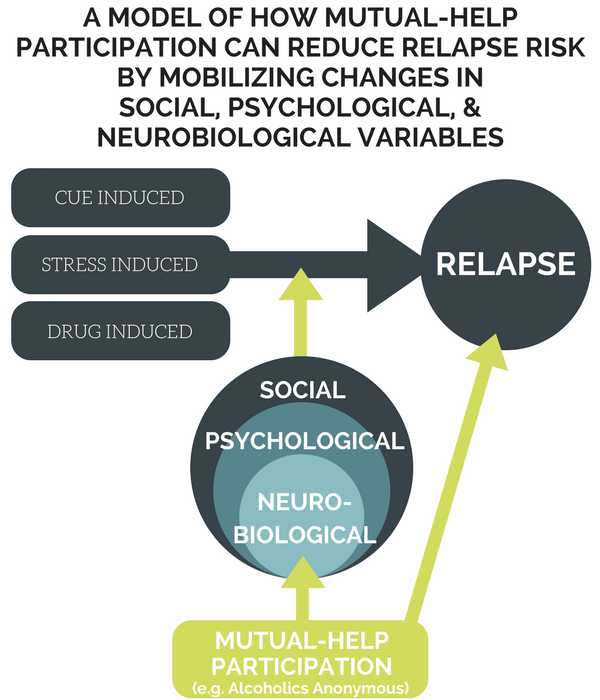
As illustrated in the figure below, mutual-help participation can facilitate engagement with recovery-focused social networks, which may help mobilize related recovery-supportive changes in the brain (via abstinence or reduced substance use), as well as in someone’s psychological and social functioning. In turn, these changes may help buffer against alcohol and other drug cravings, thus reducing relapse risk.
KEY READINGS
- List of Key Readings
-
- Humphreys, K. (2004). Circles of recovery: Self-help organizations for addictions. Cambridge, UK: Cambridge University Press.
- Humphreys, K., Blodgett, J. C., & Wagner, T. H. (2014). Estimating the efficacy of Alcoholics Anonymous without self-selection bias: An instrumental variables re-analysis of randomized clinical trials. Alcoholism: Clinical and Experimental Research, 38(11), 2688-2694. doi: 10.1111/acer.12557
- Kaskutas, L. A. (2009). Alcoholics Anonymous effectiveness: Faith meets science. Journal of Addictive Diseases, 28(2), 145-157. doi: 10.1080/10550880902772464
- Kelly, J. F. (2017). Is Alcoholics Anonymous religious, spiritual, neither? Findings from 25 years of mechanisms of behavior change research. Addiction, 112(6), 929-936. doi: 10.1111/add.1359
- Kelly J. F. & White W. L. (2012). Broadening the base of addiction mutual-help organizations. Journal of Groups in Addiction & Recovery, 7(2-4), 82-101. doi: 10.1080/1556035X.2012.705646
- Kelly, J. F. & Yeterian, J. D. (2012). Empirical awakening: The new science on mutual help and implications for cost containment under health care reform. Substance Abuse, 33, 85-91. doi: 10.1080/08897077.2011.634965
- Magura S., McKean J., Kosten S., Tonigan J. S. A novel application of propensity score matching to estimate Alcoholics Anonymous’ effect on drinking outcomes. Drug and Alcohol Dependence, 129(1-2), 54-59. doi: 10.1016/j.drugalcdep.2012.09.011
- Tonigan, J. S., Connors, G. J., & Miller, W. R. (2003). Participation and involvement in Alcoholics Anonymous. In T. F. Babor & F. K. Del Boca (Eds.), International research monographs in the addictions. Treatment matching in alcoholism (pp. 184-204). New York, NY, US: Cambridge University Press.
- Ye, Y., & Kaskutas, L. A. (2009). Using propensity scores to adjust for selection bias when assessing the effectiveness of Alcoholics Anonymous in observational studies. Drug and Alcohol Dependence, 104(1-2), 56-64. doi: 10.1016/j.drugalcdep.2009.03.018

