Who receives contingency management for stimulant use disorder?
Despite a widespread rollout of contingency management in the Veteran Affairs (VA) Healthcare System in 2011, most patients with stimulant use disorder still do not receive this gold standard treatment, reflecting a broader trend of slow uptake in healthcare systems across the country. This study examined patient characteristics associated with getting contingency management using data from within the VA.
Stimulant use, such as methamphetamine or cocaine use, has rapidly increased in the past decade. Despite extensive development efforts, there are currently no Food and Drug Administration (FDA)-approved medications to treat stimulant use disorder. However, one intervention in particular, contingency management has proven quite useful for treating stimulant use disorder. Contingency management is a method in which rewards, such as money or vouchers, are provided to patients contingent upon their ability to meet some outcome, such as attending a treatment session or remaining abstinent (i.e., testing negative on a drug screen). These contingencies also create what is known as an “opportunity cost”: using substances takes away the opportunity to get the monetary/voucher reward they would otherwise receive. Studies have demonstrated that contingency management is a very helpful approach to increase abstinence broadly for people who have substance use disorders, and for people with stimulant use disorder more specifically.
Contingency management’s promise as a treatment for stimulant use disorder has not manifested in widespread dissemination across healthcare systems due to notable barriers that include stigma and national policies that prevent giving gifts with monetary value to patients. Some of the more fervent opposition notes that, in some cases, the rewards are drawn from many options, which can be perceived as a form of gambling. In 2011, however, The Department of Veteran Affairs officially “rolled out” implementation of contingency management across the Veteran Affairs Healthcare System. Initial evaluations found widespread uptake of contingency management in targeted clinics, alongside promising engagement and substance use outcomes. Yet, recent studies have shown that only a small number of people with stimulant use disorder in the Veteran Affairs Healthcare System actually receive this empirically supported intervention. To inform ways to enhance uptake, this study investigated characteristics of patients who did and did not receive contingency management among patients with stimulant use disorder within VA programs that begun to implement such programming in the US VA Healthcare System.
HOW WAS THIS STUDY CONDUCTED?
This study used archival data from the Veteran Affairs Healthcare System electronic medical record. Within facilities that had begun to implement contingency management, the authors extracted all patients who had at least one visit occurring between the 2-year period of October 1, 2020 and September 30, 2022, and had a chart diagnosis of stimulant use disorder. The authors wanted to know how many people with stimulant use disorder across the VA Healthcare System were receiving contingency management, and whether certain patient characteristics predicted who did and did not receive contingency management.
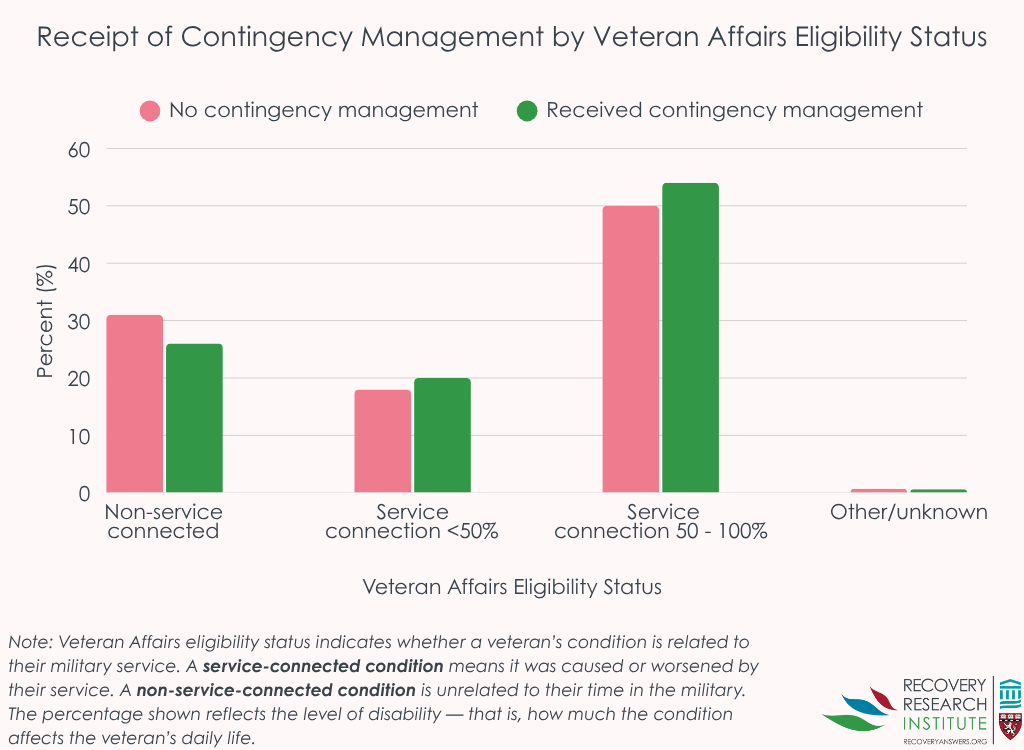
To this end, the authors also extracted data on sex, age, race, ethnicity, rurality, Veteran Affairs service connection (service connection ratings are based on whether a disability is linked to their military service, and the degree to which it impacts their functioning, as determined by the Department of Veteran Affairs), housing instability, substance use disorder comorbidity, mental health comorbidity, prior stimulant use disorder treatment engagement, and the number of stimulant use disorder medication management visits. These variables were included together in a model predicting contingency management utilization. Such statistical adjustments help to isolate the effect of interest – i.e., whether a participant characteristic is independently related to receiving contingency management. Also, in order to increase confidence that effects are true, the authors used complex statistical models to account for the fact that some patients came from the same facilities, and that facilities may differ in their ability to implement contingency management.
Importantly, to determine who used contingency management, the VA Healthcare System developed a common contingency management note template in 2018. The authors defined contingency management engagement as those with at least one contingency management note. All predictors (e.g., age, comorbidities, etc.) were extracted either at the time of the index visit, or from notes within the prior year.
The sample was, on average, 55 years of age, 93% male, 49% White, 42% Black, and 2% identified as another race; 7% identified as Hispanic. Approximately half had a service connection above 50%, 40% were experiencing homelessness, and 90% lived in urban areas.
WHAT DID THIS STUDY FIND?
Few patients with stimulant use disorder were receiving contingency management
The authors identified 93,960 patients who met criteria for stimulant use disorder during this period. Only 1% (1,113 VA patients) received contingency management in the year after their first visit.
Contingency management utilization was determined by key variables such as age, race, service connection, treatment engagement, and comorbidity
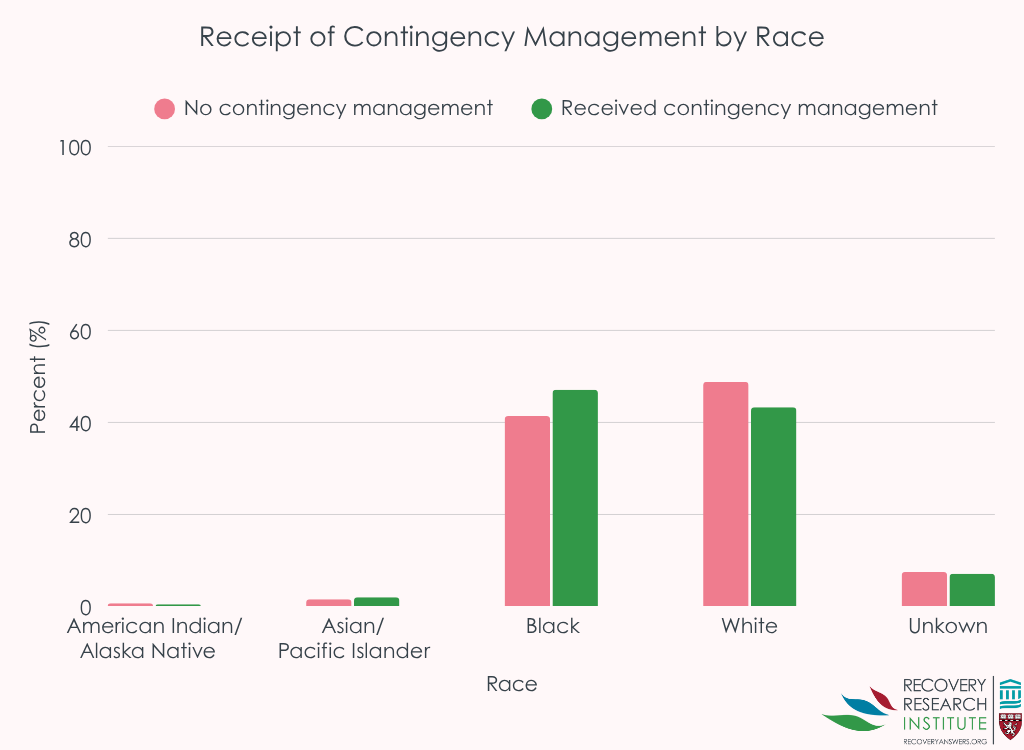
Compared to those between the ages of 18-29, those who were between 30-44 and those between 45-64 were approximately twice as likely to receive contingency management. Black patients were approximately 50% more likely to receive contingency management relative to White patients; other racial groups were not more or less likely to receive contingency management relative to White patients (see Graph below).
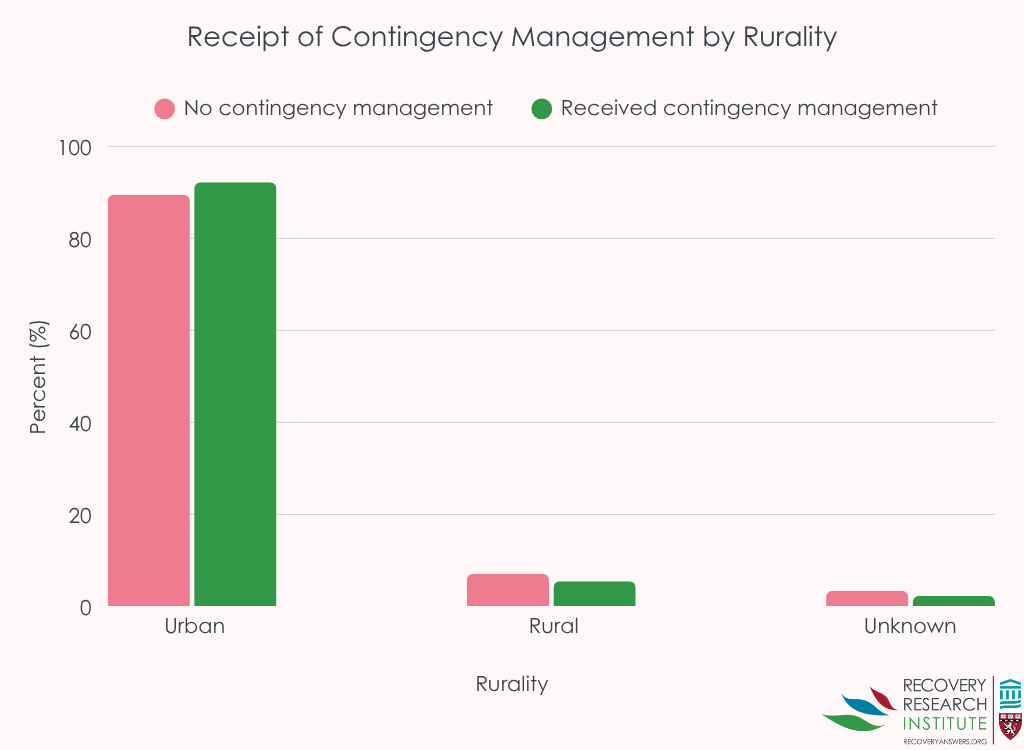
Those in rural areas were 35% less likely to receive contingency management.
Housing instability was also associated with a 70% greater likelihood of receiving contingency management. Also, comorbidity – other disorders in addition to stimulant use disorder – was associated with likelihood of receiving contingency management, but in different directions for substance and mental health comorbidities. Those meeting criteria for opioid use disorder or alcohol use disorder were approximately 20% more likely to receive contingency management, and those with “other drug disorder” (which in this study was defined by sedatives, hallucinogens, and inhalants) were approximately 33% more likely to receive contingency management compared to those without one of those diagnoses. On the other hand, those with a posttraumatic stress disorder diagnosis (in addition to their stimulant use disorder diagnosis) were 15% less likely to receive contingency management compared to those without that diagnosis.
Relative to those without service connection, those with service connections were 25-35% more likely to receive contingency management.
Finally, the number of past year stimulant use disorder treatment visits predicted greater likelihood of receiving contingency management, with each additional psychotherapy visit increasing the likelihood by 1%, and each medication management visit increasing the likelihood by 5%.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Despite the national rollout of contingency management in the Veteran Affairs Healthcare System, patients with stimulant use disorder were still unlikely to receive contingency management: only 1% received at least one session of contingency management. It is unclear why contingency management, a very useful intervention for stimulant use disorder, has been adopted so infrequently. One possibility is that these data were collected at the beginning of the COVID-19 pandemic, a time when contingency management was not being deployed as often. Irrespective of the underlying reasons, engagement in any treatment requires the procedures to be implemented in clinics, for providers to be trained to properly execute the treatment and to begin to use that treatment when necessary, and for patients to select this treatment when given the opportunity. It is difficult to know where in this cascade we see the greatest impact on utilization of this treatment.
Nevertheless, there were some patient characteristics that were associated with the likelihood of receiving contingency management, including those who are between ages 30–64, Black race, experiencing housing instability, service-connected disability, and those who live in rural areas. Understanding how these factors impact receipt of a robust treatment for stimulant use disorder may help providers and Veteran Affairs decision makers increase uptake among populations that are less likelihood to receive it.
The finding that those who have alcohol, opioid or other drug use disorders in addition to stimulant use disorder, as well as those with more therapy and medication visits, were more likely to receive contingency management suggests that greater severity may in part predict contingency management receipt. Unfortunately, the method of data collection prevents exploring this question more closely, and future research may consider exploring substance use disorder severity as a predictor of contingency management. On the other hand, those with diagnoses of posttraumatic stress disorder or 3+ medical comorbidities were less likely to receive contingency management. Clinics serving those with substance use disorder are often siloed from clinics serving other conditions in the Veteran Affair Healthcare System, even though they commonly co-occur. It is possible, for example, that those with posttraumatic stress disorder are more likely to be referred to a PTSD-specific clinic. The methods did not allow the study to determine which diagnosis was “primary” for the participant – if PTSD was primary for the participant, this could help explain why those with PTSD were less likely to receive contingency management. In those cases, strategies to integrate contingency management for substance use, including but not limited to stimulant use, into mental health treatment settings may prove helpful.
The authors defined contingency management treatment as having a single session. Although this does provide an overview of who was likely to receive any contingency management at all, future research may examine predictors of the number of sessions they completed to better understand factors associated with the dose of treatment.
There was a decrease in contingency management utilization during the COVID-19 pandemic, and this study period began in late 2020. It is possible that a greater number of individuals were receiving care before the pandemic or in the years that followed, and the authors did not look at year as a predictor.
Although prior research has found good positive effects for contingency management as a treatment for stimulant use disorder, this study did not examine the substance use outcomes.
BOTTOM LINE
Contingency management is shown to be helpful in reducing stimulant use but has not been widely adopted across the VA Healthcare System, despite extensive dissemination and implementation efforts. Over the two-year span from 2020 to 2022, contingency management receipt was more likely for patients who were between the ages 30–64, Black race, had a service-connected disability, was experiencing housing instability, had alcohol, opioid or other drug use disorders in addition to stimulant use disorder, or had more prior stimulant use disorder treatment visits; contingency management was less likely for patients who live in rural areas, have PTSD, or have a higher number of medical comorbidities. More research is needed to understand more about the low degree of uptake of this potentially beneficial practice and why only certain patients seem to get it and not others.
For individuals and families seeking recovery: If you are struggling to reduce your use of stimulants such as cocaine or amphetamine/methamphetamine, there are effective treatments that may help you, such as contingency management. Although there are barriers to receiving contingency management, many places are beginning to offer these services. If you are a Veteran and you receive services in in the VA, ask your healthcare providers for a referral to receive contingency management.
For treatment professionals and treatment systems: If your patients struggle with stimulant use disorder, you may consider learning more about contingency management and whether you may implement this treatment within your clinic or broader treatment environment. In the USA, you may obtain free consultation and training on how to deliver contingency management in your practice through the Opioid Response Network (see: opioidresponsenetwork.org). If you have reservations about contingency management, consider learning more about the research and theory that drove its development, and the potential individual and societal benefits.
For scientists: This research tells us who had a stimulant use disorder and received contingency management, which may help guide efforts to increase utilization of this empirically-supported intervention. However, this study was unable to answer why these patient characteristics were associated with contingency management. Future research may consider exploring factors that explain this effect to learn better how to mechanistically target gaps in implementation and dissemination. For example, if provider beliefs about contingency management or people with stimulant use disorder interfere with utilization of contingency management. Also, greater specific knowledge of the effects of contingency management implementation and duration of its effects on substance use and related outcomes within the VA population would be helpful.
For policy makers: There are considerable policy barriers that prevent the implementation of contingency management, including those related to anti-kickback statutes. Policies that reduce barriers to contingency management might help reduce the public health burden of stimulant use disorder. Further, more funding is needed to understand gaps in contingency management implementation.
Stimulant use, such as methamphetamine or cocaine use, has rapidly increased in the past decade. Despite extensive development efforts, there are currently no Food and Drug Administration (FDA)-approved medications to treat stimulant use disorder. However, one intervention in particular, contingency management has proven quite useful for treating stimulant use disorder. Contingency management is a method in which rewards, such as money or vouchers, are provided to patients contingent upon their ability to meet some outcome, such as attending a treatment session or remaining abstinent (i.e., testing negative on a drug screen). These contingencies also create what is known as an “opportunity cost”: using substances takes away the opportunity to get the monetary/voucher reward they would otherwise receive. Studies have demonstrated that contingency management is a very helpful approach to increase abstinence broadly for people who have substance use disorders, and for people with stimulant use disorder more specifically.
Contingency management’s promise as a treatment for stimulant use disorder has not manifested in widespread dissemination across healthcare systems due to notable barriers that include stigma and national policies that prevent giving gifts with monetary value to patients. Some of the more fervent opposition notes that, in some cases, the rewards are drawn from many options, which can be perceived as a form of gambling. In 2011, however, The Department of Veteran Affairs officially “rolled out” implementation of contingency management across the Veteran Affairs Healthcare System. Initial evaluations found widespread uptake of contingency management in targeted clinics, alongside promising engagement and substance use outcomes. Yet, recent studies have shown that only a small number of people with stimulant use disorder in the Veteran Affairs Healthcare System actually receive this empirically supported intervention. To inform ways to enhance uptake, this study investigated characteristics of patients who did and did not receive contingency management among patients with stimulant use disorder within VA programs that begun to implement such programming in the US VA Healthcare System.
HOW WAS THIS STUDY CONDUCTED?
This study used archival data from the Veteran Affairs Healthcare System electronic medical record. Within facilities that had begun to implement contingency management, the authors extracted all patients who had at least one visit occurring between the 2-year period of October 1, 2020 and September 30, 2022, and had a chart diagnosis of stimulant use disorder. The authors wanted to know how many people with stimulant use disorder across the VA Healthcare System were receiving contingency management, and whether certain patient characteristics predicted who did and did not receive contingency management.
To this end, the authors also extracted data on sex, age, race, ethnicity, rurality, Veteran Affairs service connection (service connection ratings are based on whether a disability is linked to their military service, and the degree to which it impacts their functioning, as determined by the Department of Veteran Affairs), housing instability, substance use disorder comorbidity, mental health comorbidity, prior stimulant use disorder treatment engagement, and the number of stimulant use disorder medication management visits. These variables were included together in a model predicting contingency management utilization. Such statistical adjustments help to isolate the effect of interest – i.e., whether a participant characteristic is independently related to receiving contingency management. Also, in order to increase confidence that effects are true, the authors used complex statistical models to account for the fact that some patients came from the same facilities, and that facilities may differ in their ability to implement contingency management.
Importantly, to determine who used contingency management, the VA Healthcare System developed a common contingency management note template in 2018. The authors defined contingency management engagement as those with at least one contingency management note. All predictors (e.g., age, comorbidities, etc.) were extracted either at the time of the index visit, or from notes within the prior year.
The sample was, on average, 55 years of age, 93% male, 49% White, 42% Black, and 2% identified as another race; 7% identified as Hispanic. Approximately half had a service connection above 50%, 40% were experiencing homelessness, and 90% lived in urban areas.
WHAT DID THIS STUDY FIND?
Few patients with stimulant use disorder were receiving contingency management
The authors identified 93,960 patients who met criteria for stimulant use disorder during this period. Only 1% (1,113 VA patients) received contingency management in the year after their first visit.
Contingency management utilization was determined by key variables such as age, race, service connection, treatment engagement, and comorbidity
Compared to those between the ages of 18-29, those who were between 30-44 and those between 45-64 were approximately twice as likely to receive contingency management. Black patients were approximately 50% more likely to receive contingency management relative to White patients; other racial groups were not more or less likely to receive contingency management relative to White patients (see Graph below).
Those in rural areas were 35% less likely to receive contingency management.
Housing instability was also associated with a 70% greater likelihood of receiving contingency management. Also, comorbidity – other disorders in addition to stimulant use disorder – was associated with likelihood of receiving contingency management, but in different directions for substance and mental health comorbidities. Those meeting criteria for opioid use disorder or alcohol use disorder were approximately 20% more likely to receive contingency management, and those with “other drug disorder” (which in this study was defined by sedatives, hallucinogens, and inhalants) were approximately 33% more likely to receive contingency management compared to those without one of those diagnoses. On the other hand, those with a posttraumatic stress disorder diagnosis (in addition to their stimulant use disorder diagnosis) were 15% less likely to receive contingency management compared to those without that diagnosis.
Relative to those without service connection, those with service connections were 25-35% more likely to receive contingency management.
Finally, the number of past year stimulant use disorder treatment visits predicted greater likelihood of receiving contingency management, with each additional psychotherapy visit increasing the likelihood by 1%, and each medication management visit increasing the likelihood by 5%.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Despite the national rollout of contingency management in the Veteran Affairs Healthcare System, patients with stimulant use disorder were still unlikely to receive contingency management: only 1% received at least one session of contingency management. It is unclear why contingency management, a very useful intervention for stimulant use disorder, has been adopted so infrequently. One possibility is that these data were collected at the beginning of the COVID-19 pandemic, a time when contingency management was not being deployed as often. Irrespective of the underlying reasons, engagement in any treatment requires the procedures to be implemented in clinics, for providers to be trained to properly execute the treatment and to begin to use that treatment when necessary, and for patients to select this treatment when given the opportunity. It is difficult to know where in this cascade we see the greatest impact on utilization of this treatment.
Nevertheless, there were some patient characteristics that were associated with the likelihood of receiving contingency management, including those who are between ages 30–64, Black race, experiencing housing instability, service-connected disability, and those who live in rural areas. Understanding how these factors impact receipt of a robust treatment for stimulant use disorder may help providers and Veteran Affairs decision makers increase uptake among populations that are less likelihood to receive it.
The finding that those who have alcohol, opioid or other drug use disorders in addition to stimulant use disorder, as well as those with more therapy and medication visits, were more likely to receive contingency management suggests that greater severity may in part predict contingency management receipt. Unfortunately, the method of data collection prevents exploring this question more closely, and future research may consider exploring substance use disorder severity as a predictor of contingency management. On the other hand, those with diagnoses of posttraumatic stress disorder or 3+ medical comorbidities were less likely to receive contingency management. Clinics serving those with substance use disorder are often siloed from clinics serving other conditions in the Veteran Affair Healthcare System, even though they commonly co-occur. It is possible, for example, that those with posttraumatic stress disorder are more likely to be referred to a PTSD-specific clinic. The methods did not allow the study to determine which diagnosis was “primary” for the participant – if PTSD was primary for the participant, this could help explain why those with PTSD were less likely to receive contingency management. In those cases, strategies to integrate contingency management for substance use, including but not limited to stimulant use, into mental health treatment settings may prove helpful.
The authors defined contingency management treatment as having a single session. Although this does provide an overview of who was likely to receive any contingency management at all, future research may examine predictors of the number of sessions they completed to better understand factors associated with the dose of treatment.
There was a decrease in contingency management utilization during the COVID-19 pandemic, and this study period began in late 2020. It is possible that a greater number of individuals were receiving care before the pandemic or in the years that followed, and the authors did not look at year as a predictor.
Although prior research has found good positive effects for contingency management as a treatment for stimulant use disorder, this study did not examine the substance use outcomes.
BOTTOM LINE
Contingency management is shown to be helpful in reducing stimulant use but has not been widely adopted across the VA Healthcare System, despite extensive dissemination and implementation efforts. Over the two-year span from 2020 to 2022, contingency management receipt was more likely for patients who were between the ages 30–64, Black race, had a service-connected disability, was experiencing housing instability, had alcohol, opioid or other drug use disorders in addition to stimulant use disorder, or had more prior stimulant use disorder treatment visits; contingency management was less likely for patients who live in rural areas, have PTSD, or have a higher number of medical comorbidities. More research is needed to understand more about the low degree of uptake of this potentially beneficial practice and why only certain patients seem to get it and not others.
For individuals and families seeking recovery: If you are struggling to reduce your use of stimulants such as cocaine or amphetamine/methamphetamine, there are effective treatments that may help you, such as contingency management. Although there are barriers to receiving contingency management, many places are beginning to offer these services. If you are a Veteran and you receive services in in the VA, ask your healthcare providers for a referral to receive contingency management.
For treatment professionals and treatment systems: If your patients struggle with stimulant use disorder, you may consider learning more about contingency management and whether you may implement this treatment within your clinic or broader treatment environment. In the USA, you may obtain free consultation and training on how to deliver contingency management in your practice through the Opioid Response Network (see: opioidresponsenetwork.org). If you have reservations about contingency management, consider learning more about the research and theory that drove its development, and the potential individual and societal benefits.
For scientists: This research tells us who had a stimulant use disorder and received contingency management, which may help guide efforts to increase utilization of this empirically-supported intervention. However, this study was unable to answer why these patient characteristics were associated with contingency management. Future research may consider exploring factors that explain this effect to learn better how to mechanistically target gaps in implementation and dissemination. For example, if provider beliefs about contingency management or people with stimulant use disorder interfere with utilization of contingency management. Also, greater specific knowledge of the effects of contingency management implementation and duration of its effects on substance use and related outcomes within the VA population would be helpful.
For policy makers: There are considerable policy barriers that prevent the implementation of contingency management, including those related to anti-kickback statutes. Policies that reduce barriers to contingency management might help reduce the public health burden of stimulant use disorder. Further, more funding is needed to understand gaps in contingency management implementation.
Stimulant use, such as methamphetamine or cocaine use, has rapidly increased in the past decade. Despite extensive development efforts, there are currently no Food and Drug Administration (FDA)-approved medications to treat stimulant use disorder. However, one intervention in particular, contingency management has proven quite useful for treating stimulant use disorder. Contingency management is a method in which rewards, such as money or vouchers, are provided to patients contingent upon their ability to meet some outcome, such as attending a treatment session or remaining abstinent (i.e., testing negative on a drug screen). These contingencies also create what is known as an “opportunity cost”: using substances takes away the opportunity to get the monetary/voucher reward they would otherwise receive. Studies have demonstrated that contingency management is a very helpful approach to increase abstinence broadly for people who have substance use disorders, and for people with stimulant use disorder more specifically.
Contingency management’s promise as a treatment for stimulant use disorder has not manifested in widespread dissemination across healthcare systems due to notable barriers that include stigma and national policies that prevent giving gifts with monetary value to patients. Some of the more fervent opposition notes that, in some cases, the rewards are drawn from many options, which can be perceived as a form of gambling. In 2011, however, The Department of Veteran Affairs officially “rolled out” implementation of contingency management across the Veteran Affairs Healthcare System. Initial evaluations found widespread uptake of contingency management in targeted clinics, alongside promising engagement and substance use outcomes. Yet, recent studies have shown that only a small number of people with stimulant use disorder in the Veteran Affairs Healthcare System actually receive this empirically supported intervention. To inform ways to enhance uptake, this study investigated characteristics of patients who did and did not receive contingency management among patients with stimulant use disorder within VA programs that begun to implement such programming in the US VA Healthcare System.
HOW WAS THIS STUDY CONDUCTED?
This study used archival data from the Veteran Affairs Healthcare System electronic medical record. Within facilities that had begun to implement contingency management, the authors extracted all patients who had at least one visit occurring between the 2-year period of October 1, 2020 and September 30, 2022, and had a chart diagnosis of stimulant use disorder. The authors wanted to know how many people with stimulant use disorder across the VA Healthcare System were receiving contingency management, and whether certain patient characteristics predicted who did and did not receive contingency management.
To this end, the authors also extracted data on sex, age, race, ethnicity, rurality, Veteran Affairs service connection (service connection ratings are based on whether a disability is linked to their military service, and the degree to which it impacts their functioning, as determined by the Department of Veteran Affairs), housing instability, substance use disorder comorbidity, mental health comorbidity, prior stimulant use disorder treatment engagement, and the number of stimulant use disorder medication management visits. These variables were included together in a model predicting contingency management utilization. Such statistical adjustments help to isolate the effect of interest – i.e., whether a participant characteristic is independently related to receiving contingency management. Also, in order to increase confidence that effects are true, the authors used complex statistical models to account for the fact that some patients came from the same facilities, and that facilities may differ in their ability to implement contingency management.
Importantly, to determine who used contingency management, the VA Healthcare System developed a common contingency management note template in 2018. The authors defined contingency management engagement as those with at least one contingency management note. All predictors (e.g., age, comorbidities, etc.) were extracted either at the time of the index visit, or from notes within the prior year.
The sample was, on average, 55 years of age, 93% male, 49% White, 42% Black, and 2% identified as another race; 7% identified as Hispanic. Approximately half had a service connection above 50%, 40% were experiencing homelessness, and 90% lived in urban areas.
WHAT DID THIS STUDY FIND?
Few patients with stimulant use disorder were receiving contingency management
The authors identified 93,960 patients who met criteria for stimulant use disorder during this period. Only 1% (1,113 VA patients) received contingency management in the year after their first visit.
Contingency management utilization was determined by key variables such as age, race, service connection, treatment engagement, and comorbidity
Compared to those between the ages of 18-29, those who were between 30-44 and those between 45-64 were approximately twice as likely to receive contingency management. Black patients were approximately 50% more likely to receive contingency management relative to White patients; other racial groups were not more or less likely to receive contingency management relative to White patients (see Graph below).
Those in rural areas were 35% less likely to receive contingency management.
Housing instability was also associated with a 70% greater likelihood of receiving contingency management. Also, comorbidity – other disorders in addition to stimulant use disorder – was associated with likelihood of receiving contingency management, but in different directions for substance and mental health comorbidities. Those meeting criteria for opioid use disorder or alcohol use disorder were approximately 20% more likely to receive contingency management, and those with “other drug disorder” (which in this study was defined by sedatives, hallucinogens, and inhalants) were approximately 33% more likely to receive contingency management compared to those without one of those diagnoses. On the other hand, those with a posttraumatic stress disorder diagnosis (in addition to their stimulant use disorder diagnosis) were 15% less likely to receive contingency management compared to those without that diagnosis.
Relative to those without service connection, those with service connections were 25-35% more likely to receive contingency management.
Finally, the number of past year stimulant use disorder treatment visits predicted greater likelihood of receiving contingency management, with each additional psychotherapy visit increasing the likelihood by 1%, and each medication management visit increasing the likelihood by 5%.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Despite the national rollout of contingency management in the Veteran Affairs Healthcare System, patients with stimulant use disorder were still unlikely to receive contingency management: only 1% received at least one session of contingency management. It is unclear why contingency management, a very useful intervention for stimulant use disorder, has been adopted so infrequently. One possibility is that these data were collected at the beginning of the COVID-19 pandemic, a time when contingency management was not being deployed as often. Irrespective of the underlying reasons, engagement in any treatment requires the procedures to be implemented in clinics, for providers to be trained to properly execute the treatment and to begin to use that treatment when necessary, and for patients to select this treatment when given the opportunity. It is difficult to know where in this cascade we see the greatest impact on utilization of this treatment.
Nevertheless, there were some patient characteristics that were associated with the likelihood of receiving contingency management, including those who are between ages 30–64, Black race, experiencing housing instability, service-connected disability, and those who live in rural areas. Understanding how these factors impact receipt of a robust treatment for stimulant use disorder may help providers and Veteran Affairs decision makers increase uptake among populations that are less likelihood to receive it.
The finding that those who have alcohol, opioid or other drug use disorders in addition to stimulant use disorder, as well as those with more therapy and medication visits, were more likely to receive contingency management suggests that greater severity may in part predict contingency management receipt. Unfortunately, the method of data collection prevents exploring this question more closely, and future research may consider exploring substance use disorder severity as a predictor of contingency management. On the other hand, those with diagnoses of posttraumatic stress disorder or 3+ medical comorbidities were less likely to receive contingency management. Clinics serving those with substance use disorder are often siloed from clinics serving other conditions in the Veteran Affair Healthcare System, even though they commonly co-occur. It is possible, for example, that those with posttraumatic stress disorder are more likely to be referred to a PTSD-specific clinic. The methods did not allow the study to determine which diagnosis was “primary” for the participant – if PTSD was primary for the participant, this could help explain why those with PTSD were less likely to receive contingency management. In those cases, strategies to integrate contingency management for substance use, including but not limited to stimulant use, into mental health treatment settings may prove helpful.
The authors defined contingency management treatment as having a single session. Although this does provide an overview of who was likely to receive any contingency management at all, future research may examine predictors of the number of sessions they completed to better understand factors associated with the dose of treatment.
There was a decrease in contingency management utilization during the COVID-19 pandemic, and this study period began in late 2020. It is possible that a greater number of individuals were receiving care before the pandemic or in the years that followed, and the authors did not look at year as a predictor.
Although prior research has found good positive effects for contingency management as a treatment for stimulant use disorder, this study did not examine the substance use outcomes.
BOTTOM LINE
Contingency management is shown to be helpful in reducing stimulant use but has not been widely adopted across the VA Healthcare System, despite extensive dissemination and implementation efforts. Over the two-year span from 2020 to 2022, contingency management receipt was more likely for patients who were between the ages 30–64, Black race, had a service-connected disability, was experiencing housing instability, had alcohol, opioid or other drug use disorders in addition to stimulant use disorder, or had more prior stimulant use disorder treatment visits; contingency management was less likely for patients who live in rural areas, have PTSD, or have a higher number of medical comorbidities. More research is needed to understand more about the low degree of uptake of this potentially beneficial practice and why only certain patients seem to get it and not others.
For individuals and families seeking recovery: If you are struggling to reduce your use of stimulants such as cocaine or amphetamine/methamphetamine, there are effective treatments that may help you, such as contingency management. Although there are barriers to receiving contingency management, many places are beginning to offer these services. If you are a Veteran and you receive services in in the VA, ask your healthcare providers for a referral to receive contingency management.
For treatment professionals and treatment systems: If your patients struggle with stimulant use disorder, you may consider learning more about contingency management and whether you may implement this treatment within your clinic or broader treatment environment. In the USA, you may obtain free consultation and training on how to deliver contingency management in your practice through the Opioid Response Network (see: opioidresponsenetwork.org). If you have reservations about contingency management, consider learning more about the research and theory that drove its development, and the potential individual and societal benefits.
For scientists: This research tells us who had a stimulant use disorder and received contingency management, which may help guide efforts to increase utilization of this empirically-supported intervention. However, this study was unable to answer why these patient characteristics were associated with contingency management. Future research may consider exploring factors that explain this effect to learn better how to mechanistically target gaps in implementation and dissemination. For example, if provider beliefs about contingency management or people with stimulant use disorder interfere with utilization of contingency management. Also, greater specific knowledge of the effects of contingency management implementation and duration of its effects on substance use and related outcomes within the VA population would be helpful.
For policy makers: There are considerable policy barriers that prevent the implementation of contingency management, including those related to anti-kickback statutes. Policies that reduce barriers to contingency management might help reduce the public health burden of stimulant use disorder. Further, more funding is needed to understand gaps in contingency management implementation.